
Abstract
Studies examining risk factors for problem gambling amongst sports bettors have used screens that assess gambling problems in general. Because people experiencing gambling-related problems tend to gamble on multiple forms, it is unclear whether problems identified amongst sports bettors are due to sports betting itself. The present study examined a range of distal and proximal demographic, behavioural and psychological risk factors using a modified version of the Problem Gambling Severity Index which respondents answered only in relation to their sports betting. In general, those at risk were younger, spoke a language other than English, were more engaged sports bettors and gamblers, and tended not to watch the event they had bet on. They particularly endorsed money-oriented motivations, and had higher erroneous cognitions, gambling urges, and were more likely to experience alcohol issues. Higher-risk sports bettors were also more likely to apportion less responsibility for their gambling to themselves, and to have lower self control. A penalised model found that key predictors were money motivations, gambling urges and erroneous cognitions, alcohol issues and lower self-control, but not sports betting behaviour. These findings suggest that one’s psychological relationship to sports betting is a primary driver of gambling-related problems, rather than just betting behaviour. As sports betting expands through new products and legalisation in additional jurisdictions, understanding who is most at risk from this form of gambling is important to inform legislation as well as harm reduction and treatment measures.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sports betting is increasing worldwide through increased turnover in existing markets and expansion into new markets as legislation becomes more liberal. Given technological advances that allow innovations such as in-play betting and micro-betting, the structural nature of sports betting is changing, and sports betting is increasingly linked to problem gambling. In Australia, where the current study was conducted, 41% of at-least monthly sports bettors experience one or more gambling problems (Armstrong and Carroll 2017). However, recent studies into risk factors for problem gambling amongst sports bettors have found that those with gambling problems tend to be more involved gamblers who engage in a higher number of additional gambling forms (Hing et al. 2016; LaPlante et al. 2014). These studies have used the Problem Gambling Severity Index (PGSI; Ferris and Wynne 2001) or similar measures as the dependent variable, which ask about problems relating to gambling in general, not specifically to sports betting. It is therefore unclear if sports bettors classified as problem gamblers with these general screens experience gambling problems related specifically to their sports betting, or instead related to other forms of gambling they may engage in. This distinction is important to understand the contribution of sports betting to gambling problems and harms, and the risk factors specifically associated with problematic sports betting. To advance this understanding, this study used an adapted measure of problem gambling severity specific to sports betting and assessed associated risk factors. Improved knowledge of demographic, psychological and behavioural risk factors for sports betting problems can inform appropriate harm reduction efforts and treatment approaches. Previous studies of these risk factors amongst sports bettors are reviewed below to identify salient variables for inclusion in the current study; however, they have all used general measures of problem gambling severity.
Demographic Risk Factors Amongst Sports Bettors
Previous research has found that being young and male is a consistent risk factor for gambling-related problems in general (Johansson et al. 2009), as well as amongst sports bettors, who may also gamble on other forms (Russell et al. 2018b). Other demographic factors associated with gambling-related problems include being single, educated, and employed or studying full-time (Hing et al. 2016), although these factors are likely to be confounded with age (Delfabbro 2012). Contradictory results have been found for other demographic factors, notably income and ethnicity (Hing et al. 2016, 2017b; Russell et al. 2018b). Overall, young adult males appear to be the most at-risk group of sports bettors, and this is reflected amongst clients seeking treatment for sports betting-related problems (Hunt 2017), including financial problems (Financial Counselling Australia 2015). This demographic profile is not surprising, given that young men are the main targets of prolific sports betting advertising, which in turn has been shown to increase sports betting expenditure (Hing et al. 2018c; Sproston et al. 2015).
Behavioural Risk Factors Amongst Sports Bettors
Sports bettors at risk of gambling-related problems tend to be more involved gamblers. They spend more, bet more often, tend to have accounts with multiple operators, bet using more diverse modes of access, including online, by telephone and in land-based betting venues, and on a greater variety of domestic, foreign and international events (Braverman and Shaffer 2012; Gainsbury et al. 2013, 2015; LaBrie and Shaffer 2011; Wardle et al. 2011). In Australia, in-play or live betting cannot be offered by Australian-licensed wagering operators online; bettors must place in-play bets via a telephone call or in a venue. Because more problematic sports bettors tend to bet in-play (Hing et al. 2018; Russell et al. 2018b), including betting on micro events (Russell et al. 2018a), modes of access are also recognised as risk factors, particularly placing a higher proportion of bets via telephone amongst moderate risk and problem gamblers (Russell et al. 2018b). Sports bettors at risk of gambling-related problems also tend to bet on other forms of gambling (Hing et al. 2016; LaPlante et al. 2014), which obscures the contribution of sports betting to problem gambling severity when measured using general screens.
Using a higher number of payment methods may also be associated with gambling-related problems amongst sports bettors. In reviewing case studies of Australians with severe financial losses and debts due to uncontrolled and problematic sports betting, Financial Counselling Australia (2015) identified betting using credit cards, operator credit and payday loans as demonstrably more risky than betting using one’s own money. Some payment methods for online betting are instant (e.g., a cash advance via credit card), so may be particularly used for impulse betting, which is more common amongst bettors with gambling problems (Hing et al. 2018a, b). In addition, credit cards, operator credit and payday loans have inflated interest rates, potentially increasing the financial harms from betting. While most Australian online gamblers (71%) report that betting via credit card has no impact on their spending, and is their most common payment method for online gambling (Hing et al. 2014), the inherent risks of betting using any form of credit means that payment methods used are worthy of investigation as a potential risk factor for gambling problems amongst sports bettors.
Research into gambling motivations has found that that emotion-focused reasons (rather than to make money) predict problem gambling (Flack and Morris 2015), although this has not been investigated specifically for sports betting. Nevertheless, numerous studies identify emotionally charged reasons for sports betting. One study comparing betting motivations amongst weekly and occasional sports bettors found that the former were more likely to endorse betting because: they “enjoy a punt”, to increase the excitement of watching sport, to utilise their extensive knowledge of sport, “for an adrenaline rush”, to get ahead financially, to chase losses, to ease boredom, in response to advertising and promotions, and because betting is easily accessible (Jenkinson et al. 2018). Qualitative research has identified competition amongst peers, demonstrating loyalty to favourite sports/teams/players, and displaying acumen in their knowledge of the game and in navigating the odds to come out on top, as fundamental drivers of sports betting amongst friendship groups of young male sports bettors (Gordon et al. 2015). Perceived as involving an element of skill, sports betting wins can enhance ego, cultural capital and social standing (Raymen and Smith 2017). A grounded theory analysis concluded that young men undertook sports betting primarily to bond with and demonstrate competence to others, for excitement, and to enhance masculine identity and social acceptance (Lamont and Hing 2018). In comparing motivations for different gambling forms, Fang and Mowen (2013) found that those driving sports betting were to make money, for self-esteem enhancement and for social interaction. These diverse motivations for sports betting suggest that it is worth examining those that may distinguish problematic sports betting.
Psychological Risk Factors Amongst Sports Bettors
A range of psychological factors are considered direct risk factors for problem gambling as they represent the more immediate influences on the likelihood of developing gambling problems (Williams et al. 2012). One of these is erroneous cognitions which have been recognised as an important component of problem gambling (Blaszczynski and Nower 2002), with elevated levels generally found amongst those with gambling problems (e.g., Lindberg et al. 2014; Michalczuk et al. 2011). These faulty cognitions can include: interpretive bias (cognitions relating to reframing gambling outcomes), illusion of control (cognitions relating to ability to control gambling outcomes), predictive control (cognitions relating to ability to predict gambling outcomes), gambling-related expectancies (cognitions relating to how they expect gambling to affect them), and perceived inability to stop gambling (Raylu and Oei 2004a). Erroneous cognitions have typically been researched in relation to games of pure chance, such as electronic gaming machines, and little is known about erroneous cognitions for sports betting. However, they have specifically been related to gambling problems amongst online gamblers (MacKay and Hodgins 2012), including in Australia (Gainsbury et al. 2015), where sports betting is one of the few forms that can legally be provided by Australian-licensed operators. Further, a study of betting by expert hockey players concluded that the “skills” of these sports bettors represented cognitive distortions, with perceptions of expertise reinforced by interpretive biases and near-misses (Cantinotti et al. 2004). As such, a higher level of erroneous cognitions may be a risk factor for problem gambling amongst sports bettors.
Gambling-related urges are also commonly associated with problem gambling (Raylu and Oei 2004b). They can arise from both internal (e.g., depression) and external (e.g., gambling advertising) sources (Smith et al. 2013), and have also been associated with relapse (Smith et al. 2015). As such, urges are also likely to be a risk factor for problem gambling amongst sports bettors, particularly because urges may be triggered by the plethora of sports betting advertising common in various jurisdictions (Hing et al. 2015, 2018c; Lopez-Gonzalez et al. 2017, 2018a, b; Pitt et al. 2017).
Comorbidities between problem gambling and alcohol use disorder have frequently been observed (Baldo et al. 2006; Cowlishaw 2014; Grant et al. 2002; Hing et al. 2017a; Lorains et al. 2011; Russell et al. 2018c; Sundqvist et al. 2015). A systematic review and meta-analysis of population representative studies examining comorbid disorders and problem gambling found a mean prevalence of 28.1% for alcohol use disorder amongst problem and pathological gamblers, although this ranged from 9.9 to 73.2% across the 11 different studies examined (Lorains et al. 2011). While rates of alcohol use disorder amongst sports bettors are not known, studies have found that alcohol is often consumed while sports betting (Gordon et al. 2015; Raymen and Smith 2017), and this appears to be more common amongst regular sports bettors. For example, Jenkinson et al. (2018) found that 73% of weekly sports bettors bet when affected by alcohol, compared to 55% of occasional sports bettors. They point out that sports betting often occurs in licensed venues, sports betting and alcohol are often marketed together, and young men are high consumers of both products. Further, about half of sports bettors in their study reported spending more money or placing more bets than intended when affected by alcohol. Lamont et al. (2016) also found that impulse betting was more likely when drinking alcohol. Given the well established links between alcohol use and misuse and problem gambling, these links warrant examination in the current study.
Lack of self-control has been widely recognised as a key cause of gambling problems, with a subjective sense of impaired control being a defining feature of problem gambling (Bergen et al. 2014; Blaszczynski and Nower 2002; Dickerson and O’Connor 2006). Impaired self-control over gambling behaviour also appears to reflect lower trait self-control in general, reducing the ability to self-regulate behaviour (Bergen et al. 2012, 2014). To our knowledge, self-control has not specifically been examined as a risk factor for problem gambling amongst sports bettors. However, impaired self-control is associated with impulsiveness (Baumeister 2002; Sultan et al. 2012), and impulsiveness has been found to be a key risk factor for problem gambling amongst sports bettors (Russell et al. 2018b). Because problematic sports bettors are more likely to place impulsive bets (Hing et al. 2016, 2018b), and to be more impulsive in general (Russell et al. 2018b), impaired self-control is likely to be evident amongst problem sports bettors. Greater self-control may also be reflected in taking more personal responsibility for one’s behaviour and its outcomes (i.e., an internal locus of control), rather than an external locus of control which has previously been linked to gambling pathology (Shumlich et al. 2017).
Importantly, some risk factors represent underlying vulnerabilities to gambling-related problems and harm (distal or indirect risk factors, such as trait self-control and demographic characteristics), while other risk factors represent more immediate vulnerabilities (proximal or direct risk factors, such as gambling behaviour, erroneous cognitions and motivations; Williams et al. 2012). Williams et al.’s model describes a path to problem gambling, whereby distal vulnerabilities lead to problem gambling through more proximal risk factors. Recognising the separate roles of distal and proximal risk factors, and modelling them separately, can lead to more useful information than multivariate models that include all factors together.
The present study aimed to determine whether demographic, behavioural and psychological risk factors—that have previously been identified as problem gambling risk factors amongst sports bettors—are risk factors for problems specifically related to sports betting, rather than gambling in general. The dependent variable was a modified version of the PGSI, which specifically asked about sports betting related problems (referred to below as the PGSI-SB). We hypothesised that proximal (rather than distal) risk factors were more likely to be significant risk factors in multivariate models due to their more direct association with gambling-related problems. More specifically, we hypothesised that those at risk of gambling-related problems specifically due to sports betting would be younger males, with lower levels of self control, who were more engaged in sports betting, and gambling in general. They would have higher gambling urges, erroneous cognitions, and higher scores on motivations compared to those at lower risk of sports betting related problems.
Method
Recruitment and Sampling
The study was approved by (anonymised for review) Human Research Ethics Committee. Potential respondents to the online survey were recruited from online research panels and compensated in line with the practices of these panels. Once informed consent was obtained, respondents completed screening questions to determine their eligibility. Inclusion criteria were: being 18 years of age or older, living in Australia, betting on sports at least monthly, and passing attention checks during the survey. Age and gender quotas were applied to ensure a mix of ages and genders in the final sample.
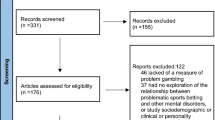
A total of 15,225 respondents started the survey. Of those, 11,587 were excluded because they did not meet the inclusion criterion of betting on sports at least monthly. A further 4 were excluded as they were aged under 18. Two attention check questions were included in the survey (e.g., “Please select ‘almost always’” for a particular question), and 768 respondents were excluded for failing these checks. A further 29 were excluded for speeding through the survey, defined as completing the survey in less than 1/3 of the median time taken during an initial soft launch of the survey. Of the 2837 remaining respondents, 993 were excluded because age and/or gender quotas had been met. From the remaining 1844 respondents, 615 started but did not complete the survey, and 82 were found to be duplicate responses during analysis, leaving a final total of 1147 cases for analysis.
Respondents
The sample of 1147 respondents was mostly male (66.5%), with a mean age of 41.17 years (SD = 14.50). Based on the PGSI-SB, using the original PGSI cutoffs, 394 (34.3%) respondents were classified as non-problem gamblers, 239 (20.8%) as low risk gamblers, 209 (18.2%) as moderate risk gamblers and 306 (26.7%) as problem gamblers. Most were born in Australia (83.5%) and spoke English as their main language at home (95.5%). Respondents came from a range of states, mostly the three most populous (34.2% New South Wales, 27.7% Victoria, 14.8% Queensland). Median personal pre-tax income was $60,000–$69,999 per annum. Around half (48.1%) were married, 15.3% living with partner/de facto, 29.0% single/never married, 6.4% divorced or separated and 1.1% widowed. Most (56.0%) had children.
Measures
Sports Betting Problem Gambling Severity Index (SB-PGSI, Adapted from the Original PGSI by Ferris and Wynne 2001)
To explore problem gambling severity specifically in relation to the respondents’ sports betting, we modified the original PGSI by adding the words “on sports” to each item, and also included images of sports with the text “Please note that these questions refer to your SPORTS BETTING ONLY” at the top of each relevant page of the survey. Reliability for this scale is described in the results.
Distal Risk Factors
Demographic questions consisted of gender (male, female), age (in years), main language spoken at home (English or other), marital status (recoded as single, married/de facto/living with partner, divorced/separated/widowed), whether the respondent has children (no, yes), income and disposable income (both in brackets).
Self control was assessed using the Brief Self Control Scale (BSCS; Tangney et al. 2004). The BSCS contains 13 items focusing on self-discipline, deliberate/non-impulsive action, healthy habits, work ethic, and reliability. Each item is measured on a five point scale from 1 (not at all) to 5 (very much). Nine items are reverse scored and total scores range from 13 to 65 with higher scores indicating higher levels of self-control. Cronbach’s alpha in this sample was 0.86.
Proximal Risk Factors
Gambling behaviour Respondents reported how frequently they bet on sports (from not at all in the last 12 months to 4 or more times a week), as well as their frequency of betting on six other forms of gambling (race betting, casino table games, keno, lottery-type games including instant scratch tickets, electronic gaming machines and bingo), which was summed to compute how many forms they had engaged in during the last 12 months. Respondents reported their typical monthly sports betting expenditure in the last 12 months, with expenditure defined as “money that you have invested and does not count recycling wins. So if you put $20 on bets during a typical month, then won $50, your answer would be $20, whether or not you reinvested your $50 winnings”. Expenditure was skewed and thus log transformed. Respondents also reported how many bets they placed in a typical day of betting (open-ended question, also skewed and therefore log-transformed).
Respondents also reported the proportion of sports bets they placed in land-based venues, via the Internet and via telephone calls (with responses required to sum to 100%), and the proportion of bets placed on Australian-based competitions (e.g., National Rugby League or Australian Football League), overseas-based competitions (e.g., the National Basketball Association or the English Premier League), or on international competitions (e.g., sports with competitions around the world like tennis or golf, or sports involving international teams such as cricket test matches). Responses were also required to sum to 100%.
Respondents were asked to report which payment methods they had used for sports betting in the last 12 months: credit card, debit card, PayPal, deposit into a bank account via a bank branch, deposit into a bank account online or via the telephone, BPay, payment of cash in land-based gambling venue (e.g., TAB), or other (please specify). Few respondents selected “other” and this was excluded from analysis. A summary variable was also created to reflect how many payment methods (excluding other) respondents used.
Respondents were also asked how old they were when they first bet on sports, and reported in age brackets. This was recoded into those who had first bet while underage (under the age of 18 in Australia) versus those who had first bet while aged 18 or older.
Sports involvement Respondents were asked how frequently they watched the sporting contests on which they had bet (never, sometimes, most of the time, almost always), and the proportion of sports bets they placed on matches involving a team or individual that they support (compared to proportion bet on matches not involving a team or individual they support, with responses required to sum to 100%). Respondents were also asked if they had engaged in sports tipping competitions, or fantasy sports, within the last 12 months (responses: no or yes for both).
Psychological measures Respondents reported their motivations for gambling via the Gambling Outcomes Expectancies Scale (GOES; Flack and Morris 2016), an 18 item measure with response options collected on six point Likert scales, from strongly disagree (1) to strongly agree (6). Total scores were generated for each of five motivations (social, money, excitement, escape, and ego enhancement), and higher scores for each motivation indicate stronger endorsement of that motivation. Cronbach’s alpha for the five domains ranged between 0.85 and 0.92 in this sample.
Gambling urges were assessed using the Gambling Urge Scale (GUS; Raylu and Oei 2004b). The GUS measures thoughts and feelings about gambling urges through 6 items (such as ‘I crave a gamble right now’). Each item is measured on a seven point scale (0 = strongly disagree, 6 = strongly agree) with higher total scores indicating greater urges to gamble. Cronbach’s alpha in this sample was 0.97.
Erroneous cognitions were assessed using the Gambler’s Beliefs Questionnaire (GBQ; Steenbergh et al. 2002). The GBQ measures a gambler’s cognitive distortions using 21 items each measured on a seven point scale from strongly disagree (1) to neutral (4) to strongly agree (7). While this scale consists of two factors (luck/perseverance and illusion of control), these factors were closely related (r = 0.87) and could not both be included in the multivariate models below due to collinearity concerns. Thus we instead treated this scale as unidimensional (Cronbach’s alpha = 0.96). Total scores range from 21 to 147; higher scores indicate higher levels of cognitive distortions.
Respondents were asked to rate how much responsibility various parties have to ensure that the respondent gambles on sports responsibly. The response options were: myself, my family, my friends, the venue/club/hotel/etc., the wagering operator, the government (at any level: local, state and/or federal), and other. Respondents responded by assigning a percentage of the responsibility to each party, with responses required to sum to 100%. Initial analysis of this question found that “myself” was the response with the most endorsement, and only this was included in present analyses.
Alcohol misuse was assessed using the 4 item CAGE (Ewing 1984): Items are scored 0 (no) or 1 (yes) with higher scores indicating alcohol problems. A total score of two or more is considered as clinically significant for alcohol problems.
Data Analysis
We first checked reliability and dimensionality of the customised PGSI-SB, and found them to be virtually identical to the regular PGSI. To determine risk factors, the analyses compared non-problem and low risk gamblers (combined) to moderate risk and problem gamblers (combined), based on the original PGSI cutoffs, and in line with previous risk factor studies (e.g., Russell et al. 2018b). We also considered comparing problem gamblers versus all other groups, but the results were generally similar, and thus we opted to report the former results in line with existing literature. We initially conducted bivariate analyses, treating each variable as an independent variable, and the combined PGSI-SB groups as the dependent variable. All analyses were conducted as binary logistic regressions. Some variables were ordinal in nature, such as education and income. We explored treating these variables as ordinal (i.e., the results would include a separate coefficient and test for each level of education and income) and as continuous (i.e., one coefficient for each variable). Both approaches found similar results, and thus we report the continuous versions for easier interpretation and more parsimonious output.
Significant variables in the bivariate models were then considered for inclusion in multivariate models. Initial analyses indicated high levels of correlation between some variables, notably gambling motivations, gambling urges, and erroneous gambling cognitions. We opted to include gambling urges, and exclude motivations and erroneous cognitions due to collinearity concerns. Disposable income and income were also correlated, and thus disposable income was removed from the model. Where two versions of a variable were available (e.g., age of first gamble on EGMs, and gambling underage, or CAGE as raw scores and a grouping variable), only the latter of each was included.
Because of the collinearity concerns in the multivariate model, we also explored a more parsimonious model that allows for collinearity amongst predictors. We used the elastic net procedure, which reduces the number of predictors in the model (lasso approach) and penalises them for collinearity (ridge approach). The result is a model that includes the most important predictors of gambling-related risk severity, whether or not collinearity is present amongst them. All variables were considered for inclusion, whether significant in the bivariate models or not, because they may have been important predictors (and thus significant) when controlling for other variables in the model, with the exception of age of first gamble and CAGE scores, because gambling underage and the CAGE grouping variable were used instead.
Both sets of multivariate results (multivariate and penalised models) found that only proximal risk factors were significant (e.g., gambling urges and erroneous beliefs), and that no distal risk factors (demographics) were significant predictors when controlling for other variables, with the exception of self control. We thus also modelled proximal and distal variables separately in multivariate regressions. In the Williams et al. (2012) model, comorbid addictive behaviours are not a part of the paths leading to problem gambling, but instead are at the same level as problem gambling. Thus, while alcohol misuse does not appear to be a distal factor, it is unclear if it can be treated as a proximal risk factor. As such, alcohol misuse was not included in the distal or proximal models.
Results
Dimensionality and Reliability of PGSI-SB
The PGSI-SB in this sample displayed a high reliability (Cronbach’s alpha = 0.96) and removal of any item within the scale did not increase reliability, which is in line with the original PGSI. Exploratory factor analysis clearly indicated a single factor solution, accounting for 73.51% of variance, and any subsequent factors displayed eigenvalues below 0.5. As such, the PGSI-SB displays similar psychometric properties to the regular PGSI.
Bivariate Results
Bivariate risk factors are reported in Table 1.
Demographic Risk Factors
Demographic risk factors for being classified as a moderate risk or problem sports bettor were: being younger, speaking a language other than English at home, being single (vs married/de facto/living with partner or divorced/separated/widowed), having a higher income and having a higher disposable income. Gender and having children were not significant risk factors, although we note that the bivariate p value for gender was 0.053, and thus suggest that this result is not strong evidence against gender as a risk factor for sports betting related problems.
Behavioural Risk Factors
Risk factors related to gambling behaviour were: betting on sports more frequently, betting on a higher number of other gambling forms, betting on a higher number of different sports, higher monthly sports betting expenditure, placing more bets on a typical betting day, placing a lower proportion of bets via the Internet and higher proportion via telephone, placing a lower proportion of bets on Australian-based competitions and a higher proportion on either overseas-based and/or international-based competitions, paying via most payment methods (apart from deposits online and cash) and using a higher number of different payment methods, watching the contest on which one is betting less frequently, not engaging in fantasy sports contests, and first betting on sports while underage.
Non-significant risk factors were: proportion of bets placed in land-based venues, percentage of bets placed on their favourite team and partaking in sports tipping competitions.
Psychological Risk Factors
Respondents classified as moderate risk or problem sports bettors were more likely to be motivated by each of the motivations (excitement, escape, ego, money and social), to have higher gambling urges, and to have higher erroneous cognitions in relation to their sports betting, compared to those classified as non-problem or low risk gamblers. Similarly, higher risk sports bettors rated their responsibility for their own gambling as significantly lower compared to non-problem and low risk sports bettors, and were also more likely to have alcohol issues, and lower self control.
Multivariate Model
Many variables that were significant in the bivariate models were no longer significant in the multivariate model when controlling for other variables (Table 1).
Significant risk factors for being a moderate risk or problem sports bettor according to the multivariate model were having: higher monthly sports betting expenditure, higher gambling urges, alcohol issues, and lower self control.
Penalised Model
The penalised model (Table 1) identified the following variables as the most important predictors of being classified as a moderate risk or problem sports bettor: being motivated by money, higher gambling urges, higher erroneous cognitions, alcohol issues, and lower self control.
Proximal Versus Distal
When considering only proximal risk factors, the results were similar to the overall multivariate model (Table 1). Those at higher risk had higher monthly sports betting expenditure and higher gambling urges. Results that were now significant in the proximal only analysis, aligning with the bivariate results but not the full model multivariate results, were betting less on Australian-based competitions, and using a higher number of different payment methods.
Distal factors, apart from self control, were non-significant in the multivariate model, probably because they were mediated by the proximal factors. Multiple mediation analyses were unclear, particularly with this number of distal and proximal factors, and thus we report the distal factors only. Those at higher risk of sports betting-related problems were younger, spoke a language other than English as their main language, and had lower self control.
Discussion
This study is the first to our knowledge to examine risk factors for gambling problems specifically related to sports betting, rather than gambling in general. The results generally align with other studies that have examined risk factors amongst sports bettors using more general problem gambling screens, confirming that sports betting itself—rather than co-occurring gambling on other forms—contributes to gambling problems and harms. The study is also novel in that it is the first to consider, separately, distal and proximal risk factors, and includes a penalised model that allows for collinearity amongst predictors.
In support of our first hypothesis, in general, the distal factors (with the exception of self-control) were not significant when proximal factors were present (multivariate model), or were not selected for inclusion in the penalised model. This suggests a potential causal chain, similar to that proposed by Williams et al. (2012). Their model proposed that biological (e.g. self-control) and environmental (e.g. demographic) risk factors feed into problem gambling via erroneous cognitions, gambling motivations (e.g. serving a psychological need), and early gambling experiences with subsequent conditioning (e.g. gambling uptake and behaviour). In the present research, due to the number of variables involved, the exact mediation paths were unclear. However, it can be concluded that distal effects that were not significant when proximal effects were included, such as age and disposable income, are mediated by one or more proximal variables.
Distal risk factors can nevertheless inform the targeting of interventions aimed at reducing problematic sports betting. Our separate analysis of distal risk factors indicates that these should be designed appropriately for sports bettors of younger age, those who speak a language other than English at home, and males. While gender was not a statistically significant risk factor in bivariate analyses, the p value was 0.053, and in the direction of males, so this does not constitute strong evidence against males being most at risk for sports betting problems, as identified in previous research (Hing et al. 2016, 2017a; Hunt 2017; Russell et al. 2018b). However, a few studies have noted increasing uptake of sports betting by women and called for more research into women experiencing sport betting problems (Hing et al. 2018b; McCormack et al. 2014).
As hypothesised, those in the moderate-risk and problem gambler groups were more engaged gamblers, both in terms of their sports betting (more frequent sports betting, betting on more sports, having higher expenditure, placing more bets per day, using more payment methods), and in terms of the number of other forms on which they gambled. Some risk factors relating to the proportion of bets placed via different channels (less via the internet, more via telephone) and some payment methods used may be unique to Australia due to restrictions on in-play sports betting, which cannot legally be offered online, but only by telephone or in land-based venues. In-play betting (Hing et al. 2016, 2018b; Lopez-Gonzalez et al. 2018b), including betting on micro-events (Russell et al. 2018a) has been linked to gambling problems in general, and the present study shows a link specifically to sports betting-related problems. However, they were not necessarily more involved sports watchers. In bivariate results, watching the sporting contest on which one was betting occurred less frequently amongst those experiencing sports betting-related problems. This finding may be because higher risk bettors could bet on simultaneous matches, and cannot watch all of them. A more likely explanation is that, for those in higher risk groups, betting on sports itself is no longer related to enhancing the spectacle of watching sport, but instead said betting has become the main form of entertainment. As such, betting only on events one is interested in watching presents a potential guide for limiting sports betting-related problems.
However, sports betting behaviours did not emerge as important factors in the penalised model. Instead, and in line with our hypotheses, the risk factors that emerged from the penalised model were the motivation of making money (in line with Fang and Mowen 2013) erroneous cognitions (Blaszczynski and Nower 2002; Lindberg et al. 2014; Michalczuk et al. 2011), higher gambling-related urges (Raylu and Oei 2004b), alcohol problems (Baldo et al. 2006; Cowlishaw 2014; Grant et al. 2002; Hing et al. 2017a; Lorains et al. 2011; Russell et al. 2018c; Sundqvist et al. 2015), and lower levels of self-control (Bergen et al. 2014; Blaszczynski and Nower 2002; Dickerson and O’Connor 2006). This model is particularly important, because motivations, urges, erroneous cognitions and alcohol problems could not be included together in the multivariate model due to multicollinearity, but emerged as separate, unique risk factors in the penalised model. This model suggests that it is one’s psychological relationship with gambling, rather than just the gambling behaviour itself, that is a primary driver of gambling-related problems, in line with Williams et al. (2012).
Gambling urges, erroneous cognitions and motivations may change over time, and can thus be addressed in treatment, such as cognitive-behavioural and exposure therapy that seeks to correct cognitive distortions and erroneous beliefs, and to develop urge-management strategies. However, lower self-control amongst gamblers may not necessarily be as easy to treat as it reflects lower trait self-control in general (Bergen et al. 2012, 2014). Lower self-control was a significant risk factor in all models, and was the only distal factor that emerged in the penalised model. Lower self-control can also be reflected in impulsive betting (Hing et al. 2016, 2018b) and higher impulsiveness in general (Russell et al. 2018b) which have both been linked to problem gambling. Because self-control is relatively stable, and an underlying vulnerability amongst at-risk gamblers, impulsive forms of betting are likely to be particularly problematic for these gamblers. As such, appropriate protections or restrictions must be considered for betting products (e.g. micro-betting) and betting promotions (e.g. wagering inducements) that encourage an impulsive response.
The present study has some limitations. Like all surveys, it relied on self-report. A modified version of the PGSI was used (the PGSI-SB), which has not been validated, but which has similar psychometric properties to the regular PGSI. The study was conducted on members of a research panel, who may not be representative of the Australian population of at-least monthly sports bettors. However, the present study also has some strengths. It is the first to specifically assess risk factors for problems specifically related to sports betting, using approaches that enabled distal and proximal factors to be modelled.
Taken together, the results indicate that those who experience problems specifically related to sports betting are younger people with some disposable income, who are more engaged sports bettors (and gamblers in general), who gamble for a variety of motivations but particularly for money, have higher gambling urges and more erroneous cognitions, who experience alcohol issues, and have lower self-control. As sports betting is legalised in more jurisdictions, and as more sports betting products become available, understanding who is most at risk from this form of gambling is important, in order to inform regulation as well as harm reduction and treatment measures.
References
Armstrong, A., & Carroll, M. (2017). Sports betting in Australia. Melbourne: Australian Gambling Research Centre. Retrieved January 7, 2019 from https://aifs.gov.au/agrc/publications/sports-betting-australia.
Baldo, V., Cristofoletti, M., Majori, S., Cibin, M., Peron, C., Dal Zotto, A., et al. (2006). Relationship between pathological gambling, alcoholism and drug addiction. Annali di Igiene: Medicina Preventiva e di Comunita, 18(2), 147–153.
Baumeister, R. F. (2002). Yielding to temptation: Self-control failure, impulsive purchasing, and consumer behavior. The Journal of Consumer Research, 28(4), 670–676.
Bergen, A. E., Newby-Clark, I. R., & Brown, A. (2012). Low trait self-control in problem gamblers: Evidence from self-report and behavioral measures. Journal of Gambling Studies, 28(4), 637–648.
Bergen, A. E., Newby-Clark, I. R., & Brown, A. (2014). Gambling increases self-control strength in problem gamblers. Journal of Gambling Studies, 30(1), 153–162.
Blaszczynski, A., & Nower, L. (2002). A pathways model of problem and pathological gambling. Addiction, 97(5), 487–499.
Braverman, J., & Shaffer, H. J. (2012). How do gamblers start gambling: Identifying behavioural markers for high-risk internet gambling. European Journal of Public Health, 22(2), 273–278.
Cantinotti, M., Ladouceur, R., & Jacques, C. (2004). Sports betting: Can gamblers beat randomness? Psychology of Addictive Behaviors, 18(2), 143–147.
Cowlishaw, S. (2014). Comorbid problem gambling in substance users seeking treatment. Melbourne: Victorian Responsible Gambling Foundation. Retrieved January 7, 2019 from https://responsiblegambling.vic.gov.au/documents/79/Research-report-comorbid-problem-gambling-in-substance-users-seeking-treatment.pdf.
Delfabbro, P. H. (2012). Australasian gambling review—5th Edition—Independent Gambling. Adelaide: Independent Gambling Authority. Retrieved January 7, 2019 from http://iga.sa.gov.au/sites/default/files/publication-documents/Australian%20Gambling%20Review-5th%20Edition.pdf.
Dickerson, M., & O’Connor, J. (2006). Gambling as an addictive behaviour: Impaired control, harm minimisation, treatment and prevention. Cambridge: Cambridge University Press.
Ewing, J. A. (1984). Detecting alcoholism. The CAGE questionnaire. JAMA: The Journal of the American Medical Association, 252(14), 1905–1907.
Fang, X., & Mowen, J. C. (2013). Examining the trait and functional motive antecedents of four gambling activities: Slot machines, skilled card games, sports betting, and promotional games. Journal of Consumer Marketing. https://doi.org/10.1108/07363760910940483.
Ferris, J. A., & Wynne, H. J. (2001). The Canadian problem gambling index: Final report. Ottawa: Canadian Centre on Substance Abuse.
Financial Counselling Australia. (2015). Duds, mugs and the A-List: The impact of uncontrolled sports betting. Melbourne. Retrieved January 7, 2019 from https://www.financialcounsellingaustralia.org.au/getattachment/Corporate/Home/FINAL-PDF-Duds,-Mugs-and-the-A-List-The-Impact-of-Uncontrolled-Sports-Betting-low-res.pdf.
Flack, M., & Morris, M. (2015). Problem gambling: One for the money…? Journal of Gambling Studies, 31(4), 1561–1578.
Flack, M., & Morris, M. (2016). The temporal stability and predictive ability of the Gambling Outcome Expectancies Scale (GOES): A prospective study. Journal of Gambling Studies, 32(3), 923–933.
Gainsbury, S. M., Russell, A., Blaszczynski, A., & Hing, N. (2015a). Greater involvement and diversity of Internet gambling as a risk factor for problem gambling. European Journal of Public Health, 25(4), 723.
Gainsbury, S. M., Russell, A., Hing, N., Wood, R., & Blaszczynski, A. (2013). The impact of internet gambling on gambling problems: A comparison of moderate-risk and problem Internet and non-Internet gamblers. Psychology of Addictive Behaviors, 27(4), 1092–1101.
Gainsbury, S. M., Russell, A., Wood, R., Hing, N., & Blaszczynski, A. (2015b). How risky is Internet gambling? A comparison of subgroups of Internet gamblers based on problem gambling status. New Media and Society, 17(6), 861–879.
Gordon, R., Gurrieri, L., & Chapman, M. (2015). Broadening an understanding of problem gambling: The lifestyle consumption community of sports betting. Journal of Business Research, 68(10), 2164–2172.
Grant, J. E., Kushner, M. D., & Kim, S. W. (2002). Pathological gambling and alcohol use disorder. https://pubs.niaaa.nih.gov/publications/arh26-2/143-150.htm. Accessed November 14, 2018.
Hing, N., Gainsbury, S. M., Blaszczynski, A., Wood, R., Lubman, D., & Russell, A. M. T. (2014). Interactive gambling. Melbourne: Gambling Research Australia.
Hing, N., Lamont, M., Vitartas, P., & Fink, E. (2015). Sports bettors’ responses to sports-embedded gambling promotions: Implications for compulsive consumption. Journal of Business Research, 68(10), 2057–2066.
Hing, N., Li, E., Vitartas, P., & Russell, A. M. T. (2018a). On the spur of the moment: Intrinsic predictors of impulse sports betting. Journal of Gambling Studies, 34(2), 413–428.
Hing, N., Russell, A. M., & Browne, M. (2017a). Risk factors for gambling problems on online electronic gaming machines, race betting and sports betting. Frontiers in Psychology, 8, 779.
Hing, N., Russell, A. M. T., Lamont, A. M. T., & Vitartas, P. (2017b). Bet anywhere, anytime: An analysis of Internet sports bettors’ responses to gambling promotions during sports broadcasts by problem gambling severity. Journal of Gambling Studies. https://doi.org/10.1007/s10899-017-9671-9.
Hing, N., Russell, A. M. T., Li, E., & Vitartas, P. (2018b). Does the uptake of wagering inducements predict impulse betting on sport? Journal of Behavioral Addictions, 7(1), 146–157.
Hing, N., Russell, A. M. T., Rockloff, M. J., Browne, M., Langham, E., Li, E., et al. (2018c). Effects of wagering marketing on vulnerable adults. Melbourne: Victorian Responsible Gambling Foundation.
Hing, N., Russell, A. M. T., Vitartas, P., & Lamont, M. (2016). Demographic, behavioural and normative risk factors for gambling problems amongst sports bettors. Journal of Gambling Studies, 32(2), 625–641.
Hunt, C. J. (2017). Wide-ranging ban on gambling ads during sport broadcasts is needed to tackle problem gambling. The conversation. Retrieved January 7, 2019 from http://theconversation.com/wide-ranging-ban-on-gambling-ads-during-sport-broadcasts-is-needed-to-tackle-problem-gambling-74687.
Jenkinson, R., de Lacey-Vawdon, C., & Carroll, M. (2018). Weighing up the odds: Young men, sports and betting. Melbourne: Victorian Responsible Gambling Foundation.
Johansson, A., Grant, J. E., Kim, S. W., Odlaug, B. L., & Götestam, K. G. (2009). Risk factors for problematic gambling: A critical literature review. Journal of Gambling Studies, 25(1), 67–92.
LaBrie, R. A., & Shaffer, H. J. (2011). Identifying behavioral markers of disordered Internet sports gambling. Addiction Research and Theory, 19(1), 56–65.
Lamont, M., & Hing, N. (2018). Sports betting motivations among young men: An adaptive theory analysis. Leisure Sciences. https://doi.org/10.1080/01490400.2018.1483852.
Lamont, M., Hing, N., & Vitartas, P. (2016). Affective response to gambling promotions during televised sport: A qualitative analysis. Sport Management Review, 19(3), 319–331.
LaPlante, D. A., Nelson, S. E., & Gray, H. M. (2014). Breadth and depth involvement: Understanding Internet gambling involvement and its relationship to gambling problems. Psychology of Addictive Behaviors, 28(2), 396–403.
Lindberg, A., Clark, L., & Bowden-Jones, H. (2014). Impulsivity and cognitive distortions in problem gambling: Theory and application. In F. Gobet & M. Schiller (Eds.), Problem gambling: Cognition, prevention and treatment (pp. 252–286). London: Palgrave Macmillan UK.
Lopez-Gonzalez, H., Estévez, A., & Griffiths, M. D. (2017). Marketing and advertising online sports betting: A problem gambling perspective. Journal of Sport and Social Issues, 41(3), 256–272.
Lopez-Gonzalez, H., Estévez, A., & Griffiths, M. D. (2018a). Controlling the illusion of control: A grounded theory of sports betting advertising in the UK. International Gambling Studies, 18(1), 39–55.
Lopez-Gonzalez, H., Guerrero-Solé, F., & Griffiths, M. D. (2018b). A content analysis of how “normal” sports betting behaviour is represented in gambling advertising. Addiction Research and Theory, 26(3), 238–247.
Lorains, F. K., Cowlishaw, S., & Thomas, S. A. (2011). Prevalence of comorbid disorders in problem and pathological gambling: Systematic review and meta-analysis of population surveys. Addiction, 106(3), 490–498.
MacKay, T.-L., & Hodgins, D. C. (2012). Cognitive distortions as a problem gambling risk factor in Internet gambling. International Gambling Studies, 12(2), 163–175.
McCormack, A., Shorter, G. W., & Griffiths, M. D. (2014). An empirical study of gender differences in online gambling. Journal of Gambling Studies, 30(1), 71–88.
Michalczuk, R., Bowden-Jones, H., Verdejo-Garcia, A., & Clark, L. (2011). Impulsivity and cognitive distortions in pathological gamblers attending the UK National Problem Gambling Clinic: A preliminary report. Psychological Medicine, 41(12), 2625–2635.
Pitt, H., Thomas, S. L., Bestman, A., Daube, M., & Derevensky, J. (2017). What do children observe and learn from televised sports betting advertisements? A qualitative study among Australian children. Australian and New Zealand Journal of Public Health, 41(6), 604–610.
Raylu, N., & Oei, T. P. S. (2004a). The Gambling Related Cognitions Scale (GRCS): Development, confirmatory factor validation and psychometric properties. Addiction, 99(6), 757–769.
Raylu, N., & Oei, T. P. S. (2004b). The gambling urge scale: Development, confirmatory factor validation, and psychometric properties. Psychology of Addictive Behaviors, 18(2), 100–105.
Raymen, T., & Smith, O. (2017). Lifestyle gambling, indebtedness and anxiety: A deviant leisure perspective. Journal of Consumer Culture. https://doi.org/10.1177/1469540517736559.
Russell, A. M. T., Hing, N., Browne, M., Li, E., & Vitartas, P. (2018a). Who bets on micro events (microbets) in sports? Journal of Gambling Studies. https://doi.org/10.1007/s10899-018-9810-y.
Russell, A. M. T., Hing, N., Li, E., & Vitartas, P. (2018b). Gambling risk groups are not all the same: Risk factors amongst sports bettors. Journal of Gambling Studies. https://doi.org/10.1007/s10899-018-9765-z.
Russell, A. M. T., Langham, E., Hing, N., & Rawat, V. (2018c). Social influences on gamblers by risk group: An egocentric social network analysis. Melbourne: Victorian Responsible Gambling Foundation.
Shumlich, E. J., Perez, S., & Hoaken, P. N. S. (2017). The influence of locus of control and sensation seeking among undergraduate Texas Hold’em players. Journal of Gambling Issues. https://doi.org/10.4309/jgi.v0i37.3990.
Smith, D. P., Battersby, M. W., Pols, R. G., Harvey, P. W., Oakes, J. E., & Baigent, M. F. (2015). Predictors of relapse in problem gambling: A prospective cohort study. Journal of Gambling Studies, 31(1), 299–313.
Smith, D. P., Pols, R. G., Battersby, M. W., & Harvey, P. W. (2013). The Gambling Urge Scale: Reliability and validity in a clinical population. Addiction Research and Theory, 21(2), 113–122.
Sproston, K., Hanley, C., Brook, K., Hing, N., & Gainsbury, S. M. (2015). Marketing of sports betting and racing. Melbourne: Gambling Research Australia.
Steenbergh, T. A., Meyers, A. W., May, R. K., & Whelan, J. P. (2002). Development and validation of the Gamblers’ Beliefs Questionnaire. Psychology of Addictive Behaviors, 16(2), 143–149.
Sultan, A. J., Joireman, J., & Sprott, D. E. (2012). Building consumer self-control: The effect of self-control exercises on impulse buying urges. Marketing Letters, 23(1), 61–72.
Sundqvist, K., Rosendahl, I., & Wennberg, P. (2015). The association between at-risk gambling and binge drinking in the general Swedish population. Addictive Behaviors Reports, 2, 49–54.
Tangney, J. P., Baumeister, R. F., & Boone, A. L. (2004). High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. Journal of Personality, 72(2), 271–324.
Wardle, H., Moody, A., Griffiths, M., Orford, J., & Volberg, R. (2011). Defining the online gambler and patterns of behaviour integration: Evidence from the British Gambling Prevalence Survey 2010. International Gambling Studies, 11(3), 339–356.
Williams, R., West, B., & Simpson, R. (2012). Prevention of problem gambling: A comprehensive review of the evidence and identified best practices. Retrieved January 7, 2019 from https://www.uleth.ca/dspace/bitstream/handle/10133/3121/2012-PREVENTION-OPGRC.pdf.
Acknowledgements
This study was funded by internal funding from the Centre for Gambling Education and Research at Southern Cross University (Grant No. NA). The first author was a member of this Centre at the time that the data were collected.
Funding
Alex Russell has received funding from Victorian Responsible Gambling Foundation; Queensland Justice and Attorney-General; Gambling Research Australia; National Association for Gambling Studies; Australian Communications and Media Authority and the Alberta Gambling Research Institute. He has received industry funding for an evaluation of problem gambling amongst casino employees from Echo/Star Entertainment Group. He is also affiliated with the University of Sydney. Nerilee Hing has received research funds from the Victorian Responsible Gambling Foundation, Gambling Research Australia, Australian Government Department of Social Services, Alberta Gambling Research Institute, the Australian Gambling Research Centre, the Queensland, New South Wales, Victorian and South Australian Governments, the Australian Research Council, and Australia’s National Research Organisation for Women’s Safety. She has also received consultancy funds from Echo Entertainment and Sportsbet and an honorarium from Singapore Pools for membership of its International Advisory Committee. Matthew Browne has received research funds from the Victorian Responsible Gambling Foundation, Queensland Government Department of Health, Australian Department of Social Services, New Zealand Ministry of Health, Department of Families, Housing, Community Services and Indigenous Affairs, Department of Innovation, Industry, Science and Research, Australian Department of Foreign Affairs and Trade, Japanese Ministry of Economy, Trade and Industry.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Russell, A.M.T., Hing, N. & Browne, M. Risk Factors for Gambling Problems Specifically Associated with Sports Betting. J Gambl Stud 35, 1211–1228 (2019). https://doi.org/10.1007/s10899-019-09848-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-019-09848-x