
Abstract
This study identified middle school students who were less than delighted with their lives (reported life satisfaction scores between 1 and 6 on a 7-point scale), and attempted to improve these students’ mental health via a 10-week group wellness-promotion intervention developed from prior applications of positive psychology research. Complete data at baseline, post-intervention, and 6-month follow-up was gathered from 55 sixth grade students who were randomly assigned to the intervention condition (n = 28) or wait-list control (n = 27). Repeated measures analyses of a propensity score matched sample of 40 participants indicated a significant group by time interaction for global life satisfaction from baseline to post-intervention. Specifically, life satisfaction of students in the intervention group increased significantly, while the control group declined during the same period (although this change was not statistically significant). The intervention group’s gains were maintained at follow-up, but were matched by similar gains for students in the control group. No effects of intervention group were identified in the indicators of affect or psychopathology. The improvements in life satisfaction evidenced by students in the intervention group during the first semester of middle school are important given the adjustment difficulties that often appear during this sensitive developmental period marked by biological and educational changes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Mental health is increasingly viewed as consisting not merely of the absence of illness or disorder, but also the presence of positive indicators such as subjective well-being (SWB). Children and adolescents with complete mental health (defined as high SWB in tandem with low psychopathology) have social and educational functioning that is superior to their peers who are also without clinical levels of mental illness but who have low SWB (Greenspoon and Saklofske 2001; Suldo and Shaffer 2008). Thus, aiming to simply prevent and ameliorate psychopathology is not sufficient; SWB must be fostered. In contrast to the growing number of evidence-based interventions to decrease psychopathology, few studies have examined the efficacy of psychological interventions designed to increase SWB in youth. This study evaluated the efficacy of a novel group intervention intended to increase the SWB of early adolescents who are less than delighted with their lives.
1.1 Fostering Youth Subjective Well-Being
Traditional views on improving mental health largely entail the healing of wounds, solving of problems, and reduction of stress that are at the heart of disorder (Seligman and Csikszentmihalyi 2000). However, the sole measure of negative emotional states (e.g., anxiety, depression) provides a limited view of mental health. The absence of mental illness is only one part of the equation, which is completed by the presence of SWB. Subjective well-being, sometimes referred to as a scientific operational definition for happiness, includes both a cognitive and affective self-evaluation of one’s life and experiences (Diener et al. 2009). A person with high SWB experiences frequent positive emotion, infrequent negative emotion, and an overall judgment of high satisfaction with his or her life on the whole.
Regarding determinants of happiness, Lyubomirsky et al. (2005) synthesized the literature into a three factor model, including set point, circumstance, and intentional activity. Regarding the former, happiness is set within a chronic range that is stable over time and presumably linked to one’s genetics. Although variability occurs from baseline, levels of happiness remain in a stable range over time. However, environmental factors (i.e., circumstance, intentional activity) influence the extent to which a person’s happiness level is in the upper or lower end of his or her potential range. Circumstances are incidental but relatively stable facts of an individual’s life (i.e., region lived in, age, gender, socioeconomic status, occupation). Although circumstances can influence a person’s point of happiness within one’s range, only approximately 8–15 % of the variance in SWB appears accounted for by such factors. In contrast, Lyubomirsky and colleagues assert that approximately 40 % of the variance in happiness levels is due to intentional activity in one’s daily life, including purposeful behaviors such as amount of exercise, cognitions such as looking at things in a positive light, and volitional activity such as setting and striving for goals. Intentional activity implies a personal choice to engage and requires effort to perform, which leaves a wide range in which one’s happiness is amenable to change. This understanding of the broad determinants of happiness implies that “increasing one’s set point and changing one’s life circumstances are not fruitful avenues for sustainable increases in chronic happiness… intentional behavioral, cognitive, or volitional activity offers the best potential route” (Lyubomirsky et al. 2005, p. 119). Positive changes in intentional activity appear possible with professional guidance, as summarized next.
A growing body of research with adult samples has demonstrated improvements in individuals’ well-being as a result of (a) existing clinical interventions, even when delivered to individuals with minimal psychopathology symptoms (for instance, behavioral activation to treat depression; Mazzucchelli et al. 2010), and (b) specific intentional activities purposefully designed to increase SWB through targeted facilitation of positive feelings, behaviors, or thoughts. Such positive psychology interventions (PPIs) include: increasing grateful thinking (Emmons and McCullough 2003), performing acts of kindness (Lyubomirsky et al. 2005), identification and use of one’s character strengths in new ways (Seligman et al. 2005), and writing about and visualizing methods to achieve life goals (King 2001). Such research supports Seligman’s (2002) multidimensional framework for increasing SWB through intentional activities related to one’s past, present, and future emotional experience. The rising menu of available PPIs enables practitioners to offer clients choice in their intervention activities (which is helpful in that preference for a specific PPI is tied to increased adherence to exercise completion and greater increases in well-being while the preferred PPI is being practiced; Schueller 2010) and to create comprehensive interventions that include multiple PPIs.
Only in the last 5 years have the first studies of PPIs intended to systematically increase youth SWB appeared in the literature. These studies show promising effects of focused interventions targeting gratitude, hope, or character strengths, all of which have been provided at children’s schools by either psychologists or classroom teachers. With respect to a PPI facilitated by psychologists, Marques et al. (2011) implemented a 5-week intervention designed to increase hope with 31 middle school students. In addition to providing children with weekly counselor-led group sessions focused on teaching children to increase their hopeful thinking and goal-directed behavior, at the start of the intervention children’s parents and teachers were provided with a 1-h training session on hope-related topics taught to children in the direct intervention. Compared to a matched wait-list control group, the intervention group experienced lasting gains (at 6- and 18-month follow-up) in hope, as well as lasting secondary gains in life satisfaction and self-worth (but no changes in emotional distress or academic achievement).
Gains in some indicators of SWB have also been obtained with the youth PPIs that were provided by classroom teachers and integrated into the curriculum. Specifically, a teacher-delivered 6-month curriculum consisting of character strengths-based exercises found that the 218 adolescents (ages 12–14) who participated in the intervention evidenced gains in life satisfaction (but no statistically significant changes in positive affect, negative affect, or self-esteem) compared to the 101 adolescent students who did not participate in the Strengths Gym program (Proctor et al. 2011). To test the effect of a gratitude intervention, Froh et al. (2008) randomly assigned 11 classes of middle school students (n = 211), to one of three conditions: gratitude (4 classes), hassles (4 classes), and control (3 classes). Daily for 2 weeks during class instruction time, students in the gratitude condition listed up to five things they were grateful for since yesterday, while students in the hassles condition wrote about things that annoyed or bothered them over the past day. The control group was limited to completing measures of the outcomes. Youth in the gratitude condition reported greater school satisfaction and reduced negative affect immediately after the intervention and at 3-week follow-up, particularly in relation to the hassles condition. The gratitude intervention was not associated with significant changes in global life satisfaction (reflection on past few weeks of life), positive affect, prosocial behavior, or physical health.
Regarding multi-target, comprehensive interventions for youth, Rashid and Anjum (2008) utilized positive psychotherapy (PPT), a model focused on developing resources of positive emotion, character strengths, and a sense of meaning in life to counteract depressive symptomology, in a randomized control trial with 22 middle school students. In addition to traditional psychotherapeutic techniques, students were engaged in PPIs (e.g., expressions of gratitude, utilization of character strengths, savoring enjoyments) in 8 weekly psychologist-led meetings. Compared to the no-treatment control group, the intervention group evidenced a significant increase in scores on a measure of happiness and well-being (the Positive Psychotherapy Index; Seligman et al. 2006) as well as improved weekly behavioral ratings that were provided by teachers. There were no significant group differences on depression or global life satisfaction after the intervention period concluded. In sum, although PPT was designed with depressed individuals as the target population, increases in happiness and well-being emerged in this non-depressed sample. These findings suggest that interventions targeting SWB may be beneficial to a wide variety of youth, perhaps even as a method of building resilience to mental health disorder. Further research is needed to determine if the gains in happiness and well-being that were associated with PPT endured across time.
1.2 Purpose of Current Study
Based upon the literature, we developed and tested a positive psychology manualized intervention intended to purposefully increase adolescents SWB. Utilizing Seligman’s (2002) framework for increasing happiness, the intervention consisted of 10 weekly sessions of intentional activities that were developmentally modified from research on adult samples. Rather than focusing on one area of intervention (e.g., gratitude, character strengths, optimistic thinking), we used a combination of evidence-based PPIs found in the literature. The intervention was evaluated in terms of associated changes with students’ SWB (life satisfaction, positive and negative affect frequency levels), as well as traditional negative indicators of mental health in order to explore possible secondary effects of the intervention on psychopathology. Outcome data were gathered immediately after the intervention concluded as well as 6 months later.
2 Method
2.1 Participants
A total of 55 students (28 in the intervention condition, 27 in the wait-list control condition) had complete data at all 3 time points. Table 1 presents the demographic characteristics of a subsample of 40 participants retained for analyses after the groups were matched on propensity scores (via procedures described later). The matched sample was almost equally split by gender and socioeconomic group (SES, as determined by receipt of free or reduced-price school lunch). Regarding ethnicity, the majority of these participants self-reported as Caucasian (35 %) or Hispanic (30 %). The participant age range was 10–12 years old, with a mean age of 11.43 (SD = .55) in the matched subsample. All students were in sixth grade, which corresponds to the first grade level of the middle school years (grades 6–8) in the participating school district.
Chi square tests of independence between the intervention sample (i.e., 28 students who completed the intervention group and provided complete data) and the 27 participants assigned to the wait-list control condition were conducted to test for potential effects of demographic characteristics on group assignment. Students in the intervention group were no more likely to be of a particular gender, χ2 (1, N = 55) = .17, p = .68, SES, χ2 (1, N = 54) = .67, p = .41, ethnicity, χ2 (6, N = 55) = 9.75, p = .14, parental marital status, χ2 (5, N = 55) = 3.35, p = .65, or guardianship, χ2 (6, N = 55) = 12.56, p = .051.
2.2 Procedures
2.2.1 Screening
The first author’s university Human Research Protection Program approved a waiver of informed consent documentation for the screening procedure. Specifically, all parents of sixth grade students at a single middle school received a letter that described the screening process with the option to inform the research team if they did not wish for their child to participate. Only 1 parent exercised this option. All other sixth grade students (N = 333) completed a screening measure of life satisfaction (the Brief Multidimensional Students’ Life Satisfaction Scale [BMSLSS], described below) during the first 2 weeks of school. The mean score within the overall sample was 5.95 (SD = 0.99). A subgroup of students (n = 132) reported life satisfaction with some (to substantial) room for growth, as defined as an average BMSLSS score between 1 and 6 on the 7-point metric. This subgroup was recruited for participation in the intervention because they had room for improvement, whereas students with mean scores above 6 were excluded because their life satisfaction was quite near the top of the range of possible scores (precluding the need for intervention resources). The mean BMSLSS score was 4.80 (SD = .90) for the 28 students ultimately included in the intervention condition, and 4.72 (SD = 1.20) for the 27 students in the control condition.
2.2.2 Participant Recruitment and Retention
A letter describing the intervention (termed a “wellness-promotion program”) was sent to the families of all 132 students identified in the screening. Parents of 72 students (55 % of target sample) provided written consent for participation. Five of the students reported disinterest in participation due to the social stigma of group counseling and did not assent. The 67 students with both consent and assent to participate completed a demographic survey and baseline measures of SWB (life satisfaction and affect) and psychopathology in the early fall. Upon completion of self-report measures, students were randomly assigned to 1 of 2 conditions: immediate receipt of intervention (n = 35) or a delayed-intervention control group (n = 32). Ten students (6 from intervention, 4 from control) withdrew from the study throughout the 10-week intervention period due to (a) moving from the area (n = 8) and student choice to discontinue participation in the intervention (n = 2) in order to attend physical education class. One additional student who completed the intervention condition was removed from the dataset due to missing baseline data. In the 6-month period from post-intervention to follow-up, 1 more participant (from the control group) changed schools, leaving a final sample of 55 students with complete data at 3 time points.
2.2.3 Intervention Implementation
Youth assigned to the intervention condition were evenly divided into five groups. In addition to the 7 student participants, each group had 1 leader and 1 co-facilitator. Each group received 10 weekly sessions of group intervention (described below) during their elective period (e.g., in place of art, physical education, computers, etc.) at a set day/time each week throughout the fall semester. All students who completed the intervention condition participated in all 10 sessions, either within the regularly scheduled group or through individual make-up sessions with group leaders. Six school psychologists provided the intervention via their designated roles as leader (the first and second authors) or co-facilitator (4 additional doctoral students in school psychology). Students in the control condition received the intervention the following school year; during their 6th grade year, they served as a wait-list control, with no exposure to the PPIs or the research team outside of assessment sessions.
2.2.4 Post-Intervention and Follow-Up Data Collection
The week after the intervention concluded (shortly before the holiday break), all 57 remaining participants in either condition completed the same measures administered at baseline. At 6-month follow-up (the end of the school year), the 56 students who remained enrolled at the school repeated the measures.
2.3 Measures
Students’ mental health was assessed by four self-report instruments (described next), administered at different time points in the study. The BMSLSS was used first, to screen all 6th grade students for life satisfaction. This measure was selected because of its brevity in gauging youths’ satisfaction in major domains of life. Three different measures (Students’ Life Satisfaction Scale for global life satisfaction, Positive and Negative Affect Scale for Children for affect, and Youth Self Report form of the Child Behavior Checklist for psychopathology) were administered to the students in the intervention and control groups at three time points: pre, post- and follow-up. The outcome measures selected reflect gold standards for self-report assessments of the constructs of interest, with an abundance of support for strong psychometric properties among early adolescent samples. The BMSLSS was used in the screening instead of the SLSS in part due to its brevity and simplicity (i.e., straightforward items), rendering it useful as a blanket screener for the entire sixth grade population to complete in a minimally invasive manner. The BMSLSS was specifically designed to provide a snapshot of well-being, which could be further assessed as needed in those who report less than maximum life satisfaction scores.
2.3.1 Brief Multidimensional Students’ Life Satisfaction Scale (BMSLSS)
The BMSLSS (Seligson et al. 2003) is a brief form of the Multidimensional Students’ Life Satisfaction Scale (MSLSS; Huebner 1994), which was developed as a comprehensive measure of the five domains (i.e., Family, Friends, School, Self, and Living Environment) that contribute to general life satisfaction in youth. The BMSLSS contains 6 items, 5 of which represent the domains of life satisfaction (e.g., I would describe my satisfaction with my family life as…) and one taps global satisfaction with one’s life overall (i.e., I would describe my satisfaction with my overall life as…). Students respond on the following 7-point scale: 1 = terrible, 2 = unhappy, 3 = mostly dissatisfied, 4 = mixed (about equally satisfied and dissatisfied), 5 = mostly satisfied, 6 = pleased, and 7 = delighted. The 5 domain items are averaged to create a total life satisfaction score while the global life satisfaction question stands alone as a 1-item indicator.
Previous research with middle school students indicated satisfactory internal consistency for the total score (α = .75), a strong correlation (r = .66) between the total scores from the BMSLSS and the lengthier MSLSS, and moderate intercorrelations among the domains on the BMSLSS (r = .30 to .42) that are similar to that with the MSLSS (Seligson et al. 2003). Seligson and colleagues’ multitrait-multimethod matrix supported convergent validity through significant correlations between the domains of the BMSLSS and MSLSS, ranging from .47 to .60 with a mean of .53. In the current study, the coefficient alpha for the BMSLSS in the total sample (n = 55) was .44.
2.3.2 Students’ Life Satisfaction Scale (SLSS)
The SLSS (Huebner 1991) was administered to assess students’ global satisfaction with life. Children are directed to indicate their level of agreement with 7 general statements about their life (e.g., I have a good life, I have what I want in life). Response options range from 1 (strongly disagree) to 6 (strongly agree). An overall life satisfaction score was attained by reverse-scoring 2 negatively-phrased items, then averaging participants’ responses. Higher mean SLSS scores indicate higher global life satisfaction.
The SLSS has high internal consistency (α = .82 to .88) and test–retest reliability at 1-2 weeks (r = .74; Huebner 1991) and 4 weeks (r = .64; Gilman and Huebner 1997). The construct validity of the SLSS is supported by large associations with other measures of subjective well-being (Huebner 1991). A positive relationship (r = .54) between SLSS scores and parent ratings of their children’s happiness further supports convergent validity (Gilman and Huebner 1997). In the current sample of 55 students, coefficient alpha of the SLSS was .88 at Time 1, and .91 at Time 2 and Time 3.
2.3.3 Positive and Negative Affect Scale for Children (PANAS-C)
The PANAS-C (Laurent et al. 1999) was adapted from the Positive and Negative Affect Scale (PANAS; Watson et al. 1988) to be appropriate for children in 4th to 8th grades. It assesses the frequency with which an individual experiences both emotional distress (e.g., negative mood such as fear, sadness, and anger) and emotional arousal (e.g., positive mood characterized by interest, engagement, and energy). The PANAS-C consists of a 12-item positive affect scale and a 15-item negative affect scale. Children rate 27 words that describe various positive emotions (e.g., interested, cheerful, excited) and negative emotions (e.g., miserable, lonely, guilty) on a 5-point Likert-like scale to indicate the extent to which they have experienced each emotion in the past few weeks, from 1 (very slightly or not at all) to 5 (extremely). Responses to items within the positive and negative affect scales are averaged in order to generate scores by scale.
Laurent et al. (1999) reported high internal consistency for the negative affect (α = .92) and positive affect (α = .89) scales, and a moderate negative correlation between the positive and negative scales (r = −.36), indicating they divergently measure opposing constructs. Evidence of convergent validity was provided via strong correlations between the negative affect scale and narrowband measures of depression and anxiety, and divergent validity was supported by moderate, inverse correlations between the positive affect scale and the same indicators of internalizing distress. In the current study, alphas values for the positive and negative affect scales were .90 and .92 at Time 1, .92 and .94 at Time 2, and .95 and .92 at Time 3, respectively.
2.3.4 Youth Self Report Form of the Child Behavior Checklist (YSR)
The YSR (Achenbach and Rescorla 2001) is a 112-item self-report measure of psychopathology that assesses eight areas of problem behavior in children. The current study analyzed the 31- and 32-item composites for internalizing problems (sum of items in the anxious/depressed, somatic complaints, and withdrawn/depressed subscales) and externalizing problems (sum of items in the aggressive behavior and rule-breaking behavior subscales), respectively. Students reported the degree to which feelings or behaviors were accurate for them currently or in the past 6 months, using a 3-point scale from 0 (not true) to 2 (very true or often true).
The YSR internalizing and externalizing problems composites represent patters of co-occurring behaviors as indicated by factor analysis (Achenbach and Rescorla 2001). The reliability of these problem composite scores is considered high, as coefficient alpha values exceed .90 (Achenbach and Rescorla 2001). The YSR has demonstrated high test–retest reliability at 8-days for the internalizing and externalizing problems composites, with correlations of .80 and .89, respectively. The YSR technical manual provides evidence of the construct validity of the internalizing problems composite, including a strong correlation with the depression checklist of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV; r = .59). Construct validity of the YSR externalizing problems composite is supported by a large correlation with the conduct disorder checklist of the DSM-IV (r = .62). In the current study, coefficient alphas for the YSR internalizing and externalizing problem composites were .91 and .90 at Time 1, .93 and .94 at Time 2, and .92 and .92 at Time 3, respectively.
2.4 Wellness-Promotion Intervention
Development of the intervention manual was guided by (a) Seligman’s (2002) framework for increasing happiness and (b) PPIs that have worked to increase adults’ happiness in the literature that were developmentally modified by the current research team for middle school students. The 78-page manual (available upon request from the first author) details procedures for each intervention, along with reference to the research-based underpinnings. Table 2 contains a summary of the intervention procedures, with regard to the goals of each session, activities and discussions facilitated in order to meet those goals, and rough estimates of the amount of time group leaders allocated to a given activity in order to ensure completion of session content. All sessions contained counselor-facilitated discussions of concepts relevant to happiness, introductions to specific PPIs, and homework assignments that involved completion or rehearsal of the PPI taught during the group session. Each session, students received small treats (candy, school supplies) contingent on homework completion and/or participation in group discussions and activities. The first session contained an introduction to the intervention format and purpose, in addition to completion and discussion of the “You at your best” PPI that is associated with a short-term boost in SWB (Seligman et al. 2005). The last (tenth) session focused on termination, including a review of concepts followed by reflection on the intervention experience. Sessions 2 through 9 were organized into three sections in alignment with Seligman’s (2002) framework for increasing happiness into one’s upper ranges through intentional activities, including by increasing (a) expressions of gratitude for past events, (b) gratifications through novel use of character strengths, and (c) positive future-oriented emotions through development of an optimistic explanatory style and hopeful, goal-directed thinking.
2.4.1 Past-Focused Positive Feelings
The goal of sessions 2 and 3 was to create positive interpretations of past events. Gratitude journals were developed as a method of focusing student thoughts on things, people, and events for which they are grateful. Students were asked to write 5 things for which they are grateful in each journal entry and to provide a variety of responses across entries (“include events, people, talents, or anything else you think of, whether it is large or small”). The intensity is high for the first week, in that students are asked to journal daily, in line with Emmons and McCullough’s (2003) finding that higher intensity lead to greater increases in happiness. Subsequent journaling was completed on a once per week basis due to the introduction of other activities. The gratitude visit (Seligman et al. 2005) was intended to increase the experience of gratitude by intensifying the connection between thoughts, feelings, and actions. It consisted of an expression of gratitude in a letter and delivery of the letter to someone who has been especially kind but never properly thanked. Group leaders helped students to determine who in their lives had been especially kind to them and choose an individual to whom they could enact a face to face visit. Students were then assisted in writing 1-page letters describing reasons why they were grateful to that person, and reported the outcome of their gratitude visit at the next session.
2.4.2 Present-Focused Positive Feelings
The primary purpose of sessions 4 through 7 was to facilitate engagement in activities that are enjoyed through identifying, interpreting, and tapping into strengths. First, acts of kindness were defined as behaviors that benefited others or made others happy, at the cost of your time or effort (Lyubomirsky et al. 2005; Otake et al. 2006). Students were asked to perform 5 acts of kindness during 1 designated day per week over at least 2 weeks. Some examples of acts of kindness included doing household chores typically assigned to parents (e.g., walking the dog, washing dishes), helping sibling(s) or classmates with school assignments, and helping the teacher clean up the classroom. Next, students completed the Values in Action Inventory of Strengths for Youth (VIA-Youth; Park and Peterson 2006) online at www.authentichappiness.org. With a group leader, students (a) reviewed their computer-generated report that listed and described their character strengths, (b) identified their signature strengths, and (c) selected a signature strength to use in a new way each day for 1 week. Due to the complexity of some strengths (e.g., appreciation of beauty and art, perspective, prudence), some participants had challenges planning multiple developmentally appropriate activities. Therefore, students and group leaders brainstormed together as many unique ways to enact strengths as possible and students were asked to add in new ways they thought of during the week or to repeat one to two ways of performing the strength. The next week included new uses of another signature strength with the addition of using strengths across life domains (i.e., family, friends, and school). Students were asked to record their feelings after each use of their chosen signature strength in order to enhance the connection between thoughts, actions, and feelings of well-being, and prompted to savor the positive experiences that stemmed from use of signature strengths (Bryant and Veroff 2007).
2.4.3 Future-Focused Positive Feelings
Sessions 8 and 9 focused on development of a positive framework for explanation of current life events and expectation of future events. Learned optimism (Seligman 1990) is a cognitive-behavioral method for changing one’s explanatory style in making attributions about events. An optimistic explanatory style includes attributions of permanency to positive life events and temporary attributions to negative life events. Optimists see the positive as universal (e.g., “I’m good at all of my classes because I’m smart”) and the negative as specific (e.g., “Mr. Smith gave an unfair test”). The final piece of explanatory style is personalization, specifically optimists self-blame for positive events. Seligman’s description was utilized to teach students how to increase use of optimistic thinking, through learning to restructure thoughts to be optimistic (using developmentally appropriate language) in session and student use of optimistic thinking 1 time each day for a week as homework. Students received specific forms to guide them through this process in and out of session.
Activities designed to engender hope were in line with Snyder et al. (2005) conceptualization of hope theory, in which hopeful thinking comprises both the ability to envision viable methods for goal attainment and belief in one’s ability to utilize those methods in reaching specific goals. King (2001) found that writing about life goals in the form of an exercise described as one’s “best possible self” (i.e., a version of the future self having accomplished desired life goals) was highly associated with increased happiness and decreased negative affect. “Best possible self” was modified by asking middle school students to write for 5 min about how they would achieve their life goals and then add new ideas each night for 1 week, encouraging them to think about specific ways in which they might accomplish goals. Examples of student goals included: Having a big house, becoming a doctor/lawyer/sports star, and having a spouse and children. Typical methods for achieving goals included working hard in school, going to college, and practicing athletics. Students shared their stories in session 10.
2.4.4 Student Feedback
At the end of the tenth session, participants completed a one-page feedback form that contained five open-ended questions: What do you feel are some of the most important things you learned in the program? What did you like best about the program? … Least? Suggestions to improve the program? Additional comments? The form also listed the 8 PPIs covered in the intervention, and asked students to check “Which activities that you learned in the meetings are you likely to continue to do on your own?”
2.4.5 Intervention Fidelity
To ensure consistency of implementation between group leaders, the leaders and co-facilitators collaborated weekly to plan for the next group session, including detailed review of the manual that was completed in its entirety by the research team prior to the onset of the intervention. After completing the first group session of each week, the first author communicated to the second author her impressions of student understanding and participation. The second author noted specific examples and unique methods used to facilitate learning and replicated these strategies with the intervention groups she led later in the week. During sessions, the group co-facilitator checked each activity as it occurred in session. The co-facilitators informed the leader of any areas needing further attention prior to the end of the session and used cues to help the leaders pace activities within the allotted time. These procedures resulted in 100 % fidelity with planned session activities.
2.5 Overview of Data Analysis Plan
Prior to analyses, 2 students (1 from the control condition, 1 from the intervention condition) identified as univariate outliers (across-time changes in an indicator of SWB were >3 SD from the sample mean on change scores) were removed. Because t-tests of between-group differences indicated that at baseline the 27 students randomly assigned to the intervention group had lower life satisfaction scores and reported significantly more externalizing symptoms of psychopathology than the 26 students assigned to the control group, propensity score matching (see Fan and Nowell 2011, for an overview) was used to identify subsets of students in the intervention and control groups with approximately equivalent baseline scores. To calculate propensity scores representing the likelihood of being assigned to the intervention condition based on baseline characteristics, baseline life satisfaction, positive affect, negative affect, internalizing, and externalizing scores were entered as predictors of assignment to the intervention condition in a logistic regression analysis, with predicted probabilities of being assigned to the treatment group saved as propensity scores. Absolute differences between the propensity scores of students in the intervention and control conditions were calculated using the dist macro (Kosanke and Bergstralh 2004a), and the vmatch macro (Kosanke and Bergstralh 2004b) was used to match students based on these absolute differences. The vmatch macro was specified with a maximum absolute difference of .20, .15, and .10 between matched pairs, and the matches with a maximum difference of .15 were retained as the best solution because baseline differences between the intervention and control groups were trivial with this solution and more students were matched than with a .10 maximum difference. A total of 40 students (20 intervention and 20 control) were matched, and baseline differences between the groups in the matched samples are presented in Table 3.
All data analyses were conducted using Statistical Analysis Software (SAS). An alpha level of .05 was used to determine statistical significance and η2 was used as the primary measure of effect size. Commonly-used guidelines for small, medium, and large values of η2 are .01, .06, and .14, respectively (Cohen 1988). Repeated measures analysis of variance (ANOVA) was used to determine if there were between-groups differences in (a) overall patterns of change from pre-intervention to post-intervention to follow-up, (b) change from pre-intervention to post-intervention, and (c) change from post-intervention to follow-up. In these analyses, F statistics for the group by time interaction are reported as tests of whether changes were significantly different across the intervention and control groups.
3 Results
3.1 Intervention Acceptability
On the feedback form, students expressed considerable interest in and enjoyment of intervention sessions through statements such as “I liked the program very well and look forward to a brighter and happier future.” Regarding the most important or preferred aspects of the intervention, most students (86 % of the 29 respondents) mentioned specific PPIs, including gratitude journals and visits, performing acts of kindness, optimistic thinking, using signature strengths, hope, and savoring (e.g., “I learned that being hopeful and savoring happy feelings help out when you’re trying to be happy”). Beyond discussion of specific PPIs, students commented positively on (a) receiving candy during group sessions (24 % of sample; e.g., “whenever we participated in trying to make ourselves happier, we got a treat”), (b) the opportunity to share feelings in a group counseling format (17 %; e.g., “I could express my own opinions without being afraid it would sound dumb”), and (c) forming friendships with other students in their group (10 %; e.g., “the fact that I know there are people like me”). Regarding suggestions for improvement, 34.5 % of students wrote “nothing” (an additional 10 % of respondents left the section blank); the two suggestions mentioned by more than one individual involved provision of additional candy or treats (17 % of sample) or extending the duration or intensity of the program (14 % of sample; e.g., “do [the program] three times a week”). Regarding which of the PPIs that they were likely to continue to do on their own, all students checked at least 1 activity. The largest proportion of students (69 %) indicated character strengths, followed by: acts of kindness (66 %), optimistic thinking (66 %), Best possible self (62 %), gratitude journals (48 %), gratitude visit (41 %), savoring (41 %), and Me at my Best (38 %). Summative comments indicated that students appeared to benefit from the experience of the intervention as a social setting as well as the actual didactic content (e.g., “Thank you for helping me cheer up about myself and helping me make more friends”).
3.2 Changes in Subjective Well-Being
Table 3 presents mean scores, by group, on all constructs of interests at all times for the 40 participants in the matched pairs that were retained for data analyses.
3.2.1 Life Satisfaction
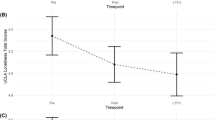
Results of a between-groups repeated measures ANOVA analyzing scores for the matched sample from pre-intervention to post-intervention to follow-up yielded a non-statistically significant trend toward a group by time interaction, F(2, 37) = 2.50, p = .096, η2 = .12. Although patterns of overall change did not statistically differ between groups, there were statistically significant between-group differences in change from pre- to post-intervention, F(1, 38) = 4.26, p = .046, η2 = .10. Specifically, the SLSS scores of students in the intervention group significantly increased from pre- to post-intervention [F(1, 19) = 4.81, p = .041, η2 = .20], while the SLSS scores of students in the wait-list control group declined, but not to a statistically significant degree [F(1, 19) = .59, p = .450, η2 = .03], during the same period (see Fig. 1). When investigating between-group changes from post-intervention to follow-up, there was a trend toward a group by time interaction [F(1, 38) = 3.19, p = .082, η2 = .08], in part due to a statistically significant increase in SLSS for students in the wait-list control group, F(1, 19) = 8.94, p = .008, η2 = .32. Changes in SLSS from post-intervention to follow-up for the intervention group were not statistically significant [F(1, 19) = .93, p = .348, η2 = .05], indicating the aforementioned intervention gains were maintained.

Participants’ mean levels of subjective well-being at baseline, post-intervention, and follow-up. a Life satisfaction. b Positive affect. c Negative affect
3.2.2 Affect
As displayed in Fig. 1, there were no statistically significant between-group differences in overall change (i.e., no significant group by time interaction effects) from pre-intervention to post-intervention to follow-up on positive affect [F(2, 37) = .74, p = .484, η2 = .04] or negative affect [F(2, 37) = .13, p = .878, η2 = .01]. In addition, there were no statistically significant between-group differences in change from pre- to post-intervention in terms of positive affect [F(1, 38) = .21, p = .653, η2 = .01] or negative affect [F(1, 38) = .27, p = .609, η2 = .01]. For positive affect, changes from pre- to post-intervention were not statistically significant for either the intervention [F(1, 19) = 3.22, p = .089, η2 = .15] or control group [F(1, 19) = 1.58, p = .223, η2 = .08]. For negative affect, neither the control group [F(1, 19) = .17, p = .687, η2 = .01] nor the intervention group [F(1, 19) = .10, p = .757, η2 = .01] reported statistically significant changes pre- to post-intervention. From post-intervention to follow-up, there were no statistically significant between-group differences in change on positive affect [F(1, 38) = 1.51, p = .227, η2 = .04] or negative affect [F(1, 38) = .03, p = .867, η2 = .00]. For positive affect, there was a statistically significant increase from post-intervention to follow-up for the control group [F(1, 19) = 5.25, p = .034, η2 = .22), but the increase in the intervention group was not statistically significant [F(1, 19) = .34, p = .565, η2 = .02]. For negative affect, both the intervention [F(1, 19) = 5.44, p = .031, η2 = .22) and control [F(1, 19) = 4.51, p = .047, η2 = .19) groups reported statistically significant decreases from post-intervention to follow-up.
3.3 Changes in Psychopathology
As displayed in Fig. 2, there were no statistically significant between-group differences in overall change from pre-intervention to post-intervention to follow-up on internalizing [F(2, 37) = .32, p = .725, η2 = .02] or externalizing [F(2, 37) = .78, p = .467, η2 = .04] symptoms of psychopathology. In addition, there were no statistically significant differences between matched groups in change from pre- to post-intervention in terms of internalizing [F(1, 38) = .66, p = .421, η2 = .02] or externalizing [F(1, 38) = .15, p = .700, η2 = .00] symptoms. Both the intervention [F(1, 19) = 6.37, p = .021, η2 = .25] and control [F(1, 19) = 4.61, p = .045, η2 = .20] groups reported statistically significant decreases in internalizing symptoms, but experienced no statistically significant changes in externalizing symptoms [F(1, 19) = 1.16, p = .296, η2 = .06, and F(1, 19) = .32, p = .580, η2 = .02, respectively] from pre- to post-intervention. There were also no statistically significant between-group differences in change from post-intervention to follow-up on internalizing [F(1, 38) = .01, p = .896, η2 = .00] or externalizing [F(1, 38) = 1.59, p = .215, η2 = .04) symptoms. Changes in internalizing symptoms were not statistically significant for either the intervention or control groups from post-intervention to follow-up [F(1, 19) = 3.84, p = .065, η2 = .17, and F(1, 19) = 4.33, p = .051, η2 = .19, respectively). The control group reported a statistically significant decrease in externalizing symptoms from post-intervention to follow-up [F(1, 19) = 6.47, p = .020, η2 = .25], but the decrease for the intervention group was not statistically significant [F(1, 19) = .77, p = .392, η2 = .04].

Participants’ mean levels of psychopathology at baseline, post-intervention, and follow-up. a Internalizing psychopathology. b Externalizing psychopathology
4 Discussion
The current study found that early adolescents’ participation in a 10-week group intervention that incorporated the principles of positive psychology and happiness-increasing strategies (i.e., positive psychology interventions; PPIs) was associated with student enjoyment of the intervention and simultaneous increases in global life satisfaction. Gains in life satisfaction specific to students who received the intervention provide preliminary support for the efficacy of a comprehensive wellness-promotion intervention for adolescents who initially report room for increases in life satisfaction. Confidence that improved life satisfaction was attributable to the intervention is enhanced by the rigor of the study design, specifically use of random assignment to condition followed by use of propensity score matching to limit statistical comparisons to subsets of students in the intervention and control groups with approximately equivalent baseline scores. In contrast to the positive short-term effect on life satisfaction, no additional short-term effects on other indicators of mental health or additional long-term gains on any aspect of SWB or psychopathology were identified in the current study. The variability in study outcomes is consistent with results of all other PPIs conducted with youth in which positive effects were detected on some (but not all) indicators of SWB (Froh et al. 2008; Proctor et al. 2011; Rashid and Anjum 2008) and no changes were evidenced on indicators of emotional distress (Marques et al. 2011; Rashid and Anjum 2008).
Of the five indicators of mental health examined in the current study, global life satisfaction may be the one of greatest relevance due to its reputation as the most stable component of subjective well-being (Diener et al. 2009). Because the affective components of SWB capture both momentary emotional states as well as longer-term moods and tendencies, affect ratings may be rather transient and unduly influenced by a rater’s present mood (and thus temporary circumstance) when completing the rating forms. In contrast, global life satisfaction ratings, which require a respondent to appraise the overall quality of one’s life, may be the most reliable indicator of persistent changes in one’s emotional quality of life.
In addition to assessing SWB, the intended target of the wellness-focused intervention, the current study also evaluated youth psychopathology in order to detect for possible secondary effects on related outcomes. The lack of significant changes in either internalizing or externalizing psychopathology as a result of participation in the positive psychology intervention further supports the notion that wellness and pathology are separable constructs (Keyes 2005; Suldo and Shaffer 2008), and clinician-facilitated change in the determinants of one may not be sufficient to effect change in levels of the other. When working with youth with elevated psychopathology, psychologists have a growing number of efficacious clinical interventions from which to draw (e.g., Weisz and Kazdin 2010). It is possible that both negative and positive outcomes could be improved simultaneously by addressing both SWB and psychopathology through purposeful facilitation of positive emotions via PPIs (c.f., Boehm and Lyubomirsky 2009) in addition to implementation of evidence-based clinical interventions to reduce symptoms of psychopathology (c.f., Mazzucchelli et al. 2010).
The moderate increase in global life satisfaction observed in students in the intervention group may be particularly clinically significant when considered in the context of the transition to middle school. In part due to the difficulty in making a school transition at the same time that pubertal changes are occurring, students often experience academic, social, emotional and behavioral difficulties upon entering middle or junior high school (Eccles et al. 1991; McDougall and Hymel 1998). In this study, students in the intervention group experienced gains in life satisfaction by mid-year that were greater than students in the wait-list control. The improvements in quality of life exhibited by the students in the intervention group during the first semester of middle school are particularly promising given the adjustment difficulties that are often present during this transition period. Students in the wait-list control experienced similar gains over the second semester of the school year, suggesting that without support early adolescents may settle down in the new school stage somewhat later.
4.1 Limitations
Design features of the current study that limit the confidence in findings primarily include a potential SWB ceiling effect due to the screening process for participant recruitment and the nature of life satisfaction, the low internal consistency of the BMSLSS, reduced power due to small sample size, and generalizability of results based on intervention setting. First, consistent with the general intent of positive psychology to improve wellness in all people rather than limit services to clinically ill individuals, we invited all youth with any room for growth in life satisfaction (including adolescents whose average life satisfaction scores corresponded to a response of “pleased,” a rating of 6 on the 7-point screening measure) to take part in the intervention. As reflected in the relatively high mean BMSLSS scores by group (i.e., mean score corresponding to a rating of “mostly satisfied”), many participants had limited room for increases due to initial high levels, creating a ceiling effect. Findings may have differed within a sample of participants with lower initial levels of life satisfaction (i.e., a clinical sample).
The poor internal consistency for the BMSLSS among the intervention sample is much lower than that reported by Seligson et al. (2003), perhaps due to the current study’s restricted range after all students with very high scores were eliminated during the screening process. The low alpha may also reflect the multi-dimensional measure of the BMSLSS, as students who were recruited for intervention could be happy with one area of life but dissatisfied in other domains (whereas students not recruited were mostly happy across all domains). As only the BMSLSS composite score was considered in the screening, students with room for increases in satisfaction only in specific domains were not purposefully targeted for participation but may have ended up in the intervention or control conditions. It is unknown if the intervention is differentially effective with youth whose life satisfaction is diminished globally or in certain areas of life.
Regarding sample size, the current study may be best conceptualized as a pilot for the wellness-promotion intervention developed by the research team. The sample size suggested limited power to detect statistically significant effects; however, a larger sample size was not possible due to finite resources and moderate attrition associated with student mobility, and the current sample size was adequate to detect the observed effects on life satisfaction. The sample size was more problematic due to limited ability to minimize baseline differences through randomization—the groups differed on baseline life satisfaction and externalizing behavior, with participants in the intervention condition having worse mental health. The possible influence of these pre-existing differences on later levels of mental health was ameliorated by restricting analyses to a matched sample of 20 per condition, which further reduced sample size and power to detect an effect (i.e., increased chance for Type II error). It is thus possible that between-group differences exist but could not have been detected at a statistically significant level due to the power of analyses being limited by sample size. This phenomenon is reflected in data trends in internalizing psychopathology, in which the intervention condition evidenced a sharper decrease in symptoms from pre- to post-intervention, but not at a statistically significant level.
Last, this study is limited in terms of ecological validity. Specifically, conclusions regarding the intervention may only be generalizable to a group condition in a school setting. It is unknown if similar results would be obtained if the intervention was delivered individually, and/or in another setting such as an outpatient clinic.
4.2 Directions for Future Research
In addition to replicating the current study with larger and more diverse samples of youth to address the aforementioned limitations, it is recommended that samples of older students in the later grades of middle school or high school be purposefully recruited for inclusion in future studies. Due to the cognitive complexity of some PPIs such as learned optimism, the intervention tested in the current study may evidence greater effects within samples of youth with higher cognitive abilities.
Future evaluations of the intervention developed and piloted in the current study may also consider modifying the intervention with the goal of extending youth exposure to program content and activities by either (a) including parents and/or teachers in the intervention, ideally to reinforce concepts and skills learned in group sessions, (b) adding follow-up meetings with group leaders (i.e., “booster sessions”), perhaps tailored to adolescents’ preferences for specific PPIs, or (c) evaluating if the intervention could be delivered effectively by classroom teachers. The former idea is in line with the fact that the only positive psychology intervention to date to evidence maintained gains in children’s global life satisfaction incorporated participants’ caregivers in the intervention (Marques et al. 2011). While it is unknown if those effects would have emerged without the parent/teacher component, a similar child-focused intervention (although targeting gratitude instead of hope) that did not include parents did not yield significant gains in global life satisfaction (Froh et al. 2008).
Regarding the second idea, continued prompted practice for rehearsal of activities may be necessary to maintain intervention gains in life satisfaction. This notion is in line with Huppert and Johnson’s (2010) finding that increases in adolescents’ well-being associated with a classroom-based mindfulness training intervention were most apparent in those youth who practiced the mindfulness activities the most outside of the classroom. Thus, booster sessions in which group leaders track and reward participants continued use of PPIs taught such as acts of kindness and gratitude journaling may further facilitate the life satisfaction growth trajectory observed in the current study during the active intervention phase. In light of the fact that feedback from participants in the current study suggested considerable variability in children’s preferred intervention activities, and the potential benefits of tailoring PPIs in line with client preferences (Schueller 2010), group leaders may consider developing individualized plans in collaboration with adolescents to specify which PPIs they should continue to emphasize outside of group sessions as well as practice after the active intervention period has ceased. Individualized booster sessions may focus on progress with those most preferred PPIs.
The true importance of SWB-enhancing interventions for youth may lie in the extent to which they can be successfully disseminated to broad populations of children and adolescents, as opposed to reserved for clinical application to only distressed youth like most traditional psychological interventions. While the intervention developed in the current study was implemented by psychologists, the extensive detail within the intervention manual pertinent to theoretical rationale and session activities increases our confidence that school professionals (including teachers and school-based mental health providers) could integrate the intervention in the normal school routine. Indeed, provision of PPIs through the curriculum have produced support for efficacy when delivered by teachers (Froh et al. 2008), even when teachers did not receive additional training or coaching beyond written material that contained information similar to that contained in the manual developed for use in the current study (Proctor et al. 2011). Future research could compare the outcomes obtained in the current study to those yielded from research in which teachers implement the manual in an identified class (e.g., health) with various levels of coaching from mental health providers with expertise in PPIs.
Finally, future research should consider possible moderators of intervention efficacy. For example, Froh et al. (2009) found that the positive effects of their gratitude intervention were most evident in youth with lower baseline levels of positive affect. It could be that the current intervention is particularly impactful for students with particular risk factors (e.g., elevated psychopathology, family discord) or who develop additional strengths (e.g., bonds with same-age peers or group leaders) associated with participation in a group intervention.
5 Conclusions
The results of this pilot study provide some empirical support for the utility of screening all students with a brief measure of life satisfaction and intervening with those who indicate room for increases, as participation in the 10-week group counseling intervention served to improve students’ life satisfaction during the period in which they received instruction on how to change their thoughts and actions in a positive manner. Although the gains in global life satisfaction were matched by the wait-list control at follow-up, results provided valuable information for further study in terms of modifications to intervention design and target samples. Developing interventions that increase subjective well-being is consistent with the aim of positive psychology with respect to facilitating wellness in all individuals (not just those with clinical levels of problems). This project reflects a systematic effort to translate positive psychology to a real world setting: school-based mental health services. Identifying and providing PPIs to youth who report they are anything other than delighted with their lives is important given that early adolescents with both high SWB and the absence of psychopathology evidence the best outcomes across social, academic, and physical health domains (Greenspoon and Saklofske 2001; Suldo and Shaffer 2008). This study found grade-level screening to be a quick and effective means to identify students with room for improvement in their life satisfaction, and that delivery of a positive psychology group intervention at school was well-received by participating students and may be a viable means to systematically foster adolescents’ global life satisfaction.
References
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms and profiles. Burlington, VA: University of Vermont.
Boehm, J. K., & Lyubomirsky, S. (2009). The promise of sustainable happiness. In S. J. Lopez & C. R. Snyder (Eds.), Oxford handbook of positive psychology (2nd ed., pp. 667–677). New York: Oxford University Press.
Bryant, F. B., & Veroff, J. (2007). Savoring: A new model of positive experience. Mahwah, NJ: Lawrence Erlbaum Associates.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). New York: Academic Press.
Diener, E., Oishi, S., & Lucas, R. E. (2009). Subjective well-being: The science of happiness and life satisfaction. In S. J. Lopez & C. R. Snyder (Eds.), Oxford handbook of positive psychology (2nd ed., pp. 187–194). New York: Oxford University Press.
Eccles, J. S., Lord, S., & Midgley, C. (1991). What are we doing to early adolescents? The impact of educational contexts on early adolescents. American Journal of Education, 99, 521–542.
Emmons, R. A., & McCullough, M. E. (2003). Counting blessings versus burdens: An experimental investigation of gratitude and subjective well-being in daily life. Journal of Personality and Social Psychology, 84(2), 377–389.
Fan, X., & Nowell, D. L. (2011). Using propensity score matching in educational research. Gifted Child Quarterly, 55, 74–79. doi:10.1177/0016986210390635.
Froh, J. J., Kashdan, T. B., Ozimkowski, K. M., & Miller, N. (2009). Who benefits the most from a gratitude intervention in children and adolescents? Examining positive affect as a moderator. The Journal of Positive Psychology, 4(5), 408–422.
Froh, J. J., Sefick, W. J., & Emmons, R. A. (2008). Counting blessings in early adolescents: An experimental study of gratitude and subjective well-being. Journal of School Psychology, 46, 213–233.
Gilman, R., & Huebner, E. S. (1997). Children’s reports of their life satisfaction: Convergence across raters, time, and response formats. School Psychology International, 18, 229–243.
Greenspoon, P. J., & Saklofske, D. H. (2001). Toward an integration of subjective well-being and psychopathology. Social Indicators Research, 54, 81–108.
Huebner, E. S. (1991). Initial development of the Students’ Life Satisfaction Scale. School Psychology International, 12, 231–240.
Huebner, E. S. (1994). Preliminary development and validation of a multidimensional life satisfaction scale for children. Psychological Assessment, 6(2), 149–158.
Huppert, F. A., & Johnson, D. M. (2010). A controlled trial of mindfulness training in schools: The importance of practice for an impact on well-being. Journal of Positive Psychology, 5, 264–274.
Keyes, C. L. M. (2005). Mental illness and/or mental health? Investigating axioms of the complete state model of health. Journal of Consulting and Clinical Psychology, 73, 539–548.
King, L. A. (2001). The health benefits of writing about life goals. Personality and Social Psychology Bulletin, 27, 798–807.
Kosanke, J., & Bergstralh, E. (2004a). Dist: Computes a distance matrix between a set of cases and a set of potential controls. Rochester, MN: Mayo Clinic, Division of Biomedical Statistics and Informatics. Retrieved from http://mayoresearch.mayo.edu/biostat/sasmacros.cfm.
Kosanke, J., & Bergstralh, E. (2004b). Vmatch: Match cases to controls using variable optimal matching. Rochester, MN: Mayo Clinic, Division of Biomedical Statistics and Informatics. Retrieved from http://mayoresearch.mayo.edu/biostat/sasmacros.cfm.
Laurent, J., Catanzaro, S. J., Joiner, T. E., Rudolph, K. D., Potter, K. I., Lambert, S., et al. (1999). A measure of positive and negative affect for children: Scale development and preliminary validation. Psychological Assessment, 11, 326–338.
Lyubomirsky, S., Sheldon, K. M., & Schkade, D. (2005). Pursuing happiness: The architecture of sustainable change. Review of General Psychology, 9, 111–131.
Marques, S. C., Lopez, S. J., & Pais-Ribero, J. L. (2011). ‘‘Building hope for the future’’: A program to foster strengths in middle-school students. Journal of Happiness Studies, 12, 139–152.
Mazzucchelli, T. G., Kane, R. T., & Rees, C. S. (2010). Behavioral activation interventions for well-being: A meta-analysis. Journal of Positive Psychology, 5, 105–121.
McDougall, P., & Hymel, S. (1998). Moving into middle school: Individual differences in the transition experience. Canadian Journal of Behavioural Science/Revue canadienne des sciences du comportement, 30, 108–120.
Otake, K., Shimai, S., Tanaka-Matsumi, J., Otsui, K., & Fredrickson, B. L. (2006). Happy people become happier through kindness: A counting kindnesses intervention. Journal of Happiness Studies, 7, 361–375.
Park, N., Peterson, C., & Seligman, M. E. P. (2004). Strengths of character and well-being. Journal of Social and Clinical Psychology, 23, 603–619.
Park, N., & Peterson, C. (2006). Moral competence and character strengths among adolescents: The development and validation of the values in action inventory of strengths for youth. Journal of Adolescence, 29, 891–909.
Proctor, C., Tsukayama, E., Wood, A. M., Maltby, J., Eades, J. F., & Linley, P. A. (2011). Strengths gym: The impact of a character strengths-based intervention on the life satisfaction and well-being of adolescents. Journal of Positive Psychology, 6, 377–388.
Rashid, T., & Anjum, A. (2008). Positive psychotherapy for young adults and children. In J. R. Z. Abela & B. L. Hankin (Eds.), Handbook of depression in children and adolescents (pp. 250–287). New York: Guilford Press.
Schueller, S. M. (2010). Preferences for positive psychology exercises. Journal of Positive Psychology, 5, 192–203.
Seligman, M. E. P. (1990). Learned optimism: How to change your mind and your life. New York: Random House, Inc.
Seligman, M. E. P. (2002). Authentic happiness: Using the new positive psychology to realize your potential for lasting fulfillment. New York: Free Press.
Seligman, M. E. P., & Csikszentmihalyi, M. (2000). Positive psychology: An introduction. American Psychologist, 55, 5–14.
Seligman, M. E. P., Rashid, T., & Parks, A. C. (2006). Positive psychotherapy. American Psychologist, 61, 774–788.
Seligman, M. E. P., Steen, T. A., Park, N., & Peterson, C. (2005). Positive psychology progress: Empirical validation of interventions. American Psychologist, 60, 410–421.
Seligson, J. L., Huebner, E. S., & Valois, R. F. (2003). Preliminary validation of the brief multidimensional students’ life satisfaction scale. Social Indicators Research, 61, 121–145.
Snyder, C. R., Rand, K. L., & Sigmon, D. R. (2005). Hope theory: A member of the positive psychology family. In C. R. Snyder & S. J. Lopez (Eds.), Handbook of positive psychology (pp. 257–276). New York: Oxford University Press, Inc.
Suldo, S. M., & Shaffer, E. J. (2008). Looking beyond psychopathology: The dual-factor model of mental health in youth. School Psychology Review, 37, 52–68.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063–1070.
Weisz, J. R., & Kazdin, A. E. (2010). Evidence-based psychotherapies for children and adolescents (2nd ed.). New York: Guilford Press.
Acknowledgments
This work was supported, in part, by the University of South Florida Collaborative for Children, Families and Communities. The authors of this manuscript would like to acknowledge the assistance of the following members of their university research team: Amanda Thalji-Raitano, Allison Friedrich, Tiffany Stewart, Emily Shaffer-Hudkins, and Dr. Ellis Gesten.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Suldo, S.M., Savage, J.A. & Mercer, S.H. Increasing Middle School Students’ Life Satisfaction: Efficacy of a Positive Psychology Group Intervention. J Happiness Stud 15, 19–42 (2014). https://doi.org/10.1007/s10902-013-9414-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10902-013-9414-2