
Abstract
The purpose of this study was to compare the body composition and cardiorespiratory fitness levels of a sample of refugee Somali women living in New Zealand with normative data. Refugee Somali women were invited to participate in sessions to assess physical fitness and body measurements. Height, bodyweight and waist and hip circumference were measured. The Rockport Fitness Walk Test was used to estimate the women’s cardiorespiratory fitness levels. Thirty-one women between 12 and 66 years old participated in this study. There was a significantly greater proportion (71.4%) of participants with a BMI in the overweight or obese range (≥25 kg/m2) compared to normative New Zealand women’s data (49.3%; p = 0.015). The proportion of Somali women (42%) with a waist-to-hip ratio in excess of 0.8 was higher than that of New Zealand women (35.6%), but not statistically so. All women over 30 years of age (n = 12) had an estimated VO2max below the 50th percentile with eight participants below the 10th percentile. The extent of overweight and obesity and low fitness levels, particularly among the older Somali women in this study, suggests that Somali women are at increased risk of developing lifestyle related diseases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In the last 20 years, Australia and New Zealand have been host to nearly 300,000 refugees [1]. In 2001 alone, Australia accepted 6,450 refugees [2] and nearly 1,000 refugees were resettled in New Zealand [3]. Refugees from Somalia make the 6th largest group in the world and in 2001 they were the 2nd largest group coming into New Zealand [1, 3]. Somalis have been coming to New Zealand as refugees since 1993 [4, 5] and their total population in New Zealand is estimated at around 4,000 [6, 7].
Somalia comprises a majority nomadic culture with low education levels and literacy, particularly among older men and women. However, education is a high priority for Somali families, sometimes resulting in parents taking extreme measures to get appropriate education for their children [8]. With no central government for many years and a non-consumer-oriented economy, Somali life and culture are very different to that in New Zealand [9, 10]. Somali are a particularly interesting group to study because of the many issues that make many Somali very different to typical ‘westerners’ including differences in religion, skin color, education and literacy and culture in general. Nearly all Somali are Muslims, practicing the religion of Islam, so most women dress in ways that sets them apart from most New Zealanders. This, combined with their black skin, makes the women particularly visible in New Zealand communities.
Research has found that Somali women, in particular, are likely to spend much of their time at home, to engage in little physical activity, and to have a high prevalence of reported sedentary behavior [11, 12]. No research has examined the physical characteristics of Somali women refugees and the implications of these for health. However, research has found that female Bosnian refugees had higher body mass index (BMI) and other cardiovascular disease (CVD) risk factors compared to Swedish women [13]. CVD risk factors include high cholesterol, smoking, diabetes mellitus, obesity and sedentary lifestyle [14].
Regular physical activity has both short- and long-term benefits that are well documented [15, 16]. For example, some of the long-term benefits are that physical activity increases longevity and decreases risk of heart disease, diabetes, high blood pressure, obesity and development of some cancers [17–20]. Short-term benefits of regular physical activity include increased energy, improved sleeping, and stronger heart, muscles, bones and joints [20]. Physical activity also has mental health benefits, such as decreasing depression, anxiety and reducing stress [21–23]. Considering that many Somali women have had difficult lives (e.g., experienced trauma during war) and have had extreme changes in lifestyle, it is important to determine physical and fitness characteristics of this group and the implications of that for physical activity and inactivity and health in general.
Improvement of access to appropriate nutrition information and physical activity opportunities is essential to prevent the development of body weight and lifestyle-related health risks. Language barriers and cultural and religious issues, as described by others [12], need to be considered both in the assessment of these issues as well as in the provision of treatment and information. For example, Somali women usually will prefer to have their height, weight and other body measurements taken by a woman. Pamphlets describing nutrition and physical activity information are not usually helpful in the case of older women who do not speak English and often do not even read or write in their own language [11, 12].
The present study sought to examine, for the first time, lifestyle disease risk of a sample of Somali women living in New Zealand by taking a variety of measurements and comparing these to extant normative data.
Methods
Study Population
A convenience sample of a total of 31 women, who identified as Somali, between the ages of 12 and 66 (M = 34, SD = 17.2) participated in this study between March and November 2001. Census data indicated that 240 Somali women (492 total Somali) were living in the Waikato region in March 2001 and that approximately 160 of them would have been in the age range 12–66 years [6, 7]. Community networks such as radio and word of mouth were used to inform the women about the research. A female community leader (the second author) phoned many women in the community to inform them about the research and invite them to participate. Women were provided transportation if necessary and food and drink were available. Both formal and informal interpreting was provided during the sessions. All interpreters were financially compensated for their assistance.
Procedure
Physical Measurements
BMI was used as a measure to determine overweight and obesity using the equation BMI = weight in kg/height in m2. Weight was measured while wearing clothing and no shoes using electronic scales to the nearest 0.1 kg. Height was measured to the nearest cm with shoes off.
The measurement of body fat distribution in the abdominal area by calculating the waist-to-hip circumference ratio (WHR) is a way to determine CVD risk [18, 23, 24]. The WHR is also considered a more appropriate indicator of risk for ethnic groups [25]. The circumference of waist and hips were measured to the nearest 0.5 cm using a soft tape measure. These values were also compared to data for New Zealand women [24].
As the study was conducted in New Zealand (NZ), New Zealand normative data for physical measurements were used for comparisons and were obtained from NZ Food: NZ People. Key results of the 1997 National Nutrition Survey [24]. There are no anthropometric data, nationally or internationally, for Somali or Somali women in particular. In the NZ Food: NZ People report, data were provided for NZ Maori, Pacific people, and all other New Zealanders, which includes European, Asian and others. In the NZ Food: NZ People report, ‘overweight’ was defined as the percentage of NZ Maori and Pacific people with 26.0 kg/m2 ≤ BMI < 32.0 kg/m2, and NZ European, and others with 25.0 kg/m2 ≤ BMI < 30.0 kg/m2. Also, ‘obese’ was defined as the percentage of NZ Maori and Pacific people with BMI ≥ 32.0 kg/m2, NZ European and others with BMI ≥ 30.0 kg/m2 [26]. As Somali are a new group to New Zealand, there are no data to indicate which group, NZ Maori, Pacific, or all other New Zealanders is most appropriate to compare Somali data. However, a study in Minnesota found that Somali women’s bone density fell between that of African women and white women [27]. Therefore, for this study, we used the criteria for ‘NZ European and others’ for Somali women as well.
Rockport Walk Test
Cardiovascular fitness was estimated using the Rockport Fitness and Walk Test (RFWT; 28, 29) and those values were compared to available normative data [23, 28]. Research has shown that the RFWT is appropriate for older women [29]. The RFWT was determined to be the best method of assessing physical fitness among the women because walking is an activity that they could perform with easy instructions. For the RFWT, the women were instructed to walk 1 mile as quickly as possible without running [28]. Verbal encouragement in both Somali and English was provided to participants during the test. The RFWT was performed at two different indoor locations (a fitness center and a sport hall) and one outdoor location (a sport stadium). Researchers manually obtained heart rates for 15 s immediately upon completion of the walks. Reliability retests were completed for seven subjects. An estimated VO2max was calculated using the following equation [30]:
The difference between two percentages was calculated using Statistica software. All other analyses were performed using SPSS software.
Normative data for the fitness test were obtained from the American College of Sports Medicine book ACSM’s Guidelines for Exercise Testing and Prescription [28] and the U.S. Department of Health and Human Services Physical Activity & Health: A Report of the Surgeon General [23].
Ethics
This research was approved by the Waikato Institute of Technology Ethics Committee. The purpose of the research was explained in Somali to the women, individually, and consent was obtained verbally. Women were advised that they could refuse to participate or stop participating at any time without any loss of benefit to them. Because many of the women did not read written Somali, this was found to be the best method of informing the women about the purpose of the study and gaining their consent to participate [4, 12].
Results and Discussion
Important differences were found between Somali and New Zealand women in weight, BMI and excess WHR. BMI (kg/m2) was calculated for 28 Somali women (Table 1). BMI was not calculated for three participants due to missing height values. The New Zealand criteria for ‘overweight’ and ‘obese’ are slightly higher for NZ Maori and Pacific people than for ‘NZ European and others’. Table 1 shows mean and standard deviations as well as the percentage of women falling within the BMI values. ‘Overweight’ was defined as the percentage of NZ Maori and Pacific people with 26.0 kg/m2 ≤ BMI < 32.0 kg/m2, and NZ European and others with 25.0 kg/m2 ≤ BMI < 30.0 kg/m2. ‘Obese’ was defined as the percentage of NZ Maori and Pacific people with BMI ≥ 32.0 kg/m2, NZ European and others with BMI ≥ 30.0 kg/m2 [24, 31]. The mean BMI for the Somali women was 27.8 kg/m2 (range = 18.3–38.3 kg/m2), which approached significance compared to New Zealand women (26.1 kg/m2; p = 0.08). The percentage of women with a BMI in the overweight range was slightly greater for Somali women (35.7%) compared to New Zealand women (30.1%) but was not significant (p = 0.46). In the obese range, there was a significantly greater proportion of Somali women (35.7%) compared with New Zealand women (19.2%; p = 0.01). Combining overweight and obese proportions further illuminates this important difference with 71.4% (20/28) of the Somali women in the overweight or obese range compared with only 49.3% of the New Zealand women (p = 0.01).
The WHR is a measure of central obesity. For women, a WHR greater than 0.8 indicates increased risk of CVD and diabetes [23]. While the mean WHR was similar between Somali and New Zealand women (0.79 and 0.78, respectively), there was a slightly higher proportion of Somali women (42%) with a waist to hip ratio in excess of 0.8 compared to New Zealand women (35.6%), but this difference was not significant (p = 0.39).
For the RFWT, seven women performed repeat tests on different occasions (Pearson’s r = 0.91, p < 0.01). For consistency, when a participant performed more than one RFWT, only the first test was used for all further analyses. RFWTs were performed by 23 women and analyzed for this study.
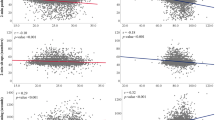
Figure 1 depicts the relationship between age and estimated VO2max for this group and extracted normative average (50th percentile) and poor data (10th percentile; 23, 29). This figure reveals an interesting age divide in that while the Somali women under 30 in this study had average or above average fitness levels, all the women older than 30 (n = 12) had below average or very poor fitness levels. Eight women had an estimated VO2max below the 10th percentile and all of these women were older than 30 years. The average BMI for the eight women with an estimated VO2max below the 10th percentile was 32.44 kg/m2 (28.0–38.3 kg/m2) and their average age was 53 years (32–66 years). Indeed, this is supported by research showing adverse health impacts of migration [31, 32].

Relationship between maximal oxygen uptake and age for Somali women and normative data for 50th and 10th percentiles [23, 28]
Conclusions and Implications
This research found that a high proportion of Somali women were overweight or obese with excess WHRs and low predicted VO2max. This indicates compromised health and cardiorespiratory fitness that can lead to more serious medical conditions. In particular, lifestyle related disease risk, such as diabetes, CVD and cancer, would be predicted to be higher among this group than the general population. However, there is a growing literature suggesting the need for more research on the appropriateness of BMI and other criteria for assessing health risk in different ethnic groups [33–35]. More research is needed with Somali to determine if, indeed, the data presented in this report are indicative of higher lifestyle disease risk.
While all attempts were made to acquire an adequate sample of Somali women, it is possible, at least among the older women that only overweight women volunteered for the study as average or underweight women could view exercise and fitness as something that is done only if one is overweight. Regardless, the low fitness levels and extent of overweight revealed in this study are important enough to warrant attention.
General Practitioners and other medical and health professionals who consult with Somali refugees should be made aware of these issues and assess Somali clients, particularly older women, for lifestyle related diseases such as diabetes, cancer and CVD. Although BMI is a crude risk assessment tool, it is valuable in providing some initial indication of health risks [25, 26, 31]. The long gowns usually worn by Somali women can conceal the extent of overweight and obesity, with health professionals inadvertently overlooking the need to assess and obtain actual bodyweight and height. Also, language and other barriers and concerns may make obtaining weight and height for Somali women a low priority for some health professionals.
Guerin et al. [12] describe some possible approaches to addressing physical inactivity with Somali women, taking into consideration individual differences and preferences. For example, walking groups, sport groups, community exercise classes and gym memberships are just a few options health professionals can suggest and facilitate participation by phoning coordinators of such programs to find out what assistance might be available to encourage participation. While some Somali women may prefer to exercise only with other women, others will exercise in the presence of men, but this issue needs to be addressed clearly with women.
It is also important to consider the dramatic lifestyle changes that these women have experienced which are major contributors to their current health [10, 32, 33, 36, 37]. For example, for many of these women, walking was a central part of their daily lives prior to coming to New Zealand. Because of fear, climate, unfamiliar environment and other issues, most of these women do not walk as much as they used to which may contribute to their excess weight and low fitness levels. The age implications in this study are consistent with other research suggesting that obesity and sedentary behavior are more a reflection of the extreme lifestyle and environmental changes inherent in moving to, in this case, New Zealand from Africa and not inherent biological or cultural characteristics of Somali women [33]. It would be interesting to further study the length of time living in New Zealand and age when moving to determine the combined impacts of environmental and lifestyle changes and educational and cultural exposure.
Health care services for Somali are influenced by an array of factors such as transportation, language ability and cost, which can all be barriers [4, 12] and present significant challenges to health professionals. Often, Somali women will prefer to have female health professionals take measurements such as body weight and height. Some, particularly older, Somali women also do not read or write, even in their own language, which presents difficulties in providing written health promotion materials, even if they are translated [4].
References
United Nations High Commissioner for Refugees. Statistical Yearbook 2001. Geneva: UNHCR; 2002
Department of Immigration & Multicultural & Indigenous Affairs (DIMIA). Australia’s Refugee and Humanitarian Program: Fact Sheet 60; 2003. From URL: http://www.immi.gov.au, accessed May 2003
Refugee and Migrant Service. Annual Report 2001/2002. Wellington, New Zealand: Refugee and Migrant Service; 2002
Guerin B, Abdi A, Guerin PB. Health status of Somali refugees living in Hamilton and their experiences with the medical system. N Z J Psychol 2003;32:27–32
New Zealand Immigration Service. Refugee Quota All Years, accessed May 2004, from URL: http://www.immigration.govt.nz/Migrant/General/GeneralInformation/Statistics/Refugees.htm; 2004
Guerin PB, Diiriye RO. Conducting a census of Somali in a small New Zealand City. Institute of Australian Geographers Conference. April 13–16, Glenelg, Adelaide, South Australia; 2004
Statistics New Zealand. New Zealand Census of Population and Dwellings 2001. From URL: www.stats.govt.nz accessed November 2002, Statistics New Zealand, Wellington; 2001
United Nations Office for the Coordination of Humanitarian Affairs. IRIN Web Special on Separated Somali Children; 2003. Available on URL: http://www.irinnews.org/webspecials/Somalichildren/default.asp, accessed May 2004
Abdullahi MD. Culture and customs of Somalia. London: Greenwood Press; 2001
Guerin PB, Guerin B. Relocating refugees in developed countries: the poverty experiences of Somali resettling in New Zealand. In Lyon K, Voight-Graf C, editors. 5th International APMRN Conference, Fiji 2002: Selected papers. University of Wollongong: Wollongong; 2002. pp. 64–70
Ministry of Health. Refugee health care: a handbook for health professionals. Wellington, New Zealand: Ministry of Health; 2001
Guerin PB, Diiriye RO, Corrigan C, Guerin B. Physical activity programs for refugee Somali women: working out in a new country. Women Health 2003;38(1):83–99
Sundquist J, Cmelic-Eng M, Johansson SE. Body mass index and distribution of body fat in female Bosnian refugees—a study in primary health care. Pub Health 1999;113:89–93
Padwal R, Straus SE, McAlister FA. Cardiovascular risk factors and their effects on the decision to treat hypertension: evidence based review. BMJ 2001;322:977–80
Medicine and Science in Sports. [Supplement on effects of exercise]. Med Sci Sports; June 2001:33
Meisler JD. Towards optimal health: the experts discuss physical fitness. J Womens’ Health Gend Based Med 2002;11:11–6
Batty D, Thune I. Does physical activity prevent cancer? Evidence suggests protection against colon cancer and probably breast cancer. BMJ 2000;321(7274):1424–5
Ministry of Health. Chapter 3: Physical activity. In: Taking the pulse. Wellington: Ministry of Health; 1999
Ministry of Health. Chapter 6: Combined cardiovascular risk factors. In: Taking the pulse. Wellington: Ministry of Health; 1999
Pace B. The benefits of regular physical activity. JAMA 2000;283:3030
Meyer T, Broocks A. Therapeutic impact of exercise on psychiatric diseases: guidelines for exercise testing and prescription. Sports Med 2000;30:269–79
Salmon P. Effects of physical exercise on anxiety, depression, and sensitivity to stress: a unifying theory. Clin Psychol Rev 2001;21:33–61
U.S. Department of Health and Human Services. Physical Activity & Health: A Report of the Surgeon General. Atlanta, Georgia: U.S. DHHS, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; 1996
Ministry of Health. NZ Food: NZ People. Key results of the 1997 National Nutrition Survey. Wellington, New Zealand: Ministry of Health; 1999
Welborn TA, Dhaliwal SS, Bennett SA. Waist-hip ratio is the dominant risk factor predicting cardiovascular death in Australia. MJA 2003;179:580–5
Swinburn B. Using the body mass index: weigh then weigh up. N Z Med J 1998;111(1075):377–9
Melton III LJ, Marquez MA, Achenbach SJ, Tefferi A, O’Connor MK, O’Fallon WM, Riggs BL. Variations in bone density among persons of African heritage. Osteoporos Int 2002;13(7):551–9
American College of Sports Medicine. ACSM’s guidelines for exercise testing and prescription, 6th ed. London: Lippincott Williams & Wilkins; 2000
Fenstermaker KL, Plowman SA, Looney MA. Validation of the Rockport fitness walking test in females 65 years and older. Res Q Exerc Sport 1992;63:322–7
Kline GM, Porcari JP, Hintermeister R, Freedson PS, Ward A, McCarron RF, Ross J, Rippe JM. Estimation of VO2max from one mile track walk, gender, age and body weight. Med Sci Sports Exerc 1987;19:253–59
Ministry of Health. Progress on health outcome targets 1999. Wellington, New Zealand: Ministry of Health; 1999
Burns C. Moving to Australia could be bad for your health: food and nutrition issues of Somali women arriving in Australia as refugees. Nutridate 2002;13:5–7
Cooper RS, Rotimi CN, Kaufman JS, et al. Prevalence of NIDDM among populations of the African Diaspora. Diabetes Care 1997;20:343–8
Rush E, Plank L, Chandu V, Laulu M, Simmons D, Swinburn B, Yajnik C. Body size, body composition, and fat distribution: a comparison of young New Zealand men of European, Pacific Island, and Asian Indian ethnicities. NZ Med J 2004;117(1207)
Shiwaku K, Anuurad E, Enkhmaa B, Kitajima K, Yamane Y. Appropriate BMI for Asian populations. Lancet 2004;363(9414):1077
Guerin B, Guerin PB, Diiriye RO, Abdi A. Living in a close community: the everyday life of Somali refugees. Network 2004;16:7–17
Guerin PB, Corrigan C. Helping to make exercise and fitness an easier option for refugee Somali women. In: Women’s Studies Association (NZ) conference papers: words, action, change; 2001. pp. 83–7
Acknowledgments
The authors would like to thank Barbara Redfern, from RMS Refugee Resettlement for her support of this research, Dharma Arunachalam for statistical assistance and valuable feedback, Bernard Guerin for reviewing drafts of this article and making valuable suggestions, and the anonymous reviewers for comments on earlier versions of this paper. This research was supported with funding from the Foundation for Research, Science and Technology (UOWX0203); the Waikato Institute of Technology, Faculty of Applied Technology and Centre for Sport and Exercise Science Research funds; and RMS Refugee Resettlement.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Guerin, P.B., Elmi, F.H. & Corrigan, C. Body Composition and Cardiorespiratory Fitness among Refugee Somali Women Living in New Zealand. J Immigrant & Minority Health 9, 191–196 (2007). https://doi.org/10.1007/s10903-006-9030-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10903-006-9030-x