
Abstract
Cultural variations between communities may impact injury rates, especially among children. We conducted a retrospective study of three communities in Israel using data from the Israel National Trauma Registry (1998–2007). Pediatric injury hospitalization rates in urban communities with varied levels of socio-economic status (low, medium, and high) were compared for all injuries and cause-specific injuries. Age-standardized and age-specific rates were calculated. Age-standardized injury hospitalization rates were lowest for the low socio-economic status (SES) community (299.7, 95% confidence interval [CI] 289.8–309.6) compared to the medium SES (658.2, 95% CI 629.1–687.3) and high SES (443.7, 95% CI 422.2–465.3) communities. Similar rates were observed for injuries from falls, transportation, accidental striking and intentional causes. For example, rate ratios for falls were 149.1 (95% CI 142.0–156.2), 340.8 (95% CI 319.5–362.1) and 245.7 (229.9–261.5) in the low, medium and high SES communities, respectively. Deviations from these overall trends were noted, however, for pedestrian injuries and burns that were relatively higher in the low SES community and injuries from motorized vehicles that were greater among children living in the high SES community. These results suggest that strong social capital is associated with reduced pediatric injury risks regardless of community wealth. However, targeted interventions for reducing injuries in at-risk populations that rely solely on injury rates may omit culturally distinct communities and overlook their uneven burden to the trauma care system.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Childhood injuries are responsible for close to a million deaths globally while non-fatal injuries, frequently resulting in hospitalizations and lifelong disabilities, affect tens of millions of children worldwide [1, 2]. Risks of injury are influenced by individual and contextual factors such as demographic, social and economic characteristics [1, 3–5]. While there is substantial evidence of an inverse relationship between socioeconomic status (SES) and risks of non-fatal injury, the relationship between social capital and injury is less clear [3, 5, 6].
The causal relationship linking SES and injury includes psychosocial factors, access to material resources and health behaviors [3, 7]. Similar pathways relate social capital to injury on the community level and primarily include societal attitudes and norms that foster healthy behaviors, reduce emotional and behavioral stressors and promote reciprocity [6, 8, 9]. Distinguishing between the effects of SES and social capital on injury may not be clear since many factors are interdependent [10]. This relationship is further complicated by the intent and cause of injury. For example, risk of violent and self-inflicted injuries are correlated with individuals and communities of low SES, weak family and community ties, and high levels of neglect, abuse and antisocial behavior [6, 11]. Injuries such as violence are more likely to occur in or around the home for adolescents of lower SES, while sports and recreational injuries are more prevalent among those more affluent [11, 12]. In a recent study, economic deprivation and social fragmentation were inversely related to childhood injuries from motor vehicle riders; in fully adjusted models however, no association between economic or social factors were found with intentional injuries [5]. Safety measures and targeted interventions intended to reduce a broad spectrum of injuries across diverse population subgroups may have a limited effect, since safety-related behaviors and attitudes vary by contextual socio-economic and social attributes [5, 11, 12].
Childhood injuries are one of the leading causes of death among children in Israel at a rate of about 5 per 1,00,000 children ages 1–14 years [13]. In 2006, traffic-related injuries were estimated at about 233 per 1,00,000 children ages 0–17 years [14]. Injury rates across the Israeli society likely differ, since behaviors and attitudes towards risk-taking and preventive behaviors vary between sub-populations [15–17]. Ethnic and religious groups in Israel have diverse demographic, cultural and economic characteristics and values. Often these groups, that seek to maintain traditions, retain cultural norms and offer mutual support, live in closed neighborhoods. Examples of this type of self-segregation are Ultra-Orthodox Jews who comprise approximately 5% of the Israeli population [18]. Homogeneity of communities has been associated with increased social capital and specifically, collective efficacy, which has been used to explain health advantage, as opposed to integrated communities in which health disparities have been observed [19, 20].
In general, Ultra-Orthodox communities are close-knit, clustered societies that encourage reduced contact with the outside secular world in order to focus on spiritual rather than material wealth [18, 21]. These communities are hierarchical with a rabbinic leader providing guidance on all religious and secular matters. Men assume communal responsibilities including participation in public prayer three times daily while women care for the home and children. Ultra-Orthodox communities typically comprise two-parent, large families (average 7.7 children per woman), living in densely populated areas, with self-limited formal secular education and low employment rates among males [18, 21]. Adolescent boys and men through age 40 years, are encouraged to devote themselves to religious study, typically in religious seminaries (‘yeshiva’), a phenomenon that all but guarantees a welfare-dependent lifestyle or voluntary poverty [21].
As an indicator of social capital, religion reflects mutual insurance networks, strong generalized reciprocity that includes honesty and trust, and greater involvement in altruistic and civic activities [17, 21, 22]. Numerous studies have used religious affiliation to represent social capital in order to predict morbidity and mortality [17, 23–25]. For example, in Israel, smoking rates among religious women are almost negligible and rates of physical activity are low [17, 24, 26]. Jaffe et al. showed that, after accounting for individual—and area—level SES, men and women living in religiously affiliated areas had lower mortality rates than those living in unaffiliated areas [25].
The present study examined pediatric injury hospitalization rates in low, medium and high area-SES urban communities in Israel. Changes in the SES gradient in injury rates were anticipated due to the cultural and social capital differences between communities.
Methods
Data
A retrospective study was performed using data from the Israel National Trauma Registry (ITR) from January 1, 1998 through December 31, 2007. During this study period the ITR recorded all trauma hospital admissions, in-hospital deaths or transfers to 10 of 24 trauma centers in Israel (all six level I trauma centers and four of the largest regional level II trauma centers). The ITR includes patient information such as demographic characteristics, injury details, hospital utilization and discharge information. Data are uniformly collected by trained medical registrars at each trauma center and electronic files are transferred to the ITR for quality assurance.
Community Selection
Three urban communities were selected for comparison of pediatric injury hospitalizations based on the following criteria: (1) high coverage by the ITR, (2) representation of each level of socio-economic status—low, medium and high, (3) similar geographic location (i.e., urban communities in central Israel), and (4) ethnic homogeneity (>93% Israeli Jews) [27]. While the ITR covers a wide range of the population in Israel, the availability of data for low SES communities is limited. For example, many low SES communities are located in areas in the periphery of Israel where trauma hospitalization data are not recorded in the ITR.
Identification of an Ultra-Orthodox community satisfying these criteria was based on the designation of area-level Ultra-Orthodox homogeneity by the ICBS [18]. In Israel, forty-two geographic areas ranging from statistical areas of 5,000+ residents to entire towns were identified by the ICBS as having a high degree of Ultra-Orthodox homogeneity [18]. Designation of these areas was based on voting patterns from the 1996 national elections, which has been shown to be a strong indicator of individual—and area—level religious affiliation [25, 28, 29]. The Ultra-Orthodox classification included demographic and socio-economic factors such as population growth, fertility rates, % unemployment, median age, number of children and elderly, marital status and income, which differ substantially from national averages [18].
For the purposes of the present study, the community of Bnei B’rak was considered to have a high degree of Ultra-Orthodox homogeneity. Of its 31 statistical areas, 17 had a high degree of homogeneity, eight were moderately homogenous and six had a low degree of homogeneity [21]. Two other urban communities, Hadera and Ramat Gan were not considered to have any degree of Ultra-Orthodox homogeneity, but fulfilled the study criteria (Table 1). Coverage of these three communities by the ITR was considered to be high based on data from the Ministry of Health [30].
Socio-economic Status
Socio-economic status was calculated for each municipality by the Israel Central Bureau of Statistics [31]. This ranking, ranging from 1 to 10 (low to high), was based on numerous indicators of social and economic position including financial resources, housing density and quality, home appliances, motorization level, schooling and education, employment and unemployment profile, dependency ratio and family composition. The socioeconomic profile of the three communities remained stable throughout the study period: Bnei B’rak = 2 (herein ‘low SES’), Hadera = 5 (herein ‘medium SES’) and Ramat Gan = 8 (herein ‘high SES’).
Outcome Variables
E-codes were used to categorize injuries. Unintentional injuries were divided into five groupings: falls, transportation, accidental striking, burns and other unintentional injuries. Falls included falls from a height (e.g., tree or ladder, or into a pit), furniture, stairs, playground structure, sport-related falls (e.g., while riding scooters, roller skating, playing football or running), slips, same-level falls and other non-specific falls. Transportation injuries were categorized as pedestrian, bicycle, motorized vehicles and other causes. Thermal burns (herein ‘burns’) were dichotomized into burns from flames or from a hot substance (herein ‘flames’) or scalds and contact burns (herein ‘scalds’). Accidental striking was classified as either being struck by a falling object or striking against or colliding into a person or object. Other unintentional injuries included accidental cuts or pierces. Intentional injuries included assault (e.g., brawl or injury inflicted by another person) and other injuries (e.g., self-inflicted injuries, terror—and war—related injuries). The injury severity score (ISS) was calculated as mild (1–8), moderate (9–14), severe (16–24) and critical (25 +).
Statistical Analysis
Age-adjusted injury rates per 1,00,000 person-years were standardized to the Israel pediatric population for 0–17 year olds. The pediatric population size for each community remained fairly stable throughout the study period and therefore denominator data and distribution according to age groups, 0–4, 5–9, 10–14 and 15–17 years, was based on population data from 2003 [31]. Associations were estimated using chi-square and Fisher’s exact tests and analysis of variance. Analyses were performed using SAS (version 9.2) and PEPI statistical software.
Results
Over the 10 year study period 4,544 children ages 0–17 years living in a low, medium or high SES community in Israel had injuries resulting in a hospitalization (Table 2). Age of patients differed between communities (P < 0.001). Injury severity rates varied between communities, with more severe and critical injuries (ISS 16+) in the medium than in the low and high SES communities (P = 0.001). Unintentional injuries were the primary cause of injury in all communities, however the prevalence of intentional injuries was higher in the medium SES community compared to the low or high SES communities (P < 0.001).
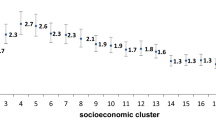
Age-adjusted injury hospitalization rates for each community according to injury type are presented in Table 3. Age-standardized rates per 100,000 person-years were 300, 658 and 444 for the low, medium and high SES communities, respectively. Rate ratios relative to the high SES community followed a similar pattern for most childhood injuries whereby higher rates were observed in the medium SES community (RR = 1.48, 95% CI 1.39–1.58) and lower rates were seen in the low SES community (RR = 0.68, 95% CI 0.64–0.72).
Falls
Ninety-seven percent of fall-related injuries occurred to boys and were mild or moderate in severity. Cause of falls differed between communities (P < 0.05). Injury hospitalization rates in each community decreased with age (Fig. 1a). Rate ratios showed a protective effect for children living in the low SES community (RR = 0.61, 95% CI 0.56–0.66) and detrimental effect of the medium SES community (RR = 1.39, 95% CI 1.27–1.52) when compared to the high SES community.

Rates of hospitalization from childhood injuries per 1,00,000 person-years by cause and community characteristics
Transportation
More pedestrian and fewer motorized vehicle injuries occurred in the low SES community than in the other two communities. Injuries were primarily mild and moderate in severity (92%), however, in the medium SES community there was a substantially higher prevalence of severe to critical injuries—13% compared to 6–7% in the low and high SES communities, respectively (P < 0.001). Injury rates by age group are presented in Fig. 1b. Rate ratios showed that children living in the low or medium SES communities compared to those in the high SES community were more likely to sustain pedestrian injuries (RRlow SES = 1.33, 95% CI 1.09–1.63; RRmedium SES = 1.71, 95% CI 1.33–2.19). Rate ratios for motorized vehicles were lower in the low and medium SES communities compared to the high SES community, although only significant in the former.
Burns
Burns represented a higher percentage of pediatric injury hospitalizations for the low SES community compared to the other communities (9 vs. 5–6%, respectively). Burn injuries were slightly more prevalent among girls in the low SES community than in the other communities (40 vs. 29%, respectively), although differences were not statistically significant. Cause of burn (flames vs. scalds) differed significantly by community (P < 0.001). Age-specific rates were relatively high for 0–4 year olds and decreased with age (Fig. 1c). Rate ratios showed an increased rate of injury among low (RR = 1.31, 95% CI 1.01–1.70) and medium (RR = 1.92, 95% CI 1.41–2.62) SES communities compared with the high SES community.
Struck, Accidental
Approximately 70% of all accidental striking were from collisions with a person or object. Injuries from an accidental striking were more prevalent among boys than girls (76 vs. 24%, respectively). Injury rates for each community remained relatively stable across age groups (Fig. 1d). Rate ratios revealed that in comparison to children living in the high SES community, injuries from accidental striking were less likely among children living in the low SES community (RR = 0.58, 95% CI 0.47–0.71) and more likely among those in the medium SES community (RR = 1.51, 95% CI 1.22–1.88).
Other Unintentional
Accidental cuts or pierces represented 59% of all other unintentional injuries. While boys were more likely to be hospitalized with unintentional injuries than girls (69 vs. 31%, respectively), the male-to-female ratio varied for each community (P = 0.009): low SES = 3.2:1; medium SES = 2.3:1; and high SES = 1.3:1. Most injuries (>97%) were mild to moderate in severity. Other unintentional injury hospitalization rates for each community were fairly stable across age-groups (Fig. 1e). Rate ratios showed that in comparison to the high SES community there was a protective effect of low SES and detrimental effect of medium SES on injuries.
Intentional
Intentional injuries comprised less than 3% of all pediatric trauma hospitalizations. Boys were more likely than girls to be hospitalized from an intentional injury (82 vs. 18%, respectively) and injuries were more prevalent among children 10+ years, but varied substantially by community (P = 0.010). Ninety-two percent of all hospitalizations for intentional injuries were mild to moderate injuries. Intentional injury rates were relatively low for the low and high communities compared with the medium SES community (Fig. 1f). Age-adjusted rates varied substantially across communities with four injuries per 100,000 in the low SES community, 32 injuries per 100,000 in the medium SES community and 8 injuries per 100,000 in the high SES community. Rate ratios showed a substantial protective effect of low SES (RR = 0.49, 95% CI 0.30–0.82) and detrimental effect of medium SES compared to high SES (RR = 4.08, 95% CI 2.71–6.14).
Discussion
We found no evidence of a socio-economic gradient in injury hospitalization rates likely due to the influence of cultural and social capital differences between communities. Injury hospitalization rates among children 0–17 years differed by cause of injury according to individual and area characteristics. Children living in the low SES community had consistently and significantly lower injury hospitalization rates than those living in communities with higher SES. Lower injury rates among children in the low SES area likely reflect communal characteristics unique to the community’s religious affiliation. Deviations from these overall trends were noted for pedestrian injuries and burns that were relatively higher in the low SES community and injuries from motorized vehicles that were greater among children living in the high SES community. These observations may be explained by cultural and social attributes of the low SES community. In particular, the strong social capital that the Ultra-Orthodox community possesses may mediate the influence of SES on injury.
Two of the major preventive strategies for childhood injuries include improved supervision and a safe environment [1]. Socio-economic conditions and the disruption of social networks may directly and indirectly affect these factors [1, 32]. In disadvantaged families, for example, children may not only be left unsupervised, but find themselves acting as caregivers to younger siblings [1, 32]. Although we did not measure supervision, strong social capital within the Ultra-Orthodox community, such as reciprocity (rule adherence), self organization or the collective efficacy (assuming a part in the collective), and safe environments (responsibility to social resources) may have provided the protective influence of a supervising adult on injuries that occur outside of the home, namely falls, transportation injuries and intentional injuries [33]. In addition to these preventative measures, cultural attitudes may affect injury rates. The Amish community may be a useful comparison group to the Ultra-Orthodox since they are a conservative, private community with emphasis on large families and strong social networks [34, 35]. One study of childhood injuries in that community showed that injuries often occur when children are given farm jobs that they are physically or mentally unable to perform [35]. It may well be that in the Ultra-Orthodox communities older children have care-giving responsibilities and are unable to judge potential risks that lead to scalds during bath time or pedestrian injuries when accompanying a younger sibling across the street.
Hospitalization rates are likely affected by risk exposures that vary by community according to SES and culture. For example, individuals from low SES communities may have increased exposure to pedestrian injuries since resources such as sidewalks and private motor vehicles are limited. The positive association between motor vehicle injuries and area SES may reflect increased access to cars among those in wealthier areas [5, 31]. In a recent study, pediatric injuries varied by ethnicity regardless of area deprivation [7]. It may well be that exposure risks are affected by the cultural norms of the Ultra-Orthodox community. The reduced rate of transportation injuries and relatively increased rates of burns in this community may be attributed in part to the religious observance of the Sabbath. The Sabbath laws prohibit “work” during a 25-hour period—from approximately sunset on Friday to sunset on Saturday. The work prohibition includes transportation via motorized vehicles and cooking. In practice, the Ultra-Orthodox community benefits from a one-seventh risk reduction from transportation exposure especially on weekends when traffic injury risks are increased. An increased exposure risk to burns may be due to increased exposure to electric hot plates and urns used to warm food and water on the Sabbath (instead of cooking) [36, 37]. This ‘Sabbath’ theory has been proposed previously to explain the reduced risk of cardiovascular disease due to smoking among religious versus secular Jewish kibbutz members [24].
As already noted, intentional injuries are associated with low SES. [3, 6, 11] In addition, decreased social connectedness and low levels of mutual trust are correlated with increased anxiety and depression, higher levels of firearm ownership and aggressive behaviors [6, 38]. Many studies have shown that church or synagogue attendance is a key indicator of strong social networks that benefits one’s mental health [8, 25]. Kark et al. (1996b) showed that religious compared with secular kibbutz members had a greater sense of coherence and less hostility [39]. The strict communal requirements among adolescent boys and men may enhance their sense of belonging and mutual responsibility while reducing loneliness and depression—factors that are associated with violent behaviors. In the present study, children living in the low SES community had substantially lower rates of intentional injuries and those living in the medium SES community had substantially higher rates of intentional injuries compared to the high SES community. The low rates in the low SES community may also be affected by the cultural norm within the Ultra-Orthodox culture of sending high-school boys to dormitory ‘yeshiva’ schools with strict learning schedules for many hours each day and a devotion to religious practice that may limit their exposure to risky behaviors and intentional injuries [21]. In addition, the aggressive behavior associated with poverty may not be applicable to the Ultra-Orthodox population, as their lifestyle is by choice. Berman notes that present in this poor Ultra-Orthodox community are extraordinarily high degrees of mutual insurance and charity [21]. Thus, communities created by choice may represent a model of strong social capital that represents an effective pathway for injury prevention regardless of material wealth.
Estimations of community-specific hospitalization rates are useful for identifying at-risk groups and designing prevention strategies. The Ultra-Orthodox community of Bnei B’rak had surprisingly low childhood injury rates but substantially high numbers of injuries relative to the other two communities. Thus, while the high social capital belonging to the Ultra-Orthodox society may have provided a protective effect on injury risks, the positive cultural attitude toward larger families increased exposure risks and resulted in greater absolute numbers of cases. Targeted interventions for reducing injuries in at-risk populations that rely solely on injury rates may omit this low SES Ultra-Orthodox community and overlook its uneven burden to the trauma care system.
Strengths and Limitations
In the present study, hospitalization and injury rates for injuries and distribution according to etiology, age group and gender were consistent with previous studies from Israel and other Western countries thus adding to the external validity of the study [1, 4, 16, 40, 41]. We note that the ecological design of this study allows for hypothesis generating only and not for establishing causality. In addition, social capital was not directly measured, rather religious affiliation was used as a proxy, though this variable has been used previously and is supported in the literature [21, 23, 25, 39]. Access to hospital trauma care was considered to be similar between communities since Israel maintains a universal medical care system whereby all residents have access to basic medical care. Patients were identified according to residence and not place of injury, thereby increasing the likelihood of identifying all trauma injuries. Injury rates for children who were admitted to a clinic or to an emergency room and were not hospitalized were not included in this study. While minor injuries are not accounted for, we expect the data to include all moderate and severe injuries where medical attention was needed. Ideally, the inclusion of a low social capital/low SES community would have strengthened the results; however data for this community-type was not available in the ITR.
Conclusion
The influence of SES on injury rates is not straightforward and poverty alone does not predict injury. Community differences in pediatric injury rates are likely the influence of strong cultural and community traits, in addition to area SES. In the challenge to reduce childhood injuries, attention to cultural variability and social capital must be considered as pathways to reducing and preventing injuries.
References
Peden, M., Oyegbite, K., Ozanne-Smith, J., et al. (2008) Geneva: World report on child injury prevention. World Health Organization.
World Health Organization (2008). Geneva: Global burden of disease: 2004 update. World Health Organization.
Cubbin, C., & Smith, G. S. (2002). Socioeconomic inequalities in injury: Critical issues in design and analysis. Annual Review of Public Health, 23, 349–375.
Edwards, P., Green, J., Lachowycz, K., Grundy, C., & Roberts, I. (2008). Serious injuries in children: Variation by area deprivation and settlement type. Archives of Disease in Childhood, 93, 485–489.
Laflamme, L., Hasselberg, M., Reimers, A. M., Cavalini, L. T., & Ponce de Leon, A. (2009). Social determinants of child and adolescent traffic-related and intentional injuries: A multilevel study in Stockholm county. Social Science and Medicine, 68, 1826–1834.
Mercy, J. A., Mack, K. A., & Steenkamp, M. (2007). Changing the social environment to prevent injuries. In L. S. Doll, S. E. Bonzo, J. A. Mercy, D. A. Sleet, & E. N. Haas (Eds.), Handbook of injury and violence protection (pp. 277–294). New York: Springer.
Steinbach, R., Green, J., Edwards, P., & Grundy, C. (2010). ‘Race’ or place? Explaining ethnic variations in childhood pedestrian injury rates in London. Health Place, 16, 34–42.
Berkman, L. F., Glass, T., Brissette, I., & Seeman, T. E. (2000). From social integration to health: Durkheim in the new millennium. Social Science and Medicine, 51, 843–857.
Kawachi, I., & Berkman, L. S. (2000). Social cohesion, social capital, and health. In I. Kawachi & L. S. Berkman (Eds.), Social epidemiology (pp. 174–190). New York: Oxford University Press.
Geckova, A., van Dijk, J. P., Stewart, R., Groothoff, J. W., & Post, D. (2003). Influence of social support on health among gender and socio-economic groups of adolescents. European Journal of Public Health, 13, 44–50.
Pickett, W., Molcho, M., Simpson, K., et al. (2005). Cross national study of injury and social determinants in adolescents. Injury Prevention, 11, 213–218.
Williams, J. M., Currie, C. E., Wright, P., Elton, R. A., & Beattie, T. F. (1997). Socioeconomic status and adolescent injuries. Social Science and Medicine, 44, 1881–1891.
Stein, N., Aboraba, M., & Haklai, Z. (2008). Leading causes of death in Israel, 1998–2004. Jerusalem (Israel): Ministry of Health. (Hebrew).
Israel Police Force. Road Accidents. In: Zionit, Y., Kimchi, M., Ben-Aryeh, A., eds. (2006). Children in Israel. Jerusalem (Israel): National center for children, 200, p 303 (Hebrew).
Gofin, R., Avitzour, M., Haklai, Z., & Jellin, N. (2002). Injury inequalities: Morbidity and mortality of 0–17 year olds in Israel. International Journal of Epidemiology, 31, 593–599.
Savitsky, B., Aharonson-Daniel, L., Giveon, A., & Peleg, K. (2007). Israel trauma group. Variability in pediatric injury patterns by age and ethnic groups in Israel. Ethnicity & Health, 12, 129–139.
Shmueli, A., & Tamir, D. (2007). Health behavior and religiosity among Israeli Jews. The Israel Medical Association Journal, 9, 703–707.
Gurovich, N., & Cohen-Kastro, E. (2004). Ultra-Orthodox Jews: Geographic distribution and demographic, social and economic characteristics of the Ultra-Orthodox Jewish population in Israel, 1996–2001. Jerusalem (Israel): Israel Central Bureau of Statistics. (Hebrew).
Cagney, K. A., Browning, C. R., & Wallace, D. M. (2007). The Latino Paradox in neighborhood context: The case of asthma and other respiratory conditions. American Journal of Public Health, 97, 919–925.
LaVeist, T., Thorpe, R., Jr, Bowen-Reid, T., et al. (2007). Exploring health disparities in integrated communities: Overview of the EHDIC Study. Journal of Urban Health, 85(1), 11–19.
Berman, E. (2006). Sect, subsidy, and sacrifice: An economist’s view of Ultra-Orthodox Jews. Quarterly Journal of Economics, 115(3), 905–953.
Putnam, R. (2000). Bowling alone (pp. 65–79). New York: Simon & Schuster.
Hyyppä, M. T., & Mäki, J. (2003). Social participation and health in a community rich in stock of social capital. Health Education Research, 18, 770–779.
Kark, J. D., Carmel, S., Sinnreich, R., Goldberger, N., & Friedlander, Y. (1996). Psychosocial factors among members of religious and secular kibbutzim. Israel Journal of Medical Sciences, 32, 185–194.
Jaffe, D. H., Eisenbach, Z., Neumark, Y. D., & Manor, O. (2005). Does living in a religiously affiliated neighborhood lower mortality? Annals of Epidemiology, 15, 804–810.
Baron-Epel, O., Haviv, A., Garty, N., Tamir, D., & Green, M. S. (2005). Who are the sedentary people in Israel? A public health indicator. The Israel Medical Association Journal, 7, 694–699.
Central Bureau of Statistics. Geographic location of ultra-orthodox communities according to the level of religious homogeneity. Israel: http://www.cbs.gov.il/popisr/haredi_areas_2003.xls Accessed 2 Feb 2010.
Anson, J., & Meir, A. (1996). Religiosity, nationalism, and fertility in Israel. European Journal of Population, 12, 1–25.
Arian, A., & Shamir, M. (1986). The elections in Israel–1984. New Brunswick: Anson Transaction Books.
Haklai, Z., Gordon, S., Hillel, S., & Aburaba, M. (2009). Emergency department visits: Demographic characteristics, 2004–2007. Jerusalem (Israel): Ministry of Health. (Hebrew).
Central bureau of statistics. Local authorities in Israel, 2003. Israel: http://www.cbs.gov.il/www/publications/local_authorities03/local_authorities03_h.htm Accessed 2 Feb 2010.
Khambalia, A., Joshi, P., Brussoni, M., Raina, P., Morrongiello, B., & Macarthur, C. (2006). Risk factors for unintentional injuries due to falls in children aged 0–6 years: A systematic review. Injury Prevention, 12, 378–381.
Inclán, C., Hijar, M., & Tovar, V. (2005). Social capital in settings with a high concentration of road traffic injuries. The case of Cuernavaca, Mexico. Social Science and Medicine, 61, 2007–2017.
Herd, J. P. (2006). The shape of high fertility in a traditional Mennonite population. Annals of Human Biology, 33, 557–569.
Vitale, M. A., Rzucidlo, S., Shaffer, M. L., Ceneviva, G. D., & Thomas, N. J. (2006). The impact of pediatric trauma in the Amish community. Journal of Pediatrics, 148, 359–365.
Benmeir, P., Sagi, A., Rosenberg, L., Picard, E., & Ben Yakar, Y. (1989). ‘Sabbath’ electric plate burn: A ritual hazard. Burns, Including Thermal Injury, 15, 39–41.
Haik, J., Liran, A., Tessone, A., et al. (2007). Burns in Israel: Demographic, etiologic and clinical trends, 1997–2003. The Israel Medical Association Journal, 9, 659–662.
Hemenway, D., Kennedy, B. P., Kawachi, I., & Putnam, R. D. (2001). Firearm prevalence and social capital. Annals of Epidemiology, 11, 484–490.
Kark, J. D., Shemi, G., Friedlander, Y., Martin, O., Manor, O., & Blondheim, S. H. (1996). Does religious observance promote health? Mortality in secular vs. religious kibbutzim in Israel. American Journal of Health Promotion, 86, 341–346.
Agran, P. F., Winn, D., Anderson, C., Trent, R., & Walton-Haynes, L. (2001). Rates of pediatric and adolescent injuries by year of age. Pediatrics, 108, E45.
Sinclair, S., Smith, G., & Xiang, H. (2006). A comparison of nonfatal unintentional injuries in the US among US born and foreign born persons. Journal of Community Health, 31(4), 303–325.
National Council for Child Safety (2004). Children in Israel statistical abstract. Jerusalem (Israel): National Council for Child Safety. 67–70 (Hebrew).
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
The Israel Trauma Group includes: Ricardo Alficci, MD, Igor Jeroukhimov, MD, Boris Kassel, MD, Yoram Klein, MD, Moshe Michaelson, MD, Avraham Rivkind, MD, Gad Shaked, MD, Daniel Simon, MD, Dror Soffer, MD, and Michael Stein, MD.
Rights and permissions
About this article
Cite this article
Jaffe, D.H., Goldman, S., The Israel Trauma Group. et al. The Role of Community in Pediatric Injury. J Community Health 36, 244–252 (2011). https://doi.org/10.1007/s10900-010-9304-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-010-9304-z