
Abstract
American Indian and Alaska Native Veterans are more rural than Veterans of any other race or ethnicity and face significant barriers to accessing care. Since 2001, the Tribal Veterans Representative (TVR) Program, a partnership between the U.S. Department of Veterans Affairs (VA) and tribal nations, has trained liaisons from tribal communities to facilitate access to VA benefits and services. We delineate the TVR program model alongside supporting data. We reviewed TVR training materials and program evaluations to identify components of the program essential for increasing access to VA services and benefits. We then report a quantitative assessment of benefits attained in one tribal community. The TVR model is characterized by the exchange of two sets of knowledge and resources—‘institutional’ and ‘community’—during a co-sponsored educational program aiming to train community liaisons about the institution. The institution leads the program’s content; the community’s traditions inform its process. Following the program, liaisons use support networks comprising trainers, trainees and local organizations to teach other community members to access health care and benefits. In the evaluation community, one liaison has facilitated access for hundreds of Veterans, with financial compensation exceeding $400,000 annually. The TVR program has begun to demonstrate its utility for other rural populations, though further formal evaluation is recommended. Compared with similar models to increase rural populations’ access to health care and benefits, the long-term support networks from the TVR model may be most useful when the institution must build trust and engage with the target population.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Many American Indian and Alaska Native (AI/AN) nations value military service as a means of serving one’s community, and of honoring service members who preceded them [1,2,3]. They venerate Veterans during community events and hold special events for returning service members. These rich traditions facilitate Veterans’ re-integration into the community and instill a sense of duty [1,2,3], which in part drives AI/ANs’ high rates of participation in the military relative to other groups [4], rendering them the most over-represented minority race among Veterans [5].
Not only are AI/AN Veterans over-represented, they have disproportionately filled dangerous military roles and endured the consequences. According to the 2010 National Survey of Veterans, AI/AN-only Veterans are more likely than all Veterans to serve in combat (48% vs. 34%), and to be exposed to “dead, dying or wounded” (also 48% vs. 34%) [6]. Greater exposure to warzone stress accounts for a prevalence of post-traumatic stress disorder (PTSD) in male AI/AN Vietnam Veterans that is 2–2.5 times that for male white Vietnam Veterans [7]. AI/AN-only Veterans are also more likely than white Veterans to be “definitely” or “probably” exposed to environmental hazards (38% vs. 23% overall), and less likely to report good-to-excellent health (59% vs. 74%) [6]. Poverty and unemployment rates for AI/AN Veterans are higher than all other Veteran groups [5, 8]. These disparities underscore the need to address health and its social determinants in AI/AN Veterans.
Like all eligible Veterans, AI/AN Veterans have earned the right to benefits and services from the U.S. Department of Veterans Affairs (VA), including healthcare from the Veterans Health Administration (VHA); financial compensation, education and housing assistance, transportation reimbursement for medical care from the Veterans Benefit Administration (VBA); and cemetery and burial benefits from the National Cemetery Administration (NCA). Yet, despite their record of service, AI/AN Veterans are the least likely to use VA benefits relative to Veterans of other single races [9]. Part of this discrepancy could be related to some AI/AN Veterans’ use of Indian Health Service (IHS) care in place of VHA care [10]. However, AI/AN Veterans are also more likely than white Veterans to lack any kind of health care coverage (21% vs. 8%), even after considering government programs like Medicare and IHS [6]. More likely, this discrepancy is due to location and cultural barriers.
AI/AN VHA patients are more likely than patients of any other race to live in rural or highly rural areas (e.g., 53.5% vs. 43.7% for white VHA patients) [11]. Rural AI/AN Veterans face even greater barriers to accessing VHA care than rural non-AI/AN Veterans [12, 13]. Rural residence is compounded by other barriers to VHA care among AI/AN Veterans, including difficulty navigating the VA system, difficulty discussing personal matters, lack of trust of the VA system, an inflexible VA system, lack of culturally competent care, and lack of outreach to American Indian communities [1, 14].
The Tribal Veterans Representative (TVR) program arose in 2001 in the Northern Plains from conversations between VA employees and tribes that revealed serious barriers to VA care and benefits for rural AI/AN Veterans. The TVR program, a peer liaison program organized by the Veterans Integrated Service Network (VISN) 19 Minority Outreach Coordinator in collaboration with cosponsoring tribes, was developed with the goal of improving rural AI/AN Veterans’ access to the VA system. Since its inception, the TVR program has continued to evolve in collaboration with AI/AN communities, becoming a national model for Veteran outreach and access. Although the program has been described previously [15], it has never formally been codified, and its direct impact linking AI/AN Veterans to benefits has not been examined. In this paper we review the available data from the internal program evaluation in order to describe the unique characteristics of the model and examine the impact of the TVR program. In the discussion, we consider the model’s utility for other populations, particularly rural and underserved populations.
Methods and Results
We derive a model of the TVR program by reviewing materials collected since its inception and through our own participation in the program as observer, coordinator and trainer. Two authors catalogued all materials, including training agendas, handouts, presentations, press releases, media interviews, newspaper articles, white papers, and internal evaluations instituted for programmatic feedback and improvement. Internal evaluations included an analysis of TVR activities in one tribal community, and a report of key lessons learned from semi-structured interviews with nine senior TVRs in 2016. At the time of analysis, all authors had attended between 3 and 38 TVR training sessions. Differences in model conceptualization were discussed until consensus was reached.
To examine the TVR program’s impact, we separately report the analysis of TVR activities in one tribal community. Methods were carried out as quality assurance and did not meet the definition of research according to regulations set by the U.S. Department of Health and Human Services.
The TVR Program Model
The TVR program prepares representatives from different tribal nations to help their peers obtain VA benefits and services. Although trainees can be any member of the public, most are Veterans and family members who have been nominated by their tribes, or are VA, IHS and tribal health employees who encounter AI/AN Veterans through service work.
Trainees attend a weeklong training course offered in rural locations around the country. Training relays the most recent information about VA policies and programs. During training week cosponsoring or other local tribes guide rituals (e.g., talking circles and ceremonies), provide training facilities, and invite trainees to their nations’ cultural events.
When trained TVRs return to their communities, they assist Veterans and their family members in enrolling in VA health care and navigating VA benefits. They also frequently join or host local outreach events, such as benefits fairs and stand-downs.
Other projects and programs for rural AI/AN Veterans have partnered with and drawn from the TVR program, including a Veterans Transportation Service, a Veterans Tribal Clinic, a Veterans Resource Center, and VA American Indian Telemental Health Clinics [15]. Some VA facilities incorporated cultural healing spaces, such as sweat lodges and medicine wheel gardens. The VA Office of Tribal and Government Relations arose in part from a need identified by the TVR program for support developing policies and building relationships among governing bodies. (please see Kaufmann et al. [15] for more detail).
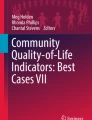
The theoretical model is shown in Fig. 1. Each element—community-specific knowledge and resources, institution-specific knowledge and resources, education of community-based liaisons, and community action—feeds forward into the next. TVRs and partnering tribal nations contribute culture- and community-specific knowledge and resources—an understanding of rural AI/AN Veterans’ needs, of how to connect with rural AI/AN Veterans, and of community resources (e.g., local health facilities, Veterans organizations). VA provides institution-specific knowledge and resources—infrastructure like medical facilities, services and benefits for rural AI/AN Veterans, and knowledge about how to access them. These sets of ‘insider’ resources meld at an in-person TVR training (education of community-based liaisons), an event further shaped by cultural activities like ceremonies, talking circles, community dinners and dances. Following training TVRs apply their new knowledge to increase access for all Veterans in their community, often rural AI/AN Veterans. This community action yields new information that feeds back into the system, deepening community and institutional knowledge. Throughout the process the VISN 19 Minority Outreach Coordinator facilitates communication pathways between TVRs and VA. Descriptions of each element are elaborated in the following sections.

Diagram of the tribal veterans representative program model
Community-Specific Knowledge and Resources
As both community members and Veterans (or family members of Veterans), TVRs see the gestalt of local Veteran culture. Their personal experience as tribal members and patients at local VA, IHS, or tribal health facilities and their connections with other local Veterans and community resources (e.g., Veterans service organizations, churches, local colleges, tribal leadership, elderly services, public safety) provide this comprehensive perspective. TVRs know where to find Veterans in need of services. They also understand reasons Veterans forego VA benefits, including prioritizing other Veterans’ needs over their own, distrust of government agencies in rural and tribal areas, concerns about privacy, and being declined for care due to misunderstandings among VA and IHS staff. Yet, despite having valuable community-specific knowledge, TVRs seek detailed guidance navigating VA.
Institution-Specific Knowledge and Resources
Institution-specific knowledge and resources include infrastructure (e.g., medical facilities), benefits, and services, as well as ‘insider’ understanding of VA operations (e.g., how benefits claims are evaluated, new policies). ‘Insider’ knowledge is generally available to the public but might be difficult to find among overwhelming amounts of information for Veterans, or to see relevance for individual Veterans.
Education of Community-Based Liaisons
TVR training integrates institution- and community-specific knowledge and resources. Trainers are VA leaders, VA subject matter experts, local organization representatives, and senior TVRs; trainees are Veterans, family members, VA providers, and VA staff. Together they possess a mix of institutional and community knowledge. Training catalyzes knowledge transfer.
The training process (Table 1) encourages each trainee to sow a support network of peers and trainers. Training content emphasizes new and updated VA policies and programs, delivers actionable knowledge about services and benefits, and explains adjudication of claims. Trainees have access to online presentation materials and a comprehensive TVR Resource Guide [16] containing updated claims forms, fact sheets, and links to VA Web pages.
TVR training distinguishes itself from other trainings offered by VA because it is shaped by community culture and tradition. Hosting nations invite the Minority Outreach Coordinator to offer a training. They collaborate on preparations, including planning ceremonies [17]. Hosting nations recruit spiritual leaders to guide opening and closing talking circles, color guards or drum groups to lead the opening ceremony to honor Veterans, and local organizations to present services relevant to Veterans. In addition to facilitating knowledge transfer to participants, the hosting nation’s involvement enables VA to show respect for tribal traditions. Health care providers have observed that their participation in TVR training improves their delivery of culturally appropriate services to AI/AN Veterans.
Community Action
After training, TVRs apply their integrated knowledge to increase Veterans’ access to benefits and services, relying on their networks for support [18]. They reach out to Veterans, learn their needs, teach them to file claims, advocate, arrange transportation to health and benefits appointments, and visit ailing Veterans and their families. Still, translating training to community action carries separate challenges of engaging Veterans and tailoring assistance to their unique needs.
A set of best practices for community action emerged among experienced TVRs (Table 2). Outreach to Veterans requires initiative and tactful persistence. To engage fellow Veterans, TVRs may share their own stories of enrolling in VHA, narratives that often entail an initial reluctance to work with VA, followed by improvements in quality of life after receiving health care and benefits. TVRs’ openness and honesty counters distrust among Veterans who may need services but resist engaging with VA. Establishing trust maintains engagement when VA denies a request or asks for more information, which extends processing time and can lead to feelings of frustration and rejection. Ultimately, TVRs’ expertise grows from striving to help multiple Veterans with diverse requests, as the needs of two Veterans are rarely alike. When TVRs encounter new situations, they seek guidance from their support network. Seasoned TVRs note that their network includes the VISN 19 Minority Outreach Coordinator, who has advised on the most difficult challenges. The Coordinator’s continuous support of TVRs’ community activities helps ensure that future trainings address ongoing issues for Veterans.
Feedback Loop
Recurrent TVR trainings reinforce existing knowledge and disseminate policy updates, but they also are a key method for adding new knowledge into the system. During these follow-up trainings, returning TVRs share stories of their activities in the field, request presentations on field-related issues, and identify areas for improvement in VA policy. For example, at one training a TVR explained that travel reimbursement for medical appointments aids only those Veterans who can afford to wait for reimbursement. He shared how his community initiated a travel fund that Veterans could borrow from in advance of their travel, and then repay when VA reimbursed them. Not only does this example demonstrate how follow-up trainings leverage new knowledge from experienced TVRs, it also shows how tribal communities can respond nimbly to issues facing Veterans.
TVRs who have been most active in their communities anecdotally report substantial benefits to hundreds of Veterans, including improved health, increased self-esteem, strengthened family ties, family assistance, and monetary compensation. These benefits are difficult to quantify because, as volunteers, TVRs are not required to log their work; however, one TVR had recorded his activities, offering an opportunity to measure benefits in one community.
Evaluation of TVR benefits and services delivered in one tribal community
We partnered with one tribal nation, headquartered on a reservation in the western United States, to quantify benefits obtained during TVR program activity, and to assess economic impacts for Veterans in the community. This nation retains one active TVR who has volunteered since 2002 and constitutes the community’s TVR program.
The TVR’s records included completed claims forms, contact logs, and one summary report of requests for health care, benefits, and burials and memorials. From these records, we estimate the number of Veterans served, number and types of requests filed with VA, and financial benefits. Regarding the number of Veterans served and requests filed, we counted any degree of assistance or guidance provided to the Veteran. Many Veterans included in these data might have briefly consulted the TVR before completing the benefits process relatively independently. Level of assistance provided is not considered, as the aim of the TVR program is for TVRs to teach Veterans to access their own benefits and services. With respect to financial benefits, assessment is limited to compensation for service-connected disabilities (i.e., an injury or illness incurred or aggravated during active military service) because estimates were feasible from the available data. Tribal Council permission was obtained to publish the program’s descriptive results.
We found that between 2002 and 2016, one TVR assisted approximately 300 Veterans with 403 requests for VA benefits, health care, funeral support, and other information. Most requests (n = 337) were for benefits or services beyond information solicitation, therefore required a decision by VA. Of the 222 (66%) requests where a decision was known, about every 4 out of 5 were approved, after taking reconsideration and appeal into account. The remaining claims were still under consideration at the time of the review or were not pursued further due to the Veteran’s wishes. Inability to determine outcome for a third of claims was due to the voluntary nature of TVR activities: Veterans are ultimately responsible for corresponding with VA and do not always debrief TVRs on claim decisions.
Table 3 displays the wide range of benefits and services sought with TVR assistance. The most common types of claims were for health benefits, followed by service-connected disabilities, headstones, flags for funerals, and compensation for dependents. Claims for cemetery benefits were most likely to be approved. For claims that were denied, the TVR offered the Veteran assistance with the appeal. The outcome of many of the 40 appeals filed is unknown, as several were pending at the time of evaluation.
Between 2002 and 2016 financial compensation to Veterans with service-connected disabilities (n = 39) is estimated to total $6.3 million. This estimate is likely conservative: when the exact rating for a disability was unknown, the lowest of possible ratings was assumed.
A number of activities were beyond the scope of the evaluation but appeared in the TVR’s logs, highlighting the role of improving access to care and benefits in TVR activities. Such activities include assisting Veterans with obtaining appointments and transportation, scheduling Compensation & Pension exams (to determine the extent of a service-connected disability), calling VA and other agencies on the Veteran’s behalf, obtaining travel reimbursements, and house calls to discuss Veterans’ concerns.
Discussion
Evaluation of one tribal community’s TVR program shows how one TVR assisted Veterans and their family members with a wide range of requests for VA benefits and services, reflecting both the TVR’s broad knowledge base and his ability to adapt assistance to Veterans’ complex needs. The TVR also facilitated Veterans’ procurement of millions of dollars in earned compensation. In fiscal year 2015, the average annual service-connected disability compensation rate for Veterans receiving TVR assistance in this community exceeded $20,000, higher than the average annual compensation rate of $14,444 for all U.S. Veterans [19]. With respect to health care services, the TVR helped Veterans file a total of 113 claims for health benefits, financial assistance for in-home care, vocational rehabilitation, prosthetics, and health-related home improvements. When determinable, approximately 90% of these claims were successful. In addition, the TVR’s support at all stages of the application process, including appeals, is noteworthy considering that it could have ameliorated the process, one which most Veterans find stressful [20, 21].
As this evaluation aimed to assess the influence of one community with an active TVR, results cannot be generalized to other TVRs or communities. Other limitations include the retrospective uncontrolled design. A control community or pretest period was precluded by the absence of claims records in communities without active TVRs, with only anecdotes from the evaluation community to suggest that far fewer Veterans received VA health services and benefits before the TVR program began. Nonetheless, Veterans who sought TVR assistance received over $5000 more in disability compensation annually relative to national data from fiscal year 2015 [19]. Thus, the present evaluation supports the TVR program’s favorable influence on rural AI/AN Veterans’ access to VA care and benefits, as the TVR model posits. Controlled investigation is needed to understand whether TVR activities explain this higher rate of compensation, and to explore potential confounding factors like severity of service-connected disabilities, as well as age and service era.
The TVR model recognizes the extent to which the rural AI/AN community and VA system are ordinarily isolated from each other, and grasps the value of both community and institutional assets. It facilitates exchange of these assets through joint, culturally-shaped education, and empowers community liaisons to teach rural Veterans to access their services and benefits. A number of systematized models exist for increasing rural and underserved populations’ access to health care and benefits. e.g., [22,23,24,25] Table 4 compares the TVR model with other select models, most of which were developed specifically to increase Veterans’ access to benefits. ‘Outreach models’ (Rural Veterans Outreach [22], Stand Downs [25], Veterans Benefits Fairs and Reaching Rural Veterans [24]) involve a community-led or joint VA-community effort to pool resources (state, university, federal, nonprofit) for Veterans that culminates in an outreach event. ‘Liaison models’ (TVR and Promotora [23, 26,27,28,29,30,31]) train representatives from a target population to connect other members of the target population with care or benefits from an institution, culminating in community service by liaisons.
Of the outreach models, the TVR program most closely resembles Rural Veterans Outreach [22]. Both models center on an event that is co-sponsored by VA and the community and hinge on the VA learning about the community early in the partnership. In the Rural Veterans Outreach model, partnerships and capacity are built at the community-level, while the TVR model builds individual TVRs’ support networks. Hence, selection between models may depend on whether the community wants to achieve sustainment through its local organizations or through its individual members.
Though similar to the Promotora (‘liaison’) model [26,27,28,29,30,31], the TVR model seems uniquely suited for target populations that have complex relationships with the institution, or reasons to distrust it. The training process includes an active role for cultural tradition that serves to educate the institution and honor the culture. As volunteers, TVRs act independently of the institution, countering doubts about whether actions are in the Veterans’ best interest. Support networks formed during training and strengthened through community service and subsequent trainings are lasting, with the Minority Outreach Coordinator ensuring the effort’s success. Indeed, some TVRs have served since the program’s inception in 2001. The TVR model has maintained high fidelity under leadership of the Minority Outreach Coordinator. On the other hand, it resides within one health care system while the Promotora model has been adapted across many systems.
Conclusions
Evaluation of preliminary data shows promise of the TVR model for increasing rural Veterans’ access to health care and benefits. In comparison to similar models, the TVR model seems particularly promising in instances where the community has a complex relationship with the institution. Evaluators examining volunteer versus paid roles of community health workers may be interested in further assessment of the TVR program’s retention and cost effectiveness. The TVR program’s success pivots on the commitment of its individual TVRs and its program coordinator, a consideration for any adaptation.
TVRs are proving essential partners to VA and Veterans. The lessons of TVRs are likely useful to programs striving to reach hard-to-reach groups. Though designed for AI/AN populations, the TVR program has been adapted and used in at least one non-AI/AN population.
Selecting an appropriate model for reaching rural and underserved Veterans may depend on the partner level (i.e., organizations vs individuals), the community’s trust of the institution, the specific needs of the population being served, and the degree to which the institution needs to initiate the partnership. With its unique strength in long-term partnerships, the TVR model is a valuable approach to connecting other rural and underserved populations with health care.
References
Kaufman, C. E., Kaufman, L. J., Shangreau, C., Dailey, N., Blair, B., & Shore, J. (2016). American Indian Veterans and VA services in three tribes. American Indian and Alaska Native Mental Health Research, 23(2), 64–83. https://doi.org/10.5820/aian.2302.2016.64.
Ledesma, R. (2006). Entrance and exit from the military. Journal of Ethnic & Cultural Diversity in Social Work, 15(1–2), 27–53. https://doi.org/10.1300/J051v15n01_02.
Ward, C. J., Cope, M. R., & Elmont, L. (2017). Native American Vietnam-era Veterans’ access to VA healthcare: Vulnerability and resilience in two Montana reservation communities. Journal of Community Health, 42(5), 887–893. https://doi.org/10.1007/s10900-017-0330-y.
Office of the Under Secretary of Defense, Personnel and Readiness. (2017). Population representation in the military services: Fiscal Year 2016. Table D-27: American Indian/Alaskan Native non-prior service (NPS) active component enlisted accessions and corps by service with civilian comparison group, FYs 2003-2016. Retrieved from https://www.cna.org/pop-rep/2016/.
National Center for Veterans Analysis and Statistics. (2017). Profile of Veterans: 2015. Data from the American Community Survey. Retrieved from https://www.va.gov/vetdata/docs/SpecialReports/Profile_of_Veterans_2015.pdf.
Westat. (2010). National Survey of Veterans, Active Duty Service Members, Demobilized National Guard and Reserve Members, Family Members, and Surviving Spouses. Final Report. Retrieved from https://www.va.gov/vetdata/docs/SurveysAndStudies/NVSSurveyFinalWeightedReport.pdf.
Beals, J., Manson, S. M., Shore, J. H., et al. (2002). The prevalence of posttraumatic stress disorder among American Indian Vietnam Veterans: Disparities and context. Journal of Traumatic Stress, 15(2), 89–97. https://doi.org/10.1023/A:1014894506325.
Office of Data Governance and Analytics. (2017). Minority Veterans report: Military service history and VA benefit utilization statistics. Washington, DC: US Department of Veterans Affairs.
National Center for Veterans Analysis and Statistics, Office of Policy and Planning. (2016). Unique Veteran users profile: FY 2015. Washington, DC: US Department of Veterans Affairs.
Kramer, B., Vivrette, R., Satter, D., Jouldjian, S., & McDonald, L. (2009). Dual use of Veterans Health Administration and Indian Health Service: Healthcare provider and patient perspectives. Journal of General Internal Medicine, 24(6), 758–764. https://doi.org/10.1007/s11606-009-0962-4.
Office of Health Equity. (2016). National Veteran health equity report—FY 2013. Washington, DC: US Department of Veterans Affairs.
Brooks, E., Kaufman, C., Nagamoto, H. T., Dailey, N. K., Bair, B. D., & Shore, J. (2015). The impact of demographic differences on Native Veterans’ outpatient service utilization. Psychological Services, 12(2), 134–140. https://doi.org/10.1037/a0038687.
Kaufman, C. E., Brooks, E., Kaufmann, L. J., et al. (2013). Rural Native Veterans in the Veterans Health Administration: Characteristics and service utilization patterns. Journal of Rural Health, 29(3), 304–310. https://doi.org/10.1111/j.1748-0361.2012.00450.x.
Westermeyer, J., Canive, J., Thuras, P., Chesness, D., & Thompson, J. (2002). Perceived barriers to VA mental health care among upper Midwest American Indian Veterans: Description and associations. Medical Care, 40(Suppl 1), 62–70.
Kaufmann, L. J., Richardson, W. J., Floyd, J., & Shore, J. (2014). Tribal Veterans Representative (TVR) training program: The effect of community outreach workers on American Indian and Alaska Native Veterans’ access to and utilization of the Veterans Health Administration. Journal of Community Health, 39(5), 990–996. https://doi.org/10.1007/s10900-014-9846-6.
Richardson, W. J. (2016). Tribal Veteran representative resource guide. Washington, DC: Department of Veterans Affairs Employee Education System.
Niedo, D. (2016). Where are we and where are we going? Tribal Veteran Representative Resource Guide. Washington, DC: Department of Veterans Affairs Employee Education System.
Niedo, D., & Wadda, L. (2016). Role of the tribal Veterans representative (TVR). Tribal Veteran represenative resource guide. Washington, DC: Department of Veterans Affairs Employee Education System.
U.S. Department of Veterans Affairs, Veterans Benefit Administration. (2016). Compensation: Service-connected disability or death benefits. Retrieved from https://www.benefits.va.gov/REPORTS/abr/ABR-Compensation-FY15-05092016.pdf.
Rosen, M. I. (2010). Compensation examinations for PTSD—an opportunity for treatment? Journal of Rehabilitation Research and Development, 47(5), xv–xxii.
Spoont, M., Greer, N., Su, J., et al. (2011). Rural vs. urban ambulatory health care: A systematic review (VA-ESP Project #09-009). Washington, DC: US Department of Veterans Affairs.
Veterans Rural Health Resource Center-Salt Lake City, Office of Rural Health. (2018). Rural Veteran outreach toolkit & workbook v30. Washington, DC: U.S. Department of Veterans Affairs.
Verhagen, I., Steunenberg, B., de Wit, N. J., & Ros, W. J. (2014). Community health worker interventions to improve access to health care services for older adults from ethnic minorities: A systematic review. BMC Health Services Research, 14, 497. https://doi.org/10.1186/s12913-014-0497-1.
Sternberg, M., Wellnitz, A., Wright, B., Eicher-Miller, H., Topp, D., & MacDermid Wadsworth, S. (2016). Reaching rural Veterans: Engaging faith-based food pantries in serving low-income, homeless, and at-risk Veterans in rural areas. West Lafayette: The Military Family Research Institute at Purdue University.
National Coalition for Homeless Veterans. (2014). Stand down promising practices. Washington, DC: National Coalition for Homeless Veterans.
Shommu, N. S., Ahmed, S., Rumana, N., Barron, G. R., McBrien, K. A., & Turin, T. C. (2016). What is the scope of improving immigrant and ethnic minority healthcare using community navigators: A systematic scoping review. International Journal for Equity in Health, 15, 6. https://doi.org/10.1186/s12939-016-0298-8.
Hou, S. I., & Roberson, K. (2015). A systematic review on US-based community health navigator (CHN) interventions for cancer screening promotion–comparing community—versus clinic-based navigator models. Journal of Cancer Education, 30(1), 173–186. https://doi.org/10.1007/s13187-014-0723-x.
Zulu, J. M., Kinsman, J., Michelo, C., & Hurtig, A. K. (2014). Integrating national community-based health worker programmes into health systems: A systematic review identifying lessons learned from low-and middle-income countries. BMC Public Health, 14, 987. https://doi.org/10.1186/1471-2458-14-987.
Koskan, A. M., Friedman, D. B., Brandt, H. M., Walsemann, K. M., & Messias, D. K. (2013). Preparing promotoras to deliver health programs for Hispanic communities: Training processes and curricula. Health Promotion Practice, 14(3), 390–399. https://doi.org/10.1177/1524839912457176.
O’Brien, M. J., Squires, A. P., Bixby, R. A., & Larson, S. C. (2009). Role development of community health workers: An examination of selection and training processes in the intervention literature. American Journal of Preventive Medicine, 37(6 Suppl 1), S262–S269. https://doi.org/10.1016/j.amepre.2009.08.011.
Islam, N. S., Zanowiak, J. M., Riley, L., Nadkarni, S. K., Kwon, S. C., & Trinh-Shevrin, C. (2015). Characteristics of Asian American, Native Hawaiian, and Pacific Islander community health worker programs: A systematic review. Journal of Health Care for the Poor and Underserved, 26(2 Suppl), 238–268. https://doi.org/10.1353/hpu.2015.0062.
Acknowledgment
We are most grateful to the Tribal Veterans Representatives and communities who have partnered in this program.
Funding
Funding provided by the U.S. Department of Veterans Affairs (VA) Office of Rural Health (ORH). Visit www.ruralhealth.va.gov to learn more. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the U.S. Department of Veterans Affairs (VA).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Goss, C.W., Richardson, W.J. & Shore, J.H. Outcomes and Lessons Learned from the Tribal Veterans Representative Program: A Model for System Engagement. J Community Health 44, 1076–1085 (2019). https://doi.org/10.1007/s10900-019-00683-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-019-00683-0