
Abstract
Understanding the concepts of mental health and help seeking behaviours of migrant and ethnic minority families constitutes an important step toward improving the intercultural competence of health and education professionals. This paper addresses these goals among ethnic and migrant minorities in Portugal. For this a multi-informant approach was selected. The study involved nine focus groups (N = 39) conducted with different samples: young immigrants (12–17 years), immigrant parents, teachers and health professionals. The results showed similarities and differences in concepts of mental health, as well as help seeking processes. Stigma continued to be recognized as a barrier in the access to mental health care. The paper argues that providing adequate training on mental health on cultural diversity competencies to health and education professionals can contribute to a better inter-communication and -relation system in the family-school-primary care triangle and thus facilitate access to mental health care for youth.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Public mental health has recently become an international research priority due to the increased risk of poor mental health [38]. According to the World Health Organization [39], depression will be the second highest cause of death in the world in 10 years’ time. Based on a survey addressing existing policy decisions, using international datasets and expert opinions in this area, Shatkin and Belfer [33] concluded that there are few global policy guidelines supporting mental health, particularly that of children and young people. Guidelines for services, research, professional training and children’s education would contribute to the expansion of service systems, the institutionalization of culturally relevant datasets and funding. Fifty two European countries signed a declaration and action plan for mental health at the Helsinki Conference in January 2005. Each country pledged to make mental health, and in particular that of children and young people, a top priority in their country.
Access to Child and Adolescent Mental Health
International findings confirm that about one fifth of children and adolescents in industrialized countries suffer from mental distress [34]. The disorders of a quarter of these are sufficiently severe to warrant psychiatric treatment [35]. However, studies in Europe and the US reveal that most of these children are not being properly diagnosed or treated [4, 14, 40]. Epidemiological studies have demonstrated that only a small number of vulnerable children and young people benefit from relevant and timely health care, even in countries where the health care system is good. This may negatively impact their development into adulthood [15].
Accessing mental health care services is more difficult for migrant and ethnic minorities as they must overcome a range of barriers, at multiple levels [1, 2, 7, 28]. Once accessed, the care they receive is often of a lower quality [2]. This situation must be changed, notably because children and adolescents from migrant and ethnic minorities are exposed to risk factors such as acculturation stress, prejudice and discrimination which make them more vulnerable to mental health problems (e.g. [41]).
According to Carta et al. [5], epidemiological studies on the mental health of migrants in Europe are limited. Instead, there are a number of descriptive studies with convenience samples, and a few clinical trials based on small samples that do not relate to all European countries. They therefore believe there is a need for additional psychosocial studies on the mental health of migrants so that factors which increase the risk of psychiatric disorders and affect the demand for psychiatric care can be identified [5]. The potential barriers facing migrants when accessing mental health care can be divided into objective and subjective barriers and include administrative obstacles, fears, lack of information about health care, language problems and stigma. Objective barriers relate to the structure of health care, available treatments and information. Subjective barriers are related to the patients themselves, the people who serve them, or those planning health care decisions. Carta et al. [5] believe that it would be beneficial to integrate migrants in a network of psychiatric care.
Very few studies have examined barriers to children’s access to mental health care in particular. The study by Owens et al. [27] on parents’ perceptions of the barriers to mental health care distinguished various types of barrier. On the one hand, there were external structural constraints including the lack of providers, long waiting lists, insufficient or lack of insurance coverage, inability to pay for services, transportation problems, and services described as uncomfortable. On the other hand, there were barriers related to differences in perceptions of mental health and illness; these included the difficulties of parents, teachers and primary care providers in identifying children’s needs for mental health care, and even the denial of the seriousness of mental health problems and the belief that the problem can be resolved without treatment. Finally, some barriers were related to the perception of services: lack of trust in providers or previous negative experiences with them, the child’s reluctance to seek help, and associated stigma. In order to identify all barriers, Owens et al. [27] argue researchers should not only consult those who have experienced accessing mental health care but also the general population because, for example, the parents’ inability to identify the need for psychosocial support may already represent a major barrier. Researchers and policy makers interested in improving children’s access to mental health care need to reduce the barriers associated with how care is perceived. Furthermore, intervention programs should take into account the way children’s psychosocial problems affect families’ needs.
This was the approach taken in the Swiss Study AMHC—Access to Mental Health Care in Children [8, 10, 11, 16], which is now being replicated in Brazil and Portugal. The aim of the AMHC study was to understand how children, adolescents and parents perceive their mental health and to what extent they consider personal and/or family difficulties as mental dysfunctions/disorders. A second aim was to determine the factors associated with failure to use preventive services and treatment options in the field of child and adolescent mental health. The AMHC study sought to examine the individual, family and social influences on trans-generationally transmitted mental health concepts and thresholds in the use of help, and also involved migrant and ethnic minorities in Switzerland. This study concluded that mental health concepts and action strategies of parents are more similar to each other, than to those of their children. Parents usually advise their children to speak about their problems with others, whereas the latter prefer to adopt other strategies (such as distracting themselves e.g. watching TV). According to this study, teachers and primary care providers can be facilitators in migrant and ethnic minority families’ access to mental health care; however, they require more training and information about both mental health and migration.
Portuguese Context: Mental Health of Children and Adolescent of Migrant and Ethnic Minorities
According to the Report of the National Commission of Mental Health Services Reform in Portugal [30], no epidemiological study on children’s mental health has yet been conducted in the country. Moreover, the geographic and professional diversity of child and adolescent mental health care is insufficient. The report clearly stated: “The multidisciplinarity of services/units envisaged by the law 35/99 is not present in many of the services currently available. The interventions directed toward mental health promotion are scarce and internationally validated prevention programs are almost nonexistent” (p. 45).
According to the United Nations, the number of immigrants around the world has doubled since 1975 and more than 30% live in Europe [31]. European societies are characterized by an increasing number of immigrants, and in several European countries around one third of adolescents have a migratory background [25]. Portugal is an interesting country in this respect. There has always been a strong tradition of emigration in part due to its history of maritime discoveries. It is estimated that one third of Portuguese people have emigrated. On the other hand, Portugal is a multicultural country with a social and cultural milieu formed by ethnic and immigrant minorities from different parts of the world with varying linguistic skills, religious affiliations, and cultural backgrounds.
The number of immigrants in Portugal has increased significantly in the last two decades. Recent official reports indicate that there has been a 200% rise in the immigrant population since the 1990s [20], increasing concerns about social integration and the development of new approaches to migrant health. However, it is difficult to give a precise estimate of the number of immigrants as many are undocumented. According to SEF—Portuguese Foreigner and Boarder Service [29], 4.14% of the population living in Portugal are immigrants. These 440 thousand people have different cultures of origin. Brazilians form the largest immigrant group (24.3%), followed by Ukrainians and then Cape-Verdeans, who represent 12.2% (N = 53,494) and 11.7% (N = 51,353) respectively of the immigrant population. Romanians (6.31%; N = 27,769) and Angolans (6.27%; N = 27,619) are in fourth and fifth place with similar percentages. Immigrants from Guinea-Bissau and Moldavia represent 5.54% (N = 24,391) and 3.19% (N = 14,053) respectively of the total. It should be noted that 2.6% of these immigrants are children aged between 0 and 15 years.
Recent legislation has been introduced to guarantee universal access to health care services for immigrants who have been in the country for over 90 days regardless of their legal status (free of charge in the case of children; [20]. However, this legislation alone has proven to be far from sufficient as a means of improving immigrants’ access to health services and promoting migrant-friendly health centers and hospitals. In a study by Moleiro et al. [23], immigrants asked about their experiences and needs in the health care system in Portugal reported instances of discrimination generally, including within the health care system, educational system, work place and every-day life. These findings are consistent with the report by the International Organization for Migration [13]—“Developing a Public Health Workforce to Address Migrant Health Needs in Europe”- which concluded that most health systems do not assure fair, equitable and culturally appropriate treatment for migrants and ethnic minorities.
Main Goal of this Study
Following the referred Swiss AMHC study, the aim of this present project is to shed light on the family-school-primary care triangle and the access to mental health care for migrant and ethnic minority families in Portugal.
Methods
Working from a multiple informant perspective [17, 19], we adopted a focus group methodology (with youth, parents, teachers and primary care providers). This qualitative methodology facilitates the exploration and discussion of complex topics [36]. It is a collective research method that allows for individual expression of opinions and experiences, as well as the collective discussion and emergence of topics [6, 9, 18]. It also lets researchers observe social processes/interactions [21].
Sample
A total of nine focus groups were conducted: three with adolescents aged between 12 and 17 years (attending 6th to 11th grades), two with parents, two with teachers and two with primary care providers (N = 39 participants). Table 1 presents a socio-demographic characterization of the study sample.
Overall, the sample of adolescents was composed of 16 youth, most of whom were male (N = 11). The most represented countries of birth were Cape Verde, Brazil and Angola. The mean age of the adolescents was 14.8 years. Parents participating in this study were all mothers, though fathers’ participation was strongly encouraged. These mothers were mostly in the 35–45 age group and had more than one child. The mothers’ countries of birth varied between Angola, Mozambique, Cape-Verde and Guinea-Bissau. Most teachers were also women and had an average of 17 years’ professional experience. Health professionals, on the other hand, had an average of 15 years’ professional experience.
Instrument
A semi-structured interview protocol was developed, adapted from the Swiss Study AMHC [8, 10, 11, 16, 24]. The actual protocol (Table 2) contemplated topics such as concepts of mental health, action strategies in case of psychological distress, barriers to help seeking behaviors, facilitators in the access to mental health care and the “ideal” intercultural competence of the mental health professionals (e.g. psychologists).
For this study, three versions of the interview protocol were developed, depending on the target: (1) adolescents, (2) parents and (3) professionals—teachers and primary care providers. The interview guide for parents differed only in the question concerning action strategies: “What do you suggest your children do when they feel down?”; and in the one related to facilitators “…help immigrant families to get care from a psychologist?”. The interview protocol for professionals always inquired about their perspective in relation to immigrant adolescents and their families as follows: “What do you think it means to be psychologically well to the immigrant families with whom you work?”.
Procedure
The sample was recruited from 7th to 9th grades in public schools from three areas with moderate to high representation of immigrant families (Sintra, Amadora and Cascais). Immigrant associations, the High Commissioner for Immigration, and the Health Regional Administration were also contacted. Firstly, the project had to be submitted and accepted by the General Directorate of Curriculum Innovation and Development. Informed consent was obtained and volunteer participation was ensured, including that of adolescents and legal guardians, as mandated by international guidelines [3].
The focus groups were transcribed by a non interviewer researcher. The written material was analyzed in terms of content, following the Mayring reduction method [22]. It is an inductive process that allows categories to emerge from the written material. This analysis was conducted separately by two persons independently, who then came together to generate consensus. The categories that emerged were finally compared with the category system created in the Swiss AMHC study [8, 10, 11, 16].
Results
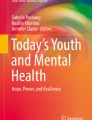
In order to better summarize the topic of access to mental health care in a multi-informant perspective, diagrams (as Fig. 1) were constructed. In this paper, however, most results will be presented in a narrative format; reference will be made to the categories that emerged with some examples from participants per sample group.

Access to mental health among ethnic and migrant families (according to health professionals)
For adolescents, ‘Mental health’ meant well-being (e.g. “to be happy because it helps to calm down and decide things”), interaction/social support (e.g. “to be with the family, with siblings, get family and friends’ support”) or the utilization of a cognitive strategy such as thinking (e.g. “to think about the future”). In case of psychological distress, these adolescents tended to communicate with others (e.g. “try to let things go, speak with friends, especially with parents”), distract themselves (e.g. “try to distract myself with other things, so as not to think about the same thing all the time, such as reading a book, going online, going out, listening to music, eating is always good”), isolate themselves (e.g. “I stay at home”) or use cognitive avoidance (e.g. “I try not to think about the matter, resolve it with time”) or emotional expression (e.g. “to cry”). The people these adolescents contacted in these situations were usually their friends, teachers and parents. In terms of barriers to accessing mental health care, they mentioned reliance on self-support (e.g. “to prefer to resolve one’s own problems in another way”) and preference for informal social support, as well as financial reasons (e.g. “perhaps having no money to pay”). They also reported shyness, shame, fear, stigma (e.g. “friends can say they’re crazy”), language issues, and the denial of the right of choice (e.g. “to be obliged to go”—by parents or teachers). On the other hand, the adolescents mentioned that friends, teachers, parents and primary care providers can serve as facilitators in this process of accessing mental health care. As one participant mentioned: “They [doctors and teachers] should talk with adolescents, try to understand what is going on in their heads, advise them to speak with the family or with a psychologist”. For the young participants, the psychologist’s intercultural competences included knowledge about the patient’s language (e.g. “they can learn a few words in order to understand each other better”), traditions and habits (e.g. “to learn about traditional dishes in order to speak a bit about what the patient likes”), preferences (e.g. “to find something they like and to work from there, for example the person likes to read and the psychologist could bring books or similar things to attract the person more”), family and problems (e.g. “to ask how the family is, if they have something in mind that is disturbing”), ways of life, personality and education (e.g. “the way of life, the education parents give, influences since childhood”), and integration process (e.g. “how they are getting used to being here”).
For the mothers who participated in these focus groups, ‘mental health’ was a synonym for socio-economic well-being (e.g. “to be good in life, at home, at work”), good communication in the family (e.g. “to be good in the family, everyone understanding each other, to sit down at the dinner table, to discuss what happened during the day”), and correct social behavior (e.g. “who behaves well, does things within law, knows what to do”). Mental illness meant having a chronic disease or something associated with financial problems. As one mother mentioned: “A person who does not feel well, never thinks he/she needs help from a psychologist; they’d rather admit that it is just a monetary problem”. If their children had a problem, mothers suggested they should talk about it when they feel down (e.g. “when I see my child feeling down, I ask what happened. If they say nothing, I respect it, but then I give my opinion”). Mothers thought in these situations that their children seek help from teachers and the parents themselves. These mothers emphasized reliance on self-support as a barrier to accessing mental health care (e.g. “they can keep it only to themselves, and not speak with a doctor or anyone else”); they also referred to financial reasons, language difficulties, stigma (e.g. “people think others are crazy when they go to the psychologist”), different ways of thinking (e.g. “people’s mentality”), and legal questions such as “not having documents”. Teachers and primary care providers could serve as facilitators in the access to mental health care, according to these mothers (e.g. “Teachers spend more time with children, don’t they? So they should notice how children are…”). In their opinion, intercultural competence of the psychologist was related to knowledge about the patient’s life history, in what way the school and the primary care providers could help (e.g. “all schools should have full time psychologists”), and in the knowledge of aspects such as beliefs, values, and characteristics of the patient’s culture of origin.
According to the teachers participating in these focus groups, mental health meant social integration (e.g. “it means inclusion, because even going through difficulties, if they know they are included, it seems they are well psychologically”) and family reunion (e.g. “the problem is that many come and stay with their family, others come with the mother and the father stays back, or they come only with their siblings to live with uncles and aunts”). On the other hand, their perception was that mental illness was a synonym for aggressive behavior for these immigrant families. One emphasized: “When we are talking to a 12 year old about being happy at school, and having good friends and a cordial relationship with teachers, it is enough. For parents, it is much more than that, it is to ensure the day-to-day care, it is to ensure food on the table, it is to ensure the home, employment, education, and then to integrate themselves.”. Teachers argued that immigrant families value communication (e.g. “they come to us to vent their feelings”), distraction (e.g. “sports and cultural events; dancing is very present here at school”), isolation and emotional expression. They also suggest that some adolescents tend to use leadership within the peer group as a strategy to deal with psychological distress. Teachers perceived themselves as contact persons for immigrant adolescents in situations of psychological distress as they spend a significant amount of time with them each day. Teachers made reference to the following barriers to accessing mental health care among immigrant families: non-recognition of the problem (e.g. “We are often told: my child does not need it so he will not go”), financial hardship, legal reasons, limited timetables (e.g. “conflict scheduling”) and localization outside the community, duration of the treatment, and stigma (e.g. “I often hear: I am not crazy, I am not different from the others, so I do not need to go”). On the other hand, these teachers considered themselves facilitators of the process along with the primary care providers. Teachers considered that intercultural competence of the psychologist implies knowledge about the specific family dynamics and clinical and individual history of the immigrant adolescent (e.g. “how he got here, his trajectory, the experience so far, this is important especially to help uncover something that we might miss”). They emphasized that this competence should be included in teacher training (e.g. “more psychologists in schools, and we should have specific training, I think, on how to manage this, training sessions for teachers would be very important, especially on how to deal with problematic cases. We need all this support at a psychological level, to be able to consult with other professionals”). They also highlighted the importance of creating multidisciplinary teams (e.g. “there is a need for teams, teams of various professionals, psychologists, social workers,…they must be multidisciplinary teams”).
Primary care providers who participated in this study indicated that the concept of mental health of immigrant families in Portugal is associated with their socio-economic well-being (e.g. “mental well-being is having work, housing, education, and health”). They also perceived that social interaction was an important aspect (e.g. “it is the question of interaction within the family, among people from the same ethnic group and neighborhood; having that capacity to interact regularly”). Finally, reference was also made to their performance as parents and their social integration as part of well-being. However, they also mentioned that mental health is still a taboo (e.g. “mental health for immigrants is still taboo, problems that they do not recognize yet and that some recognize but try to hide”). These professionals perceived severe mental illness as often being related to the absolute lack of social integration of immigrant families (e.g. “the absence of work, being totally obliged to live in the margins of society”). According to primary care providers, the main action strategies of immigrant families in the case of psychological distress were either isolation (e.g. “they hide themselves, self-protect themselves”) or reliance on natural social support (e.g. “family resources, so use of family support and, of community support somewhat”). In this situation, primary care providers considered themselves as the immigrant families’ main contact in Portugal. These primary care providers believed the following were barriers to accessing mental health care for immigrant families: the non-recognition of the problem (e.g. “when parents realize that the problem can be psychological, they usually associate it with not developing at school”), the duration and location of the therapies, lack of trust and fear. They also referred to the complex structure of the health care system, financial issues and stigma.
As facilitators of access to mental health care, these primary care providers did not mention individual people or professional categories, but rather the network between the family, the educational and health systems, and the community. In their opinion, this interaction between systems could help immigrant families in Portugal access mental health care. One mentioned: “Schools go to the health centre every month, they bring their problems, and after referral, a group of psychologists, social workers, sociologists, a whole network, a type of social network that works in this area: school, health centre, community, and child psychiatry service.” Another emphasized: “People in the community, from the area of primary health or even from the religious community, cultural associations, can serve as facilitators because they know that community and that family; they work with them, they know what it means for them to have to go to services, to use the services. So proximity and dialogue is a big step towards that”.
In relation to the psychologist’s intercultural competences, these primary care providers referred to the ability to develop a trusting relationship and emphasized the importance of multicultural teams (e.g. “There are several strategies, one of which is to contact, for example to enable professionals from other countries to join teams”) and multidisciplinary teams (e.g. “I strongly believe that multidisciplinary teams have great potential, at a local level, to work on all health aspects, not only mental health; [they] should be integrated with other health services at the primary care level, through multidisciplinary teams within the community, especially for specific groups at risk”) and of cultural medicine.
Discussion
The present study sought to contribute to the understanding of mental health concepts and help-seeking behaviors of migrant and ethnic minority families in Portugal. Our results showed that there are similarities and differences not only in the concepts of mental health held by the involved agents (adolescents, parents, teachers, health professionals), but also in the help-seeking strategies. For children, mental health means an overall well-being, interaction/social support and thinking/cognitive regulation strategies. For mothers, it means socio-economic well-being, communication in the family and appropriate social behavior. These results are consistent with those found among immigrant families in Switzerland. Portuguese immigrant parents in Switzerland also mentioned correct social behavior as a synonym for mental health [10, 11]. The absence of aggressive behavior appeared to be important to this adequate social behavior. However, “not taking drugs” was not discussed explicitly in the Portuguese study as it was in Switzerland [10, 11, 24]. In the present Portuguese study, both teachers and primary care providers mentioned social integration as a synonym of mental health for these families, although primary care providers emphasized that mental health is still a taboo for some of these families. In case of psychological distress, these adolescents tended to communicate with others, distract themselves, isolate themselves or use cognitive avoidance or emotional expression. On the other hand, mothers suggested their children should talk about their problems when they feel down. This differs from the results of the Swiss AMHC study where children made no mention of speaking to others as an action strategy [10, 11, 24]. This as well as other distinctions already mentioned may be due to differences between the studies (sample sizes, methodologies), but it may also reflect different cultural contexts.
One interesting result is the fact that parents did not mention their children’s friends as people to contact in case of mental distress. A similar conclusion was found in the Swiss AMHC study where parents believed that adolescents accessed their mother first when in psychological distress, while adolescents themselves referred to friends as the initial source of support [10, 11, 24]. Parents seem to be unaware of the influence of the peer group as their children’s primary social support even though it is in fact expected to be an important source of social support in adolescence [12, 32].
Regarding the experienced or perceived barriers to the access of care, overall stigma continues to be recognized as a barrier in access to mental health care for immigrants, consistent with findings of AMHC Switzerland [10, 11, 24]. Both teachers and primary care providers mentioned the non-recognition of the problem as one of the main obstacles to these families accessing mental health care. Both children and mothers mentioned the reliance on self-support, financial difficulties, language differences and stigma as barriers. Children added the reliance on informal social support, shyness, shame, fear and the right to choose; mothers included differences in the way of thinking and legal conditions. Children and parents did not identify the duration of therapy as an obstacle, as teachers and primary care providers suggested. Both professional groups considered themselves as the main contact for these families. It is also interesting to note that primary care providers consider the family-school-primary care triangle as one of the main facilitators of the access to mental health care, consistent with findings of AMHC Switzerland [10, 11, 24]. Concerning intercultural competence, it is interesting that both teachers and primary care providers mentioned the role of multidisciplinary teams.
These finding are also in line with those of the Owens et al. [27] study on parents’ perceptions of the barriers to mental health care which also involved concepts of mental health and illness, action strategies, facilitators and a multi-informant perspective. Moreover, these studies illustrate the wealth of data that can be drawn from client-oriented research, supporting other authors who advocate that the migrant population is a valuable information source [8, 10, 11, 16, 23, 24].
It is also clear from these findings that legislation changes are not in themselves sufficient to improve access to health care and promote quality of service. In Portugal, youth, families, and professionals in the field all identify a significant number of difficulties despite considerable changes made in the last decade to extend universal access of health care to immigrants [20]. Moreover, differences in perceptions between teachers and health care providers on the one hand, and migrants on the other, highlight the need to give professionals further specialized training in cultural diversity competencies in order to effectively break down the barriers to service. This is in line with the recommendations of the International Organization for Migration [13], which emphasizes the need to improve the quality of professionals in the health system. While the literature in social sciences has clearly debated and argued for training on cultural diversity competencies since the 1990s (see [37], increased awareness of the need for specific training in health (e.g. EuroMed Network on Migration and Mental Health) and education (see [26] is only recent. Promoting these competencies, both at an individual (teachers, clinicians) and an organizational level (schools, health centers), while involving the migrant communities as informants and collaborators in the development of services, may be pivotal to facilitating the decrease of both structural and perceived barriers to accessing mental health care.
Despite this study’s contribution to understanding mental health concepts and help seeking behaviors of migrant and ethnic minority families in Portugal from a multi-informant perspective, the following limitations must be recognized.
Firstly, the sample is small and its representativeness is not assured. This was a qualitative and exploratory study of the Portuguese territory. The instruments used had already been tested in previous research. The main objective was to provide a multi-informant approach to the topic. It is also important to take the link with previous research in Switzerland and with current work being done in Portugal and Brazil into consideration. Secondly, the parental sample has limited variability. Although the participation of fathers was greatly encouraged, we recognize that the research team’s time constraints influenced the situation and only mothers ended up participating. Thirdly, the group discussion format is a unique methodology which was selected from experience and previous work in Switzerland. Yet again, we consider this decision important to the research process involving previous and actual studies in Switzerland, Brazil and Portugal.
Nevertheless, it should be stressed that an improved understanding of concepts and requirements for immigrant children and youth mental health as well as knowledge of current interventions involving the family-school-primary care triangle will lead to a better match between needs and supply. Future studies could explore these concepts and action strategies in larger samples, including Portuguese samples. The surveying of 500 children and 100 parents as part of the ongoing AMHC study in Portugal is essential so that data can be compared with that of Swiss AMHC study and the ongoing AMHC study in Brazil.
References
Abe-Kim J, Takeuchi D, Hong S, Zane N, Sue S, Spencer M, Appel H, Nicdao E, Alegria M. Use of mental health related services among immigrants and US born Asian Americans: results from the National Latino and Asian American Study. Am J Public Health. 2007;97(1):91–8.
Alegría M, Canino G, Pescosolido B. A socio-cultural framework for mental health and substance abuse service disparities. In: Sadock BJ, Sadock VA, Ruiz P, editors. Comprehensive textbook of psychiatry. Baltimore: Wolters Kluwer Health, Lippincott Williams & Wilkins; 2009. p. 4370–4379.
American Psychological Association. Ethical principles of psychologists and code of conduct. Washington, DC: American Psychological Association; 2002.
Burns BJ, Costello EJ, Angold A, Tweed D, Stangl D, Farmer EM, Erkanli A. Data watch. Children’s mental health service use across service sectors. Health Aff. 1995;14(3):147–59.
Carta MG, Bernal M, Hardoy MC, Haro-Abad JM. Migration and mental health in Europe. Clin Pract Epidemiol Mental Health. 2005;1(13).
Castellblanch R, Abrahamson DJ. What focus groups suggest about mental health parity policymaking. Prof Psychol Res Prac. 2003;34(5):540–7.
Fortuna L, Porche M, Alegria M. Political violence, psychosocial trauma, and the context of mental health services use among immigrant Latinos in the United States. Ethnicity Health. 2008;13(5):435–63.
Gianella D, Gonçalves M, Höfler S, Inglin S, Borges M, Käppler C, Mohler B. Access to mental health care in children: the AMHC—study. Concepts of mental health and perception of services from the perspective of children, adolescents and their families: In: Rubinelli S, Haes J, editors. Tailoring health messages. Bridging the gap between social and humanistic perspectives on health communication. Proceedings of the international conference. Lugano: Università della Svizzera italiana; 2005: p. 95–100.
Glaser BG, Strauss A. The discovery of grounded theory. New York: Aldine De Gruyter; 1967.
Gonçalves M. Der Zugang von Migrantenkindern zur psychischen Gesundheitsversorgung. Eine Untersuchung mit portugiesisch-sprachigen Familien im multikulturellen Umfeld der Schweiz. Hamburg: Verlag Dr. Kovac; 2009.
Gonçalves M, Käppler C. The access to mental health care in children: Portuguese speaking families living in a multicultural context in Europe. Interam J Psychol. 2010;44(3):411–20.
Helsen M, Vollebergh W, Meeus W. Social support from parents and friends and emotional problems in adolescence. J Youth Adolesc. 2000;29:319–35.
International Organization for Migration. Developing a public health workforce to address migrant health needs in Europe. http://www.migrant-health-europe.org/files/Capacity%20Building%20in%20Healthcare_Background%20Paper(2).pdf, 2009.
John LH, Offord DR, Boyle MH, Racine YA. Factors predicting use of mental health and social services by children 6–16 years old: findings from the Ontario Health Study. Am J Orthopsych. 1995;65:76–86.
Jones PB, Bebbington P, Foerster A, Lewis SW, Murray RN, Russek A, Sham PC, Toone BK, Wilkins S. Premorbid social underachievement in schizophrenia: results from the Camberwell collaborative psychosis study. Br J Psych. 1993;162:65–71.
Käppler C, Mohler-Kuo M, Gonçalves M, Gianella D, Peng A, Zehner S, Anastasi B, Nussbaumer D. Psychische Gesundheit und Zugang zu Professioneller Hilfe: Wie denken Kinder, Jugendliche und ihre Eltern? Themenheft des NFP52: Antisoziales Verhalten bei Kindern, Psychosoziale Risiken von Jugendlichen: Was bringt Prävention und Beratung? 2006: p. 18–21.
Kraemer HC, Measelle JR, Ablow JC, Essex MJ, Boyce WT, Kupfer DJ. A new approach to integrating data from multiple informants in psychiatric assessment and research: mixing and matching contexts and perspectives. Am J Psych. 2003;160:1566–77.
Krüger RA. Focus groups. 2nd ed. USA: Sage; 1994.
Kuo M, Mohler B, Raudenbush SL, Earls FJ. Assessing exposure to violence using multiple informants: application of hierarchical linear model. J Psychol Psych. 2000;41(8):1049–56.
Machado MC, Pereira F, Machaqueiro S. Approaches to migrant health in Portugal. Eurohealth. 2010;16(1):30–1.
Madriz E. Focus groups in feminist research. In: Denzin NK, Lincoln YS, editors. Handbook of qualitative research. 2nd ed. USA: Sage; 2000. p. 835–50.
Mayring P. Qualitative Inhaltsanalyse: Grundlagen und Techniken (7. Aufl.). Weinheim: Dt. Studien-Verlag; 2000.
Moleiro C, Silva A, Rodrigues R, Borges V. Health and mental health needs and experiences of minority clients in Portugal. Int J Migration Health Social Care. 2009;5(1):15–24.
Moleiro C, Goncalves M. Saúde na Diversidade: Desenvolvimento de serviços de saúde mental sensíveis à cultura. Análise Psicológica. 2010;28(3):505–15.
Ocak-Schouler M, Haasen C, Heinz A. Migration and transcultural psychiatry in Europe. Euro Psych. 2008;23:1–3.
Organization for Economic Co-Operation and Development. Educating teachers for diversity: meeting the challenge. OECD Publishing; 2010.
Owens PL, Hoagwood K, Horwitz SM, Leaf PJ, Poduska JM, Kellam SG, Ialongo NS. Barriers to children’s mental health services. J Am Acad Child Adolesc Psychiatry. 2002;41(6):731–8.
Pierce CD, Reid R. Attention deficit hyperactivity disorder: assessment and treatment of children from culturally different groups. Semin Speech Lang. 2004;25(3):233–40.
Portuguese Service of Foreigners and Boarders. http://www.sef.pt/portal/v10/PT/aspx/estatisticas/relatorios.aspx?id_linha=4265&menu_position=4141#0; 2009.
Report of National Commission of Mental Health Services Restructuration in Portugal; 2007.
United Nations. Number of world’s migrants reaches 175 million. http://www.un.org/News/Press/docs/2002/pop844.doc.htm; 2002.
Scholte RHJ, van Lieshout CFM, van Aken MAG. Perceived relational support in adolescence: dimensions, configurations, and adolescent adjustment. J Res Adolesc. 2001;11:71–94.
Shatkin JP, Belfer ML. The global absence of child and adolescent mental health policy. Child Adolesc Mental Health. 2004;9(3):104–8.
Steinhausen HC, Winkler-Metzke C. Seelische Gesundheit und psychische Probleme im Jugendalter: Verbreitung und Bedingungsfaktoren: In: Institut für Sozial- und Präventivmedizin der Universität Zürich, editors. Die Gesundheit Jugendlicher im Kanton Zürich. Serie Gesundheit, Gesundheitsförderung und Gesundheitswesen im Kanton Zürich, im Auftrag der Gesundheitsdirektion Zürich; 2002: p. 51–60.
Stephenson J. Children with mental problems not getting the care they need. JAMA. 2000;284(16):2043–4.
Stewart DW, Shamdasani PN, Rook DW. Focus groups: theory and practice. 2nd ed. Thousand Oaks, CA: Sage; 2007.
Sue DW, Arredondo P, McDavis RJ. Multicultural counseling competencies and standards: a call to the profession. J Couns Dev. 1992;70(4):477–86.
Twenge JM. The age of anxiety? The birth cohort change in anxiety and neuroticism, 1952–1993. J Pers Soc Psychol. 2000;79(6):1007–21.
World Health Organization. Depression. http://www.who.int/mental_health/management/depression/definition/en/; 2010.
Wittchen HU. Epidemiological research in mental disorders: lessons for the next decade of research—the NAPE lecture 1999. Acta Psychiatr Scand. 2000;101(1):2–10.
Yeh C, Pituc S, Atkins M, Kim A. Poverty, loss and resilience: the story of Chinese immigrant youth. J Couns Psychol. 2008;55(1):34–48.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gonçalves, M., Moleiro, C. The Family-School-Primary Care Triangle and the Access to Mental Health Care Among Migrant and Ethnic Minorities. J Immigrant Minority Health 14, 682–690 (2012). https://doi.org/10.1007/s10903-011-9527-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10903-011-9527-9