
Abstract
Studies in industrialized nations suggest that severe edentulism correlates with cognitive impairment, but there is little information on this association in underserved populations. We conducted a community-based study to assess whether edentulism associates with cognitive impairment in elders living in rural Ecuador. Atahualpa residents aged ≥60 years were identified during a door-to-door census and evaluated using the Montreal Cognitive Assessment (MoCA). Persons were classified into two groups according to whether they have severe edentulism (<10 remaining teeth) or not. In addition, a questionnaire allowed self-rating of oral health. A total of 274 persons (mean age 69.6 ± 7.7 years; 59 % women) were included. Persons with <10 remaining teeth (n = 116) have significantly lower MoCA scores than those with ≥10 teeth (n = 158), after adjusting for demographics, cardiovascular risk factors, depression and dementia (β = −1.06, p = 0.03). Self-rated poor oral health was more prevalent among persons with <10 teeth (p < 0.0001), but did not correlate with MoCA scores (good vs. poor, β = −0.89, p = 0.89). Severe edentulism is associated with poor cognitive performance in elders living in rural Ecuador. Public health campaigns directed to improve oral health may facilitate early recognition of persons with cognitive impairment in underserved populations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The number of persons with cognitive impairment and dementia is progressively increasing in low- and middle-income countries [1]. For example, in Latin America, the contribution of psychiatric and neurological disorders to the total burden of illness has almost triplicated during the past few years [2]. Traditional and non-traditional modifiable risk factors need to be properly recognized in these areas in order to develop cost-effective strategies directed to reduce the impact of these new epidemics.
Cross-sectional surveys have found an association between edentulism and cognitive impairment [3–5], and longitudinal studies have suggested that a reduced number of teeth precede or may even predict the occurrence of cognitive impairment and dementia later in life [6–8]. While this relationship has been studied in industrialized nations, there is limited information on its relevance in people living in rural areas of developing countries. It is just in these regions, where limited access to dental care and lack of awareness on the repercussions of a poor oral hygiene on systemic health contributes to the problem [9]. Epidemiologic surveys assessing the relevance of dental problems and their systemic correlates in underserved populations may provide useful insights on its public health impact at regional levels. We report the finding of a cross-sectional survey hypothesizing that severe edentulism is independently associated with cognitive impairment in community-dwelling elders living in rural coastal Ecuador.
Methods
The Atahualpa Project is a multi-step, population-based study, designed to reduce the burden of cardiovascular and neurological disorders in rural Ecuador. Atahualpa was selected as it is representative of the villages of rural coastal Ecuador. More than 95 % of the population belongs to the Native/Mestizo ethnic groups, and their cardiovascular health (CVH) status is acceptable owing to a simple lifestyle at the rural level [10]. Most men work as artisan carpenters and most women are homemakers. Family income is rather homogeneous, and fluctuates from $5,000 to $12,000/year.
Methodology and operational definitions of the project have been described elsewhere [11]. The IRB of Hospital-Clínica Kennedy (FWA 00006867) approved the protocol and the informed consent form. Trained field personnel performed a door-to-door survey to identify all Atahualpa residents aged ≥60 years. A rural dentist performed an oral exam in consenting persons with an emphasis on the number of remaining teeth. For the purpose of this study, individuals were classified in two groups according to whether they have severe edentulism—defined as those who have <10 remaining teeth—or not. In addition, a questionnaire allowed participants to self-rate their oral hygiene as poor, fair or good, on the basis of questions regarding regular tooth brushing, use of mouthwash antiseptics and dental floss, and periodic preventive visits to the dentist.
Cognition was assessed with the Spanish version of the Montreal Cognitive Assessment (MoCA) test (www.mocatest.org, ©Z. Nasreddine MD, version 07 November 2004). The MoCA evaluates major cognitive domains, including: visuospatial-executive, language, short-term memory, abstraction, attention and calculation, and orientation: maximum MoCA score is 30 points, with an additional point is given to persons with ≤12 years of education [12]. CVH status of participants was evaluated by the use of the seven CVH metrics proposed by the American Heart Association, including: smoking status, body mass index, physical activity, diet, blood pressure, fasting glucose blood levels, and total cholesterol blood levels [13]. According to these criteria, each metric was classified as “ideal”, “intermediate” or “poor”, and the CVH status of a person was classified as poor if at least one metric was in the poor range.
Participants were also evaluated with the depression axis of the DASS 21, a consistent field instrument that quantitatively measures dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest/involvement, anhedonia and inertia, with seven questions that are rated on a four-point Likert scale ranging from 0 (not at all) to 3 (almost always) with a maximum total score of 21, and a diagnosis of depression in persons who have ≥5 points [14]. Persons with dementia were recognized by the use of the Leganés Cognitive Test, a reliable instrument that has been used in elders living in poor-educated communities. The maximum score is 32 points, and a score of ≤22 indicates dementia [15].
Descriptive statistics are presented as mean ± standard deviations for continuous variables and as percentages (with 95 % CI) for categorical variables. Statistical significance was tested by using the χ 2 test for categorical variables or ANOVA or the Kruskal–Wallis test for continuous variables. We evaluated relationships between severe edentulism and age, sex, years of education, CVH status, dementia, depression, and MoCA scores. Then, using linear regression analysis, we examined the association between severe edentulism and MoCA score, after adjusting for demographics, CVH status, depression or dementia. Additionally, we estimated the relationship between self-reported oral health in categories of good versus fair and good versus poor, and severe tooth loss and MoCA score. The latter was also evaluated in a linear regression model, after adjustment for demographics, CVH status, dementia, and depression. All analyses were performed using SAS software version 9.3 (SAS Institute Inc., Cary, NC).
Results
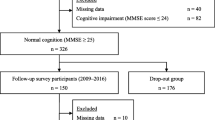
The door-to-door survey identified 323 Atahualpa residents aged ≥60 years, of whom 17 declined to participate and 32 (mean age 79 ± 12 years; 34 % women) could not perform the MoCA due to aphasia or severe visual or hearing impairment. Of the remaining 274 persons (mean age 69.6 ± 7.7 years; 59 % women), 116 had severe edentulism and 158 did not. Table 1 presents the characteristics of the total sample and across categories of edentulism. The group of persons with <10 remaining teeth was older and less educated than the group with ≥10 teeth. There were no significant differences between the groups in gender distribution, or in the percentage of persons with poor CVH status, depression or dementia. A poor oral health was more prevalent among persons with severe edentulism. Mean MoCA score was 18.5 ± 4.6 points. Persons with <10 teeth scored significantly worse in this test when compared with those with ≥10 teeth.
Results of linear regression showed significantly lower MoCA scores for persons with <10 remaining teeth, after adjusting for age, sex, years of education, CVH status, depression, and dementia (β = −1.06, p = 0.03). In a similar model, we did not find differences between self-reported oral health and MoCA scores (good vs. fair, β = 0.49, p = 0.42; good vs. poor, β = −0.89, p = 0.89).
Discussion
This study suggests that severe edentulism is associated with a poorer performance in the MoCA in elders living in rural Ecuador. While pathogenetic mechanisms explaining this association are not fully understood, it is likely that chronic periodontitis stimulates the production of inflammatory cytokines that, in turn, may damage the brain; indeed, edentulism has often been considered a proxy for chronic periodontitis [16, 17]. It has also been suggested that poor dentition may be associated with nutritional deficiencies and that lower levels of B vitamins may account for the cognitive decline seen in persons with severe tooth loss [18]. However, this is less likely to occur in Atahualpa (and probably in other rural villages of Latin American developing countries as well) where B vitamins-enriched white rice is an important part of the diet and almost all persons eat—irrespective of the number of teeth—one or two servings of white rice per day.
This is the only study where the MoCA has been used for evaluation of cognitive status according to the number of teeth. Other studies have used the Folstein’s Mini Mental State Examination (MMSE) for this purpose [3–6]. However, it is known the lack of sensitivity of the latter for detection of persons with mild cognitive impairment. In a comparative study, the MoCA and the MMSE were equally specific (93 %) but the MoCA had a significantly better sensitivity (67 vs. 13 %) [19]. In addition, we did not used a cutoff score for defining cognitive impairment, but the continuous MoCA score to compare performance in the test across persons with and without severe edentulism, to avoid problems related to poor reliability of specific cutoffs. Also, some previous studies of edentulism in relation to cognitive impairment were hampered by selection bias of enrolled participants or lack of adjustment for confounding factors [20]. In the present study, we enrolled an entire population of community-dwelling elders living in a rural village, avoiding participants’ selection bias, and the analysis was conducted after adjustment for all potential confounders.
As we assessed missing teeth in a cross-sectional survey, we cannot be sure about the cause of edentulism. Another potentially perceived weakness of our study could be the relatively small sample size. However, the homogeneous characteristics of Atahualpa’s residents regarding race/ethnicity and socio-economic status, together with the model used for assessing the association between edentulism and cognitive performance, argues for the strength of our results.
In summary, severe edentulism is associated with a poorer cognitive performance in elders living in rural Ecuador. Public health campaigns directed to improve oral health to detect persons with severe edentulism may facilitate early recognition and treatment of those with cognitive impairment. Further longitudinal studies in these underserved populations are warranted to settle the cause-and-effect relationships of this association.
References
Scazufca, M., Cerqueira, A. T., Menezes, P. R., et al. (2002). Investigações epidemiológicas sobre demencia nos países em desenvolvimiento. Rev Saúde Pública, 36(6), 773–778.
World Health Organization. (2007). Health in the Americas: An overview of regional health. Geneva: World Health Organization.
Okamoto, N., Morikawa, M., Okamoto, K., et al. (2010). Relationship of tooth loss to mild memory impairment and cognitive impairment: Findings from the fujiwara-kyo study. Behavioral and Brain Functions, 6, 77.
Saito, Y., Sugawara, N., Yasui-Furukori, N., et al. (2013). Cognitive function and number of teeth in a community-dwelling population of Japan. Annals of General Psychiatry, 12(1), 20.
Takata, Y., Ansai, T., Soh, I., et al. (2009). Cognitive function and number of teeth in a community-dwelling elderly population without dementia. Journal of Oral Rehabilitation, 36(11), 808–813.
Gatz, M., Mortimer, J. A., Fratiglioni, L., et al. (2006). Potentially modifiable risk factors for dementia in identical twins. Alzheimer’s and Dementia, 2(2), 110–117.
Kaye, E. K., Valencia, A., Baba, N., et al. (2010). Tooth loss and periodontal disease predict poor cognitive function in older men. Journal of the American Geriatrics Society, 58(4), 713–718.
Stein, P. S., Desrosiers, M., Donegan, S. J., et al. (2007). Tooth loss, dementia and neuropathology in the Nun study. Journal of the American Dental Association, 138(10), 1314–1322.
Auluck, A. (2005). Oral health of poor people in rural areas of developing countries. Journal/Canadian Dental Association, 71(10), 753–755.
Del Brutto, O. H., Dong, C., Rundek, T., et al. (2013). Cardiovascular health status among Caribbean Hispanics living in Northern Manhattan and Ecuadorian natives/mestizos in rural coastal Ecuador: A comparative study. Journal of Community Health, 38(4), 634–641.
Del Brutto, O. H., Peñaherrera, E., & Ochoa, E. (2013). Door-to-door survey of cardiovascular health, stroke and ischemic heart disease in rural coastal Ecuador—The Atahualpa Project. Methodology and operational definitions. International Journal of Stroke. doi:10.1111/ijs.12030.
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., et al. (2005). The Montreal cognitive assessment, MoCA: A brief screening tool for mild cognitive impairment. Journal of the American Geriatrics Society, 53(4), 695–699.
Lloyd-Jones, D., Hong, Y., Labarthe, D., et al. (2010). American Heart Association strategic planning task force and statistics committee. Defining and setting national goals for cardiovascular health promotion. The American Heart Association’s strategic impact goal through 2020 and beyond. Circulation, 121(4), 586–613.
Osman, A., Wong, J. L., Bagge, C. L., et al. (2012). The depression anxiety stress scale-21 (DASS-21): Further examination of dimensions, scale reliability, and correlates. Journal of Clinical Psychology, 68(12), 1322–1338.
de Yébenes, M. J., Otero, A., Zunzunegui, M. V., et al. (2013). Validation of a short cognitive tool for the screening of dementia in elderly people with low educational level. International Journal of Geriatric Psychiatry, 18(10), 925–936.
Schmidt, R., Schmidt, H., Curb, J. D., et al. (2002). Early inflammation and dementia: A 25-year follow-up of the Honolulu–Asia Aging study. Annals of Neurology, 52(2), 168–174.
Kamer, A. R., Craig, R. G., Dasanayake, A. P., et al. (2008). Inflammation and Alzheimer’s disease: Possible role of periodontal disease. Alzheimer’s and Dementia, 4(4), 242–250.
Tucker, K. L., Qiao, N., Scott, T., et al. (2005). High homocysteine and low B vitamins predict cognitive decline in aging men: the Veterans Affairs Normative Aging study. American Journal of Clinical Nutrition, 82(3), 627–635.
Alagiakrishnan, K., Zhao, N., Mereu, L., et al. (2013). Montreal cognitive assessment is superior to standardized Mini mental status exam in detecting mild cognitive impairment in the middle-aged and elderly patients with type 2 diabetes mellitus. BioMed Research International, 2013, 186106.
Stewart, R., Sabbah, W., Tsakos, G., et al. (2008). Oral health and cognitive function in the Third National Health and Nutrition Examination Survey (NHANES III). Psychosomatic Medicine, 70(8), 936–941.
Acknowledgments
This study was partly supported by Universidad Espíritu Santo—Ecuador, Guayaquil, Ecuador.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Del Brutto, O.H., Gardener, H., Del Brutto, V.J. et al. Edentulism Associates with Worse Cognitive Performance in Community-Dwelling Elders in Rural Ecuador: Results of the Atahualpa Project. J Community Health 39, 1097–1100 (2014). https://doi.org/10.1007/s10900-014-9857-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-014-9857-3