
Abstract
The objective of this study was to explore whether the time at which sex education was provided had any impact on reported cases of unintended pregnancies. A cross-sectional survey of secondary school students and their teachers was conducted using self-administered questionnaires. The participants were 1,234 students aged 14–17 years and 46 teachers in 5 secondary schools in South Eastern Nigeria. The outcome measures were reported pregnancies within the last 3 years by type of school and class level; class level at the time of receiving sex education at school; and age at the time of receiving sex education at home. In all schools, sex education was provided at all the junior and senior secondary school levels (JSS and SSS, respectively). Overall, reported cases of unintended pregnancies were highest among the junior students. In the private schools, four in ten teachers reported pregnancies among JSS 3 students. Almost four in ten teachers in public schools reported pregnancies among JSS 2 students. Of all the students, about three in ten reported pregnancies among JSS 2 and 3 students respectively. At home, sex education was provided at the mean age of 16 years (SD ±2.2). All participants cited financial need and marital promise as major predisposing factors. About four in ten students did not use contraceptives during their first sexual experience. This study highlights the need to introduce sex education much earlier, possibly before the JSS levels. At home, sex education may have greater impact if provided before the age of 14 years. Efforts should be made to address the factors predisposing to teenage pregnancy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
About three out of ten Nigerian women of reproductive age have experienced unintended pregnancies and these pregnancies are more common among women aged below 20 years [1]. In an effort to reduce unintended pregnancies among female secondary school students, a curriculum for sex education was introduced in Nigerian schools in 2002 [2]. Failure to fully implement this curriculum has been attributed mostly to poor attitude of the teachers, and inadequate support from parents and religious leaders. However, a review of 53 studies by Grunseit has raised questions about the efficacy of sex education in preventing unintended pregnancies [3].
The review showed that sex education had no effect on sexual activity and attendant rates of pregnancy in over fifty percent of the studies. The remaining studies showed either a reduction or increase in sexual behaviour associated with the sex education programmes. Despite such conflicting results, providing teenagers with accurate reproductive health information is important—not only to prevent unintended pregnancies but also to prevent abortion and its complications, sexually transmitted infections (STIs) and HIV/AIDS. In Nigeria, pregnancy and teenage motherhood often lead to termination of studies and deferment of academic or career aspiration of the teenagers [4].
Teenagers spend reasonable part of their time at school and this places the teachers in good position to offer guidance and influence their students’ sexual/reproductive health decisions alongside their parents. Teenagers with whom parents have discussed sexuality issues are less likely to be sexually active, which further reduces their risks of unintended pregnancies [5]. However, young people are able to imbibe appropriate sexual behaviour and make informed decisions if they receive early sex education [6]. Prior to the onset of puberty, young people have not developed established sexual behavioural pattern and may be more receptive to guidance [7]. Had this need been recognized earlier, the effectiveness of sex education might have been improved resulting to lower number of unintended pregnancies among students.
In this study area, there was high prevalence of unintended pregnancies among students despite their exposure to sex education. Although previous studies have been conducted on unintended pregnancy in Anambra state, they were limited to unmarried pregnant teens attending antenatal clinics; complications arising from abortion due to unintended pregnancy and opinions of religious leaders on unintended pregnancy. This study aims to explore the impact of sex education based on the time at which it was provided and its resultant effect on unintended pregnancies.
Methods
Survey Site
The study took place in Anambra state, in southeastern Nigeria. The state is urban and a major commercial hub with a population of 4.5 million comprising of 21 local government areas. After 6 years of primary/elementary education, students proceed to secondary education, starting with the junior secondary school levels (JSS 1-3) up to senior secondary school levels (SSS 1-3). English is the primary language of instruction in schools, and by the secondary level all students can read and write in basic English.
Participants
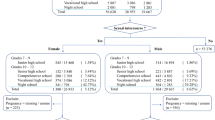
In all, 1,234 students and 46 teachers from 5 (3 public and 2 private) secondary schools took part in the study (Table 1). Participation was voluntary for both students and teachers.
Questionnaire
A self administered, English language questionnaire comprising mostly of multiple-choice items and a few open-ended questions was developed for the study. For the students, the questionnaire consisted of 5 items on educational and demographic characteristics, 4 items on sexual experience, 21 items on female students who have been pregnant in the last 3 years, 6 items on sex education, and 1 item on prevention of unintended pregnancy. The questionnaire for the teachers comprised of 2 items on demographic characteristics, 3 items on knowledge of adolescent sexual activities, 5 items on students who have been pregnant in the last 3 years, 2 items on schools’ written policies on pregnancy, 5 items on availability of school nurses and counselling/support services and 1 item on prevention of unintended pregnancy. Participants’ names and schools were not disclosed on the questionnaires to ensure confidentiality.
Data Collection
The main author and two trained research assistants did the data collection. Prior to the survey, the questionnaire was pilot tested on a young volunteer and areas of difficulties were modified. In all the schools, the questionnaires were completed by the students in their classrooms and by the teachers in their staff rooms. It was clearly stated on all the questionnaires that participants’ responses would remain anonymous. Participation was voluntary and participants were free to withdraw at any stage without any unpleasant consequences.
Data Analysis
Statistical Package for Social Sciences 14 (SPSS-14) for windows was used for all statistical analysis. Teachers’ responses were analysed based on type of school—public and private school—in order to obtain more comprehensive information. Unlike the teachers’, the students’ responses were not analysed based on type of school except in two instances; the aim was to obtain general perspectives of the problem by the students. The gender of the students was analysed by type of school and the question on class/educational levels of the students who got pregnant in the last 3-years was also analysed based on type of school. This was meant to compare the responses of both teachers and students to the same question and to see if cases of pregnancies were more common in a particular type of school. The mean and standard deviation were calculated for the age of the student participants and the age at first sexual experience.
Ethical Consideration
The study protocol was approved by the Ethics Committee of Nnamdi Azikiwe University Teaching Hospital Nnewi, which is responsible for ethical review of most research studies in Anambra state. Before the study, permissions were obtained from the principals/proprietors of all the schools.
Results
Teachers
Forty-six (46) teachers took part in the study, with almost equal gender participation. About nine out of every ten teachers affirmed that young people were sexually active, and reported cases of pregnancy among students within the last 3 years. Generally, the reported cases of pregnancy were highest among JSS 2 and JSS 3 students and lowest among the SS 2 students. When analyzed by the type of school, the prevalence in private schools was highest in JSS 3 class level and in public schools it was highest in JSS 2 class level (Table 2A).
According to the teachers, the most important predisposing factors to teenage pregnancy were financial need and poor parental support (27%), and marital promise or peer pressure to get married (25%). In addition, ignorance (9%), sexual abuse/rape (7%), and others including lack of religious commitment, and family instability (17%) were also reported as risk factors.
With regards to their opinion of sex education, most of the teachers (77% in public school and 75% in private schools) opined that sex education was very important. The teachers were not very specific about the class level at which sex education was provided to the students. In Table 3, 17% of all the teachers (in both public and private schools), reported that sex education was offered at class levels other than JSS 2 to SSS 2. Of this percentage, 4% reported that it was offered at JSS 1, 13% reported it was given at all the class levels. However, majority of the teachers did not respond to the question.
During sex education, emphasis was laid on STIs including HIV/AIDS (17%) and socioeconomic consequences of unintended pregnancy (17%). Other topics included were abortion and its consequences (9%), contraception (2%) and other topics, which were not specified by the teachers (55%).
Students
A total of 1,234 students participated in the study from both public and private secondary schools. Majority of the participants from both schools were females (Table 1B) and all the schools were co-educational (or mixed) in composition. The mean age of the students was 16 years (SD ±1.7) and about half of them did not respond to the question about age at first sexual experience (Table 4). Of those who responded, the mean age at first sexual experience was 17 years (SD ±2.1). Majority (43%) did not use contraceptives during their first sexual experience, and 14% had multiple sexual partners.
Most of the respondents (77%) knew another student who got pregnant within the last 3 years. When analyzed by type of school, JSS 3 class level had the highest reported number of cases in public schools, followed by JSS 2. Similarly, in the private schools, majority of the cases were reported for the JSS 3 and JSS 2 class levels (Table 2B).
According to the students, the most important contributory factor to teenage pregnancy was sex in exchange for money (44%). Other risk factors were marital promise or peer pressure to get married (17%), ignorance (16%), sexual abuse/rape (11%), and others including lack of religious commitment, and family instability (12%).
Among the students who got pregnant, 62% of them were living with their parents at the time of the pregnancy. About 53% of their fathers were reported to be subsistent farmers while others were petty traders (17%), civil servants (i.e. highly skilled workers) (8%) or unemployed (9%). Similarly, 37% of the mothers were subsistence farmers, 32% were petty traders, 9% were civil servants and 10% were unemployed.
Majority of the students (66%) affirmed that they had received some teaching on sex education which took place either at school, at home, or both (67%). Further information about sex or pregnancy was received through the mass media (49%) and their friends (41%).
At school, sex education was received at JSS 2 (22%), JSS 3 (18%), SSS 1 (16%) and SSS 2 (9%) class levels. However, 35% of the students did not respond to this question. The mean age at receiving sex education at home was 16 years (SD ±2.2) but most students received sex education at home at 14 years (Table 4).
Discussion
Main Findings
Majority of the teachers in this community reported that students were sexually active. Sex education was provided at all the class levels in both schools; in spite of this, the prevalence of unintended pregnancies was high among junior secondary students. There was a decrease in the reported cases of pregnancy with increasing class level in all schools. This shows that students were more vulnerable during the JSS levels. Three in ten students (Table 4) did not specify when they received sex education at home. However, of those who did, majority received sex education at home by their 14th birthday. In this study, the major predisposing factor to teenage pregnancy was inadequate financial provision. Marital promise or peer pressure to get married was another important predisposing factor reported by both students and teachers. Perhaps, early marriage was seen as an escape route from financial need and poverty.
Comparison with Existing Literature
Providing sex education by 14th birthday did not reduce the reported cases of pregnancy among the female students. The results of this study lends credence to a study by Anochie and Ikpeme [6] which suggests that early sexual health education starting from primary school might be helpful in influencing the reproductive behaviour of the students in order to minimize teenage pregnancy. In addition, this study raises further questions—could there be problems with the contents/topics covered during sex education or with the reproductive health knowledge of the teachers and parents? In their research study, Kirby et al. [7] suggested that the impact of sex education instruction might vary with the topics covered.
Most of the students engaged in pre-marital sex for economic reasons and many of the pregnant teens’ parents were subsistent farmers, which places them within the lower social and economic levels in the society. This confirms a correlation between socioeconomic status and teenage pregnancy. This result is in line with a previous study by Madise et al. [8], which shows that poor females were more vulnerable to infections and pregnancies compared with other females from wealthy families.
In this study, poor use of contraceptives (probably due to poor teaching of contraception) may explain the high prevalence of unintended pregnancy among the students. This is consistent with the World Health Report [9] and a similar study by Ilika and Igwegbe [10], which linked rate of contraceptive use to the risk of unintended pregnancy. The issue of contraception is particularly important since about 4 in every 10 students in this study did not use contraceptives during their first sexual experience, and 14% had multiple sexual partners.
Although some of the teachers in both schools reported that sex education was provided to the students at all class levels, almost half (43%) did not respond to the question. Moreso, 55% of the teachers did not specify the contents of sex education offered to the students. This raises doubts on the reliability of the information and the level of implementation of sex education in secondary schools, which may be related to the teachers’ knowledge of reproductive health. A study by Adegbenro et al. demonstrated an increase in teachers’ knowledge, attitude and disposition to the teaching of reproductive health education /sex education following a post-training assessment [11].
Further, sexual abuse/rape accounted for a small proportion of the teenage pregnancies in this study. This corresponds to the result of a previous study [12], which found rape/sexual abuse as a predisposing factor to teenage pregnancy. However, the relatively small proportion of pregnancies attributed to sexual abuse/rape in this study, contradicts a previous study, which found that 44% of pregnant teens had been raped [13].
Apart from the mass media, many of the students turned to their friends as other sources of information about sex or pregnancy. This finding supports incorporation of peer groups in the prevention of unintended pregnancy, especially since it has been proven to be an effective strategy in other public health prevention programmes [14].
Strength and Weaknesses
The strengths of this study are the large sample size of the students and the inclusion of students and teachers from both public and private schools. However, due to the sensitive nature and societal reactions to sex-related issues, students may have under-reported sexual activities and teachers may have offered inaccurate information to protect the image of their schools.
Implication for Practice
The result of this study must be interpreted with caution—it is not sufficient to infer that sex education does not have any impact on unintended pregnancy as suggested in previous research studies [15]. Early introduction of sex education both at home and at school, while paying attention to the contents/topics, will help adolescent reproductive health planners to evaluate the overall impact of sex education on unintended pregnancy. In other to ensure that adequate contents are covered, formal training and seminars on adolescent sex education should be organized for teachers. Similarly, some form of education should be provided for parents to enable them overcome cultural barriers that discourage them from providing sex education (especially at early age) to their children. Efforts should also be made to address the various factors that predispose students to teenage pregnancy. Active steps should be taken to increase family income and to de-emphasize the value placed on early marriage, probably as solution to financial need.
References
Okonofua, F. E., Odimegwu, C., Ajabor, H., Daru, P. H., & Johnson, A. (1999). Assessing the prevalence and determinants of unwanted pregnancy and induced abortion in Nigeria. Studies in Family Planning, 30(1), 67–77.
Country brief series no. 2 (2004) Youth reproductive health policy. Nigeria: Advocacy and Strategic Planning for Youth Reproductive Health in Edo State. Policy Project. http://www.policyproject.com/pubs/YRHCBS/Nig_YRH.pdf.
Grunseit A (2008) Impact of HIV and sexual health education on the sexual behaviour of young people: a review update. Available at: http://data.unaids.org/Publications/IRC-pub01/JC010-ImpactYoungPeople_en.pdf. Accessed 10/08/2008.
Slap, G. B., Lot, L., Huang, B., Daniyam, C. A., Zink, T. M., & Succop, P. A. (2003). Sexual behaviour of adolescents in Nigeria: cross-sectional survey of secondary school students. BMJ, 326(7379), 15–18.
Odimegwu, C. O., Solanke, L. B., & Adedokun, A. (2002). Parental characteristics and Adolescent Sexaul behavior in Bida Local government area of State, Nigeria. Afr J Reprod Health, 6(1), 95–106.
Anochie, I. C., & Ikpeme, E. E. (2001). Prevalence of sexual activity and outcome among female secondary school students in Port Harcourt, Nigeria. Afr J Reprod Health, 5(2), 63–67.
Kirby, D., Short, L., Collins, J., Rugg, D., Kolbe, L., Howard, M., et al. (1994). School-based programs to reduce sexual risk behaviors: a review of effectiveness. Public Health Reports, 109(3), 339–360.
Madise, N., Zulu, E., & Ciera, J. (2007). Is poverty a driver for risky sexual behaviour? Evidence from national surveys of adolescents in four African Countries. Afr J Reprod Health, 11(3), 83–98.
World Health Organization (2002) The World Health Report 2002: Sexual and reproductive health. Accessed 06/07/2008. Available at: http://www.who.int/whr/2002/chapter4/en/index5.html.
Ilika, A., & Igwegbe, A. (2004). Unintended pregnancy among unmarried adolescents and young women in Anambra State, South East Nigeria. Afr J Reprod Health, 8(3), 92–102.
Adegbenro, C. A., Adeniyi, J. D., & Oladepo, O. (2006). Effect of training programme on secondary schools teachers’ knowledge and attitude towards reproductive health education in rural schools IIe-Ife, Nigeria. Afr J Reprod Health, 10(2), 98–105.
Bailey, P. (2005). Teenage pregnancies: is the high rate of teenage pregnancy and parenthood in the UK a public health problem? J Fam Plann Reprod Health Care, 31(4), 315–319.
Boyer, D., & Fine, D. (1992). Sexual abuse as a factor in adolescent pregnancy and child maltreatment. Family Plann Perspect, 24(1), 4–11. 19.
Flanagan D, Mahler H (2008) How to create an effective peer education project: guidelines for AIDS prevention projects. Available at: http://www.fhi.org/NR/rdonlyres/efec2fjcedftpcqabrs5oluwwvdu5jofqmwg6hwjkwrl7gsgpzjt24ceuyccva4vvsbgydx3fwgwdo/createeffectpeereducation.pdf. Accessed 13/07/2008.
DiCenso, A., Guyatt, G., Willan, A., & Griffith, L. (2002). Interventions to reduce unintended pregnancies among adolescents: systematic review of randomized controlled trials. BMJ, 324(7351), 1426–1430.
Acknowledgments
This research received no grant from any funding agency. We thank the students, teachers and principals/proprietors of secondary schools that participated in this study in Anambra state, Nigeria for their invaluable contributions towards this work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ochiogu, I.N., Miettola, J., Ilika, A.L. et al. Impact of Timing of Sex Education on Teenage Pregnancy in Nigeria: Cross-sectional Survey of Secondary School Students. J Community Health 36, 375–380 (2011). https://doi.org/10.1007/s10900-010-9318-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-010-9318-6