
Abstract
While the majority of viral hepatitis is experienced in the developing world, migration of people from high prevalence countries contributes to health outcomes in the United States. The purpose of this study was to estimate the prevalence of hepatitis B virus (HBV) and hepatitis C virus (HCV) infection in foreign-born immigrants living in the Baltimore-Washington metropolitan area. This study used cross-sectional data from 5982 individuals screened at community events held from 2009 to 2015. Descriptive statistics were generated to describe the screening results. Positive results for HBV infection (HBsAg+) and HCV infection (HCVAb+) were analyzed according to age, gender, and country of birth. Of 5982, the majority of participants were born in Asia (77.8%). The prevalence of infection was 6.1% for HBV and 3.8% for HCV in Asia-born immigrants compared to 3.7% for HBV and 2.8% for HCV in Africa-born immigrants. Among participants who were Asia-born, prevalence of HBV infection was highest for those from Cambodia (11.9%) compared to Vietnam (8.2%), China (8.1%), Laos (6.1%), and Korea (4.6%). Among participants who were Africa-born, prevalence of HBV was highest for those from Liberia (6.7%) and Sierra Leone (6.7%), followed by Cameroon (4.4%) and Nigeria (4.2%). The highest HCV prevalence occurred among those from Cambodia (10.8%) and Myanmar (4.9%) in Asia and those from Cameroon (11.4%) and Nigeria (4.8%) in Africa. This study suggests that screening data are disaggregated by country of birth, then improvements can be made to programs for prevention, earlier diagnosis, and linkage to care.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatocellular carcinoma (HCC) ranks second in cancer mortality worldwide [1]. HCC especially impacts less developed regions where 83% of the estimated 782,000 new cases of HCC worldwide occurred in 2012 [1]. Most cases of primary liver cancer (estimated 78%) are caused by chronic hepatitis B virus (HBV) or hepatitis C virus (HCV) infection [2]. Worldwide prevalence of chronic HBV infection is estimated at 257 million and of HCV infection is estimated at 130–170 million [2].
The majority of viral hepatitis is experienced in the developing world. Individuals living in the United States who have HBV or HCV have an increased likelihood of having migrated from a high prevalence region. Of the foreign-born U.S. residents with chronic HBV infection, the majority (58%) were born in Asia, and 11% were born in sub-Saharan Africa [3]. This also includes, in particular, Central and East Asia and North Africa, regions which are estimated to have high prevalence of HCV (> 3.5%), and South and Southeast Asia and sub-Saharan Africa, regions which have moderate prevalence of HCV (1.5–3.5%) [4].
Current epidemiological information for HBV and HCV infection in U.S. immigrants is limited and there is inadequate data about infection prevalence among immigrant populations who are from endemic areas. Moreover, little is known about the disaggregated distribution of HBV and HCV infection among subpopulations of Asian- and African-born immigrants. Current guidelines recommend HBV screening for persons with high risk for infection, but routine testing has not been initiated. Because HBV infection is preventable by vaccination, disaggregation of HBV infection demographic data is beneficial for targeted prevention against liver cancer. Because HCV can now be cured with a recently approved drug, education and early detection is important to reduce HCV transmission and complications.
To fill the information gaps, this report uses community-based screening data to estimate the prevalence of HBV and HCV infection within Asian- and African-born immigrants in the Baltimore-Washington Metropolitan area. In particular, we aimed to determine the prevalence for specific subpopulations in order to better estimate of the burden of viral hepatitis in the United States. Knowing this information can help guide HCC prevention and targeted screenings efforts for HBV and HCV.
Methods
Data Collection
The Hepatitis B Initiative of Washington, DC (HBI-DC), is a community-based organization founded in 1996 to prevent liver diseases caused by viral hepatitis in high-risk immigrant groups. Through collaborative partnerships, HBI-DC provides education, free viral hepatitis screenings, hepatitis B vaccination, and patient navigation services for impacted communities. From November 2009 to December 2015, HBI-DC organized free screening events at churches, temples, health fairs, and community centers in the Baltimore-Washington metropolitan area (Maryland, northern Virginia, and Washington, D.C.).
By following community-based participatory research principles, HBI-DC worked with community leaders to develop recruitment strategies. Linguistically- and culturally-tailored flyers were designed to announce the events and were posted in prominent locations in the community. The events were also publicized by local ethnic radio stations and newspapers.
On the day of the events, screening staff included community partner representatives, bilingual volunteers, and trained phlebotomists. Health educators were also present to provide further information about chronic hepatitis infection and the importance of hepatitis B vaccinations based on screening results. Event participants ages 18 and over were consented and given a brief intake form about their demographic information, which included questions about country of birth, age, and sex. They were asked in either English or in their native languages (e.g., Chinese, Korean, Vietnamese). Free on-site HBV and HCV testing was then administered by the phlebotomists. Participants were contacted within 2–3 weeks with their results. This study was approved by The George Washington University’s Institutional Review Board.
Measures
Serology results included status of hepatitis B surface antigen (HBsAg), hepatitis B surface antibody (anti-HBs), and hepatitis C antibody (anti-HCV). For HBV screening, participant results were divided into one of three groups as follows: (a) HBV infected (positive HBsAg); (b) susceptible to HBV infection (negative HBsAg and negative anti-HBs); or (c) immune to HBV infection (negative HBsAg and positive anti-HBs). Participants who were positive for anti-HCV also had results for reflex HCV RNA quantitative testing through reverse transcription polymerase chain reaction assay (RT-PCR). The sensitivity threshold for HCV RNA was 15 IU/mL.
Analysis
Descriptive statistics were generated to describe the screening results. Positive results for HBV infection (HBsAg+) and HCV infection (HCVAb+) were analyzed according to age, gender, and country of birth. The prevalence of sample subpopulations was further calculated for birth countries represented by at least 30 participants. All statistical analysis was performed with Stata, version 14 (StataCorp LLC).
Results
A total of 5982 adults older than 18 years participated in the screenings. A majority of participants were born in Asia (77.8%), Africa (11.4%), and North America (7.8%). Of those Asian-born, the majority were from Vietnam (24%), China (22.8%), Myanmar/Burma (22.5%), and Korea (16.9%). Of those African-born, the majority were from Ethiopia (31.6%), Nigeria (13.9%), Cameroon (9.9%), and Ghana (8.9%). About 5% of participants were from Sierra Leone, Liberia, and Togo. Of the participants who were born in North America, about two-thirds (62.7%) were U.S.-born, followed by El Salvador (16.3%) and Mexico (9.2%) (Table 1).
A total of 5762 individuals underwent HBV screening and 5.3% of them were found to be infected with HBV. Prevalence of HBV was higher in those born in Asia (6.1%) and in those born in Africa (3.7%) compared to those born in the United States (< 1%) (Table 2).
Individuals who were born in the United States had the highest rate of unprotected from HBV (58.1%) and the lowest rate of protected from HBV (40.9%), compared to those foreign-born immigrants (p < .001) (Table 2). Males were statistically more likely to be infected with HBV than females (6.3% vs. 4.2%; p < .001), and participants in their 40 s had highest prevalence of HBV infection (6.5%) followed by those in their 30 s (6.0%) and in their 50 s (5.5%; p < .004) (Table 3).
A total of 3351 underwent HCV screening and 3.5% of them were found to be sero-positive for HCV antibody. Prevalence of HCV was higher among those born in Asia (3.8%), followed by those born in the United States (3.2%) and Africa (2.8%). The prevalence of HCV infection was particularly higher among those older than 70 years old (6.5%) compared to the other age groups (range 1.3–4.1%, p < .007) (Table 3).
The prevalence of HBV or HCV infection also varied by country of origin (Table 4). Among Asia-born participants, prevalence of hepatitis infection was significantly higher for Cambodians (11.9% HBV; 10.8% HCV) than other individuals born in Asia. For other Asia-born participants, the prevalence of HBV infection and HCV infection was as follows: Vietnamese (8.2%; 4.4%), Chinese (8.1%; 0.4%), Laotian (6.1%; 3.0%), and Koreans (4.6%; 1.0%). There was also a high prevalence of HCV infection among Burmese (4.9%) and Asian Indian (4.1%) participants. Among Africa-born participants, the highest HBV prevalence occurred among those from Liberia (6.7%) and Sierra Leone (6.7%), followed by Cameroon (4.4%) and Nigeria (4.2%); and the highest HCV prevalence occurred among those from Cameroon (11.4%), followed by Nigeria (4.8%).
Discussion
Our findings estimate the chronic HBV and HCV prevalence in immigrants of the Baltimore-Washington Metropolitan area. Our findings on HBV and HCV prevalence differed from other studies with community screening data. These differences between our study’s and other studies’ findings may be due to the varied ethnicities within sample population, socioeconomic differences between populations of different U.S. cities, and screening recruitment method.
For HBV, our finding of 6.1% prevalence among Asian Americans was similar to studies in Los Angeles, California (5.3%), but lower compared to studies in New York City (13%) and Houston, Texas (13.6%) [5,6,7]. Our finding of 3.7% HBV prevalence among African immigrants was lower than studies in New York City (9.3%) and Chicago, Illinois (8%) [8, 9]. When we disaggregated our data by country of birth, the prevalence of HBV infection was highest among immigrants from Cambodia, Vietnam, and China, similar to other studies that also showed prevalence for individuals from these countries [3]. Of the African countries, Sierra Leone and Liberia had the highest HBV prevalence (6.7% each), which is lower than that of a prior meta-analysis (16.5% from Liberia; 11.9% from Sierra Leone) [3].
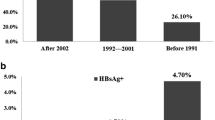
For HCV, our finding of 3.8% prevalence in Asian immigrants was lower the 6.0% prevalence in Asian Americans studied in Houston, Texas [6]. We were unable to find any studies examining HCV prevalence in African immigrants. Our findings also revealed that individuals older than 70 years old had a much higher HCV infection prevalence than the other age groups, which may be due to the lack of universal screening for HCV in blood donors before 1992. The majority of HCV infections in the United States are a result of infected blood transfusions before 1992, which likely accounts for the higher rates of chronic HCV infection among older populations in the US [10]. Further research is required to compare HCV-infected African immigrants living in different U.S. regions.
Our study had some limitations. In order to collect a sample of foreign-born immigrants, our data set was based on non-probability sampling methods through community screenings. As a result, our findings may not be representative of the entire population of foreign-born Asian and African Americans of the Baltimore-Washington metropolitan area. However, this sampling method allowed for a large recruitment of participants from a hard-to-reach immigrant population. Our strategies may have also resulted in an underestimation of HBV and HCV infection prevalence. Individuals who already knew that they were infected might have been less likely to participate in community screenings. Our findings may represent a conservative estimate of HBV and HCV prevalence due to this selection bias.
Our findings imply that immigrants from Asia and Africa uniquely differ in HBV and HCV infection prevalence than the general population. The prevalence of viral hepatitis infection also differs for populations depending on their country of birth. This suggests that more culturally-integrated intervention programs are needed to reduce the complications caused by chronic HBV or HCV infection among high-risk immigrant communities.
References
Ferlay, J., et al. (2015). Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. International Journal of Cancer, 136(5), E359–E386.
Perz, J. F., Armstrong, G. L., Farrington, L. A., Hutin, Y. J., & Bell, B. P. (2006). The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. Journal of Hepatology, 45(4), 529–538.
Kowdley, K. V., Wang, C. C., Welch, S., Roberts, H., & Brosgart, C. L. (2012). Prevalence of chronic hepatitis B among foreign-born persons living in the United States by country of origin. Hepatology, 56(2), 422–433.
Mohd Hanafiah, K., Groeger, J., Flaxman, A. D., & Wiersma, S. T. (2013). Global epidemiology of hepatitis C virus infection: New estimates of age-specific antibody to HCV seroprevalence. Hepatology, 57(4), 1333–1342.
Pollack, H. J., Kwon, S. C., Wang, S. H., Wyatt, L. C., & Trinh-Shevrin, C. (2014). Chronic hepatitis B and liver cancer risks among Asian immigrants in New York City: Results from a large, community-based screening, evaluation, and treatment program. Cancer Epidemiology, Biomarkers & Prevention, 23(11), 2229–2239.
Hwang, J. P., Mohseni, M., Gor, B. J., Wen, S., Guerrero, H., & Vierling, J. M. (2010). Hepatitis B and hepatitis C prevalence and treatment referral among Asian Americans undergoing community-based hepatitis screening. American Journal of Public Health, 100(Suppl 1), S118–S124.
Xu, J. J., Tien, C., Chang, M., et al. (2013). Demographic and serological characteristics of Asian Americans with hepatitis B infection diagnosed at community screenings. Journal of Viral Hepatitis, 20(8), 575–581.
Shankar, H., Blanas, D., Bichoupan, K., Ndiaye, D., Carmody, E., Martel-Laferriere, V., et al. (2016). A novel collaborative community-based hepatitis B screening and linkage to care program for African immigrants. Clinical Infectious Diseases, 62(Suppl 4), S289–S297.
Chandrasekar, E., Song, S., Johnson, M., Harris, A. M., Kaufman, G. I., Freedman, D., et al. (2016). A novel strategy to increase identification of African-born people with chronic hepatitis B virus infection in the Chicago metropolitan area, 2012–2014. Preventing chronic disease (vol. 13). Accessed August 22, 2017, from https://www.cdc.gov/pcd/issues/2016/16_0162.htm.
Klevens, R. M., Hu, D. J., Jiles, R., & Holmberg, S. D. (2012). Evolving epidemiology of hepatitis C virus in the United States. Clinical Infectious Diseases, 55(Supp 1), 3–9.
Acknowledgements
We would like to thank the Hepatitis B Initiative of Washington, DC (HBI-DC) for providing the data that supported this work. Free community-based health screenings organized by HBI-DC are supported by Gilead, DC Mayor’s Office on African Affairs, DC Mayor’s Office on Asian and Pacific Islander Affairs, Hep B United, Northern VA Community Foundation, Ruth H. Kuo and Rhoda How Memorial Foundation, and individual donors.
Funding
This analysis was funded by the National Cancer Institute (R01CA163805).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors have any conflict of interest to report.
Rights and permissions
About this article

Cite this article
Juon, HS., Ha, E., Kim, F. et al. Prevalence of Viral Hepatitis in Foreign-Born Populations in the Baltimore-Washington Metropolitan Area, 2009–2015. J Community Health 44, 203–207 (2019). https://doi.org/10.1007/s10900-018-0573-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-018-0573-2