
Abstract
This study provides a descriptive epidemiological data of thyroid cancer cases diagnosed from 2001 to 2008 among Saudi women, including the frequency and percentage of cases, the crude incidence rate (CIR) and the age-standardised incidence rate (ASIR) stratified by the region and year of diagnosis. This is a retrospective descriptive epidemiological analysis of all Saudi thyroid cancer cases recorded in the Saudi Cancer Registry (SCR) between January 2001 and December 2008. The statistical analyses were applied using descriptive statistics with the Statistical Package for the Social Sciences version 20.0. A total of 2,930 cases were recorded in the SCR between January 2001 and December 2008. The region of Riyadh in Saudi Arabia had the highest overall ASIR at 9.43 per 100,000 women, followed by Tabuk at 7.11 and eastern region at 6.5, while Jazan and Jouf had the lowest average ASIRs at 1.97 and at 2.72, respectively. The region of Qassim recorded the greatest changes of ASIR at 5.5 per 100,000 women from 2001 to 2008. There was a slight increase in the CIRs and ASIRs for thyroid cancer in Saudi Arabia between 2001 and 2008. Riyadh, Tabuk and eastern region were the highest overall ASIR in Saudi Arabia. While, Jazan and Hail had the lowest rates. Finally, the region of Qassim had the highest changes in CIR and ASIR from 2001 to 2008. Further analytical studies are needed to determine the potential risk factors of thyroid cancer disease among Saudi women.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Thyroid malignancy is the most diagnosed cancer of endocrine system, representing 2 % of all cancers worldwide [1–3]. The incidence rates of thyroid cancer vary by age, sex, geographic populations and ethnic groups [2]. It accounts for approximately 1.9 % of all malignant cancers in United States [4]. However, the incidence rate of thyroid cancer is increasing significantly among women compared to men, and nearly 2 out 3 cases are recorded in younger persons aged <55 years old [5]. According to the American Cancer Society, in 2013, an estimated 45,310 women will be diagnosed with thyroid cancer in United States, and 1,040 is the expected number of deaths [5].
In Saudi Arabia, the International Agency for Research on Cancer (IARC) estimated that the age-standardised incidence rate (ASIR) for thyroid cancer was 5.5 per 100,000 women in 2008, and the age-standardised mortality rate (ASMR) was 2.9 per 100,000 women [6]. Furthermore, the registry of King Faisal Specialist Hospital and Research Centre (2011) recorded 4,888 cases (6.7 %) of thyroid cancer admitted to the hospital during the years 1975–2011 [7]. In 2008, The Saudi Cancer Registry (SCR) reported that cancer of thyroid ranked second in cancer incidence among female population, and thirteenth among male [8]. The age standardized incidence rate of thyroid cancer in Saudi Arabia is slightly low in comparison with some Arabian Gulf countries. For example, in 2008, the reported ASIR for Qatar, Bahrain and Oman were higher than Saudi Arabia, at 9.3, 7.4 and 5.7, respectively [6]. However, the main objectives of this study were to investigate and describe the distribution of thyroid cancer in terms of the characteristics of person, place and time among Saudi women [9].
Materials and Methods
We conducted a retrospective descriptive epidemiological study of all Saudi women with thyroid cancer cases diagnosed between January 2001 and December 2008. The analyses were limited to women because the incidence rate of thyroid cancer is very high in Saudi women compared to Saudi men. Therefore, we concentrated to describe the pattern of the disease in Saudi female only. The source of data for this study was made possible by the SCR, which is a population-based registry established in 1994 through the Ministry of Health in Saudi Arabia. The data cannot be obtained directly from the SCR, except the published reports. There were no available data from 1994 to 2000, and the latest published report of SCR was in 2008.
Since 2001, the SCR has been providing reports on the pattern of cancer in Saudi Arabia with a primary objective of defining the population-based incidence of the disease. Based on these data, there are currently comprehensive reports for 13 administrative regions from 2001 to 2008 that discuss the frequency with percentage of cases, the CIR and the ASIR, stratified by the provinces of Saudi Arabia and the years of diagnosis. This study was conducted using these reports to critically gather all of the information from the SCR with the aim of presenting the descriptive epidemiology of thyroid cancer in Saudi Arabia.
For data analysis, we used the Statistical Package for the Social Sciences version 20.0 (SPSS). The descriptive analysis of the epidemiological data was performed by calculating the averages for percentages, CIR and ASIR stratified by the age group, region and year of diagnosis. The percentage was calculated by adding the number of cases of thyroid cancer and then dividing that number by the total number of female cancer cases. Furthermore, the age-standardised incidence rates per 100,000 women were calculated by SCR, based on a (Segi) standard for World populations who have an intermediate-age. This is a particularly important direct age standardization when making comparisons between different populations with respect to the age structure [10, 11]. The direct age standardization is calculated by identifying the age-specific incidence rate for each age group and multiply it to the number of persons in each age group of the standard population.
Results
A total of 2,930 cases were documented in the SCR between January 2001 and December 2008. The frequency of cases with thyroid cancer increased slightly from 2001 to 2008. In Fig. 1a, b it is shown that there were 254 cases in 2001 (9.3, 95 % CI 5.3–13.3 %) of female cancer cases. This figure rose to 343 by 2003, representing an increase of 1.2 %, this was the highest percentage stated by the SCR (2003). From 2005 to 2008, the number of thyroid cancer cases remained slightly high and the percentages were fluctuated between 9.4 and 10.3 %, respectively.

a, b Number and percentage of thyroid cancer cases among Saudi women from 2001 to 2008. c, d Overall number and percentage of thyroid cancer cases distribution by age group among Saudi women from 2001 to 2008
The number and percentage of thyroid cancer cases between 2001 and 2008, stratified by age group, was calculated from the SCR (Table 1) and (Fig. 1c, d). The age groups reported correspond to 00–14, 15–29, 30–44, 45–59, 60–74, and over the age of 75 years. According to the overall numbers and percentages from 2001 to 2008, the age groups that recorded the highest affected by thyroid cancer were very young women aged 30–44 years, with an average 138 cases representing 37 % of the total number of thyroid cancer cases, followed by those aged 15–29 years, with overall 97 cases representing 27 %. Alternatively, the older groups aged 45–59, 60–74 and over 75 years, recorded the lowest overall numbers and percentages, with <75 cases representing 20 % of the total number of thyroid cancer cases.
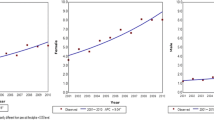
The CIRs stratified by the year of diagnosis from 2001 to 2008 per 100,000 women indicate a steady increase of thyroid cancer among women in Saudi Arabia. According to Table 2 and Fig. 2a, a CIR of 3.2 (95 % CI 1.91–4.49) per 100,000 women was estimated in 2001, and a CIR of 5.3 (95 % CI 4.23–6.37) per 100,000 women was estimated in 2008. However, in 2007, the CIR of 5.4 (95 % CI 3.96–6.84) per 100,000 women was the highest rate recorded by SCR.

a The crude incidence rate of thyroid cancer cases among Saudi women from 2001 to 2008. b Overall crude incidence rate of thyroid cancer cases distribution by region among Saudi women from 2001 to 2008. c The age-standardised incidence rate of thyroid cancer cases among Saudi women from 2001 to 2008. d Overall age-standardised incidence rate of thyroid cancer cases distribution by region among Saudi women from 2001 to 2008
The overall CIR of thyroid cancer stratified by the region of Saudi Arabia from 2001 to 2008 per 100,000 women was calculated from the SCR, as shown in Table 3 and Fig. 2b. The region of Riyadh in Saudi Arabia had the highest overall CIR for thyroid cancer at 6.78 (95 % CI 5.76–7.80) per 100,000 women, followed by Tabuk at 5.0 (95 % CI 3.38–6.61) and eastern region at 4.73 (95 % CI 3.78–5.68). Furthermore, Jazan (95 % CI 1.0–2.0), Jouf (95 % CI 0.68–2.53), and Najran (95 % CI 1.35–3.80) had the lowest average CIRs for thyroid cancer among Saudi women at 1.51, 1.61, and 2.57, respectively.
The ASIR of thyroid cancer stratified by the year of diagnosis in Saudi Arabia, from 2001 to 2008 per 100,000 women, was calculated from the SCR (Table 2) and (Fig. 2c). There was a slight increase in the cases of thyroid cancer diagnosed between 2001 and 2008, with the highest ASIR of 6.8 recorded in 2008 (95 % CI 5.23–8.37), according to reports released by the SCR. Similarly, it is shown in Table 3 and Fig. 2d, that the region of Riyadh was the highest overall ASIR for thyroid cancer at 9.43 (95 % CI 8.25–10.62) per 100,000 women, followed by Tabuk at 7.11 (95 % CI 5.18–9.03) and eastern region at 6.5 (95 % CI 5.25–7.75). Alternatively, Jazan (95 % CI 1.30–2.64), and Jouf (95 % CI 0.47–4.97) had the lowest average ASIRs for thyroid cancer among Saudi women at 1.97 and 2.72, respectively.
Finally, the differences in the CIR and ASIR between 2001 and 2008 were calculated from the data published by the SCR, and investigated the pattern of thyroid cancer among Saudi women in different regions (Table 4). The greatest changes in percentages and rates were observed only in the region of Qassim (9.5 %, 5.6 CIR 5.5 ASIR). It means that the percentage of thyroid cancer cases among Saudi women in the region of Qassim, increased significantly by 9.5 % from 2001 to 2008. Furthermore, the CIR and ASIR increased by 5.6 and 5.5 cases per 100,000 women, respectively. However, the CIR and ASIR for all regions, with the exception of Qassim, were not statistically significant (P > 0.05) compared between the year of 2001 and 2008.
Discussion
The incidence rate of thyroid cancer cases among Saudi female is a big point of concern for government and population. In this study we concentrated on the CIR and ASIR of thyroid cancer in Saudi Arabia during the year 2001–2008. Notably, our study is considered the first descriptive epidemiology of thyroid cancer among women in different regions of Saudi Arabia. It describes the pattern and trend of the disease during the years 2001–2008. In addition, this study provides an important description for the actual trend, approving the significance of the disease. Our results indicate that the region of Riyadh, Tabuk and eastern region have the highest overall ASIRs for thyroid cancer among women in Saudi Arabia. While, the regions of Jazan and Jouf have the lowest overall ASIRs of thyroid cancer among women in Saudi Arabia during 2001–2008. In addition, the most affected age groups by thyroid cancer in different regions of Saudi Arabia, were younger women aged 15–29 and 30–44 years.
In this study, we have observed the changes in the percentage, CIR and the ASIR of thyroid cancer among women in different regions of Saudi Arabia from 2001 to 2008. The region of Qassim had the highest differences in the CIRs and ASIRs of thyroid cancer during the years 2001 and 2008, the changes were above the predicted values of rates during the years 2001–2008. However, the likely explanation for these differences in rates suggest that the region of Qassim is affected more by thyroid cancer over an 8-year period (2001–2008), and the probable reasons for the observed increase in incidence may have been due primarily to changes in the procedures and methods for identifying and diagnosing thyroid cancer. Although the down-trending rates recorded in Tabuk during the years 2001–2008, the overall CIR and ASIR still very high in that region compared to other different provinces of Saudi Arabia (Table 4), the probable explanation for the down-tending rates in Tabuk include the lack of screening programs for early detection of the thyroid cancer among women. Therefore, there are no screening programs for thyroid cancer and most of cases are identified in the last stage of cancer disease.
Despite the shortage of published information about geographic and time distribution of thyroid cancer among women in Saudi Arabia, except the SCR reports, we intend to discover the real pattern and trend of thyroid cancer among Saudi women, in different regions during the years 2001–2008. Therefore, the findings of our study are very significant to the researchers and decision makers in the field of medicine and health care administrations in Saudi Arabia, through support them with epidemiological descriptive results for the actual situation of thyroid cancer among women in different provinces of Saudi Arabia. Therefore, these outcomes will build a good indicators for generating hypotheses about the potential risk factors of thyroid cancer in the highest affected regions of Saudi Arabia, by conducting analytic epidemiologic studies that identify the relationships between the exposure and disease.
Conclusion
The epidemiological analysis of the reports registered by the Saudi Cancer Registry from 2001 to 2008, revealed that the CIR and ASIR of thyroid cancer among Saudi women are increasing slightly. The regions of Riyadh, Tabuk and eastern region had the highest overall CIRs and ASIRs in Saudi Arabia. While, Jazan and Hail recorded the lowest rates. As mentioned earlier, the region of Qassim documented the greatest differences in the CIR and ASIR of thyroid cancer among Saudi women from 2001 to 2008. However, further analytical studies might be conducted to explore the potential risk factors of thyroid cancer among Saudi women.
References
Canadian Cancer Society and the National Cancer Institute of Canada. Canadian Cancer Statistics 2008. Toronto, ON, Canada, 1–14, 2008.
Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M, Boyle P. Cancer incidence in five continents. IX. Lyon: IARC; IARC Scientific Publications No. 160, 2007.
Sipos JA, Mazzaferri EL. Thyroid cancer epidemiology and prognostic variables. Clin Oncol. 2010;22(6):395–404.
Jemal A, Murray T, Ward E, et al. American cancer society. Cancer statistics, 2005. CA Cancer J Clin. 2005;55:10–30.
American Cancer Society. Global cancer facts and figures. 2nd ed. Atlanta: ACS; 2013.
GLOBOCAN (IARC). Section of Cancer Information. 2008; http://globocan.iarc.fr/. Accessed 21 Sep 2013.
King Faisal Specialist Hospital and Research Centre. Tumor registry annual report. 2011.
Saudi Cancer Registry. Cancer incidence report in Saudi Arabia. Ministry of Health. 2008.
Friis RH, Sellers TA. Epidemiology for public health practice. 4th ed. Sudbury: Jones and Bartlett; 2009.
Ahmad OB, Boschi-pinto C, Lopez AD. Age standardization of rates: a new who standard GPE Discussion Paper Series: No. 31 EIP/GPE/EBD World Health Organization 2001; (31).
Doll R, Payne PM, Waterhouse JAH. Cancer incidence in five countries. International Union Against Cancer. Berlin: Springer; 1966.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Alghamdi, I.G., Hussain, I.I., Alghamdi, M.S. et al. The Incidence Rate of Thyroid Cancer Among Women in Saudi Arabia: An Observational Descriptive Epidemiological Analysis of Data from Saudi Cancer Registry 2001–2008. J Immigrant Minority Health 17, 638–643 (2015). https://doi.org/10.1007/s10903-014-0044-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10903-014-0044-5