
Abstract
Telephone surveys of US adults were conducted in 1999–2000 and again in 2011–2013. The same questions and methods were used so as to make the surveys comparable. There was a reduction in percentage of past-year gambling and in frequency of gambling. Rates of problem gambling remained stable. Lottery was included among the specific types of gambling for which past year participation and frequency of play declined. Internet gambling was the only form of gambling for which the past-year participation rate increased. The average win/loss increased for several forms of gambling, providing a modest indication that gamblers were betting more, albeit less frequently. Between the two surveys, the rates of past-year participation in gambling declined markedly for young adults. In both surveys, rates of problem gambling were higher for males than females, and this difference increased markedly between surveys as problem gambling rates increased for males and decreased for females. For the combined surveys, rates of problem gambling were highest for blacks and Hispanics and lowest for whites and Asians. In both surveys, the rates of problem gambling declined as socio-economic status became higher. Possible explanations for these trends are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gambling opportunities and expenditures have increased in the United States in the past decade (Horvath and Paap 2012). Several states voted on the legalization of state lotteries, and many states expanded their lotteries to include new types of games. Also, many states legalized gambling machines, introduced gambling machines and table games into new venues such as racetracks, expanded off-track betting on races, and allowed the opening of new casinos. It is reasonable to expect that this increase in public visibility and availability of gambling was accompanied by an increase in gambling behavior and problems. Some have argued that the prevalence of problem gambling is trending upwards (Skolink 2011; Bortz 2013) but the empirical evidence is limited and incomplete. There are vigorous ongoing debates in many states between those who advocate and those who oppose the legalization of various forms of gambling. In the context of these debates, the measurement of the recent gambling-related trends is an important undertaking. However, there have been no US national replication surveys that allow the direct examination of trends in gambling behavior and problems for the United States as a whole. Some key questions: Are Americans gambling more and experiencing more gambling problems than a decade ago? If so, which types of gambling have gained in popularity, and in which demographic groups has the increase in problem gambling been concentrated? To address this lack of information, we conducted a telephone survey of US adults which assessed gambling behavior and problem gambling, and we compared the results with those from our previous survey of gambling in the US, conducted in 2000. The current article is the first report of those results.
Estimation of the prevalence of problem and pathological gambling is dependent on the measures used. These measures come primarily from two sources: the South Oaks Gambling Screen (SOGS) (Lesieur and Blume 1987) and the American Psychiatric Association’s Diagnostic and Statistical Manual, Version IV (APA 1994). The SOGS employs 20 questions. Positive answers on five or more questions designate pathological gambling, and three or more positive answers are now commonly used to designate problem gambling. The DSM-IV contains ten criteria that define pathological gambling. An individual who is positive on five or more of them is considered a pathological gambler. Various instruments have been developed to operationalize the DSM-IV definition of pathological gambling, including the diagnostic interview schedule (DIS) for pathological gambling (Robins et al. 1996) and the NORC DSM-IV screen for pathological gambling, known as the NODS (Gerstein et al. 1999).
The concept of pathological gambling centers on compulsive, uncontrollable gambling, and also includes negative consequences from gambling (Neal et al. 2005). There are differences in emphasis between the SOGS and the scales based on the DSM-IV. The SOGS emphasizes negative consequences of gambling, including various methods that might be used to get money to gamble. The DSM-IV criteria are strongly influenced by an analogy with drug dependence and emphasize symptoms of addiction, such as tolerance and withdrawal. During the early days of gambling research the SOGS was the most commonly used scale in surveys. DSM-IV scales came to be preferred, and more recently, the Problem Gambling Severity Index (PGSI), which is associated with the Canadian Problem Gambling Index, has become commonly used in gambling surveys (Williams et al. 2012). The PGSI is balanced between addiction symptoms, such as tolerance, and negative consequences, such as financial problems.
In this article, the term “pathological gambling” is used to reference specifically a DSM diagnosis (5+ criteria) or a SOGS assessment (5+ symptoms). The term “problem gambling” is used to refer to a DSM or SOGS assessment with a lower cutpoint, typically 3+ criteria or symptoms. Thus, in our work, problem gambling encompasses all pathological gamblers plus others with milder involvement; it never refers to only those with three or four symptoms or criteria.
The most straightforward sources of figures for the prevalence of problem and pathological gambling in the US are national surveys of adults which include gambling pathology assessments. There have been six such surveys: (1) in 1975, by the University of Michigan Institute for Social Research (Kallick et al. 1979); (2) in 1999, by the National Opinion Research Center (Gerstein et al. 1999); (3) in 2000, by our own research group (Welte et al. 2001); (4) in 2001–2002, the National Epidemiological Survey on Alcohol and Related Conditions (NESARC) (Petry et al. 2005); (5) in 2001–2003, the National Comorbidity Replication Survey (Kessler et al. 2008); and in 2011–2013, a second national survey by our research group, which is reported in this article. Another source of a prevalence statistic is the meta-analysis of state and regional surveys conducted by Shaffer et al. (1997). And finally, a second meta-analysis conducted by the National Research Council (1999) which analyzed a sub-set of the most relevant of the studies analyzed by Shaffer. These meta-analyses included dozens of surveys which were in the field from 1977 to 1997.
Prevalence statistics from these sources can be seen in Table 1. This table is adapted from Petry et al. (2005, p. 17); we have added to it as appropriate. The 1975 University of Michigan survey assessed pathological gambling by a weighted sum of personality items, most of which did not refer specifically to gambling (e.g., “I generally feel it is best to be cautious and conservative with my money”, true or false). In a validity study, these items discriminated correctly between known compulsive gamblers and controls. The measures used in the later surveys, the NODS, AUDADIS-IV, DIS and CIDI, are all based on the DSM-IV. Examining the column for past-year prevalence of pathological gambling, it can be seen that the 1997 and 1999 meta-analyses (based on dozens of surveys, mostly using the SOGS), and the two figures from our research group’s survey (from the DIS and the SOGS) are all in the 0.9–1.9 % range. The NORC study, using the NODS, produced a figure of 0.1 %, the Comorbidity Replication produced a figure of 0.3 %, and the NESARC past-year figure is likely in the 0.1 % range because its lifetime figure is only 0.42 %. As can be seen from these numbers, the SOGS tended to produce a higher rate for pathological gambling. We can also see that of the four instruments based on the DSM-IV, three of them yielded very low figures, but our group’s survey produced a figure of 1.4 %. Clearly, the estimated rate of current pathological gambling is highly dependent on the instrument used. This was also the conclusion of Williams and Volberg (2010), who systematically examined the methodology of gambling surveys.
The increase in gambling opportunities has focused interest on the question of the trend in prevalence of problem and pathological gambling. It is, however, easier to demonstrate an increase in the availability of gambling than it is to demonstrate an increase in gambling problems. The data in the table are mildly suggestive. An obvious analysis is to compare the rate of lifetime pathological gambling found in the 1975 survey with the lifetime rates found in the 5 surveys conducted in 1999–2003. These are the figures in the rightmost column of the table. If we average the five rates (collapsing across method of measurement) from 1999 to 2003, we get (0.8 + 2.0 + 4.0 + 0.42 + 0.6)/5 = 1.56 %. If we compare 1.56 % to the 0.77 % obtained in 1975, an increase is suggested. Unfortunately, the method used to measure pathological gambling in 1975 was very different from modern methods.
Shaffer et al. (1997) also dealt with the question of trends in their meta-analysis. For the general population adult regional surveys from 1977 to 1997, they computed a correlation coefficient between the year of the survey and the rate of current pathological gambling, and found a statistically significant correlation of .558. When they divided these surveys into a group representing 1977–1993 and another representing 1994–1997, they found current rates of pathological gambling of 0.84 and 1.29, respectively. This difference was statistically significant. In an update of their work on gambling trends, Shaffer and Hall (2001) examined state-level replication studies, meaning instances in which telephone prevalence surveys were conducted in the same state, using the same measures and sampling, at two different times. They found that the prevalence of pathological gambling increased from 1.02 to 1.35 % between replications, and that this increase was statistically significant.
Volberg (2002) summarized the results of state-level replication studies. For those four states in which there was at least 4 years between surveys, three states showed increases in rates of problem gambling. The fourth state showed a slight decline. Surveys that were <4 years apart showed both increases and decreases in prevalence.
Wiebe and Volberg (2007) did an updated analysis of replication studies. They found that US state replication studies in the 1990s tended to show increases in problem or pathological gambling rates. Williams et al. (2012) did a further updated examination of US state replication studies and found that pairs of studies in the 1990s tended to show increases, while replications that reached into the 2000s tended to be stable or show declines.
In addition to the analysis of replication studies, Williams et al. (2012) examined all of the 202 prevalence studies that have been conducted internationally. By comparing the different surveys, they estimated the effect of assessment instrument, administration method (i.e., face-to-face, telephone, mail), time frame (past year, lifetime) and other study design parameters on the measurement of the rate of problem gambling. They then developed weighting factors that allowed the estimation of standardized, comparable rates for all the surveys. They used a statistical smoother to produce a smooth curve tracking the prevalence of problem gambling in the US from 1988 to 2008. This curve shows the prevalence rising from the late 1980s through the late 1990s, and falling thereafter. There is perhaps room for uncertainty about these conclusions. For example, states that had had several prevalence studies had a disproportionate influence on the results, compared with states that had no state surveys. That having been said, to our knowledge this report is the most complete study of this issue.
While researchers have concentrated on problem gambling, the literature also mentions rates of gambling participation. We compared rates of past-year participation in various forms of gambling between our 2000 survey and previous studies, and we found an increase in overall gambling participation in the US and large increases in rates of participation in lottery and casino gambling (Welte et al. 2002). This is consistent with the notion that gambling involvement in the US increased in the 1990s. Black et al. (2012) compared surveys conducted in Iowa in 1989, 1995, and 2006–2008. Gambling participation fell in the most recent sample, consistent with the notion that general gambling involvement fell in the 2000s.
There has been some consistency about the demographic patterns of gambling involvement found by different studies. The University of Michigan 1975 national survey found problem gambling to be more common among men than women, more common among minorities than whites, and more common among young and middle-aged adults than among older adults. These patterns were repeated in our own national survey conducted in 2000 (Welte et al. 2001). Kessler et al. (2008) found these same patterns in the Comorbidity Replication Survey, so the predominance of males, youths, and minorities among problem gamblers seems to be a durable finding. There is an interesting difference, however, between the demographic findings of the 1975 University of Michigan national survey and or own 1999–2000 national survey. In 1975, problem gambling was less common in the lowest income group, and more common among the more affluent. Kallick et al. (1979) speculated that “Perhaps it is the lack of funds or lack of opportunities to get funds which is acting as a restraint to actualizing the compulsive gambling syndrome.” If so, the restraint vanished in the next quarter century. Welte et al. (2001) found that the lowest socioeconomic status respondents had by far the highest rates of problem gambling. In the current study, we will investigate the persistence of this pattern.
In this article, we will report on a comparison of results from two national telephone surveys of gambling, conducted by our research group in 1999–2000 and in 2011–2013. These surveys used the same assessment questions, the same mode of administration, and, in general, identical methods with one exception. The later survey contained a cell phone sample in addition to a predominantly landline sample, while the earlier survey had solely a landline sample. These surveys constitute the only national replication study of gambling involvement that has been conducted in the US, which allows for the examination of changes in gambling behavior and problems.
Methods
The research projects described in this article were approved by the Social and Behavioral Sciences Institutional Review Board of the State University of New York at Buffalo. All respondents gave informed consent for their inclusion in the study.
Our research group at the Research Institute on Addictions (RIA) conducted two telephone surveys of gambling behavior and pathology in adults in the US. Twenty-six hundred and thirty-one (2,631) interviews were conducted for the first Survey of Gambling in the US (SOGUS1) in 1999–2000, and 2,963 interviews were conducted for SOGUS2 in 2011–2013. Both surveys were conducted in all 50 states and the District of Columbia The sample for SOGUS1 contained landline numbers only; for SOGUS2 both a landline sample and a cell phone sample were used. Eligible respondents were persons 18 or older. Respondents in each landline household were recruited randomly by selecting the potential respondent with the next birthday. This has been shown to be equivalent to random selection (Lavrakas 1993) and is less intrusive because it does not require listing all household members. Cell phones were assumed to be dedicated to the person who answered, and that person was recruited if they were 18 or older. The response rate corresponding to AAPOR formula RR5 (defined as the number of interviews divided by the number of households in which we ascertained that a potential respondent resided) for SOGUS1 was 65.2 %; for the SOGUS2 landline sample (1,748 respondents) it was 54.0 % and for the cell phone sample (1,215 respondents) it was 62.7 %.
For both surveys, the telephone samples were purchased from Survey Sampling, Inc. Every landline phone number in the US had an equal probability of being included in the sample, and every cell phone number likewise had the same probability as every other cell phone number. The samples were stratified by county and by telephone block within county. This resulted in samples that were spread across the US according to population distribution. Each telephone number in the landline samples was called at least seven times to determine if that number was assigned to a household containing an eligible respondent. Once a household was designated as eligible, the number was called until an interview was obtained or refusal conversion had failed. Each number in the cell phone sample was called at least seven times in an attempt to determine whether that number was associated with an eligible respondent. Interviews for both surveys lasted from 20 to 50 min (occasionally longer), depending on the answering speed of the respondents and the extent of their involvement with gambling, alcohol, and drugs. The median interview lasted slightly over 40 min. Respondents in SOGUS1 were paid $25, and respondents in SOGUS2 were paid $30. Sample management and interviewing was conducted by trained interviewers using the Computer-Assisted Telephone Interviewing (CATI) facility at the University at Buffalo’s Research Institute on Addictions.
In SOGUS1, the weight variables were calculated in three steps. First, weights were made directly proportional to the number of potential eligible respondents in the household, to compensate for the fact that a respondent who lived with more potential respondents had a lower chance of being selected. Second, the weights were adjusted to match the gender, age and race distribution in the US census. Third, the weight variable was divided by its own mean, giving it a mean of one, so the weighted N equaled the true N.
Weighting in SOGUS2 was a more complex process than the weighting in SOGUS1 because of the dual (cell and landline) sampling frame. The weights for SOGUS2 were computed in accordance with current guidance from experts in the telephone sampling field (American Association of Public Opinion Research 2010; Kennedy and Kolenikov 2012). Since some respondents could be reached by either landline or cell phone, weighting adjustments were needed to account for the differential probabilities of selection for respondents who could have been sampled via either the landline or the cell phone sampling frame, i.e., the “dual users.” The weights were constructed in four steps.
The first step accounted for the probability of selection. Respondents were classified into three non-overlapping groups: landline only, cell phone only and both landline and cell phone. The probability of the respondent being selected was computed separately in each phone service group. For landline-only respondents, the probability of respondent selection was the ratio of the landline sample size to the landline frame size, adjusted for the number of eligible respondents in the household as described above. For cell-phone-only respondents, the probability of selection was the ratio of the cell phone sample size to the cell phone frame size. For dual users, the probability of selection was the sum of the probabilities for cell and landline users. This method of calculating weights for dual frame overlap is also called the single frame approach (Kennedy and Kolenikov 2012; Lohr 2009). Frame size figures were supplied by Survey Sampling, Inc.
The second step adjusts for differential response rates by telephone usage group. Information on the prevalence of different telephone usage groups came from the National Health Interview Survey (NHIS), a national household survey (Blumberg and Luke 2012). The percentages of the five telephone usage groups based on the NHIS are: wireless mostly, 18 %; dual, 25 %; landline mostly, 15 %; landline only, 10 %; and wireless only, 32 %. To account for the differing response rates by telephone usage group, weights were re-scaled in each of the five telephone usage groups so that the percentages in each usage group, based on the re-scaled weights, were equal to the NHIS percentages above.
The third step further adjusted the weights for the gender, age and race distribution of the US population. Data from the US Census 2010 for the United States population 18 years and over was obtained from the US Census Bureau American Factfinder web site.
At the fourth step, the weight variable was divided by its own mean, giving it a mean of one, so the weighted N equaled the true N.
These weights were applied for all the analyses reported in this article.
Both the SOGUS1 and SOGUS2 surveys included questions on the frequency of past-year gambling on specific types of gambling. These were: (1) raffles, office pools, and charitable gambling; (2) pulltabs; (3) bingo; (4) cards, not in a casino; (5) games of skill, e.g., pool, golf; (6) dice, not in a casino; (7) sports betting; (8) horse or dog track; (9) horses or dogs off-track; (10) gambling machines, not in a casino; (11) casino; (12) lottery; (13) lottery video-keno; (14) internet gambling; and (15) other gambling. An overall gambling frequency variable was produced by summing the frequency of these types of gambling, and various gambling frequency variables were constructed by recoding this overall variable. Both surveys also included, for each type of gambling, a series of questions from which the last win or loss could be calculated. The absolute value of the last win/loss is a measure of gambling quantity, a statistic which reflects the extent to which the gambler is a “big player”, as opposed to a frequent player. The absolute value is used because of a desire for a correlate of the respondent’s bet size which is unaffected by the random factor of winning or losing. Also, our analysis has shown that the absolute value is strongly predictive of problem gambling, while the signed variable is not. For purposes of comparing the two studies, this variable was corrected for change in the Consumer Price Index and expressed in constant 2012 dollars.
Our measures of pathological or problem gambling in both surveys were from the revised South Oaks Gambling Screen (SOGS-R) (Abbott and Volberg 1991) and the DIS-IV for pathological gambling (Robins et al. 1996). The SOGS contains 20 items that tap important dimensions of pathological gambling, such as going back to recover your losses (“chasing”), and using extreme measures, such as writing bad checks or selling household property, to get money to gamble. A respondent who endorsed five or more of these items qualified as a pathological gambler, with three or more indicating either a problem or pathological gambler. The DIS-IV contains 13 items that map into the 10 DSM-IV criteria, such as preoccupation with gambling and needing to gamble with increasing amounts of money to get the same excitement (“tolerance”). Endorsement of five or more criteria is considered to be DIS pathological gambling, and endorsement of three or more criteria was considered to be DIS problem gambling. Current pathological gambling by DSM-V definition could also be computed, simply by dropping the criteria that was omitted in the DSM-V (“illegal acts to finance gambling”), and by using 4 criteria rather than 5 as the standard for pathological gambling.
In both studies, the measure of socioeconomic status was based on respondent years of education, occupational prestige and family income. Occupational prestige was measured using the method of Duncan updated (Stricker 1988). For this method, the respondent’s occupation was classified into predefined categories used by the US Census, and these categories were subsequently recoded into scores based on the average prestige ratings given those categories by a US general population sample. This prestige score and the respondent’s years of education and the respondent’s family income were scaled in the 0–10 range and then averaged.
Neighborhood disadvantage was measured using a method that has been used by other researchers (Boardman et al. 2001). Data from each respondent’s census block group was attached to his or her case. (The average population of these block groups was 1,765.) The block-level variables used to make the disadvantage scale were: (1) the percentage of households on public assistance, (2) the percentage of families headed by a female, (3) the percentage of adults unemployed, and (4) the percentage of persons in poverty. These percentages were standardized and averaged with equal weights. Each respondent lived in a distinct block group, so these variables were independent across respondents.
For SOGUS1, variables reflecting distance to various gambling establishments were created as follows. Each respondent’s address was obtained during the interview. The addresses of several types of gambling establishments were obtained from Outcault Associates (Outcalt 2000). These types of establishments were: Indian casinos, non-Indian casinos, embarkation points of riverboat and cruise-ship casinos, card rooms, dog tracks, harness racing tracks, quarterhorse tracks, ordinary horse tracks, and jai alai frontons. Each respondent’s address and the gambling facility addresses were converted to map coordinates (geocoded to provide latitude and longitude) by Etak, a company specializing in digital mapping. The coordinate data were used to compute a set of proximity-to-gambling variables for each respondent. These proximity variables included radius variables (e.g., number of casinos within 10 miles) and nearest distance variables (e.g., distance to the nearest card room). Distance variables were computed using a formula which takes the curvature of the earth into account.
For SOGUS2, variables reflecting distance for various gambling establishments were created in-house by our research group at the Research Institute on Addictions. The latitude and longitude of gambling establishments was supplied by Casino City Press (2010), the successor company of Outcault Associates. The respondents’ home addresses were geocoded (converted to latitude and longitude) by using various geocoding web sites. Proximity variables were computed using a formula which takes the curvature of the earth into account.
Results
Table 2 shows a comparison of SOGUS1 and SOGUS2 on several variables that reflect gambling involvement. Because of the large number of statistical tests that were conducted, a level of .01 was used to define statistical significance. As can be seen, there are significant reductions in the percentage of respondents that gambled in the past year (82.2 % in 1999–2000 and 76.9 % in 2011–2013). Among respondents who gambled at least once in the past year, there was a significant reduction in the average number of days on which they gambled (59.9 days in 1999–2000 and 53.7 days in 2011–2013. Overall, it is clear that US residents are gambling less often. Our measure of the gambling quantity, the average win or loss in 2012 dollars, increased noticeably but was not statistically significant. The remaining dependent variables in Table 2 reflect the prevalence of problem or pathological gambling. We can see that: (1) none of these differences are statistically significant, (2) roughly half increased and half decreased, and (3) total DSM plus SOGS symptoms for the two studies are virtually identical. All indications are that the prevalence of gambling pathology in the US remained about the same over the past decade.
Table 3 compares the two surveys on the percentage of respondents who played various types of gambling in the past year. The participation rates for six types of gambling have declined significantly, including lottery and office pools etc., which are the two most popular types of gambling. Internet gambling was the only form of gambling in which the participation rate increased significantly, from 0.3 to 2.1 %, which is not surprising in view of the increase in internet use between 2000 and 2011.
The left section of Table 4 compares across surveys the number of days that respondents played various types of gambling, averaged across all respondents who played that particular type. Lottery and gambling at the track declined significantly. No type of gambling increased significantly. The right section of Table 4 compares across studies the average last win or loss in constant 2012 dollars for the various types of gambling. This measure of gambling quantity increased significantly for office pools, bingo and sports betting. It did not decline significantly for any type of gambling. During the decade of the 2000s, there apparently was a tendency for the frequency of gambling to decrease and for the size of bets to increase.
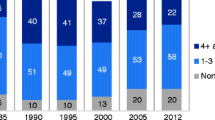
The left section of Table 5 shows how the distribution of past-year gambling has changed between studies for various demographic groups. Statistical significance is based on a logistic regression in which past-year gambling is the dependent variable and the demographic variables plus study (SOGUS1 vs. SOGUS2) are the independent variables. The asterisks in column 4 indicate that the main effect of the demographic variable is significant at the .01 level. The distribution of past-year gambling across demographic categories is shown for the separate studies only when there is a statistically significant difference between studies, that is, when the demographic variable by survey (SOGUS1 vs. SOGUS2) interaction in the logistic regression is significant at the .01 level. Males are more likely than females to have gambled in the past year (82.6 % of males vs. 76.5 %). Although significant, the various racial/ethnic groups have roughly the same past-year percentages—and this did not change between studies. However, the main effect of age shows that there is a difference in past-year gambling percentages across age groups, and this distribution is also different between surveys. Figure 1 shows the pattern. In every age group, past-year gambling was more prevalent in SOGUS1 than in SOGUS 2. However, the two surveys track closely for the three oldest age groups. In the 18–30 age group, however, the rate of past-year gambling declined substantially (88.8–78.1 %) between surveys. The last two demographic factors, SES and neighborhood disadvantage, did not have significant main effects on past-year gambling, nor did they have significant interactions between studies.

Gambling in past year by age and survey
The middle section of Table 5 shows how the distribution of frequent gambling (gambling two times a week or more) has changed between studies across various demographic groups. Gender, race, age, and SES are all related to frequent gambling. Men are twice as likely to gamble frequently as women. Blacks have the highest (14.8 %) rate of frequent gambling and Asians the lowest (3.8 %). The other racial/ethnic groups are in the 8–10 % range. The rates of frequent gambling are lowest in the youngest and oldest age groups. The tendency to gamble frequently increases in the 31–45 age group, and declines in the older age groups. The main effect of SES is significant because of a tendency for frequent gambling to be less common in the top third of SES. The interaction between SES and survey shows how the SES effect on frequent gambling has asserted itself in recent years. In SOGUS1, the rate of frequent gambling increased from the bottom third to the middle third of SES, and then dropped for the highest third. In SOGUS2, however, the rate of frequent gambling declined steadily as SES increased. Consistent in both studies is the fact that the highest SES respondents had the lowest rate of frequent gambling. The main effect of neighborhood disadvantage is not significant, but the distribution of frequent gambling across levels of neighborhood disadvantage changed between studies. Figure 2 shows that in the 1999–2000 survey, the rate of frequent gambling increased as neighborhoods became more disadvantaged. This effect disappeared in the more recent study. Between studies the SES effect became more pronounced, but the parallel neighborhood effect vanished.

Percent gambled frequently by neighborhood disadvantage and survey
The rightmost section of Table 5 shows how the distribution of current problem gambling (three or more DSM-IV pathological gambling criteria in the past year) has changed between surveys across various demographic groups. The main effects of all five of our demographic variables are significant. Combining across the two surveys, problem gambling is over twice as common among men as among women. However, the significant interaction points to an interesting finding—in the decade of the 2000s, the prevalence of problem gambling increased substantially among men (4.1 to 6.8 %), and decreased among women (2.9 to 2.5 %). Combining across surveys, problem gambling is most common among blacks (8.3 %), Hispanics (6.7 %) and Native Americans (6.6 %), and least common among Whites (2.8 %) and Asians (4.8 %). The age and SES patterns of problem gambling are clear. The prevalence of problem gambling among adults is highest in the youngest (18–30) age group, and falls off dramatically with age. The prevalence of problem gambling is highest in the lowest third of SES, and falls off dramatically with increasing SES. Combining across surveys, neighborhood disadvantage shows a clear trend with higher prevalence of problem gambling in the worst neighborhoods. The significant interaction indicates that this neighborhood effect weakened between surveys. Figure 3 shows how the problem gambling by neighborhood disadvantage curve flattened out between surveys.

Problem gambling by neighborhood disadvantage and survey
Discussion
The first notable result from the comparison of these two surveys is that rates of pathological and problem gambling remained stable during the decade of the 2000s. This occurred even though there was a general expansion of legal gambling and liberalization of gambling laws in the US during this time (Horváth and Paap 2011). In our past research (Welte et al. 2004), we found that respondents who lived within 10 miles of a casino were twice as likely to be problem gamblers as those who did not. This effect was still significant even with some possible confounding variables held constant. Respondents in both SOGUS1 and SOGUS2 lived in all 50 states, plus the District of Columbia, and were distributed geographically in proportion to the adult populations of those states. Thus, they should be affected similarly to the nation as a whole by changes in gambling laws. However, it is still theoretically possible that, by chance, the specific sample from SOGUS2 was not more exposed to nearby gambling facilities than the sample from SOGUS1. Fortunately, in both SOGUS1 and SOGUS2, we used geocoding to measure the distance from the respondent’s homes to various gambling facilities. Therefore, we can ascertain whether exposure to casinos increased for the specific respondents interviewed in our surveys. An analysis showed that in SOGUS1 (1999–2000), 11.4 % of respondents lived within 10 miles of a casino, while in SOGUS2 (2011–2013), 24.7 % of respondents lived within 10 miles of a casino. There was also an increase in the average number of casinos within 10 miles of the respondent’s homes, from 1.2 in SOGUS1 to 1.7 in SOGUS2. Thus, exposure to casinos had increased, as expected.
Based on the theory that exposure to gambling venues promotes problem gambling, one would have expected rates of problem gambling to increase between the surveys. It seemed plausible that although rates of problem gambling had been increasing early in the decade, this increase was reversed by the economic problems that started in 2008. If gambling revenues declined, as was widely reported, this would likely mean that heavy gamblers were gambling less, and therefore might be less likely to become problem or pathological gamblers. However, an examination of the economic trends in the gambling industry indicates that important gambling industries were not seriously disrupted. Horváth and Paap (2011) found that state lotteries continued to expand their business during the recent recession. Data from the American Gaming Association’s web site (www.americangaming.org, 2013) shows that casino revenue in the US was up steadily in the early 2000s, declined in 2008 and 2009, but was increasing again in the 2010–2012 period. Given these trends, the economic downturn might not be the explanation for problem/pathological gambling rates remaining stable between 2000 and 2102. However, it is possible that the incidence of new gamblers declined during the downturn in the casino business, so that there were fewer new gamblers to be recruited into the ranks of problem gamblers a few years later, and that the progression of some veteran gamblers to problem status was slowed.
Another possible explanation is the theory of adaptation. When applied to gambling, the theory of adaptation (LaPlante and Shaffer 2007) states that while initial increases in exposure to gambling venues lead to increases in rates of problem gambling, a population will eventually adapt and further negative consequences will not be forthcoming in spite of increased exposure. This might work by various mechanisms, including waning of novelty effects, development of interventions, and a reaction to increases in harmful consequences. The apparent increase revealed in the literature in the prevalence of problem gambling during the 1990s, combined with our results suggesting that problem gambling has held steady in the 2000s, seems consistent with this theory.
International experience with gambling replication surveys is mostly consistent with the theory of adaptation. The evidence shows a tendency for problem gambling rates to stabilize as opportunities to gamble expand. Abbott et al. (2004) determined that in New Zealand between 1991 and 1999, the rate of problem gambling declined in spite of increased gambling availability and gambling expenditures by the public. Bondolfi et al. (2008) noted that rate of current problem gambling remained stable in Switzerland during a 10-year period in which access to casinos was greatly expanded. In Sweden, replication surveys showed that between 1998 and 2009, past-year rates of problem gambling did not increase in spite of the fact that new forms of gambling and opportunities to gambling were introduced (Abbott et al. 2013). In a slightly discordant note, replication surveys in Britain (Wardle et al. 2011) show a small but statistically significant increase in 2010 as compared to both 2007 and 1999. However, there was no increase from 1999 to 2007, in spite of increases in gambling availability. It is clear that expansion of gambling exposure does not automatically lead to increases in the rates of problem gambling.
Storer et al. (2009) resolve the phenomenon of adaptation into three levels—individual adaptation (such as “natural recovery”), community adaptation (such as clustering gambling opportunities in a restricted location), and population adaptation (they use as one example the inability of gamblers to sustain high rates of expenditure). On close examination, individual and population adaptation seem similar, as (for example) natural recovery might involve the inability to sustain expenditures. These distinctions overlap with the contrast between the “disease model”, the advocates of which tend to stress the importance of treatment, and the public health model, the advocates of which tend to advocate restricting access. We are not encouraged to take an exclusive stand on either side of this issue. On the one hand, the results reported here do not support the notion that restricting access to gambling opportunities is necessary to prevent large increases in the rates of problem gambling. On the other hand, our own previous research and the results of Storer et al. themselves are consistent with the notion that increases in access may lead to increases in problem gambling. While acknowledging adaptation, they conclude that “actively reducing density” of gambling opportunities may be the appropriate policy response.
The percentage of respondents who gambled in the past year, as well as the frequency of gambling among those who did gamble, declined between surveys. An examination of these figures for individual types of gambling shows that office pools and charitable gambling, lottery play, and bingo are among the types of gambling for which past-year participation declined. In the case of lottery, frequency of play among those who did play in the past year also declined. While gamblers sometimes can bet heavily on any of these, they are games which tend to be associated with casual low-stakes play. It is possible that one reason that problem gambling rates did not decline while gambling participation declined is that the decline in participation tended to be among the less serious gamblers, who would not have become problem gamblers in any event. Another possibility is that the decline in gambling frequency was offset by an increase in betting quantity. The average last win or loss increased from $54 to $70 (in constant 2012 dollars) between surveys, although this change was not statistically significant.
We further examined the decline between surveys of the frequency of gambling, and the increase between surveys in the size of the average win or loss, in an attempt to understand whether these changes were associated with casual or serious gamblers. Across surveys, we looked at changes in gambling frequency and quantity for the highest 10 % in frequency and quantity in their respective surveys, and compared to those in the lowest 90 %. The frequency of gambling among the low 90 % declined 20 %, 25 times per year to 20 times per year. Frequency of gambling among the high 10 % declined 13 %, 281 times per year to 245 times per year. For gambling quantity (size of wins or losses), there was an increase of 84 % ($238–$438) for the top 10 %, and a much lower increase of 24 % ($11–$14) for the bottom 10 %. The overall pattern was that for heavier gamblers the frequency declined less and the quantity increased much more than for lighter gamblers. The size of win or loss has been shown to be a strong predictor of pathological gambling (Welte et al. 2004). The dramatic near-doubling, in constant dollars, of the win/loss size for the heaviest 10 % of bettors suggests the emergence of a new group of serious high rollers.
In her article on the “feminization” of gambling, Volberg (2003) noted that the widespread introduction of gambling machines was making gambling more female-friendly, and might be associated with increases in gambling and problem gambling among women. Nevertheless, she noted, men remained significantly more involved in gambling than women. In spite of the gambling industry’s attempts to appeal to women, that conclusion still holds. Our results from both surveys show that rates of past-year gambling, frequency of gambling among gamblers, and rates of problem gambling are all significantly higher among men than among women. Frequent gambling and problem gambling were twice as high. In addition, while the rate of problem gambling among men increased between surveys, the rate of problem gambling among women declined.
As with numerous other gambling surveys (Williams et al. 2012), we found that problem gambling was more common among blacks and Hispanics than among whites. Asians had a somewhat higher prevalence than whites, but lower than the other minorities. In problem gambling prevalence research, minority Asian populations have demonstrated mixed results. For example, Canadian (Wood and Williams 2009) and British (Wardle et al. 2011) studies have found that Asians had higher than average rates of problem gambling. However, a California survey with an exceptionally large sample of Asians found that Asians had the lowest prevalence of problem gambling of any racial group, including whites (Volberg et al. 2006). In our own survey of adolescent gambling in the US (Welte et al. 2008) we also found that Asians had the lowest rates of problem gambling. The British and Canadian results are consistent with the informal reputation of Asians as gamblers, and the US results are consistent with the reputation of Asians as avoiding problem behaviors.
The negative relationship between socio-economic status and gambling involvement continued during the decade and may have gotten stronger. In both surveys, the rate of problem gambling increased dramatically as SES declined. For frequent gambling, the pattern of steady increase with lower SES appeared in SOGUS2, while it had been less clear in SOGUS1. In our past work, we speculated that gambling pathology is particularly common among lower SES Americans because some of them are motivated to gamble by the desire to improve their financial status. This may be a particularly dangerous motive because when it doesn’t go well, the individual may gamble all the more in an attempt to turn things around.
Our past work has also shown that frequent gambling and problem gambling were more common in disadvantaged neighborhoods, even after holding socio-economic status and race constant (Barnes et al. 2013). Between the two surveys, this effect has disappeared in the case of frequent gambling and substantially weakened in the case of problem gambling. We suspected that this phenomenon might be related to a decline in lottery gambling in disadvantaged neighborhoods. Past research has shown lottery play to be common in disadvantaged neighborhoods (Barnes et al. 2011). However, in an analysis not shown in the tables, we found that eliminating lottery play from our calculation of frequent gambling did not change the pattern between surveys. Calculating frequent gambling both with and without lottery play showed that in SOGUS1 frequent gambling was more common in disadvantaged neighborhoods, while in SOGUS2 rates of frequent gambling were about the same across the neighborhood spectrum. Decline in lottery is not the explanation; some more general phenomenon is at work.
This research has some limitations. There is a potential problem to the fact that the 1999–2000 survey did not include a cell phone sample, while the 2011–2013 survey did. In 2000, it was not accepted wisdom in the survey research field that a cell phone sample was necessary, because a relatively small portion of the population was reachable only by cell phone. By 2011, this proportion of the population in the US had grown to 34 % (Blumberg and Luke 2012). Blumberg and Luke also found that cell phone subscribers were younger and poorer than the landline phone subscribers. In our own SOGUS2, the cell phone sample is more male, younger and more racial minority than the landline sample. In an Australian study, Jackson et al. (2013) found that in a dual-frame survey the cell phone respondents were more likely to be lifetime problem gamblers than the landline sample. They concluded that a cell phone sample (in addition to a landline sample) was necessary for a gambling survey to include distinct subgroups of the population. Therefore, we needed to include a cell phone sample in the recent survey, and we have taken measures to assure that our comparison of the two surveys is not compromised. In the second stage of weight development, described in the Methods section, we post-stratify by telephone type to make certain that cell phone users represent their correct proportion of the population in our analyses.
In addition to the matter of cell phones, the commonly recognized limitations of surveys—self-report and low completion rates—apply to this research. Self-report data can suffer from deceptive answers, memory “telescoping”, and other distortions. Also, there are possible biases introduced by the relatively low completion rates of modern surveys, because the potential respondents willing to be interviewed may be a biased sample of all US adults. These limitations are less onerous when comparing two surveys, as the trends between the two, both with the same methodological limitations, should be valid as the distortions cancel out. The largest limitation of this work may be the fact that we have only two surveys. To accurately determine trends, several surveys at regular intervals would be ideal. Unusual events around the time of either study could distort our view of the trend.
That being said, one of the greatest strengths of this study is that the measures and methodology used for both surveys was the same. This prevented any differences in measures or method adding to the error or bias in the results. The only difference between the two surveys is that a cell-phone sample was used in addition to the landline sample at the time of the second survey. Adding a cell-phone sample for the second survey assured that we would have access to the growing number of households and individuals with cell-phone-only accessibility. This is important because there are demographic differences between cell phone and landline populations.
References
Abbott, M., Romild, U., & Volberg, R. A. (2013). Gambling and problem gambling in Sweden: Changes between 1998 and 2009. Journal of Gambling Studies. doi:10.1007/s10899-013-9396-3. [Epub ahead of print].
Abbott, M., & Volberg, R. (1991). Gambling and problem gambling in New Zealand: Report on phase one of the national survey of problem gambling. Research Series No. 12. Wellington: New Zealand Department of Internal Affairs.
Abbott, M. W., Volberg, R. A., & Ronnberg, S. (2004). Comparing the New Zealand and Swedish national surveys of gambling and problem gambling. Journal of Gambling Studies, 20(3), 237–258.
American Association for Public Opinion Research (AAPOR) Cell Phone Task Force. (2010). Weighting in RDD cell phone surveys. In New considerations for survey researchers when planning and conducting RDD telephone surveys in the U.S. with respondents reached via cell phone numbers (pp. 61–76). Deerfield, IL: American Association for Public Opinion Research.
American Gaming Association. (2013). Gaming revenue: 10-year trend. http://www.americangaming.org.
American Psychiatric Association. (1994). DSM-IV: Diagnostic and statistical manual of mental disorders (4th ed.). Washington DC.
Barnes, G. M., Welte, J. W., Tidwell, M.-C. O., & Hoffman, J. H. (2011). Gambling on the lottery: Sociodemographic correlates across the lifespan. Journal of Gambling Studies, 27, 575–586.
Barnes, G. M., Welte, J. W., Tidwell, M.-C. O., & Hoffman, J. H. (2013). Effects of neighborhood disadvantage on problem gambling and alcohol abuse. Journal of Behavioral Addictions, 2(2), 82–89.
Black, D. W., McCormick, B., Losch, M. E., Shaw, M., Lutz, G., & Allen, J. (2012). Prevalence of problem gambling in Iowa: Revisiting Shaffer’s adaptation hypothesis. Annals of Clinical Psychiatry, 24(4), 279–284.
Blumberg, S. J., & Luke, J. V. (2012). Wireless substitution: Early release of estimates from the National Health Interview Survey, July–December 2011. National Center for Health Statistics. http://www.cdc.gov/nchs/nhis.htm.
Boardman, J. D., Finch, B. K., Ellison, C. G., Williams, D. R., & Jackson, J. S. (2001). Neighborhood disadvantage, stress, and drug use among adults. Journal of Health and Social Behavior, 42, 151–165.
Bondolfi, G., Jemann, F., Ferrero, F., Zullino, D., & Osiek, C. H. (2008). Prevalence of pathological gambling in Switzerland after the opening of casinos and the introduction of new preventive legislation. Acta Psychiatr Scand, 117, 236–239.
Bortz, D. (2013). Gambling addicts seduced by growing casino accessibility. U.S. News.com. March 28.
Casino City Press. (2010). Gaming business directory. Newton, MA: Casino City Press.
Gerstein, D. R., Volberg, R. A., Toce, M. T., Harwood, H., Christiansen, E. M., Hoffman, J., et al. (1999). Gambling impact and behavior study: Report to the National Gambling Impact Study Commission. Chicago, Il: National Opinion Research Center at the University of Chicago.
Horvath, C., & Paap, R. (2012). The effect of recessions on gambling expenditures. Journal of Gambling Studies, 28(4), 703–717.
Horváth, C., & Paap, R. (2011). The effect of recessions on gambling expenditures. Journal of Gambling Studies. doi:10.1007/s10899-011-9282-9.
Jackson, A. C., Pennay, D., Dowling, N. A., Coles-Janess B., & Christensen, D. R. (2013). Improving gambling survey research using dual-frame sampling of landline and mobile phone numbers. Journal of Gambling Studies. [Epub ahead of print].
Kallick, M., Suits, D., Dielman, T., & Hybels, J. (1979). A survey of American gambling attitudes and behavior. Ann Arbor, MI: Institute for Social Research, The University of Michigan.
Kennedy, C., & Kolenikov, S. (2012). Weighting approaches for dual frame RDD surveys. AAPOR webinar, recorded 10/11/2012, Deerfield, IL: American Association for Public Opinion Research.
Kessler, R. C., Hwang, I., LaBrie, R., Petukhova, M., Sampson, N. A., Winters, K. C., et al. (2008). DMS-IV pathological gambling in the National Comorbidity Survey Replication. Psychological Medicine, 38, 1351–1360.
LaPlante, D. A., & Shaffer, H. J. (2007). Understanding the influence of gambling opportunities: Expanding exposure models to include adaptation. American Journal of Orthopsychiatry, 77(4), 616–623.
Lavrakas, P. J. (1993). Telephone survey methods: Sampling, selection, and supervision. Newbury Park: Sage.
Lesieur, H. R., & Blume, S. B. (1987). The South Oaks Gambling Screen (SOGS): A new instrument for the identification of pathological gamblers. American Journal of Psychiatry, 144(9), 1184–1187.
Lohr, S. (2009). Multiple frame surveys. In D. Pfeffermann & C. R. Rao (Eds.), Handbook of statistics, Vol. 29A, sample surveys: Design, methods and applications (pp. 71–88). Amsterdam, The Netherlands: Elsevier.
National Research Council. (1999). Pathological gambling: A Critical Review. Washington, DC: National Academy Press.
Neal, P. N., Delfabbro, P. H., & O’Neil, M. (2005). Problem gambling and harm: Towards a national definition. Victoria, Australia: Office of Gambling and Racing, Victorian Government Department of Justice.
Outcalt, J. K. (2000). Nationwide cross reference directory of licensed gambling establishments. Gainesville, FL: Outcalt and Associates Inc.
Petry, N. M., Stinson, F. S., & Grant, B. F. (2005). Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: Results from the national epidemiologic survey on alcohol and related conditions. Journal of Clinical Psychiatry, 66(5), 564–574.
Robins, L., Marcus, L., Reich, W., Cunningham, R., & Gallagher, T. (1996). NIMH diagnostic interview schedule—Version IV (DIS-IV). St. Louis: Department of Psychiatry, Washington University School of Medicine.
Shaffer, H. J., & Hall, M. N. (2001). Updating and refining prevalence estimates of disordered gambling behavior in the United States and Canada. Canadian Journal of Public Health, 92(3), 168–172.
Shaffer, H. J., Hall, M. N., & Bilt, J. V. (1997). Estimating the prevalence of disordered gambling behavior in the United States and Canada: A meta-analysis. Boston, MA: Harvard Medical School.
Skolink, S. (2011). High Stakes: The rising cost of America’s gambling addiction. Boston, MA: Beacon Press.
Storer, J., Abbott, M., & Stubbs, J. (2009). Access or adaptation? A meta-analysis of surveys of problem gambling prevalence in Australia and New Zealand with respect to concentration of electronic gaming machines. International Gambling Studies, 9(3), 225–244.
Stricker, L. J. (1988). Measuring social status with occupational information: A simple method. Journal of Applied Social Psychology, 18(5), 423–437.
Volberg, R. A. (2002). The epidemiology of pathological gambling. Psychiatric Annals, 32(3), 171–178.
Volberg, R. A. (2003). Has there been a “feminization” of gambling and problem gambling in the United States? The Electronic Journal of Gambling Issues. eGambling, 8. http://www.camh.net/egambling/issue8/feature/index.html.
Volberg, R. A., Nysse-Carris, K. L., & Gerstein, D. R. (2006). 2006 California problem gambling prevalence survey. Submitted to California Department of Alcohol and Drug Programs Office of Problem and Pathological Gambling.
Wardle, H., Moody, A., Spence, S., Orford, J., Volberg, R., Jotangia, D., Griffiths, M., Hussey, D., & Dobbie, F. (2011). British Gambling Prevalence Survey 2010. Prepared for The Gambling Commission. London: National Centre for Social Research.
Welte, J. W., Barnes, G. M., Tidwell, M., & Hoffman, J. H. (2008). The prevalence of problem gambling among U.S. adolescents and young adults: Results from a National Survey. Journal of Gambling Studies, 24, 119–133.
Welte, J. W., Barnes, G. M., Wieczorek, W. F., Tidwell, M., & Parker, J. (2001). Alcohol and gambling pathology among U.S. adults: Prevalence, demographic patterns and co-morbidity. Journal of Studies on Alcohol, 62(5), 706–712.
Welte, J. W., Barnes, G. M., Wieczorek, W. F., Tidwell, M., & Parker, J. (2002). Gambling participation in the U.S.: Results from a national survey. Journal of Gambling Studies, 18(4), 313–337.
Welte, J. W., Barnes, G. M., Wieczorek, W. F., Tidwell, M., & Parker, J. (2004a). Risk factors for pathological gambling. Addictive Behaviors, 29, 323–335.
Welte, J. W., Wieczorek, W. F., Barnes, G. M., Tidwell, M., & Hoffman, J. H. (2004b). The relationship of ecological and geographic factors to gambling behavior and pathology. Journal of Gambling Studies, 20(4), 405–423.
Wiebe, J., & Volberg, R. A. (2007). Problem gambling prevalence research: A critical overview. A report to the Canadian Gaming Association. http://www.toronto.ca/legdocs/mmis/2013/hl/comm/communicationfile-34523.pdf.
Williams, R. J., & Volberg, R. A. (2010). Best practices in the population assessment of problem gambling. Guelph, Ontario: Ontario Problem Gambling Research Centre.
Williams, R. J., Volberg, R. A., & Stevens, R. M. G. (2012). The population prevalence of problem gambling: Methodological influences, standardized rates, jurisdictional differences, and worldwide trends. Report prepared for the Ontario Problem Gambling Research Centre and the Ontario Ministry of Health and Long Term Care. http://hdl.handle.net/10133/3068.
Wood, R. T., & Williams, R. J. (2009). Internet gambling prevalence, patterns, problems, and policy options. Guelph, Ontario: Final Report prepared for the Ontario Problem Gambling Research Centre.
Acknowledgments
This research was funded by the National Institute on Alcohol Abuse and Alcoholism Grants AA11402 and AA018097, awarded to John W. Welte.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Welte, J.W., Barnes, G.M., Tidwell, MC.O. et al. Gambling and Problem Gambling in the United States: Changes Between 1999 and 2013. J Gambl Stud 31, 695–715 (2015). https://doi.org/10.1007/s10899-014-9471-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-014-9471-4