
Abstract
Time-sampling methodology was implemented to examine the prospective associations between affect, desire to gamble, and gambling behavior in individuals diagnosed with a mood disorder. Thirty (9 male, 21 female) adults with a lifetime diagnosis of a depressive or bipolar disorder diagnosis who endorsed current gambling and lifetime gambling harm participated in the present study. Participants completed electronic diary entries of their current affective state, desire to gamble, and gambling behavior for 30 consecutive days. Hierarchical linear modelling revealed that affect was not a predictor of gambling behavior. Instead, affect predicted the desire to gamble, with high levels of sadness and arousal independently predicting an increased desire to gamble. Desire to gamble predicted actual gambling behavior. There were no differences across diagnostic groups in terms of gambling motivations at baseline; however, during the 30-day period, participants with bipolar disorder endorsed gambling to cope with negative affect more often than did participants with depressive disorder, whereas those with depressive disorder more often endorsed gambling for social reasons or enhancement of positive affect. The present findings provide evidence that negative affect is not directly related to actual gambling behavior, and suggest that affective states rather impact the desire to gamble.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Evidence has accrued to support the association between mood disorders and gambling problems. Investigations have consistently yielded an elevated prevalence of mood disorders within individuals with gambling problems (Kim et al. 2006; Lorains et al. 2011), as well as elevated rates of problem gambling in individuals with mood disorders (Kennedy et al. 2010; Quigley et al. 2015; Quilty et al. 2011). The nature of the association between mood disorders and problem gambling, however, remains unclear. Although seminal theorists have posited that gambling pathology may develop as a means to relieve aversive affective states (Blaszczynski and Nower 2002), others have suggested that depression may develop as a consequence of the negative life events that occur as a result of pathological gambling, for example (Roy et al. 1988).
Blaszczynski and Nower (2002) introduced a theoretical biopsychosocial framework outlining factors underlying three etiological, but not mutually exclusive, routes to problem gambling. The model incorporates three subtypes based on causes of and motivations for gambling as well as concurrent psychopathology and personality features. The ‘behaviorally conditioned’ subtype is characterized by the presence of cognitive distortions and processes in the absence of comorbid psychopathology. The ‘emotionally vulnerable’ subtype develops as a means to regulate emotion. These gamblers exhibit depression and anxiety, as well as maladaptive coping strategies. Lastly, ‘antisocial impulsivist’ subtype is associated with behavioral dysregulation, including substance use and attention deficit hyperactivity disorder features. These individuals exhibit impulsive cognitive processing, such as impaired decision-making, disinhibition, and risk-taking as well as adventure seeking with the constant desire to increase arousal.
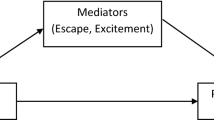
Mood-related motivations for gambling are thus implicated in the Blaszczynski and Nower (2002) model, particularly the ‘emotionally vulnerable’ pathway to problem gambling. Indeed, research in gambling motivations has empirically linked mood and gambling outcomes in numerous investigations. Stewart and Zack (2008) found that gambling for social reasons was linked with gambling frequency, whereas gambling to enhance positive moods or to cope with negative moods were linked to gambling problems. Gambling to cope with negative moods in fact predicted gambling problems even after controlling for gambling intensity, and was thus maladaptive regardless of the amount or level of gambling. The association between gambling to cope and problem gambling has been supported by other investigations as well (e.g., Clarke et al. 2007; Stewart et al. 2008; Wardell et al. 2015). In a study of motivations for electronic gaming machine gambling, for example, a significantly higher proportion of problem gamblers were motivated by the potential to avoid problems, to increase excitement, and to make money, as compared to non-problem gamblers, who were more likely to be motivated by fun and enjoyment (Nower and Blaszczynski 2010). Gamblers who expect to gain either relief of negative affect or enhancement of positive affect have been found to experience more gambling problems than gamblers without these affect regulation expectancies (Shead and Hodgins 2009). Further, the expectation that gambling will decrease negative affect is significantly associated with depressive symptoms (Young and Wohl 2009).
Negative moods have thus exhibited robust links with gambling outcomes (e.g., Matthews et al. 2009). In an investigation of the impact of a range of affective states on gambling behavior, Hills et al. (2001) conducted a laboratory study involving 60 regular gamblers (defined as gambling once a week or more) and 60 non-regular gamblers (defined as gambling less than once a month) who each received a mood induction (happy, sad, or neutral) prior to engaging in a gambling activity. The sad mood induction in fact inhibited behavior in non-regular gamblers (i.e., they gambled less), whereas no inhibitory effect was observed for regular gamblers. Hills et al. suggested that adults who gamble regularly may do so irrespective of their current mood state. A limitation of this study is its ecological validity, as the study took place in a laboratory under artificial conditions. Further, individuals with mild or greater depressive symptom severity (i.e., a score of 14 or more on the Beck Depression Inventory II) were excluded from the study, rendering the generalizability of these results to those with clinically significant mood symptoms unclear.
In contrast, Gee et al. (2005) focused on the relation between anxiety and gambling in a naturalistic study design. Participants were regular gamblers who rated their anxiety level before, during, and after a gambling episode, as well as their reasons for gambling, using mobile telephones for a period of 7–14 days. The research design permitted participants to record their responses whenever they felt the desire to gamble and immediately upon completion of a gambling activity. Gee et al. found that participants were significantly more anxious when they experienced a desire to gamble and both during and after a gambling activity than they were at baseline. The authors suggested that gambling resulted in increased anxiety, and was not used as a strategy to reduce anxiety in this investigation. Consistent with this interpretation, participants endorsed gambling “to feel better” significantly less often (15 % of the time) than they endorsed gambling “to win money” and “for enjoyment” (70 and 63 % of the time, respectively).
A notable strength of the Gee et al. (2005) study is their use of a naturalistic design and a portable device (i.e., mobile telephone) to allow for on-line reporting, which mitigates the biases that may occur as a result of artificial conditions and potential memory lapses. Further, this investigation incorporated the important intervening variable of desire to gamble. Problem gamblers endorse a greater desire to gamble than non-problem gamblers, not only during gambling-related situations, but also in non-gambling situations that evoke a sense of excitement (Sodano and Wulfert 2010). In addition, the desire to gamble appears to increase after winning for problem gamblers, but not for non-problem gamblers (Young et al. 2008). Desire to gamble has been linked to depressive symptoms in those with problem gambling in experimental work (Thomsen et al. 2009). Kushner et al. (2007) found that the majority of problem gamblers reported experiencing strong desire to gamble during exposure to a casino environment; however, a negative mood induction prior to exposure reduced rather than increased the desire to gamble. A caveat to these findings is that a “gambling specific” negative mood induction that was used, in that participants listened to the undesirable outcomes that have resulted from their gambling problem. As such, the impact of affective states on the desire to gamble and the role of desire to gamble, remain unclear.
The majority of studies that have been conducted to date have relied upon retrospective self-report measures, which assumes that individuals accurately recall and report their affective state, their reasons for gambling, and their level of gambling desire prior to past gambling activities. Further, the prospective investigations of the relationship between affect and problem gambling that have been conducted have not included individuals with mood disorders. Given that affect regulation is a well-established motivation for gambling, it is important to investigate these relations in individuals with mood disorders, as they are likely to experience elevated levels of this gambling motive due to their disorder.
The present study thus extends the work of previous investigations in a prospective examination of the relation between affective states, the desire to gamble, and gambling behavior in individuals diagnosed with a lifetime depressive disorder (DD) or bipolar disorder (BD), lifetime gambling-related harm, and current gambling involvement, with a range of motivations for gambling. We recruited participants who exhibited lifetime mood and gambling disorder and current gambling to ensure a fulsome range of mood state and gambling behavior. A time-sampling design was utilized to preserve ecological validity, by allowing data to be obtained from participants in their natural setting; this methodology was also utilized in order to eliminate possible biases in retrospective memory recall. Participants were randomly prompted to use electronic Personal Digital Assistants (PDAs) three times per day for a period of 30 consecutive days, in order to record their affective state, their desire to gamble, any recent gambling activity, and their primary motivation engaging in that gambling activity. We hypothesized that adults with lifetime DD will endorse a greater motivation to cope than those with BD, and that negative moods will predict both the desire to gamble and actual gambling behavior.
Methods
Participants
Participants were recruited from a larger study of mood disorders and gambling behavior (Quilty et al. 2011) that was conducted at a large provincial mental health facility in Canada. The sample for the larger study consisted of 275 individuals who received a lifetime diagnosis of DD (n = 138) or BD (n = 137), as assessed using the Structured Clinical Interview for DSM-IV (First et al. 1995). Individuals who met criteria for a current severe manic episode or a psychotic disorder were excluded from the study. Participants were solicited via local advertisements for a study of mood disorders and behavior, and attended two assessment sessions of interviewer-rated and self-report gambling, mood and associated behaviors. Participants completed the South Oaks Gambling Screen (SOGS; Lesieur and Blume 1987), a widely used 20-item self-report instrument designed to assess gambling pathology in a clinical context (Abbott and Volberg 2006; Gambino and Lesieur 2006; α = .94 in this sample). Individuals who endorsed one or more lifetime SOGS item and who also endorsed current gambling involvement were invited to participate in the present study after their completion of the two assessment sessions. Of the 71 potential participants informed of the current study, 30 consented to participate.
A total of 30 individuals (9 men, 21 women) agreed to participate, and were asked to respond to PDA prompts three times per day for 30 days, resulting in a maximum of 2700 PDA entries for the present study. Fifteen participants had a lifetime DD diagnosis (Major Depressive Disorder n = 12, Dysthymic Disorder n = 3; six participants were in partial or full remission), and 15 had a lifetime BD diagnosis (Bipolar Disorder I n = 14, Bipolar Disorder II n = 1; ten participants were in partial or full remission). All participants gave oral and written informed consent before participating in the study, which was approved by the Institutional Review Board (Protocol #087/2005).
Procedure
This study was approved by the institutional research ethics board. All participants provided informed consent prior to study enrolment and participation. Prior to the 30-day prospective monitoring period, participants completed the Reasons For Gambling questionnaire to determine their general motivations for gambling (RFG; Toneatto et al. unpublished manuscript). The RFG is an 11-item self-report measure of gambling motivations; each item rates reasons for gambling on a 7-point Likert scale, from −3 (strongly disagree) to 0 (neither agree nor disagree) to 3 (strongly agree). The RFG assesses three gambling motivations: (1) Winning (i.e., to win money; α = .78 in this sample), (2) Negative Affect (i.e., to gain relief from sadness/boredom; α = .88 in this sample), and (3) Social (i.e., to socialize with others; α = .69 in this sample), and has been shown to possess adequate internal consistency reliability as well as convergent validity (e.g., Wardell et al. 2015).
For a 30-day period, participants carried with them a PDA (Palm One Zire 22) with the software pre-installed. The PDAs were programmed to beep at random intervals during waking hours three times per day. At these times, participants were administered a survey of ten questions asked in a fixed sequence regarding their current location, affect, desire to gamble, most recent gambling activity, and primary motivation for gambling. If a participant failed to complete the PDA questions within 5 min, the data was considered “missed” and not used in the analyses. Participants were telephoned once each week by a trained research assistant in order to discuss any problems with entering the data, and they returned to the laboratory at day 15 and day 30 to have the data from their PDA uploaded. As compensation for participation, participants were allowed to keep the PDA after the completion of the study, and to encourage compliance with the protocol they were paid $2.00 per valid entry, up to a maximum of $180 (Whalen et al. 2001).
For each of the 90 data entry periods (3 entries per day × 30 days), participants were instructed to select their current location (home, work, school, gambling setting, or other) and social context (alone, with strangers, with friends, with family, or other). They then rated their current affect using four separate 5-point Likert scales (“How sad/happy/aroused/tranquil are you right now?” from 0 = not at all to 4 = extremely); this allowed for affect to be evaluated according to two dimensions: valence and arousal (Diener and Emmons 1984; Watson and Tellegen 1985). The valence dimension was calculated by summing the scores for the happiness item and the sadness item (which was reverse-coded) to produce a score from 0 (extremely sad/not at all happy) to 8 (extremely happy/not at all sad). The arousal dimension was calculated by summing the scores for the arousal item and the tranquility item (which was reverse-coded) to produce a score from 0 (extremely tranquil/not at all aroused) to 8 (extremely aroused/not at all tranquil).
Desire to gamble was rated by participants using a 5-point Likert scale (“How much do you feel like gambling right now” from 0 = not at all; 4 = extremely). Participants were then asked if they had gambled since their last PDA data entry, and if they had, they selected the type of gambling activity they engaged in (lottery/scratch/raffle tickets, card/dice games, bingo, stock market, slot/video lottery terminal/gambling machines, or sports/animals). Finally, participants selected their primary motivation for gambling by choosing from one of the following GMQ items: it was what my friends were doing (social), to forget my worries (coping), it is exciting (enhancement), to be sociable (social), it is fun (enhancement), or to cheer up (coping).
Data Analyses
Chi square tests were conducted to examine differences between participants with BD and with DD on demographic characteristics and the following PDA data: location, social context, type of gambling activity, and gambling motivations. Hierarchical linear modeling (HLM) was utilized to test predictions about the daily associations between affect, desire to gamble, and actual gambling behavior across the 30 days of the study. Traditional analysis of variance methods assume independence of observations. However, when the same individual completes the same measures repeatedly over several days, this independence assumption is clearly violated. Thus, to account for this interdependence, HLM (version 6.03; Raudenbush et al. 2004) was used to provide estimates among variables within events (Level 1) and model them within day (Level 2) and within person (Level 3) as random effects using maximum-likelihood estimation.
First, in order to estimate the amount of variance in the outcomes allocated at the event, day, and person levels in the prediction of desire to gamble, we constructed an unconditional model with the following equations:
in which Y ijk is desire to gamble in eventi in dayj in personk, π0jk is the mean desire in dayj for personk, and e ijk is the random event effect (deviation of desire in that event from the day mean).
in which β00k is the mean desire to gamble in person k, and r0jk is the random day effect (deviation of the day mean from the person mean).
in which γ000 is the grand mean desire to gamble, and u00k is the random person effect (deviation of person k’s mean desire to gamble from the grand mean).
To calculate the variance at each level, we used the following equations:
Second, in order to assess whether person-level variables are moderating the outcome of desire to gamble, we constructed separate models that included sex and diagnosis at Level 3. The terms at Level 1 and Level 2 remain the same as in the unconditional model, while Level 3 contains the person level predictor.
For example, using sex as the person-level predictor, γ000 is the grand mean desire to gamble, γ100 is the day level mean desire moderated by sex, and u00k is the random person effect.
Third, we constructed four separate models to test whether event level affect variables (happy, sad, aroused, tranquil) predict desire to gamble. We illustrate sadness as the event level predictor in the following model example.
where Y ijk is desire to gamble in eventi in dayj in personk, π0jk is the mean desire to gamble in dayj for personk, π1jk is the mean level of sadness experienced at the time of the event signal in dayj for personk, and e ijk is the random event effect (deviation of desire in that event from the day mean).
where β00k is the mean desire to gamble in person k, r0jk is the random day effect (deviation of the desire to gamble day mean from the person mean); β10k is the mean sadness in person k; and r1jk is the random day effect (deviation of the sadness day mean from the person mean).
where γ000 is the grand mean desire to gamble, γ100 is the day level mean desire moderated by sex, and u00k is the random person effect (deviation of person k’s mean desire from the grand mean).
Notably, these models incorporate average sadness across days (Level 2) and person level predictors (e.g., sex at Level 3). However, because person-level variables (e.g., sex, diagnosis) were not significant in the original models tested, we simplified the final models so that there were no Level 3 predictors. These analyses were repeated for the prediction of actual gambling behavior. As actual gambling behavior is a binary outcome (yes/no), estimates are based on a Bernoulli distribution.
Finally, we tested whether desire to gamble predicted whether people actually gambled on any given event. The simplest model, with desire to gamble predicting actual gambling behavior (yes/no) only converges if the slope effect is “fixed” rather than “random.” Thus, all effects of the slope were fixed.
Results
The demographic information for diagnostic groups is displayed in Table 1. There were no significant age differences across participants with DD (M = 43.67, SD = 12.52) versus BD [M = 45.60, SD = 7.49; t (28) = .51, p = 0.61]. However, there were significantly more females with BD (86.7 %) than with DD (53.3 %), χ2(1) = 3.97, p < 0.01. There were no significant differences across diagnostic groups in regards to race, marital status, education level, employment status, or annual income, all χ2s < 4.29, all ps > 0.23.
In regards to the reported severity of problem gambling, 12 participants reported a SOGS score of 5 or more, which suggests that they would meet DSM-IV criteria of a diagnosis of pathological gambling (Lesieur and Blume 1987). An examination of the number of SOGS items endorsed by participants with DD (M = 5.40, SD = 4.74) versus BD (M = 4.93, SD = 4.74) revealed no significant differences [t (28) = .25, p = 0.81], indicating similar levels of problem gambling across groups. There were also no significant differences in perceived overall motivations for gambling across diagnostic groups on each RFG factor: Winning (DD M = 2.93, SD = 6.31 vs. BD M = 3.60, SD = 5.36), Negative Affect (M = .47, SD = 6.28 vs. BD M = −1.20, SD = 6.43), Social (DD M = −4.87, SD = 2.75 vs. BD M = −2.93, SD = 3.45), all ts < 1.71, ps > 0.09.
Time-Sampling Data
A maximum of 2700 PDA entries could be collected during the study. After eliminating 731 PDA entries which were either “missed” or lost due to unit malfunction, there were 1969 valid entries (BD total = 934; DD total = 1035) for analysis.
PDA entries for participants with BD and DD are displayed in Table 2. There was a significant difference across diagnostic groups in terms of their location at time of PDA entry, χ 2(4) = 18.57, p = 0.001. Participants with DD reported being in a gambling setting at the time of entry three times more often than participants with BD. There were also significant differences in the social context at time of PDA entry, χ 2(4) = 19.96, p = 0.001. Participants with DD reported being with friends or strangers more often than participants with BD, whereas participants with BD reported being with “other” people (e.g., coworkers, students) more often than participants with DD. Type of gambling activity varied significantly across diagnostic groups, χ 2(5) = 68.27, p < 0.001. Participants with BD were significantly more likely to be engaged in the “Lottery/Scratch/Raffle Tickets” gambling activities than were participants with DD; in contrast, participants with DD were more likely to be engaged in “Card/Dice Games” and “Sports/Animals/Games of Skill” gambling activities than were participants with BD. Finally, there was a significant difference across diagnostic groups in terms of their motivations for gambling, χ 2(2) = 29.74, p < 0.001. Participants with BD were significantly more likely to endorse gambling to cope with negative affect than were participants with DD; in contrast, participants with DD were significantly more likely to endorse gambling for social reasons and for enhancement of positive affect than participants with BD.
Hierarchical Linear Models
For the outcome desire to gamble, results showed that 57 % of variance is within event, 13 % of variance is within day, and 30 % of the variance is within person. The variation between days was statistically significant such that desire to gamble varies depending on the day, χ2(734) = 957.93, p < 0.001. Moreover, the variation between people was also statistically significant such that desire to gamble varies depending on the person, χ2(29) = 545.00, p < 0.001.
For sex as the person-level moderator, results showed a statistically significant positive regression coefficient [B = .49, SE = .21, t (28) = 2.31, p = 0.03], suggesting that being a man predicts a greater desire to gamble on any given day (.49 unit increase). For diagnosis as the person-level moderator, results showed a marginally significant positive regression coefficient [B = .41, SE = .20, t (28) = 2.03, p = 0.052], suggesting that having a DD diagnosis predicts a greater desire to gamble on any given day (.41 unit increase). For the event-level affect variables, results suggest that the more the participants feel sad and the more they feel aroused, the more they desire to gamble. These effects were not moderated by their average level of sadness or arousal across the study period and they were not moderated by the sex or diagnosis of the participant (Table 3).
Turning now to actual gambling behavior as the outcome, we first wanted to assess whether person-level variables (e.g., sex, diagnosis) predicts actual gambling behavior (yes/no). Note that because actual gambling behavior is a binary outcome (yes/no), the estimate is based on a Bernoulli distribution. Neither sex nor diagnosis significantly predicted actual gambling behavior [sex: B = .88, SE = .64, t (28) = 1.37, p = 0.18; diagnosis: B = 1.06, SE = .59, t (28) = 1.80, p = 0.08]. Thus, because likelihood of actually gambling was not based on the sex or diagnosis of the participant, we eliminated these person level variables in subsequent analyses.
Similar to prior analyses with desire to gamble as the outcome, we constructed four separate models to test whether affect variables (happy, sad, aroused, tranquil) predicted actual gambling behavior. Results showed that none of the affect variables predicted actual gambling behavior [happy: B = .16, SE = .13, t (28) = 1.28, p = 0.21; sad: B = .00, SE = .15, t (28) < .01, p = 0.99; aroused: B = .05, SE = .14, t (28) = .37, p = 0.72; tranquil: B = −.21, SE = .16, t (28) = −1.30, p = 0.20]. Thus, affect was eliminated in subsequent analyses.
Finally, we wanted to test whether desire to gamble predicted whether people actually gambled on any given event. The simplest model, with desire to gamble predicting actual gambling behavior (yes/no) only converges if the slope effect is “fixed” rather than “random”. Thus, all effects of the slope were fixed. According to the unit-specific model (B = .38, SE = .09, t (28) = 3.97, p < 0.01) and population model (B = .31, SE = .08), the more a person desires to gamble, the more likely they are to actually gamble on a given event (Odds Ratio = 1.46; 95 % Confidence Interval = 1.21–1.76).
Discussion
The present study made use of time-sampling methodology to examine the prospective association between affect, desire to gamble, gambling motivations and actual gambling behavior in individuals with mood disorders. Gambling difficulties have been linked to negative affectivity within primary theoretical models (Blaszczynski and Nower 2002), empirical work has supported a link between problem gambling and negative affectivity (Bagby et al. 2007) as well as depressed mood and mood disorders (e.g., Quilty et al. 2011), and major theories of problem gambling posit a primary role of emotional regulation. Longitudinal research has supported the prospective association between gambling and depressive difficulties. Recent epidemiological research has demonstrated that risk of later mood disorders increases with gambling status (recreational gambling vs. subthreshold gambling disorder vs. gambling disorder; prospective links between mood or depressive disorders and later gambling status were not evaluated in this investigation; Parhami et al. 2014). Clinical research has also documented decreasing depression symptoms in inpatients being treated for gambling difficulties (Moghaddam et al. 2014). Qualitative research has highlighted the complexities of discerning the temporal dynamics between gambling and depressive difficulties and the need to consider individual differences (Holdsworth et al. 2012). The current project provided a nuanced investigation of the links between mood and gambling desire and behavior in a mood disordered sample with gambling symptomatology, and elucidates the temporal and possible causal sequencing of these constructs further.
The current project incorporated a sample with clinically significant mood disturbance and current gambling involvement. The incorporation of both unipolar and bipolar mood disturbance, and a range of demographic characteristics highlights the generalizability of these results despite our small sample size. Participants engaged in a range of gambling activities; although gambling products vary in their degree of risk and likely motivation (e.g., lottery versus EGM; Abarbanel 2014), all of these types have been associated with harmful or problem gambling (e.g., Quilty et al. 2014) and their links with motivation and affect have yet to evaluated prospectively in a vulnerable population. Location at time of PDA data entry and diagnostic group were found to be significantly related, indicating that participants with DD were significantly more likely than participants with BD to have been in a gambling setting at the time of the PDA entry, and were significantly more likely to have gambled during the 30-day period. It is possible that this difference this may be influenced by eligibility criteria, as individuals currently experiencing a severe manic episode were excluded from participation (i.e., at a time at which such risk taking activities might be more prevalent).
Desire to gamble was predicted by male gender as compared to female gender, as well as a DD diagnosis as compared to a BD diagnosis. The degree of sadness and arousal were also predictive of desire to gamble, such that the more the participants felt sad and the more that they felt aroused, the more they desired to gamble. These latter effects were not moderated by gender or diagnosis. Desire to gamble, in turn, was predictive of actual gambling behavior. In contrast, neither demographic nor clinical characteristics, as well as affect, were predictive of actual gambling behavior. These results converge with previous research supporting the association between depression and urge to gamble in those with gambling pathology (Thomsen et al. 2009) and provide further evidence that associations between affect and gambling behavior may not be direct (see Quilty et al. 2011), requiring the incorporation of intermediate or mediating variables.
There were no differences in overall gambling motivations across participants with DD versus those with BD. However, in the actual instances when a participant engaged in a gambling activity, motivation for gambling was related to diagnostic group. More specifically, participants with BD were more likely to endorse gambling to cope with negative affect than were participants with DD, whereas those with DD were more likely to endorse gambling for social reasons or for enhancement of positive affect than those with BD. This conflicting finding (i.e., lack of differences in self-reported gambling motivations in the laboratory versus significant differences in motivations endorsed in situ) may have important implications for future gambling motivation research, as it suggests that gambling motivations may change depending on the situational context (being in a gambling setting versus a non-gambling setting) and/or of the level of gambling desires.
Results from this study are limited by several factors. First, our eligibility criteria may have introduced some sample bias. The exclusion of individuals who reported experiencing a severe manic episode likely resulted in patients less severe forms of the disorder than would have otherwise been observed. Approximately half of our sample was in partial or full remission from their mood disorder, which may have reduced motivation to gambling for mood regulation. Yet, a full range of mood ratings was exhibited over the 30-day period, and there was no evidence of skewness or kurtosis (for daily mood, skewness <1.74 and kurtosis <2.48), suggesting that participants exhibited a normal distribution of affect. All participants endorsed lifetime gambling difficulty (as operationalized by one or more SOGS items) and current gambling involvement; however, relatively limited gambling behavior (particularly in terms of types of gambling activity) was observed during the 30-day period. Yet, a focus on participants with current mood or gambling disorder appeared likely to introduce ethical as well as scientific difficulties (i.e., a restriction of range in affect and gambling indicators). Future studies may wish to use alternate selection criteria to increase the likelihood to greater variation in gambling behavior and motivations, as well as clinically significant mood symptoms (e.g., treatment-seeking adults endorsing concurrent gambling and mood difficulties).
Another limitation of the present findings pertains to the methodology used for assessing gambling. Gambling behavior was assessed in a dichotomous fashion; it was not confirmed that each response in the affirmative represented a distinct event. Yet, a minority (n = 15) of the consecutive entries were ambiguous in this regard (i.e., the remainder of consecutive entries referred to discrete forms of gambling such as lottery play or occurred in different settings). Further, assays of gambling duration and expenditure were not included, and participants were able to select only one reason for gambling. Gambling motivations at the outset were also assessed using a novel measure, albeit one that has been successfully used in recent research (Wardell et al. 2015).
Interestingly, during the visits to the laboratory at day 15 and day 30 of the study, some participants informally reported that they had noticed changes in the frequency and intensity of gambling-related thoughts and/or changes in their gambling behavior. It is possible that the frequent responding by participants (three times a day) may have influenced their affect, desire, motivations and/or gambling activities, through the reactive effects of self-monitoring on altering the very behaviors and emotions being monitored (Korotitsch and Nelson-Gray 1999). Ecological momentary assessment has accrued evidence for its validity (Courvoisier et al. 2010); future studies might formally assess the changes in gambling desires, motivations and actual gambling behavior occurring as a result of frequent self-monitoring, in order to determine its potential therapeutic value in the treatment of problem gambling.
Overall, the findings of the present study suggest that affect was linked to cognition more so than behavior, in its links with desire to gamble in this study. Further, it was the desire to gamble that directly led to gambling behavior in this sample of adults with lifetime mood disorder. Should future research support the present findings, it could lead to potential clinical implications for the treatment of a gambling disorder in patients with mood dysregulation. In particular, an emphasis on strategies for reducing the desire to gamble and the development of self-control skills for resisting gambling urges could prove to be particularly impactful in the treatment of a gambling disorder as compared to the provision of affect management skills.
References
Abarbanel, B. L. (2014). Differences in motivational dimensions across gambling frequency, game choice and medium of play in the United Kingdom. International Gambling Studies, 14, 472–491.
Abbott, M. W., & Volberg, R. A. (2006). The measurement of adult problem and pathological gambling. International Gambling Studies, 6, 175–200.
Bagby, R. M., Vachon, D., Bulmash, E. L., Toneatto, T., Quilty, L. C., & Costa, P. T. (2007). Pathological gambling and the five-factor model of personality. Personality and Individual Differences, 43, 873–880.
Blaszczynski, A., & Nower, N. (2002). A pathways model of problem and pathological gambling. Addiction, 97, 487–499.
Clarke, D., Tse, S., Abbott, M., Townsend, S., Kingi, P., & Manaia, W. (2007). Reasons for starting and continuing gambling in a mixed ethnic community sample of pathological and non-problem gamblers. International Gambling Studies, 7, 299–313.
Courvoisier, D. S., Eid, M., Lischetzke, T., & Schreiber, W. H. (2010). Psychometric properties of a computerized mobile phone method for assessing mood in daily life. Emotion, 10, 115–124.
Diener, E., & Emmons, R. A. (1984). The independence of positive and negative affect. Journal of Personality and Social Psychology, 47, 1105–1117.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1995). Structured clinical interview for DSM-IV axis i disorders—Patient edition, version 2.0. New York, NY: New York Biometrics Research Department.
Gambino, B., & Lesieur, H. (2006). The South Oaks Gambling Screen (SOGS): A rebuttal to critics. Journal of Gambling Issues, 17. doi:10.4309/jgi.2006.17.10.
Gee, P., Coventry, K. R., & Birkenhead, D. (2005). Mood state and gambling: Using mobile telephones to track emotions. British Journal of Psychology, 96, 53–66.
Hills, A., Hill, S., Mamone, N., & Dickerson, M. (2001). Induced mood and persistence at gaming. Addiction, 96, 1629–1638.
Holdsworth, L., Haw, J., & Hing, N. (2012). The temporal sequencing of problem gambling and comorbid disorders. International Journal of Mental Health and Addiction, 10, 197–209.
Kennedy, S. H., Welsh, B. R., Fulton, K., Soczynska, J. K., McIntyre, R., et al. (2010). Frequency and correlates of gambling problems in outpatients with major depressive disorder and bipolar disorder. Canadian Journal of Psychiatry, 55, 568–576.
Kim, S. W., Grant, J. E., Eckert, E. D., Faris, P. L., & Hartman, B. K. (2006). Pathological gambling and mood disorders: Clinical associations and treatment implications. Journal of Affective Disorders, 92, 109–116.
Korotitsch, W. J., & Nelson-Gray, R. O. (1999). An overview of self-monitoring research in assessment and treatment. Psychological Assessment, 11, 415–425.
Kushner, M. G., Abrams, K., Donahue, C., Thuras, P., Frost, R., & Kim, S. W. (2007). Urge to gamble in problem gamblers exposed to a casino environment. Journal of Gambling Studies, 23, 121–132.
Lesieur, H. R., & Blume, S. B. (1987). The South Oaks Gambling Screen (SOGS): A new instrument for the identification of pathological gamblers. American Journal of Psychiatry, 144, 84–88.
Lorains, F. K., Cowlishaw, S., & Thomas, S. A. (2011). Prevalence of comorbid disorders in problem and pathological gambling: Systematic review and meta-analysis of population surveys. Addiction, 106, 490–498.
Matthews, N., Farnsworth, B., & Griffiths, M. D. (2009). A pilot study of problem gambling among student online gamblers: Mood states as predictors of problematic behavior. Cyberpsychology & Bbehavior, 12, 741–745.
Moghaddam, J. F., Campos, M. D., Myo, C., Reid, R. C., & Fong, T. W. (2014). A longitudinal examination of depression among gambling inpatients. Journal of Gambling Studies, 31, 1–11.
Nower, L., & Blaszczynski, A. (2010). Gambling motivations, money-limiting strategies, and precommitment preferences of problem versus non-problem gamblers. Journal of Gambling Studies, 26, 361–372.
Parhami, I., Mojtabai, R., Rosenthal, R. J., Afifi, T. O., & Fong, T. W. (2014). Gambling and the onset of comorbid mental disorders: A longitudinal study evaluating severity and specific symptoms. Journal of Psychiatric Practice, 20, 207–219.
Quigley, L., Yakovenko, I., Hodgins, D. C., Dobson, K. S., el-Guebaly, N., Casey, D. M., et al. (2015). Comorbid problem gambling and major depression in a community sample. Journal of Gambling Studies, 31, 1135–1152.
Quilty, L. C., Avila Murati, D., & Bagby, R. M. (2014). Identifying indicators of harmful and problem gambling in a Canadian sample through receiver operating characteristic analysis. Psychology of Addictive Behaviors, 28, 229–237.
Quilty, L. C., Watson, C., Robinson, J. J., Toneatto, T., & Bagby, R. M. (2011). The prevalence and course of pathological gambling in the mood disorders. Journal of Gambling Studies, 27, 191–201.
Raudenbush, S. W., Bryk, A. S., & Congdon, R. (2004). HLM6: Hierarchical linear and nonlinear modeling. Chicago: Scientific Software International.
Roy, A., Custer, R., Lorenz, V., & Linnoila, M. (1988). Depressed pathological gamblers. Acta Psychiatrica Scandinavica, 77, 163–165.
Shead, N., & Hodgins, D. C. (2009). Affect-regulation expectancies among gamblers. Journal of Gambling Studies, 25, 357–375.
Sodano, R., & Wulfert, E. (2010). Cue reactivity in active pathological, abstinent pathological and regular gamblers. Journal of Gambling Studies, 26, 53–65.
Stewart, S. H., & Zack, M. (2008). Development and psychometric evaluation of a three-dimensional Gambling Motives Questionnaire. Addiction, 103, 1110–1117.
Stewart, S. H., Zack, M., Collins, P., Klein, R. M., & Fragopoulos, F. (2008). Subtyping pathological gamblers on the basis of affective motivations for gambling: Relations to gambling problems, drinking problems, and affective motivations for drinking. Psychology of Addictive Behaviors, 22, 257–268.
Thomsen, K. R., Callesen, M. B., Linnet, J., Kringelbach, M. L., & Møller, A. (2009). Severity of gambling is associated with severity of depressive symptoms in pathological gamblers. Behavioral Pharmacology, 20, 527–536.
Wardell, J. D., Quilty, L. C., Hendershot, C. S., & Bagby, R. M. (2015). Motivational pathways from reward sensitivity and punishment sensitivity to gambling frequency and gambling-related problems. Psychology of Addictive Behaviors, 29, 1022–1030.
Watson, D., & Tellegen, A. (1985). Toward a consensual structure of mood. Psychological Bulletin, 98, 219–235.
Whalen, C. K., Jamner, L. D., Henker, B., & Delfino, R. J. (2001). Smoking and moods in adolescents with depressive and aggressive dispositions: Evidence from surveys and electronic diaries. Health Psychology, 20, 99–111.
Young, M. M., & Wohl, M. J. A. (2009). The Gambling Craving Scale: Psychometric validation and behavioral outcomes. Psychology of Addictive Behaviors, 23, 512–522.
Young, M. M., Wohl, M. J. A., Matheson, K., Baumann, S., & Anisman, H. (2008). The desire to gamble: The influence of outcomes on the priming effects of a gambling episode. Journal of Gambling Studies, 24, 275–293.
Acknowledgments
This study was funded by an Ontario Problem Gambling Research Centre, Level IV Grant (#2182). OPGRC approved the research proposal, including objectives and methodology, but had no involvement in the research design, conduct, analysis, or write-up.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Quilty has conducted a research project funded by Ontario Lottery and Gaming. All remaining authors declare that they have no conflict of interest.
Ethical Standard
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research ethics board, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
All participants provided informed consent and were free to withdraw at any time.
Rights and permissions
About this article

Cite this article
Quilty, L.C., Watson, C., Toneatto, T. et al. A Prospective Investigation of Affect, the Desire to Gamble, Gambling Motivations and Gambling Behavior in the Mood Disorders. J Gambl Stud 33, 115–129 (2017). https://doi.org/10.1007/s10899-016-9616-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-016-9616-8