
Abstract
Oral cancer is one of the most fatal health problems faced by the mankind today. In India, because of cultural, ethnic, geographic factors and the popularity of addictive habits, the frequency of oral cancer is high. It ranks number one in terms of incidence among men and third among women. Several factors like tobacco and tobacco related products, alcohol, genetic predisposition and hormonal factors are suspected as possible causative factors. Hence the study was designed to determine the prevalence of Oral Cancer in patients who attended the outpatient department, at Bharati Vidyapeeth Deemed University Dental College Sangli India during a period of 24 months in 2009–2010. Further various modes of tobacco and alcohol consuming habit were assessed along with the site of occurrence of oral cancer. About 35,122 subjects belonging to a semi-urban district of Sangli in Western Maharashtra (India) were screened. Tobacco and alcohol consumption was the common habit among the study population. Out of these about 112 cases showed Oral Cancer. The prevalence of Oral Cancer was 1.12%. Statistical analysis was done using the SPSS software 11. The findings in the present study reveal a high prevalence of Oral Cancer and a rampant misuse of variety of addictive substances in the community. Close follow up and systematic evaluation is required in this population. Education about ill effects of tobacco and alcohol consumption is necessary at a broader scale. There is an urgent need for awareness programs involving the community health workers, dentists and allied medical professionals.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Oral cancer is one of the most fatal health problems faced by the mankind today. The incidence of head and neck cancer varies enormously all around the world and especially oral cancer which accounts for 30–40% of all the malignant tumors in India, being only about 2–4% in western countries [1]. In India, because of cultural, ethnic, geographic factors and the popularity of addictive habits, the frequency of oral cancer is high. It ranks number one in terms of incidence among men and third among women. It has one of the lowest 5-years survival rates of all cancers, probably because most lesions are not diagnosed in the initial stages. However, if detected early, the probability of survival from oral cancer is remarkably better than for most other cancers [2]. In a study reported from Allahabad (North India) the malignant oral lesions were widespread in patients visiting their tertiary level hospital [3]. In a similar study conducted in Manipuri district of India annual incidence rate of oral cancer was 21.4 per 100,000 individuals [4].
Despite a century of cancer research, the cause of oral cancer remains debatable. Several factors like tobacco and tobacco related products, alcohol, genetic predisposition and hormonal factors are suspected as possible causative factors. Now the concept of field cancerization (Multiple cancers) is gaining lot of attention, as there is an increase in the incidence of secondary tumors following thorough excision of the primary cancerous tissue. This has added to the increased mortality rate in oral cancer [5]. There is also a considerable variation in the distribution of cancer in intra oral sites. Cancer of buccal mucosa, lower alveolus and the retromolar trigone are grouped together as cancers of gingivo-buccal complex and can be aptly called as the “Indian Oral Cancer” as they constitute 60% of all oral cancers in India. Tongue and the floor of the mouth cancers form the bulk of oral cancers in the west [6]. Hence, in the light of these aspects, the present study was taken up to assess the prevalence of oral cancer in Indian population over a period of 2 years. Various modes of tobacco/alcohol consuming habit and site of occurrence of oral cancer were studied.
Materials and Methods
Patients reporting to the Department of Oral Medicine, Diagnosis and Radiology at Bharati Vidyapeeth Deemed University Dental College and Hospital Sangli Maharashtra, India were included in the present study. The ethical committee of the institution approved the study and all subjects participating in the study gave their consent for participation. Faculty of the out patient department collected the data using a combination of clinical oral examination and standardized questionnaire. Information on demographic parameters, habits etc. were acquired using interviewer based questionnaire. Patients rinsed their mouth thoroughly with water and were examined under an incandescent light source. During the study period about 35,122 patients were examined. One hundred and twelve cases were found to have oral cancer. The Oral Cancer cases were analyzed for the following elements: features of the lesion, anatomical location, extension, etiological factors or related factors, dental status, alcohol, tobacco, use of prosthesis etc.
Statistical Analysis
The variables were analyzed on all patients, using the SPSS software (11.0).
Results and Observations
The population under study consisted mainly of individuals living in and around Sangli (India). A total of 35,122 patients were screened during the study period. 112 cases were found to have oral cancer. Out of these 81 (72.32%) were male patients and 31 (27.67%) were female patients, with an age range of 30–70 years (Table 1). The subjects in the study were either having habit of tobacco chewing, smoking, alcohol consumption or a combination of these. Tobacco consumption in form of chewing was the most common habit followed by tobacco smoking. About 7,376 (21%) study subjects chewed tobacco and 3,513 (10%) of study subjects smoked tobacco. About 4,215 (12%) subjects of study population consumed alcohol while about 5,269 (15%) subjects consumed alcohol along with tobacco (Table 2). A total 22,830 (65%) subjects were non tobacco consumers while 24,586 (70%) subjects were nonalcoholic. Thus on an Average 25% to 30% subjects consume tobacco and alcohol. The prevalence of oral cancer in study population was 0.3%, but when we analyze the prevalence in subjects having habits of tobacco and alcohol consumption the prevalence rises to 1.12% (Table 3).
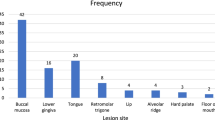
The site of occurrence of oral cancer was highest in the lower alveolus 36 (32.14%) followed by buccal mucosa 34 (30.35%), Palate and Lip 12 (10.71%), tongue 08 (7.14%), Gingivo-buccal sulcus 18 (16.07%) and retromolar trigone 04 (3.57%) as shown in Table 1.
Discussion
Tobacco in any form is dangerous to health and when it is consumed along with alcohol its action is doubled. The present study clearly showed the association of these habits and occurrence of oral cancer. Various studies have shown an increase in evidence of oral cancer in females in Indian subcontinent. The data available from Tata Memorial Cancer Hospital Mumbai shows that, the incidence rates of oral cancer in females are much higher in south-India than other parts and the ratio of male to female being 0.6:1 [7]. Gupta and Nandakumar in their editorial have stated in India cancer of oral cavity is one of the five leading sites of cancer in either sex. The age standardized incidence rates (ASR) vary from 6.5 per 100,000 in Bangalore to 15.9 per 100,000 in Trivandrum among males and from 7.2 in Bombay to 10.6 per 100,000 in Chennai among females [8]. In the present study the male to female ratio was 2.6:1. This shows that both male and females when develop the habit of consuming these things will predispose them to oral cancer. The age of the subjects ranged from 30 to 70 years. Most of the subjects with oral cancer were above 50 years of age, which shows that the incidence of oral cancer is more in elderly aged. Similar findings have also been reported in the study conducted by Sanghvi et al. [9].
The site of occurrence of oral cancer was highest in the lower alveolus followed by buccal mucosa and Palate and Lip 12 (10.71%). Study conducted by Sankaranarayanan [10] and Soben [11] reported that buccal mucosa (50%) is the commonest site for oral cancer in India followed by anterior two thirds of tongue (24%), the lower gum (12.5%), the lip (4%), the hard palate (3.2%), the floor of the mouth (3%) and the upper gum (2.8%). Cancer of buccal mucosa, lower alveolus and the retromolar trigone are grouped together as cancers of gingivo-buccal complex and can be aptly called as the “Indian Oral Cancer” as they constitute 60% of all oral cancers in India [6]. Similarly in our study the cancer involving buccal mucosa and lower alveolus was high when compared to other sites. The oral cancer involving Palate and Lip was mostly noticed in male subjects who smoked tobacco.
The prevalence of oral cancer in study population was 0.3%, but when we analyze the prevalence in subjects having habits of tobacco and alcohol consumption, the prevalence rises to 1.12%. This high prevalence clearly suggests that incidence of oral cancer in subjects consuming tobacco and alcohol is more and has to be tackled more specifically. This alarming increase in the prevalence of oral malignant disorders in India is mainly due to the culture, ethnic, geographic factors, low socio-economic status and varying lifestyle factors like consumption of various forms tobacco, alcohol, fewer intakes of fruits and vegetable etc. Studies have shown that these are the major risk factors for development of malignant disorders [12].
All the oral cancer subjects had a habit of consuming tobacco either in chewing or smoking form. Chewing form of tobacco was either plain tobacco or in its commercial available packets with additives like gutkha. Few male subjects and all female subjects chewed tobacco with pan, betel nut and lime. Alcohol consumption was noticed as a common habit in male subjects and it was associated with either smoking or tobacco chewing habit or both. It was noticed that smoking and alcohol consumption was commonly associated with carcinoma of palate while that of chewing tobacco was commonly associated with carcinoma of alveolus and buccal mucosa. Sanghvi [9] reported that consuming tobacco increases the risk for developing oral cancer. The risk ratio for cancer of oral cavity was estimated as 4-fold in chewers, 2-fold in smokers and 4-fold in chewer-smokers compared to nonchewer-nonsmokers. It has been stated that alcohol is not carcinogenic, but there is increasing evidence that a major part of the tumour promoting action of alcohol might be mediated via its first, toxic and carcinogenic metabolite acetaldehyde. Acetaldehyde is produced from ethanol in the epithelia by mucosal alcohol dehydrogenases, but much higher levels are derived from microbial oxidation of ethanol by the oral microbial flora. Thus subjects consuming alcohol are at increasing risk of developing cancer because of this synergistic action [13]. Thus tobacco and alcohol are evils of the society and proper steps should be taken to eradicate them.
Most of the cases reported were having a full blown malignancy and were at advanced stage. This suggests that the rural population may not seek the medical care until the lesions become symptomatic and attend a reasonably large size. Low literacy rate and ignorance on the part of the patients are considered as additional factors for seeking late medical attention. While emerging lifestyle and food habits have been contributing factors, the problem of bad oral health is compounded by a low dentist to population ratio. The World Health Organisation (WHO) recommends a 1:7,500 dentist to population ratio whereas the dentist to population ratio in India is as low as 1:22,500 [14]. In 2004, India had one dentist for 10,000 persons in urban areas and about 2.5 lakh persons in rural areas. Almost three-fourths of the total number of dentists are clustered in urban areas, which house only one-fourth of the country’s population [15]. This limits the curative approach to tackle dental problems in rural areas while it is widely acknowledged that oral cancer can best be prevented through early detection and primary prevention.
All the diagnosed oral cancer subjects in our study were advised abstinence from tobacco and alcohol and were treated at our Medical Hospital, Sangli. Data was collected as a chair side procedure, which involved oral examination and questionnaire administration. Since the information on the habits was gathered through questionnaire, there could be information bias.
Oral cancer has been affecting human race since time immemorial. Rapid growth of research and advancements in technology in the past few decades have not been able to reduce the prevalence of cancer. Each year about 575,000 new cases are diagnosed and as a consequence 335,000 deaths occur worldwide. Its high frequency in Central and South East Asian countries (India, Bangladesh, Sri Lanka, Thailand, Indonesia and Pakistan) has been well documented [16].
Conclusion
Tobacco and alcohol consumption is injurious to health and is evident from our study. All the oral cancer subjects enrolled in the study had a habit of either consuming tobacco or alcohol or both. It was noted that smoking and alcohol consumption was commonly associated with carcinoma of palate while that of chewing tobacco was commonly associated with carcinoma of lower alveolus and buccal mucosa. The prevalence of Oral Cancer was 1.12%. Hence education of population about ill effects of tobacco and alcohol consumption is necessary at a broader scale. Further banning of sale of tobacco and tobacco products should be implemented.
References
Greenberg, M. S., & Glick, M. (2003). Burket’s oral medicine diagnosis & treatment (10th ed., p. 195). Hamilton: BC Decker Inc.
Rajendran, R., & Sivapathasundharam, B. (2006). Shafer’s textbook of oral pathology (5th ed., pp. 113–308). New Delhi: Elsevier, Reed Elsevier India Private Limited.
Mehrotra, R., Pandya, S., Chaudhary, A. K., Kumar, M., & Singh, M. (2008). Prevalence of oral pre-malignant and malignant lesions at a tertiary level hospital in Allahabad, India. Asian Pacific Journal of Cancer Prevention, 9(2), 263–265.
Wahi, P. M. (1968). The Epidemiology of oral and oro-pharyngeal cancer. A report in Manipuri dist, Uttar Pradesh, India. Bulletin of World Health Organization, 38, 495–521.
Thomson, P. J. (2002). Field change and oral cancer: New evidence for widespread carcinogenesis? International Journal of Oral and Maxillofacial Surgery, 31, 262–266.
Mathew, B. (1993). Epidemiology of oral cancer. JIDA, 64(2), 43–46.
Rao, R. S., & Desai, P. B. (1991). Oral cancer (pp. 1–5). Bombay: Tata Press Limited.
Gupta, P. C., & Nandkumar, A. (1999). Oral cancer scene in India. Guest editorial. Oral Diseases, 5, 1–2.
Sanghvi, L. D. (1981). Cancer epidemiology. The Indian scene. Journal of Cancer Research and Clinical Oncology, 99, 1–4.
Sankaranarayanan, R. (1990). Oral cancer in India: An epidemiologic and clinical review. Oral Surgery, Oral Medicine, Oral Pathology, 69, 325–330.
Soben, P. (2003). Essentials of preventive and community dentistry (2nd ed., p. 470). New Delhi: Arya Publishing house.
Hashibe, M., Jacab, B. J., Thomas, G., Ramadas, K., Mathew, B., Sankaranarayanan, R., et al. (2003). Socio-economic status, life style factors and oral pre-malignant lesions. Oral Oncology, 39, 664–671.
Homann, N., Tillonen, J., Meurman, J. H., Rintamaki, H., Lindqvist, C., Rautio, M., et al. (2000). Increased salivary acetaldehyde levels in heavy drinkers and smokers: A microbiological approach to oral cavity cancer. Carcinogenesis, 21(4), 663–668.
World Health Organization. (1992). Recent advances in oral health. Technical report series-826. World Health Organization, 298, 1–37.
Tandon, S. (2004). Challenges to the oral health workforce in India. Journal of Dental Education, 68, 29–33.
Kramer, I. R., Pindborg, J. J., Bezroukov, V., & Infirri, J. S. (1980). Guide to epidemiology and diagnosis of oral mucosal diseases and conditions. World Health Organization. Community Dentistry and Oral Epidemiology, 8(1), 1–26.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Byakodi, R., Byakodi, S., Hiremath, S. et al. Oral Cancer in India: An Epidemiologic and Clinical Review. J Community Health 37, 316–319 (2012). https://doi.org/10.1007/s10900-011-9447-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-011-9447-6