
Abstract
In this study we quantify the impact of a partnership between a dedicated health clinic for government assisted refugees (GARs), a local reception centre and community providers, on wait times and referrals. This study used a before and after, repeated survey study design to analyze archived administrative data. Using various statistical techniques, outcomes for refugees arriving 18 months prior to the introduction of the clinic were compared with those of refugees arriving in the 18 months after the clinic was established. Our investigation revealed wait times to see a health care provider decreased by 30 % with the introduction of a dedicated refugee health clinic. The likelihood of GARs being referred to physician specialists decreased by 45 %, but those referred were more likely to require multiple referrals due to increasingly complex medical needs. Referrals to non-physician specialist health care providers nearly doubled following the availability of the clinic. The time-limited, but intense health needs of GARs, require an integrated community-based primary healthcare intervention that includes dedicated health system navigators to support timely, more culturally appropriate care and successful integration.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In 2011, 27,872 refugees arrived in Canada; a quarter of them were government assisted refugees or GARs; part of Canada’s commitment to the United Nations (1951) Convention Relating to the Status of Refugees which resettles those who have a “well-founded fear of being persecuted”. With the enactment into law of the Immigration and Refugee Protection Act (IRPA) in 2002, GARs arrive sicker and with less social capital as priority is given to those whose vulnerability and need for protection is greatest, rather than those who are most likely to settle in Canada. Consequently, GARs are expected to experience integration challenges due to complex physical and mental health care needs [1].
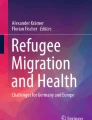
About a third of newly arrived GARs are welcomed into six cities in Ontario (London, Hamilton, Toronto, Ottawa, Windsor and Kitchener). Often they struggle to access healthcare services due to barriers at the system, organizational and individual levels (see Fig. 1). For example, shortages of primary care physicians, language, lack of familiarity with the healthcare system, cultural differences in expectations regarding which types of illnesses are perceived as treatable, the complexity of their conditions, and bureaucracy when billing Canada’s Interim Federal Health Program (IFHP) that provides coverage for health care costs until provincial health insurance is available.

Barriers to care framework for GARs
Primary care is considered a gateway to the healthcare system in many countries [2, 3], yet in Canada the sector has experienced a persistent shortage of family physicians in certain geographies [4]. This has resulted in a growing number of unattached or “orphan patients” who are unable to find a primary care practitioner to coordinate their care [5, 6]. Ontario cities experiencing a shortage of family physicians are designated as “under-serviced” and it is into this milieu that newly arrived GARs are resettled in the south-western Ontario town of Kitchener.
In 2011, Health Quality Ontario reported that 6.5 % of adult Ontarians did not have a family physician [7], down slightly from 7.4 % 2 years earlier [8]; 34 % of GARs do not have a regular doctor or health care provider [9]. In 2008, frustrated with the delays in care and an increasingly arduous process of identifying willing providers in Kitchener, the Reception House staff approached a local physician (NA) with an interest in global public health, social activism and cross-cultural studies, for assistance in establishing a refugee health clinic in his group family practice.
Methods
Studies have noted the lack of rigorous methodology in refugee health studies [10] and weak systematic evaluation of novel primary care interventions which eliminate barriers to successful settlement [11]. In this study we quantify the impact a dedicated refugee health clinic, in partnership with workers at the local receiving centre called Reception House, has on GAR’s access to services such as wait times for physician and specialist care, access to allied health services and physician specialists, familiarity with the healthcare system, and social constructs such as perceived family well-being.
The Intervention
Integrated health systems have a number of defining characteristics including a patient focus, standardized care through inter-professional teams, comprehensive services that span the continuum of care, and information systems that support communication [12]. The refugee health clinic model relies heavily on several of these integrating mechanisms to deliver responsive, culturally appropriate primary care, including an uncharacteristically close relationship with Reception House and its staff, partnerships between Reception House case workers and health professionals, translation services, comprehensive assessments, and international medical graduates in training whose input has enhanced the cultural sensitivity and competence of clinic processes.
Feldman’s (2006) framework of primary care services for refugees and asylum seekers—those enabling access to comprehensive primary care (gateway), comprehensive primary care where patients are rostered in a mainstream or “dedicated” refugee clinics (core), and essential support services (ancillary) such as interpretive services or specialty mental health services—is used to organize our description of the clinic’s care timing and workflows in Fig. 2.

Timeline and workflow for the provision of healthcare services at RH and RC
Gateway services are provided by Reception House case workers and trained professionals from the group family practice such as nurses and resident physician. Comprehensive care is delivered by family physicians at the refugee health clinic with language supports funded by Reception House, while ancillary services are delivered in the community by a variety of providers who are willing to treat GARs and are either able to bill the provincial government funded insurance plan or receive funding from IFHP. Case workers perform a critical role helping these new Canadians navigate the health system.
Accessing healthcare practitioners with appropriate knowledge of the refugee experience is particularly important for newly arrived GARs whose medical conditions are often uncommon in Canada and exacerbated by overcrowding in refugee camps due to in adequate sanitation, nutrition and infrastructure [13]. Medical staff at the refugee health clinic are experienced in diagnosing and treating GARs and have established protocols and guidelines for diagnosis and management of these diseases and conditions, including initial intake assessments performed onsite at Reception House within days of GARs’ arrival (see Table 1).
This study used a before and after, repeated survey study design comparing outcomes for GARs that received settlement assistance from Reception House before and after the establishment of the dedicated refugee clinic. Using administrative records, outcomes were anlayzed for refugees arriving 18 months prior to the introduction of the clinic and compared with those of refugees arriving in the 18 months after the clinic was established. The study received ethics clearance from the Research Ethics Board at Western University and Reception House.
Data Collection
Settlement workers maintain detailed logs of all refugee clients’ needs and appointments, including medical events. These records are entered into Citizenship and Immigration Canada’s Landed Immigrant data system. Anonymized versions of these intake and management logs were the primary source of data to evaluate outcomes such as the length of time to see a healthcare provider, and treatment and referrals for medical care. In addition, exit interviews conducted with clients after a year in Canada were used to assess self-reported outcomes.
No data from case notes was collected for a 4 month period following the date of the clinic opening to avoid artefacts arising from transitions in practice and work processes at the new clinic. Guidelines for coding and interpreting settlement workers’ case notes were discussed. Three researchers and a research assistant were trained to review and extract the relevant data. Each coded the same ten cases and compared results; inconsistencies were resolved. Subsequent random spot checks revealed no further inter-rater reliability issues.
Sample
The initial sample consisted of all GARs arriving at Reception House in the 18 months before the clinic was opened (N = 466) and, following the 4 month adjustment period, in the 18 months after (N = 406). Both adults and children were included in the sample. Various sub-samples were used to complete the analysis. A random sample from each family group was used for all binary variables, referral samples selected all individuals requiring either physician specialist only or both physicians and allied health referrals (only the first visit to each specialist was considered independent and included), and finally the exit interview sample which included all data available.
Statistical Analysis
Table 2 provides a description of the dependent variables used in the analysis and Table 3 a description of the covariates.
The dependent variables focus on outcomes that reflect the stated goals of the healthcare system in Ontario. Of note, in 2012 the quasi-autonomous organization responsible for healthcare quality in Ontario expressed a desire for improvement in wait times to see providers, and avoidance of hospitalization. Furthermore, they attributed accessibility, patient-centredness (providing care that is responsive to patients’ needs and preferences), and effectiveness as indicators of a high-performing healthcare system [14].
All five self-reported dependent variables in this study measure the refugee health clinic’s ability to deliver culturally appropriate, effective, and integrated community based primary healthcare or its impact. Some are more directly related to the work of the clinic, such as “reports improvements in ability to understand the healthcare system”, “reports improvements in ability to understand the mental health care system”, “reported improvements in family health”. Others are indirectly related, such as “reported being employed” or “reported problems accessing healthcare”, where the health status of the respondent is a contributing factor.
The remaining nine outcome variables are variants on the theme of providing appropriate and timely access to care. Lack of timely access to informed, family practitioners who were prepared to assume the care of this vulnerable population was a determining factor in the establishment of the refugee health clinic; hence variables such as “saw a healthcare provider”, “days to see a healthcare provider”, and “saw any type of specialist” are anticipated to provide a measure of the clinic’s success in accessing care. However, the clinic was unable to care for clients over the long-term; dependent variables such as “found a family physician”, reflect the goal of the clinic to transfer primary care to a permanent family practitioner.
A number of factors were identified as having the potential to confound or interact with the dependent variables and are listed in Table 3. Those with technical or professional skills and English-speaking ability, and the more educated and literate were predicted to be more likely to find employment. Older adults are more likely to report age-related illness in addition to other conditions, and refugees with more social support are expected to better navigate the healthcare system. Self-reported health problems will prompt more immediate access to care, and health risks identified by a physician were predicted to increase the likelihood of a referral—the impact of both variables was controlled during the analysis.
We analyzed client characteristics and the outcome variables using descriptive statistics. Bivariate associations between clinic exposure and all covariates were assessed using correlation analysis and Chi square (excepting age, which was evaluated using a t test). Social support, education and English ability had associations with exposure at p < 0.05, identifying them as potential confounders. Independent samples t tests identified no significant differences between the pre- and post-clinic samples for age, gender, and years and living situation in the last country, nor were there significant differences in self-identified health issues or physician identified health risks. Frequency data on referral events were also analyzed at this stage.
A combination of alternative regression techniques were used to measure the associations between clinic exposure and the outcome variables. The associations between clinic exposure and binary outcome variables were tested using binary logistical regression. These included “saw a healthcare provider”, “found a family physician”, “referral required to any type of specialist”, “saw a specialist”, and all the outcome variables derived from the exit interviews. In binary logistical regression the odds ratio generated by the logistic model represents the change in the likelihood of the event occurring after the clinic was established compared to before. In these regressions “clinic availability” was entered in step one, followed by the control variables relevant to each analysis (specified in the results section).
Interactions between clinic exposure, the potentially effect-modifying covariates, and time-related dependent variables (including days to see a healthcare provider, find a family physician, see a specialist and see a physician specialist) were tested using simple linear regression. For these regressions the variables were entered in three steps. The first step included “clinic availability”, the second step added in the covariates “social support”, “education”, and “English ability”. The third step included interaction terms between “clinic availability” and all three covariates that were included in step 2. The linear regression results were then used to inform an analysis of covariance (ANCOVA). The ANCOVA on log transformed (normalized) data was used to compare the means for “days to see a healthcare provider” and “days to find a family physician” in the pre- and post-clinic groups while accounting for the observed variability in “social support”, “occupation”, and “English ability”.
Results
A total of 872 records were examined, including 444 males (50.9 %) and 428 females (49.1 %). A large percentage were under the age of 18 (49.2 %). Thirty-eight different countries of birth were documented, and over 40 countries were listed as the country of last residence. Although statistically significant, the differences in country of origin and residence in the before and after samples were not considered substantive since both samples had high variability (primarily coming from Northwest Africa, the Middle East, and Southeast Asia), without a single identifiable cultural group dominating. Most of the refugees had little or no ability to speak English (71.4 %). Characteristics of random and referral samples, and key outcome variables are included in Table 4.
The types and frequencies of all referrals pre- and post-clinic were compared in order to better understand the notable differences. Before the clinic a total of 253 referrals were made (mean = 0.54 per individual). Among those, 151 (59.7 %) were for allied health including dentists, nutritionists, optometrists, massage therapists, and physiotherapists, while 102 (40.3 %) were for physician specialists. After the clinic a total of 488 referrals were made (mean = 1.20 per individual), 295 (60.5 %) were for allied health while 193 (39.5 %) were for physician specialists. This indicates that the proportions of referrals going to allied health workers and physicians was largely stable. All subsequent referral analysis focuses on referrals to physician specialists only.
Table 5 presents associations between clinic availability and key outcomes. For each of these associations the potential effect modification of English ability, social support, and occupation was examined and, subsequently disregarded; none was found to be independently associated with the respective outcome. GARs were no more likely to see any healthcare provider after the clinic opened (OR = 0.99, p = 0.151). The likelihood of an individual requiring a physician specialist went down 45 % as a result of seeing an refugee health clinic physician (OR = 0.55; p = 0.004). Considering that the mean number of referrals per individual post-clinic more than doubled, this indicates that fewer refugees required referrals, but those that did were requiring multiple types of specialist care. This supports Reception House workers’ observations that new refugees increasingly arrive with highly complex medical needs.
Clinic availability was significantly and substantively negatively associated with wait times to see a healthcare provider (β = −17.81, p < 0.05), meaning that after the clinic was established refugees were seen by a healthcare provider much faster than refugees who did not have access to the clinic. No other covariates showed significant associations with this outcome variable and the clinic did not affect the time it took to find a family physician or to see a specialist. The mean wait times (in days) to see a healthcare provider and find a family physician are presented in Table 6. Refugees’ wait time to see a healthcare provider decreased 30 % from approximately 30 days in the period before to 21 days in the period after the clinic opened (ratio of means = 0.70; p < 0.001).
The long term impact of the clinic on improving GARs’ “reported improvements in ability to understand health care system” was significant at all stages (p < 0.01). The first step in the model was significant (p < 0.01), indicating that access to the clinic was positively associated with this improved understanding. The latter two steps, which added health risks and control variables to the analysis, were not significant. The full model had a Nagelkerke score of 0.244 and suggested that people who accessed the clinic were 35 % more likely to report understanding the healthcare system than people who did not have access to the clinic (β = 1.35, p < 0.05). There was no significant association between access to the clinic and GARs reporting improvement in their ability to understand the mental health care system.
The overall model predicting that GARs “reported problems accessing healthcare” was significant (p < 0.01). The first step in the model, which included access to the clinic, was not significant. The latter two steps, which added predictors that were significantly negatively associated with reporting problems accessing healthcare included having physician-diagnosed health risks (β = −1.36, p < 0.01), being older (β = −0.06, p < 0.01), and having more education (β = −0.83, p < 0.05). Women also reported problems accessing healthcare (β = 1.23, p < 0.05). There was no link between clinic availability and employment. In keeping with prior literature on the subject there was a significant positive association between English ability and employment (β = 2.483, p < 0.001), meaning that refugees with moderate or fluent English were 2.48 times more likely to be employed during their first year in Canada than refugees with no or marginal English ability.
The overall model predicting “reported improvements in family health” was not significant and none of the individual steps were significant. However, the “yes/no” nature of the question resulted in severe range restriction. Most GARs enter Canada from dire circumstances; therefore it is not surprising that 98 % of respondents reported improvements in family health in the year after arrival.
Discussion
Prior to the refugee health clinic, GARs received episodic care for urgent health conditions through walk-in clinics and hospital emergency departments. Our investigation of the impact of timely, culturally appropriate care for refugees revealed a 30 % decrease in wait times to see a health care provider, and an 18 % increase in refugees finding a permanent family physician in the community in the year after their arrival. This notable achievement occurred at a time of increasing numbers of orphan patients in the general population and is attributed to strong relationships developed with the local physician community, timely transfer of comprehensive assessment and treatment records, and ongoing consultation between refugee health clinic and community family physicians post-transfer. GARs’ likelihood of finding a permanent family physician went up 18 % (OR = 1.18; p = 0.069); while the p value for this association does not meet conventional levels of statistical significance, as a trend value it indicates the probability of association being due to chance is small.
Referrals to non-physician primary health care providers (therapists, dentists, optometrists) nearly doubled after the clinic was established. As there were no significant differences in the number of physician-detected health risks between our before and after samples, this increase can be attributed to either better access to providers, diagnoses that required more treatment modalities, or a combination of both. Fewer GARs are being referred to physician specialists for care, suggesting that the clinic service providers are better equipped to diagnose and treat conditions prevalent amongst the refugee population. However, those patients who are referred are more likely to require referrals to multiple specialists, which is consistent with our profile of increasing medical complexity in new arrivals. These results support the notion that physicians with expertise in global health and access to translation services are more likely to treat patients at the primary care level, and that establishing supportive relationships with committed allied health specialists in the communitywill improve access to service. Those using the clinic reported improved understanding of and ability to navigate the healthcare system after a year in Canada.
The refugee health clinic delivers specialized primary care using providers who are aligned under one organization with common medical records, policies and procedures to guide professional practice. The model is dependent upon case workers accompanying clients to appointments, arranging language support and coordinating what is often a complex array of specialist and ancillary service appointments. This system navigator role for high needs or vulnerable populations is a concept which is increasingly evident in the healthcare sector particularly for vulnerable populations [15]. Models of care that include dedicated clinics with specialized services, such as the Primary Health Care Amplification Model in Australia [16] where patients are seen by a “beacon practice” then linked with community general practice, and “medical homes” [17] and “whole community” [18] models in the United States, have been documented in the literature. However, systematic analysis of the effectiveness of these models is notably absent; most are descriptive papers providing details on the processes, but not the outcomes, at these clinics.
To the best of our knowledge, this is the first quantitative analysis of the impact of a refugee health clinic on access to care and patient-reported outcomes. While the use of secondary and self-reported data in this study might introduce its own set of biases, the use of a before and after design and robust statistical analysis provides a level of rigour which is uncommon in refugee health research. A limitation is that while data entry in the administrative records was meticulous, it was performed by settlement workers with limited clinical knowledge.
Conclusions
The community-based, integrated, primary care model described here is one built on the goodwill of participating healthcare providers. The refugee health clinic operates part-time as a complementary service in a regular family practice, there are no formal contracts to outline service expectations, and there is no funding beyond normal settlement services support to manage this increasingly disadvantaged population. While the benefits of the refugee health clinic to accessibility and wait times are evident from this study, further research is required to determine its value at a system level, such as increasing deflections away from local emergency rooms.
Equitable access to care is a cornerstone of the Ontario and many other healthcare systems, yet barriers to appropriate care for refugees are increasing [19], a potentially catastrophic situation when combined with more medically complex needs. Comprehensive economic evaluations of initiatives such as the refugee health clinic are needed to allow policy-makers and healthcare providers to purposively design and deliver more effective, and culturally sensitive healthcare to some of our most vulnerable Canadian citizens.
New Contribution to the Literature
This study quantifies the impact of a novel primary care model for refugees on medical and social dimensions which contribute to their overall health, wellbeing and successful assimilation. The results suggest that community collaborations can influence the delivery of timely, more effective care for newly arrived refugees.
References
Citizenship and Immigration Canada. Evaluation of Government Assisted Refugees (GAR) and Resettlement Assistance Program (RAP). Canada: Ottawa; 2011.
Hofmarcher MM, Oxley J, Rusticelli E. Improved health system performance through better care coordination, OECD health working paper no. 30. Paris, France: OECD Publishing; 2007.
TD Economics. Charting a path to sustainable health care in Ontario: 10 proposals to restrain cost growth without compromising quality of care. Toronto, Canada: TD Bank Financial Group; 2010.
Evans RG. The Sorcerer’s Apprentices. Healthcare Policy. 2011;7(2):14–22.
Chan B. Supply of physicians’ services in Ontario. Toronto, Canada: Institute for Clinical Evaluative Sciences; 1999.
Kralj B. Physician distribution and physician shortage intensity in Ontario. Can Public Policy. 2001;17(2):167–78.
Health Quality Ontario. Quality monitor: 2011 report on Ontario’s health system. Toronto, Canada; 2011.
Ontario Health Quality Council. QMonitor: 2009 report on Ontario’s health system. Toronto, Ontario; 2009. Available from: http://www.ohqc.ca/pdfs/ohqc_2009_report_-_english.pdf.
Kappel Ramji Consulting Group. Citizenship and immigration Canada Ontario region: client support services for government assisted refugees. Evaluation of province—wide pilot initiative: final report. Don Mills, Ontario; 2009.
Patil CL, Maripuu T, Hadley C, Sellen DW. Identifying gaps in health research among refugees resettled in Canada. Int Migr. 2012. doi:10.1111/j.1468-2435.2011.00722.x.
Feldman R. Primary health care for refugees and asylum seekers: a review of the literature and a framework for services. Public Health [Internet]. 2006;120(9):809–16. Available from: http://www.sciencedirect.com/science/article/B73H6-4KHC3BS-4/2/0313d33d11d6737999f622904fa545cb.
Suter E, Oelke ND, Adair CE, Armitage GD. Ten key principles for successful health systems integration. Healthcare Q. 2009;13(sp):16–23.
Habib RR, Basma SH, Yeretzian JS. Harboring illnesses: On the association between disease and living conditions in a Palestinian refugee camp in Lebanon. Int J Environ Health Res [Internet]. 2006;16(2):99–111. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1817669&tool=pmcentrez&rendertype=abstract.
Health Quality Ontario. Quality monitor: 2012 report on Ontario’s health system. Toronto, Ontario: Queen's Printer for Ontario; 2012.
Manderson B, McMurray J, Piraino E, Stolee P. System navigation roles to support chronically ill older adults through health care transitions: a review of the literature. Health Soc Care Commun. 2011;20(2):113–27.
Kay M, Jackson C, Nicholson C. Refugee health: a new model for delivering primary health care. Australian Journal of Primary Health [Internet]. 2010;16(1):98–103. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21133306.
Balachandra SK, Carroll JK, Fogarty CT, Finigan EG. Family-centred maternity care for deaf refugees: the patient-centered medical home in action. Fam Syst Health. 2009;27(4):362–7.
Grigg-Saito D, Toof R, Silka L, Liang S, Sou L, Najarian L, et al. Long-term development of a “whole community” best practice model to address health disparities in the Cambodian refugee and immigrant community of Lowell, Massachusetts. Am J Public Health. 2010;100(11):2026–9.
Arya N, McMurray J, Rashid M. Enter at your own risk: government changes to comprehensive care for newly arrived Canadian refugees. Can Med Assoc J. 2012;184(17):1875–6.
Acknowledgments
This research study was supported by the Social Sciences and Humanities Research Council of Canada through a Grant from the Centre of Excellence for Research on Immigration and Settlement (CERIS). Researcher Katherine Breward served on the Board of Directors of Reception House Waterloo during the time period under study. Neil Arya is the lead physician at the health clinic described and PI for the CERIS Grant. These relationships were fully disclosed during the ethics review process. The authors are not aware of any other competing interests. They would like to thank the staff and clients of Reception House and the Centre for Family Medicine in Kitchener.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McMurray, J., Breward, K., Breward, M. et al. Integrated Primary Care Improves Access to Healthcare for Newly Arrived Refugees in Canada. J Immigrant Minority Health 16, 576–585 (2014). https://doi.org/10.1007/s10903-013-9954-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10903-013-9954-x