
Abstract
Studies point to a relationship between fantasy sports/daily fantasy sports (DFS) play and gambling behavior. However, little is known about the nature of those relationships, particularly regarding the development of gambling problems. This study investigates the nature, frequency, and preferences of gambling behavior as well as problem gambling severity and comorbid conditions among DFS players. Data were collected from an epidemiologic survey of 3634 New Jersey residents on gambling and leisure activities. Participants were contacted by phone (land-line and cell) and online to obtain a representative, cross-sectional sample of non-institutionalized adults, aged 18 years or older. Excluding non-gamblers, the remaining 2146 participants, included in these analyses, indicated they had either played DFS (n = 299) or had gambled but not played DFS (1847) in the past year. Univariate comparisons and multiple logistic regression analyses were performed to identify the most significant characteristics and predictors of DFS players. Overall, a higher number of gambling activities, high frequency gambling, male gender, and reports of suicidal thoughts in the past year were most predictive of DFS players. Being Hispanic (vs. Caucasian) and/or single (vs. married or living with a partner) also doubled the odds of DFS play. Findings suggest that DFS players are characterized by high gambling frequency and problem severity and comorbid problems, notably suicidal ideation. Future research should examine the motivations and possible etiological sub-types of DFS players and the nature and course of DFS play, particularly in relation to gambling behavior and the development of gambling and other problems.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Advances in technology, including high speed Internet, access to real-time sports data, and sophisticated analytic methods, have spurred the growth and popularity of fantasy sports (FS) leagues over the last decade. FS are an online ancillary to traditional sports media, which allow fans to assume the role of team manager/owner by assembling a virtual line-up of real-world athletes from professional and non-professional sports competitions. The primary aim of FS leagues is to accrue the most FS points, which are computed from actual in-game performance statistics of athletes according to a predefined FS scoring system.
Recent figures from the Fantasy Sports Trade Association (FSTA 2016) estimated that 57.4 million people participated in FS in the U.S. and Canada, representing approximately 16% of the populations of both countries combined (US Census Bureau 2016). In the same report, it was noted that the percentage of players who participated in some form of daily fantasy sports (DFS) increased from 31 to 64% between 2012 and 2015 (FSTA 2016).
In contrast to traditional FS leagues, which are generally played over an entire season, DFS is dynamic, conducted over a single game or round of competition. DFS players are also required to pay entry fees that can range from 25c to $5000, depending on the league (DraftKings 2016). In 2015, the leading U.S. companies, FanDuel and DraftKings, reported collecting a combined $3 billion in entry fees, representing an increase of 300% from 2014 (Van Natta 2016). Enacted before the advent of DFS, the Unlawful Internet Gambling Enforcement Act (UIGEA 2006) in the U.S. specifically exempted FS as a skill-based enterprise that was not considered gambling. Accordingly, some U.S. states have extended that exemption to DFS (e.g., Colorado, Massachusetts, New York, and Virginia) while other states have not (e.g., Iowa, Nevada, Montana, and Washington) (Rodenberg 2016). The key policy distinction, however, is not whether DFS is gambling but whether the nature of harm associated with participation requires regulation (Pickering et al. 2016).
Despite high levels of participation in both FS and DFS, there is a lack of empirical studies, examining the characteristics of players and the potential risks and harms associated with excessive involvement. Comparisons between demographic characteristics of fee-paying versus non fee-paying users (Drayer et al. 2013) and traditional FS versus hybrid traditional/DFS users (Billings et al. 2016) reveal no discernible group differences. Players are predominantly men (66–97%), in their mid-30s, Caucasian (87–89%), and slightly more than half are in relationships (51–56%); they are well-educated (66% hold a college degree or greater) and employed fulltime (67%) in well-payed (51%: household income 75 k+) white-collar professions (Drayer et al. 2013; FSTA 2016; Mills et al. 2014; Ruihley and Hardin 2011).
To date, only a few studies have investigated the relationship between FS participation and gambling problems. Martin and Nelson (2014) surveyed 1556 college students and found that those who participated in FS competitions were five times more likely than non-participants to endorse at least one DSM-5 (American Psychiatric Association 2013) criterion for a gambling disorder. Moreover, those paying entry fees to participate in FS were significantly more likely to experience gambling problems than those who played for money. The authors also reported significant gender differences in that men were the main drivers of fee-paying FS participation; as such, men were more likely than women to experience gambling-related problems. Similarly, a later study reported that participation in FS strongly correlated with gambling in the past year (on any form) and experiencing gambling problems (Martin et al. 2015). Male student athletes in the study were the most likely to participate in FS and reported higher rates of gambling than other groups, suggesting that this subgroup may be particularly at-risk of developing problem gambling.
Marchica and Derevensky (2015) provided some clarification of those results in their analyses of 61,660 student-athletes of the National Collegiate Athletic Association (NCAA) in 2004, 2008, and 2012. While 64.6% of male and 42.3% of female student-athletes reported past-year gambling, only a small portion (male = 1.9%; female = 0.1%) were classified as “at-risk” or “pathological” gamblers under the DSM-IV-TR (American Psychiatric Association 2000) criteria. However, among FS players, only 18.4% of men and 1.8% of women were non-problem gamblers; in contrast, 48.1% of male FS players and 25% of female FS players were in the at-risk/pathological category.
Taken together, these studies suggest that there is a significant relationship between both FS participation and gambling behavior and FS participation and gambling problems; however, the nature of these linkages is not well understood. The existing studies also do not clarify which gambling activities are preferred by FS players with the highest levels of pathology. Additionally, the findings from these studies are based on college populations, particularly athletes, which severely limits their generalizability. More research is needed to examine these relationships in general populations of gamblers and fantasy sports participants. It is also important to note that given strong associations between problem gambling and comorbidities such as substance addiction and mental health issue (see Lorains et al. 2011 for a review), and the link between problem gambling and DFS participation, it is reasonable to explore the question of whether DFS participation is also related to such comorbid problems.
Study Aims
The purpose of this study was to examine differences in the characteristics and behaviors of regular gamblers participating in DFS compared to non-DFS participating gamblers. Such comparative data is important in determining the relationship between DFS, gambling and harm.
Method
Participants
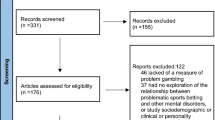
This descriptive study utilized data from a recent state-wide prevalence study of 3634 New Jersey residents. Of those, 1488 residents indicated they neither gambled nor played DFS, so they were excluded from these analyses. The remaining 2146 participants, included in these analyses, indicated they had either played DFS (n = 299) or had gambled but not played DFS (1847) in the past year.
Nearly all DFS participants (97.7%; n = 292) also gambled; only seven respondents, all male, indicated they played only DFS and did not otherwise gamble. There were no statistically significant differences between DFS players who did and did not gamble with respect to the variables tested. All females who played daily fantasy sports also gambled on other activities. Demographic data on the two groups is provided in Table 1. Data coding analyses were conducted using SPSS version 24.
Measures
The present study used data collected through an epidemiological survey, adapted from a survey utilized in multiple jurisdictions. Sections of the survey elicited data on the following variables: (1) demographics (gender, age, race/ethnicity, education level, household income, immigration status, and relationship status); (2) substance use (tobacco use, alcohol use, illegal drug use, problems and treatment seeking with substances, behavioral addictions, and binge drinking); (3) mental health and physical health (overall stress level, overall level of happiness, overall health, experiences of mental health problems in the past 30 days and 12 months, suicidal ideation, and suicidal attempts in the past year); (4) gambling activities participated in the past year (lottery, bingo, scratch offs, sports betting, horse race track betting, poker, casino table games, other games of skill, and gaming machines); (5) non-gambling activities participated in the past year (high risk stocks and daily fantasy sports); (6) gambling behavior (frequency of participation, amount of money spent, venue preference for gambling, and online gambling participation across all previously mentioned forms).
The Problem Gambling Severity Index (PGSI) of the Canadian Problem Gambling Index (CPGI, Ferris and Wynne 2001): This 9-item instrument was used to assess gambling status. Respondents indicate the extent to which an item applies to them using a four-point Likert scale ranging from 0 (never) to 3 (almost always). Scores are totalled in accordance with Ferris and Wynne’s (2001) guidelines: 0 indicates no risk; 1–2 low risk; 3–7 moderate risks; and 8–27 problem gambling, respectively. Ferris and Wynne (2001) reported satisfactory scale reliability (α = 0.84).
Procedure
The data was collected both by telephone (cell and landline phones) and Internet to address limitations inherent in either methodology alone. Stratified sampling was used in both sub-samples to ensure demographic characteristics of age, gender, and race/ethnicity were reflective of the New Jersey population.
Results
Univariate Analyses
Univariate comparisons between DFS players and non-DFS gamblers were performed for gender, age, race/ethnicity, education level, relationship status, household income, employment status, substance use and problems, mental health issues, suicidal ideation and attempts, problem behaviors, participation in different gambling activities, frequency of gambling participation, number of gambling activities participated in, preferred gambling venue(s), and PGSI score.
Compared to non-DFS gamblers, DFS players were significantly more likely to be male (χ2 = 121.52, df = 1, p = .000), Hispanic or Asian (χ2 = 70.74, df = 3, p = .000), younger (Mean = 35 vs. 47 years; F = 148.44, df = 1, p = .000) and employed for wages (χ2 = 52.53, df = 7, p = .000). Notably, although a majority of DFS players, like other gamblers, were married, a significantly higher proportion of DFS versus non-DFS gamblers were single (χ2 = 12.39, df = 2, p = .002). Level of education and household income were non-significant.
There were, similarly, a number of statistically significant differences between DFS players and non-DFS gamblers regarding substance use behaviors and mental health issues. DFS players were more likely than the non-DFS gamblers to use tobacco (χ2 = 91.87, df = 1, p = .000), consume alcohol (χ2 = 6.37, df = 1, p = .012) and binge drink (χ2 = 56.81, df = 1, p = .000), use illegal drugs (χ2 = 127.64, df = 1, p = .000), and report past-year problems with drugs or alcohol (χ2 = 181.731, df = 1, p = .000), behavioral addictions such as pornography and shopping (χ2 = 86.65, df = 1, p = .000), and mental health problems in the past 30 days (χ2 = 34.11, df = 1, p = .000). They were also significantly more likely to endorse contemplating suicide (χ2 = 94.16, df = 1, p = .000) and/or attempting suicide in the past 12 months (χ2 = 116.66, df = 1, p = .000). There were no significant differences between the groups regarding past-year mental health issues or help seeking for substance abuse.
The final set of analyses focused on between-group differences in gambling behavior. These analyses excluded the seven DFS players who did not report gambling. Overall, DFS players were significantly more likely than non-DFS gamblers to participate in the following forms of gambling: Lottery (χ2 = 22.14, df = 1, p = .000); scratch off tickets (χ2 = 55.37, df = 1, p = .000); bingo (χ2 = 216.43, df = 1, p = .000); sports betting (χ2 = 623.76, df = 1, p = .000); horse race track betting (χ2 = 319.54, df = 1, p = .000); live poker (χ2 = 420.41, df = 1, p = .000); casino table games (χ2 = 253.64, df = 1, p = .000); other games of skill (χ2 = 316.07, df = 1, p = .000); gaming machines (χ2 = 104.20, df = 1, p = .000).
In addition, the average DFS player endorsed playing nearly seven gambling activities (M = 6.93, SD = 3.22; F = 1.678.32, df = 1, p = .000), compared to non-DFS gamblers who played slightly more than two (M = 2.39, SD = 1.41). Similarly, DFS players were significantly more likely than non-DFS gamblers to be moderate risk or problem gamblers (χ2 = 494.75, df = 3, p = .000), in contrast to non-DFS gamblers who were more likely to be non-problem gamblers.
Similar findings were reported with regard to gambling frequency. A majority of DFS players were high frequency gamblers, gambling once a week or more; only 10 were low frequency gamblers, gambling less than once per month. DFS players primarily gambled both on line and in land-based venues (62.5%), which was significantly different from non-DFS gamblers who gambled primarily in land-based venues (82%) (χ2 = 415.99, df = 2, p = .000).
Multivariate Analyses
Multiple logistic regression was used to evaluate the relative contributions of the predictor variables, which had proven significant in univariate analyses, to the likelihood of membership in the DFS player group. Continuous variables included age and number of gambling activities. All other variables were dummy coded. The minimum criteria for entry of covariates into the model were a p value of less than .05. Partial odd ratios (ORs) and 95% confidence intervals (CIs) were computed for significant predictors. Model effects were estimated both by the improvement in Chi Square and by a classification matrix indicating the proportion of individuals correctly identified by the model covariates.
One important goal of this research was to begin to identify specific factors (mental health, substance use, and gambling behavior) that differentiate DFS players from non-DFS gamblers. Therefore, forward selection logistic regression analyses were performed, entering in Block 1 demographic variables that had proved to be significant in the prior analyses between the two groups. These included gender, age, race/ethnicity, relationship status, and employment status. Substance use, behavioral addiction, and mental health variables were entered in Block 2, to determine which of the significant variables added most to the regression equation overall and which, if any, had a moderating effect on the significant demographic characteristics. Gambling behavior variables were entered in Block 3 to similarly determine which added the most to the regression equation overall and had a moderating effect on the remaining Block 1 and Block 2 variables. Table 2 shows the results of the final regression.
The results of the forward logistic regression indicated a good model fit, correctly classifying 94.5% of all cases and 71.5% of DFS players. The Hosmer–Lemeshow goodness-of-fit statistic also indicated that the model fit was adequate, χ2 (8, N = 2147) = 10.424, p = .237. The most significant predictors of membership in the DFS players group in the final model were participation in more types of gambling activities than other gamblers, high frequency gambling, male gender, and reporting suicidal thoughts in the past 12 months.
Men were five times more likely than women to be DFS players. For each additional gambling activity, an individual was 7.4 times more likely to be a DFS player. High frequency gamblers were 5.2 times more likely than low-frequency gamblers to be DFS players, and moderate frequency gamblers were 2.99 times more likely to be DFS players than low frequency gamblers. DFS players were 4.1 times more likely than other participants to endorse suicidal thoughts in the past year; however, endorsing a suicide attempt in the past year was a negative predictor for DFS player membership, lowering the odds by 0.87%. Other significant predictors that nearly doubled the chances of being a DFS player included being Hispanic (vs. Caucasian) and/or single (vs. married or living with a partner). The results found a significant negative relationship for age: each one-year increase in age decreased the odds of being a DFS players by .03%.
Notably, no single gambling activity predicted membership in the DFS group. Rather, endorsing any one gambling activity alone variously lowed the odds of DFS player membership by, for example, 0.89 times for gaming machine play and 0.69 times for sports betting. However, the additive effect of playing multiple games strongly predicted the DFS player group (7.4 times).
Discussion
This is the first comprehensive look at a representative sample of DFS players in the United States, where there has been considerable debate over whether or not DFS is a form of gambling. Irrespective of classification, the findings of this study suggest that most DFS players also gamble and they experience significantly higher rates of comorbid substance and mental health problems than the average gambler. As in prior studies, the current analyses found that a majority (all but seven here) of DFS players also gambled and that they gambled on significantly more activities than did others who gambled but did not play DFS.
DFS players are characteristically young, employed, single males, however this study also found Hispanic or Asian ethnicity to be significant predictors. Compared to other gamblers who played an average of two games, DFS players endorsed an average of more than seven gambling activities, including both gambles of skill (e.g., live poker, casino table, sports) and luck (e.g., gaming machines, lottery, scratch-offs, bingo). Similarly, while a majority of non-DFS gamblers wagered without problems in primarily land-based venues, DFS players were more likely to be moderate or problem gamblers and to gamble once a week or more online as well as in land-based venues. Notably, DFS players were four times more likely than other gamblers to report suicidal thoughts in the past year and significantly more likely to report comorbid substance use and abuse, behavioral addictions and recent mental health problems, when compared to other gamblers.
Taken together, these findings suggest that DFS players likely share etiological characteristics with a subgroup of problem gamblers who are motivated by a desire to escape aversive mood states or who utilize gambling as an additional form of sensation-seeking and an outlet for impulsivity (Blaszczynski and Nower 2002). It is possible that the highly variable and dynamic nature of DFS play, analogous to sports betting and day trading, fuels a quest for action across multiple of activities that leads to increasingly frequency of play and, ultimately, to the development of gambling problems. Alternatively, gambling problems may result from the accumulative effect of involvement in multiple forms of play, including DFS play. The most troubling finding from this study, however, is the suggestion that Hispanic or Asian ethnic groups may be most at risk, although they are least likely to find targeted prevention, intervention or treatment services in most states. That finding is underscored by the revelation that DFS gamblers reported higher rates of substance use and abuse, mental health problems and suicidality, suggesting further that the most vulnerable members of this group may have the fewest outlets for help-seeking.
The study had some limitations, including a relatively small sample size and geographic limitation to New Jersey. However, the inclusion of this population in an epidemiologic study with a comprehensive and standardized questionnaire provides important baseline data for additional study. Future research should focus on identifying the nature and course of DFS play compared to gambling as well as the motivations for engaging in one or both activities. In addition, it will be important to more clearly identify the etiological risk factors that predispose DFS players to high frequency gambling and other addictive behaviors, to investigate membership in etiological subgroups, and to better understand the ethnic factors that may contribute to the development and maintenance of DFS play, particularly in concert with problem gambling.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual (4th ed.), Text Revision (DSM-IV-TR). Washington: American Psychiatric Association.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5). Washington: American Psychiatric Association.
Billings, A., Ruihley, B. J., & Yang, Y. (2016). Fantasy gaming on steroids? Contrasting fantasy sport participation by daily fantasy sport participation. Communication and Sport. https://doi.org/10.1177/2167479516644445.
Blaszczynski, A., & Nower, L. (2002). A pathways model of problem and pathological gambling. Addiction, 97(5), 487–499.
Draftkings (2016). DraftKings Lobby [Webpage]. Retrieved from August 30, 2016 https://www.draftkings.com/lobby#/featured.
Drayer, J., Dwyer, B., & Shapiro, S. L. (2013). Examining the impact of league entry fees on online fantasy sport participation and league consumption. European Sport Management Quarterly, 13(3), 339–357. https://doi.org/10.1080/16184742.2013.783605.
Fantasy Sports Trade Association. (2016). Industry demographics | FSTA. Retrieved from http://fsta.org/research/industry-demographics/.
Ferris, J. A., & Wynne, H. J. (2001). The Canadian problem gambling index. Ottawa, ON: Canadian Centre on Substance Abuse.
Lorains, F. K., Cowlishaw, S., & Thomas, S. A. (2011). Prevalence of comorbid disorders in problem and pathological gambling: Systematic review and meta-analysis of population surveys. Addiction (Abingdon, England), 106(3), 490–498. https://doi.org/10.1111/j.1360-0443.2010.03300.x.
Marchica, L., & Derevensky, J. (2015). Fantasy sports: A growing concern among college student-athletes. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-015-9610-x.
Martin, R. J., & Nelson, S. (2014). Fantasy sports, real money: Exploration of the relationship between fantasy sports participation and gambling-related problems. Addictive Behaviors, 39(10), 1377–1382. https://doi.org/10.1016/j.addbeh.2014.05.017.
Martin, R. J., Nelson, S. E., & Gallucci, A. R. (2015). Game on: Past year gambling, gambling-related problems, and fantasy sports gambling among college athletes and non-athletes. Journal of Gambling Studies. https://doi.org/10.1007/s10899-015-9561-y.
Mills, B. M., Kwak, D. H., Lee, J. S., & Lee, W.-Y. (2014). Competitive environments in fantasy sports gaming: Effects of entry fees and rewards on opposition quality and league sorting. International Gambling Studies, 14(1), 161–180. https://doi.org/10.1080/14459795.2014.881904.
Pickering, D., Blaszczynski, A., Hartmann, M., & Keen, B. (2016). Fantasy sports: Skill, gambling, or are these irrelevant issues? Current Addiction Reports, 3(3), 307–313. https://doi.org/10.1007/s40429-016-0111-1.
Rodenberg, R. (2016). Daily fantasy—DFS legalization tracker for all 50 states. Retrieved from August 30, 2016 http://www.espn.com.au/chalk/story/_/id/14799449/daily-fantasy-dfs-legalization-tracker-all-50-states.
Ruihley, B. J., & Hardin, R. L. (2011). Message boards and the fantasy sport experience. International Journal of Sport Communication, 4(2), 233–252.
Unlawful Internet Gambling Enforcement Act (UIGEA), 31 USC 5361-5366 31 USC 5361-5366. (2006). Retrieved from https://www.law.cornell.edu/uscode/text/31/subtitle-IV/chapter-53/subchapter-IV.
US Census Bureau. (2016). Population estimates. Retrieved from August 30, 2016 https://www.census.gov/popest/data/.
Van Natta, D. J. (2016). The inside story of the quick rise and quicker fall of DraftKings and FanDuel. Retrieved from August 28, 2016 http://www.espn.com/espn/feature/story/_/id/17374929/otl-investigates-implosion-daily-fantasy-sports-leaders-draftkings-fanduel.
Acknowledgements
The researchers would like to thank Director David L. Rebuck, Robert Moncrief, Shien Lafshieri and Suzanne Borys for their assistance with this ongoing research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
This study was supported by a grant from the New Jersey Divisions of Gaming Enforcement (DGE), in collaboration with the Division on Addictions, Department of Mental Health and Addictive Services. Funding was provided to the DGE by law by industry corporations with online gaming licenses in New Jersey. Drs. Nower and Blaszczynski have both received grants from or consulting contracts from industry, governmental, and/or non-profit organizations on projects unconnected to this work. Author Caler is employed through the DGE grant and declares that he has no conflict of interest. Author Pickering is supported, in part, by a research center that receives funding from the gaming industry for projects unrelated to this article.
Ethical Approval
All procedures performed in studies involving human participants were approved by the Rutgers University Internal Review Board and performed in accordance with their ethical standards and those of the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Nower, L., Caler, K.R., Pickering, D. et al. Daily Fantasy Sports Players: Gambling, Addiction, and Mental Health Problems. J Gambl Stud 34, 727–737 (2018). https://doi.org/10.1007/s10899-018-9744-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-018-9744-4