
Abstract
Although there are many cross-sectional studies of adolescent gambling, very few longitudinal investigations have been undertaken. As a result, little is known about the individual stability of gambling behaviour and the extent to which behaviour measured during adolescence is related to adult behaviour. In this paper, we report the results of a 4-wave longitudinal investigation of gambling behaviour in a probability sample of 256 young people (50 % male, 50 % female) who were interviewed in 2005 at the age of 16–18 years and then followed through to the age of 20–21 years. The results indicated that young people showed little stability in their gambling. Relatively few reported gambling on the same individual activities consistently over time. Gambling participation rates increased rapidly as young people made the transition from adolescence to adulthood and then were generally more stable. Gambling at 15–16 years was generally not associated with gambling at age 20–21 years. These results highlight the importance of individual-level analyses when examining gambling patterns over time.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since the late 1990s, there have been a number of national and international studies that have investigated the nature and prevalence of gambling in adolescents and young adults. The consistent finding is that young people, as with their older counterparts, have an interest in gambling and can develop problems if they gamble excessively (Griffiths 2011). Although some controversy surrounds the appraisal of gambling-related problems in populations under the age of 18 years (Derevensky et al. 2003), it is generally accepted that younger people are one of the highest risk groups for problem or pathological gambling (Volberg et al. 2010). Studies of adolescents have shown that pathological and problem gambling prevalence rates are higher in adolescent samples than in adult populations (Hardoon and Derevensky 2002; National Gambling Impact Study Commission 1999; National Research Council 1999). Such findings have been obtained in studies conducted in the United States (e.g., Lesieur and Klein 1987; Shaffer and Hall 1996, 2001; Volberg and Moore 1999), Canada (e,g., Derevensky and Gupta 2000; Gupta and Derevensky 1998; Ladouceur et al. 1994; Ladouceur and Mireault 1988; Wynne et al. 1996) and Australia (e,g., Delfabbro et al. 2005; Delfabbro and Thrupp 2003; Moore and Ohtsuka 1997), as well as many European countries including the United Kingdom, Belgium, Spain, Norway, Sweden, Italy, Iceland, Finland, Denmark, Slovakia, Estonia, Lithuania and Romania (see Volberg et al. for a comprehensive review of these). Moreover, in support of these findings, research involving adult populations has consistently shown that the highest levels of gambling involvement and problem gambling are usually observed in younger age cohorts (18–30 years) (Delfabbro and Le Couteur 2011).
The typical results of studies involving adolescents show that between 60 and 80 % of young people aged 13–17 years gamble at least once per year and that around 3–5 % of young people report behaviours indicative of pathological gambling with activities such as private card games, sports-betting and instant lotteries found to be most commonFootnote 1 (Derevensky and Gupta 2000; Derevensky et al. 2003; Fisher 1992; Lesieur and Klein 1987; Shaffer and Hall 1996; Volberg et al. 2010; Winters et al. 1993). These behaviours include: chasing losses, a preoccupation with gambling, overlooking important commitments (e.g., friendships, schoolwork and/or hobbies), to continue gambling despite negative consequences, lying to friends or family about the extent of their gambling, becoming irritable if unable to gamble, frequently borrowing money and/or using lunch/bus money to fund gambling, and criminal behaviour such as stealing to get funds for gambling (Griffiths 2011).
Apart from the growing awareness of the prevalence of gambling in this age group, adolescent pathological and problem gambling has also been of interest because it is known to be linked with other developmental problems such as increased involvement in risk-taking behaviours, reduced educational performance (Gupta and Derevensky 1998; Fisher 1995, 1999; Ladouceur and Mireault 1988; Lesieur and Klein 1987), as well as poorer psychosocial adjustment (Dickson et al. 1999; Hardoon et al. 2004; Jacobs 1987; Stinchfield 2000). Adolescents with gambling problems have been found to have higher rates of delinquent behaviours including petty criminal behaviour and truancy (Fisher 1992, 1993; Griffiths and Sutherland 1998; Gupta and Derevensky 1998; Shaffer and Korn 2002; Yeoman and Griffiths 1996). Those who gamble as adolescents have also been shown to be more likely to engage in other high risk behaviours, including risky driving, alcohol consumption, and illicit drug use (Burnett et al. 1999; Griffiths and Sutherland 1998; Jackson 1999). For instance, Delfabbro et al. (2005) reported that, among adolescent problem gamblers in Australia, smoking rates were four times higher, marijuana use was six times higher and hard drug use was 20 times higher than in their non-problem gambling counterparts. Similar findings have been found in other studies and in other countries (e.g., Griffiths and Sutherland (1998) in the UK). Although it is unclear whether such problems are a consequence of or contributor to problem gambling, the strong association indicates that pathological gambling is often, at the very least, symptomatic of broader difficulties in adolescent wellbeing and development (Griffiths 2011).
Another important assumption underlying much of this research is that patterns of behaviour established during adolescence may have significant implications for the longer-term wellbeing of young people as they progress into adulthood (Volberg et al. 2010). In much the same way that smoking, illicit drug-taking and excessive alcohol consumption during adolescence is often seen as a foundation stone for similar behavioural patterns during adulthood, it is possible that the same argument might apply to gambling. Those who gamble when they are younger, and particularly those who gamble to excess, are thought to be more prone to developing problems with gambling as adults (Griffiths 2011). These views are supported, for example, in studies by Shaffer and Hall (2001) as well as Abbott et al. (2000) who found that people who experience problems as adults often retrospectively report having gambled when they were adolescents and that the earlier the onset of gambling, the greater the likelihood of subsequent problems. Similar results were reported in a recent Australian study by Dowling et al. (2010) which interviewed a sample of problem gamblers in treatment to examine their family history and early gambling experiences. Their results showed that people who were raised in homes where family members had gambling problems were significantly more likely to experience similar problems themselves as adults. Presumably, this may have resulted from these people being exposed to gambling from an early age and/or because these people shared similar characteristics to their parents that made them more likely to gravitate towards activities such as gambling.
To a large extent what is known about the links between adolescent and adult gambling has been based upon retrospective self-report studies. As various authors have pointed out (e.g., Winters et al. 2005; Slutske et al. 2003), a limitation with studies of this nature is that they do not allow one to examine the association between adolescent gambling and adult gambling over time. As a consequence, many of the conclusions drawn about the longer-term effects of adolescent gambling need to be confirmed using more refined research designs that allow more detailed longitudinal comparisons.
Some studies have sought to examine gambling trends using follow-up surveys to compare the rates of youth gambling observed at different points in time (e.g., different random cohorts obtained in 1992 and 1995 from the general population) (Moore and Ohtsuka 2001; Stinchfield 2000; Stinchfield et al. 1997; Volberg and Moore 1999; Wallisch 1993, 1996). Such studies have yielded useful insights into the stability of gambling patterns over time, but are limited because it is not possible to rule out the existence of sampling differences in the different cohorts being compared. More rigorous and genuine longitudinal designs require that the same cohort of individuals to be tracked over time (Abbott and Clarke 2007; Stinchfield 2000; Vitaro et al. 1999; Winters et al. 2002). A design of this nature was used by Winters et al. (1993) who reinterviewed 532 young people (originally aged 15–18 years) from a previous telephone survey in Minnesota. The results showed that overall gambling participation rates, as well as rates for particular activities, remained very stable from 1 year to the next. Vitaro et al. (1999) showed that young Canadian adolescents (age 12–13 years) with higher impulsivity scores and who gambled at this early age were significantly more likely to report problems with gambling at the age of 17 years. Similar findings were reported in studies conducted by Slutske et al. (2003) that examined the stability of gambling patterns in a cohort tracked from the age of 18–29 years, and also in adolescent research led by Winters (i.e., Winters et al. 1995, 2002). In Winters et al.’s. (2002) study, 305 young people were tracked from mid-adolescence (age 15 years) through to early adulthood so that it was possible to examine how rates of at-risk gambling changed over time. Once again, the results showed evidence for stability over time. The proportion of young people displaying problematic levels of gambling remained very stable from adolescence to adulthood.
All of these studies concluded that gambling patterns were generally stable over time and this is broadly consistent with the view that adolescent gambling may be a reliable predictor of subsequent rates of gambling during adulthood. However, as Winters et al. (2005) have pointed out, a persistent limitation in this research (Winters et al. 1995, 2002) was that the findings were only presented in aggregate form. In other words, although it was possible to show how the group as a whole compared over time, it did not show how stable individual behaviour had remained. Some young people may have stopped gambling altogether, while a similar number may have commenced gambling, but such changes would have been masked by the overall figures. In adult populations, it is known that problem gambling is often transitory or episodic (Slutske et al. 2003; Winters et al. 2005). Those who report being problem gamblers at one point in time often report having no difficulties when interviewed at another point (Shaffer and Hall 2001). For example, an Australian study conducted by Haworth (2005), successfully re-contacted 1,748 people who had originally been surveyed as part of the 2003–2004 Queensland Household Gambling survey (56 % response rate). All of these people were readministered the Canadian Problem Gambling Index 12 or 18 months after the original survey to determine how stable their ‘status’ had remained over time. The results showed that 72.6 % of people remained in the same CPGI category as in the previous survey, 14.3 % had moved into a higher risk group, and 13.1 % had moved into a lower risk group. Only 52 % of people who had previously been classified as problem gamblers were still problem gamblers at the follow-up point, whereas 14 % of the moderate risk group had moved into the problem gambling group (Haworth, 2005). Similar analyses undertaken by Winters et al. (2005) involving 305 young people tracked since mid-adolescence showed that only 29 % of problem gamblers at time one were still problem gamblers by early adulthood (aged over 17 years), although early problem gambling was still moderately associated with later problem gambling.
So far only one Australian study has been conducted to examine the association between adolescent and adult gambling. Delfabbro et al. (2009) examined the gambling habits of 578 adolescents aged 15–16 years that were tracked over 4 years (until all were adults aged 18–19 years). The study examined the stability of gambling on specific activities over time as well as the relationship between adolescent and adult gambling. The results showed that gambling habits are very unstable over time. For instance, young people who gambled in 1 year on a particular activity did not necessarily gamble on that same activity in other years. For example, only 14 % of young people who gambled on scratch tickets (the most popular activity in the sample) reported doing so in all 4 years of the study. Less than 5 % of those who reported gambling on card games, horse/dog racing or sports reported a consistent involvement in these activities. Similarly, only around 10 % of the sample reported gambling both during adolescence and adulthood on individual activities. Participation in individual activities at the age of 15–16 years generally did not predict involvement at 18–19 years, but stronger associations were obtained for gambling at 16–17 years and adult gambling.
The aim of the present study was to test the validity of the findings of the Delfabbro et al. study using a similar range of measures and a similar time frame. Although a smaller sample size is used, the strength of this current study was that it contained a wider range of gambling measures and involved a sample of young people drawn from the community using probability sampling. Consequently, these findings can be generalised to the broader South Australian adolescent population with much greater confidence than any previous study.
Methodology
Sample
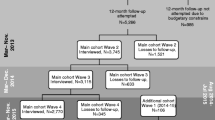
This project was based on an analysis of data collected for the Independent Gambling Authority of South Australia by the Population Research and Outcome Studies Unit, South Australian Department for Health (2008, 2009, 2010). Data were drawn from the original survey as well as the three subsequent telephone surveys. The original population survey was based on probability sampling from residential addresses in the State of South Australia. Addresses were selected at random from current telephone directory listings and data were post-weighted based on area, age, gender and the probability of selection within each household so that it reflected the Australian Bureau of Statistics (2009) census. The target age range for the survey was 16+ years. In this paper, we present the results for the subset of randomly selected respondents who were aged 16–19 years at the age of the original survey who agreed to be contacted again as a part of a longitudinal investigation. As indicated in Table 1, respondents were recontacted by phone 2, 3, and 4 years later. The number of respondents to the surveys gradually decreased over time, although much of the sample attrition occurred from Time 1–2 (63 % retention rate).
The analyses described in this paper are based on the 256 cases for which there are complete data at all four time-points. This sample comprised 50 % female and 50 % male participants and was very similar to the original sample of 341 adolescents in terms of demographics, problem gambling scores, as well as gambling participation rates for all forms of gambling at the baseline point (2005).
Measures
-
(a)
Gambling Participation
All respondents were asked to indicate whether and how often they had participated in a range of gambling activities in the previous 12 months. These activities included lotteries, keno, scratch tickets, bingo, EGMs, horse/dog racing, casino table games, sports betting, and private card games. The frequency of gambling was determined by asking respondents how many times per year, month, or week they had gambled on each activity. All of these activities were consistently available in South Australia during the period spanning the duration of the study. No major changes in the availability and prevalence of gambling activities occurred during this period (Productivity Commission, 2010).
-
(b)
Problem and/or Pathological Gambling
At time 1, 16–17 year old participants completed the DSM-IV-J (Fisher 1992), a standardised checklist designed to measure pathological gambling in adolescents as based on the DSM-IV criteria. The DSM-IV-J is a 12-item scale that includes gambling behaviours such as a preoccupation with gambling, being restless or irritable when not able to gamble, chasing losses, spending lunch money on gambling, stealing to fund gambling and the presence of social conflict. The items are scored using a ‘yes/no’ format with a total score of four or more indicative of problem gambling. The internal reliability of this scale has been found to be very good in other South Australian studies (Delfabbro and Thrupp, 2003). Adult participants (aged 18+ years) were administered the Problem Gambling Severity Index (PGSI) from the Canadian Problem Gambling Index (Ferris and Wynne 2001). The PGSI is a 9-item scale in which respondents rate their endorsement of a series of statements on a 3-point scale, where 0 = Never, 1 = Some of the time, 2 = Most of the time, and 3 = Almost always.
-
(c)
Early Experiences and Motivations
Respondents were asked to indicate whether they had obtained a big win or big loss when they had first started gambling. They were also asked at what age (in years) they first gambled for money and their primary motivations for gambling (e.g., for enjoyment, to win money, to escape problems, etc.).
Results
Prevalence of Gambling Participation Over Time
An initial analysis examined the percentage of respondents who reported gambling at each of the four interview points. A summary of these data is provided in Table 2. Table 2 shows how participation rates changed over time as the sample made the transition from adolescence into early adulthood. From Time 1 to Time 4, the rate of lottery participation increased by 2.5 times, one-third more purchased scratch tickets, three times as many respondents gambled on sports betting, and 2.5 times as many gambled on horse/dog racing. Reported EGM participation rates doubled over this four-year period. By contrast, there was relatively little change in keno, bingo, or private card games. Much of the change in participation occurred from Time 1 to Time 2. McNemar Change Tests applied to these data showed significant increases in participation from Time 1 to Time 2 for lotteries, private card games, sports betting, EGMs, and horse/dog racing. As might be expected, the participation rates for Time 3 and 4 were most similar because the entire sample was aged over 18 years by this time, and therefore legally able to gamble on all the activities listed.
Gender Differences in Participation
A second analysis involved an examination of participation trends for males and females separately. Only a summary of these findings is provided in the interests of parsimony.Footnote 2 For lotteries, females started off having a higher lottery participation rate (almost four times higher) when younger, but the participation rates rapidly converged thereafter and showed a consistent rate of growth over the ensuing 3 years. Females were more likely to purchase scratch tickets than males for the duration of the tracking period, although this difference was not significant at the final survey point. For both groups, there was evidence of an initial increase in participation rates as the majority of the sample made the transition from adolescence to early adulthood, but then the rate of participation was very consistent thereafter. Keno was consistently more popular amongst male respondents with the greatest difference being observed at the third survey point (with respondents aged 18–22 years). By Time 4, the participation rates had started to converge. Playing private card games was significantly more likely to be reported by male rather than female respondents. At Time 1, males were over twice as likely to engage in this form of gambling, but around seven times more likely by the time of the final survey. Involvement in private card games remained consistently low for females, initially increased for males, but then stabilised once the sample had reached adulthood. Sports betting participation rates were consistently higher amongst males at all time points, although participation rates steadily increased over time for both groups. This rate of increase was very consistent amongst males (almost monotonic). EGM participation rates were very similar for males and females. Participation rates were very similar at every time point and there was a steady increase in participation rates across time. There were significant differences in the participation patterns observed for casino table games. Although both groups started off relatively similar, the two rates rapidly diverged as increasing numbers of respondents in the sample made the transition into adulthood. By Time 3 (aged 18–22 years), male participation rate were over nine times higher than for females and a similar difference remained at Time 4. Finally, horse/dog racing participation rates were generally similar when the respondents were 16–17 years of age, but rapidly diverged once the sample reached adulthood. Male participation rates were around 8–10 % higher throughout the course of the study.
Consistency of Gambling Involvement over Time
Given the availability of data from the sample respondents across multiple time points, it was possible to ascertain the consistency of participation in individual activities. In other words, if a person gambled on a particular activity in one survey, it was possible to see if they gambled on the same activity when surveyed a year or two later. Consistency was determined by deriving counts for each individual across each activity: 0 = The person never gambled on the activity, 1 = The person gambled on the activity at only one point in time, 2 = Gambled at 2 points in time, 3 = Gambled at 3 points in time, and 4 = Gambled at all 4 points in time. A summary of the results of this analysis is presented in Table 3.
Table 3 provides a summary of overall participation rates across the four measurement points. By subtracting the figures in the second column from 100 %, it was possible to determine what percentage of the sample reported gambling on the different activities throughout the study. As indicated, by far the most commonly reported activity was EGM playing. Only 18 % of the sample had never played EGMs. Two-thirds of the sample gambled on scratch tickets, almost half on lotteries, and just under a half on horse/dog racing. By contrast, only 25 % had ever played keno and only around one-third had gambled on table games, cards, or placed sports bets. Table 3 shows that only a relatively small proportion of the sample reported gambling on the same activity at every time point. Thirteen percent gambled on EGMs and scratch-cards at all four survey points, 6 % consistently on lotteries, but all other figures were below 5 %. In other words, the results suggest that people’s gambling habits were quite variable from one year to the next.
Adolescent vs. Early Adult Trajectories
The original sample of young people interviewed in 2005 comprised both adolescents (<18 years) as well as some young people who were 18–19 years old. Since adolescents cannot legally gamble on commercially available forms of gambling, it may therefore be somewhat misleading for participation figures to be presented at each time point without separating out these two groups. Thus, it was important to separate out the results for those who were aged under 18 and 18+ at the time the first survey was conducted. In this way, it becomes possible to examine how participant rates changed as the same group of individuals progressed from adolescence into adulthood. To conduct these analyses, two groups were created. Group 1 (adolescents, n = 142) comprised those who were 16–17 years old at the time of the first survey and Group 2 (adults, n = 114) comprised those who had been 18–19 years when first interviewed. These two groups did not differ in their gender composition. Participation rates were determined in both of these groups at the different time points, and then compared over time.
The first set of comparisons conducted using the 2005 data (Time 1) is presented in Table 4 and shows that young adult participation rates were significantly higher than for the adolescents. In fact, very few adolescents reported gambling on anything other than scratch tickets. The largest difference was for EGMs, with young adults being over 11 times more likely to report this form of gambling than adolescents.
Table 5 shows that the participation rates amongst both groups increased over time for many of the activities, but that the increases were greater for the adolescent group as they made the transition to adulthood. By the second survey, there were only four activities (i.e., lotteries, EGMs, table games and horse/dog racing) that were more commonly reported by the adult group.
By the time of the third survey (i.e., a time when both groups were all adults), there were no significant differences in participation. In other words, the two groups ended up being very similar in their gambling preferences. Almost identical figures were obtained at the fourth survey point so these results are not presented (Table 6).
Frequency of Gambling at Time 4 as Predicted by Adolescent Gambling
An important policy issue is whether earlier involvement in gambling is related to subsequent gambling (4 years later). This issue is particularly important when considering the results for the adolescent group in determining whether under-aged gambling relates to subsequent adult gambling. To examine this question, a series of analyses were conducted using the two groups identified above (i.e., Adolescents and Young adults). For each type of gambling, respondents were divided into groups based on whether they did, or did not, gamble on that particular form of gambling in the Time 1 survey. The dependent measure for each of the analyses was the level of participation in each form of gambling at Time 4 (expressed as a rate per year). Thus, the analysis involved a 2 Group (Adolescent vs. Young Adult) × 2 Baseline Involvement (Yes/No) Analysis of Variance for each type of gambling. For example, for EGMs, this meant that the analysis examined whether participation at Time 1 (yes/no) was related to the frequency of gambling on EGMs at Time 4. This relationship was, in effect, analysed for both the original adolescent and young adult group.
The frequency of gambling on each activity in Time 4 is summarised in Table 7. As indicated, there are mean rates for all four cells of the design. For almost all of the activities, the participation rates at Time 4 were higher if the respondent had gambled on that activity at Time 1 (the Yes columns). This effect was significant for: lotteries, scratch tickets, keno, private card games, and horse/dog racing. None of the 2 Group × 2 Participation Time 1 interactions were significant, so this was not necessarily an effect that was any more strongly observed in adolescents. For both groups, having an involvement at Time 1 for the activities listed above was associated with more frequent participation at Time 4.
Multivariate Modelling of Time 4 Gambling Involvement
To determine whether earlier gambling involvement predicted gambling at Time 4, a series of logistic regression models was completed for each type of gambling. For each analysis, the dependent measure was participation at Time 4 (e.g., Lottery 0 = No, 1 = Yes) and the predictors were participation variables (0 = No, 1 = Yes) from each of the previous three surveys. A simplified version of the final analyses in provided in Table 8. The table shows the odds-ratios for significant predictors and the percentage of cases correctly satisfied (an indicator of the strength of the model). Each odds-ratio indicates the influence of each variable on participation at Time 4, e.g., 2.70 at Time 2 would indicate that a person who participated in that activity at Time 2 was 2.70 times more likely to participate at Time 4.
Table 8 indicates that, for some forms of gambling (e.g., lotteries, scratch tickets, private cards, EGMs and table games), the best predictor of participation at Time 4, was what the person had been doing the year before (Time 3). Participation at Time 1 was not generally predictive of participation at Time 4 except for scratch tickets and horse/dog racing. Participation 2 years prior to Time 4 was also generally predictive of subsequent participation, but not as strongly as for reported behaviour at Time 3.
Consistency in Gambling-Related Problems
Very few of the 256 respondents reported difficulties with gambling in any of the four surveys. At Time 1, only two respondents were classified pathological gamblers. At Time 2, two were moderately at risk on the PGSI, six were moderately at risk at Time 3, and seven were moderately at risk at Time 4. No problem gamblers were identified at Times 2–4. An analysis was undertaken to determine whether those who reported at least one symptom on the screening instruments also reported problems at other times. In total, 33 (12.9 %) scored one or more on a screen at once during the course of the study (i.e., across the 4 surveys). Of the 16 who scored at least one point at time 4, 12 of them had scored previously (75 %), but none of these 16 scored a point in the first survey. In other words, there was very little consistency in the reporting of gambling-related problems. In particular, there was little evidence that young people who scored positively at Time 4 had any history of having reported similar problems as adolescents.
Gambling-Related Problems at Time 4
As a result of the low prevalence of gambling problems, an analysis was undertaken to obtain insights into the extent to which any problematic behaviours or consequences indexed by the PGSI could be predicted by demographics and earlier gambling participation scores. This method is similar to a method used by Delfabbro and Thrupp (2003) in a study of adolescents. Although not predictive of problem gambling per se, these analyses were included to provide indicative information concerning the predictive value of earlier gambling participation in relation to the occurrence of subsequent problem gambling indicators. An analysis of the 16 respondents who scored at least one point on the PGSI at Time 4, showed that all but one of these people were male, but that there were no significant age differences. When their gambling habits at Time 1 were compared to those who scored 0 on the PGSI at Time 4, it was found that the group of 16 were significantly more likely to have played keno at Time 1 (31.3 vs. 8.8 %), played private card games (31.3 vs. 12.5 %), and to have gambled on horse/dog racing (31.3 vs. 11.3 %), all p < .05. A further analysis examined whether the 16 differenced in the number of different activities reported at Time 1. There was a trend towards the 16 having engaged in a larger number of activities (M = 2.06, SD = 1.88 for the 16 M = 1.25, SD = 1.65 for the rest of the sample), but this only approached significance, t (254) = 1.89, p = .06. However, those who had non-zero PGSI scores at Time 4 reported one important difference. This group was significantly more likely (62.5 %) to have recalled having experienced a big win when they started gambling as compared with the other group (25.1 %), χ2 (df = 1, N = 256) = 10.39, p < .01. They were also more likely to have started gambling earlier (M = 16.63 years, SD = 1.63 vs. M = 17.62, SD = 1.75), t (254) = 2.22, p < .05. Other analyses showed that the two groups did not differ in their likelihood of reporting a large loss when they started gambling, or with whom they first gambled, in their motivations for gambling, or in how they family members gambled.
Discussion
The purpose of this study was to examine the stability of gambling patterns as young people progressed from adolescence to adulthood, as well as the association between adolescent and adult gambling. On the whole, the findings were generally consistent with an earlier study conducted by Delfabbro et al. (2009). Young people’s gambling habits varied considerably from 1 year to the next. Only a relatively small proportion of the sample reported gambling any one type of gambling in all four surveys. There were also few significant associations between gambling participation at age 16–17 years and participation 4 years later. While there was evidence that early gambling on horse/dog racing and scratch cards predicted subsequent gambling, this was not found to be so for all the other forms of gambling. Instead, the best predictor of participation in specific activities during adulthood was what the respondents had reported doing in the previous year. A further series of analyses similarly found little consistency in respondents’ reporting of problems related to gambling. Once again, it was not the case that those who reported difficulties with gambling in any 1 year necessarily reported problems in subsequent years. Nevertheless, it was possible to identify some adolescent precursors that were associated with gambling-related problems during adulthood. Those who reported having at least some problems with gambling at the age of 20–21 years were more likely to have gambled on a number of activities at the age of 15–16 years, tended to start gambling at an earlier age, and also were more likely to report a big win when they first started gambling. Having a big win early in a person’ gambling career is often reported as a risk factor in the development of problem gambling (Mentzoni et al. 2012).
The finding that gambling habits were not stable over time highlights the importance of using longitudinal rather than cross-sectional studies in this area of research. The vast majority of young people in South Australia did not have regular gambling habits, but engaged in gambling in a casual and infrequent manner. Although this study did not specifically examine the detailed social context underlying gambling participation, it is likely that this inconsistency could reflect a variety of factors. For example, it may be possible that much of the reported gambling was opportunistic. In other words, gambling may have occurred only because young people happened to be in the proximity of a gambling venue or site (e.g., newsagent, hotel, etc.) while engaged in other activities, rather than the gambling being the primary motivation for going out. Others might have gambled because others around them (e.g., family members or friends) were gambling, and/or because of the occurrence of a particular event (e.g., a high profile sporting event or race, large lottery jackpot). If so, then much of the gambling observed would be subject to the same variations as these activities and opportunities, so it would therefore be less likely that respondents would gamble on the same activity over time. Not only would their frequency of gambling vary from 1 year to the next, but there would also be differences in the likelihood of them developing any problems associated with gambling because of the varying level of involvement.
Although some evidence was found to support an association between early gambling involvement and subsequent gambling problems, the balance of evidence provides little support for the view that gambling at age 15–16 years is a risk factor for subsequent problems as has been reported in a number of cross-sectional research studies (Griffiths 2011). Very few young people reported gambling problems in this sample and most positive scores on the PGSI were in the low-risk range. Moreover, as indicated above, other analyses showed that gambling at 15–16 years of age was not generally associated with gambling 4 years later (except for horse/dog racing and scratch tickets).
The study also provided useful insights into gender differences in gambling involvement and how gambling involvement developed over time. To a large extent, males reported a significantly higher degree of involvement in gambling than females for most activities and these differences were maintained over time. For both genders, there was a rapid increase in involvement once young people made the transition from adolescence to adulthood and were able to gamble legally on commercially available activities. The rates of growth were generally similar for most activities, but there was clear evidence of a divergence of interest for both sports betting and casino table games. For both of these activities, the proportion of males who reported involvement was disproportionately higher during adulthood than during adolescence and was consistent with the view that these activities still remain much more popular amongst young men than younger women. These findings are generally consistent with the results obtained in other Australian studies (e.g., S.A. Department for Families and Communities 2005) and very likely reflect broader gender differences in activity preferences, motivations for gambling, and preferences for different gambling environments (Delfabbro 2000; Delfabbro and Le Couteur 2010; McCormack et al. 2013).
The finding that reported gambling difficulties or symptoms of problem gambling during adulthood were associated with early big wins and an earlier commencement with gambling is entirely consistent with other research that has examined the same variables (Delfabbro and Le Couteur 2011; Mentzoni et al. 2012). It is known that early big wins can have what is termed a ‘priming effect’. Not only are such wins more reinforcing for gamblers, but they are also more likely to be remembered and to be influential in shaping how people perceive themselves when gambling. Those who obtain early wins are more likely to develop positive expectations about their chances of winning and to develop mental schemas that are associated with successful outcomes.
In conclusion, as with most studies of this nature it is important to take a number of methodological limitations into account when interpreting the results. First, although this study was based on participants who had originally been selected using probability sampling from the broader community, many of the original participants did not respond, or could not be contacted, in subsequent waves of the survey. It is possible, therefore, that those who chose to participate in the survey at all four time points may have differed in some systematic way from others who did not respond. These concerns are partly allayed by the fact that comparisons of base-line characteristics indicated no systematic biases in relation to the gender composition of the follow-up sample, nor in their original gambling habits, but it is not possible to rule out the possibility that the subsequent gambling habits of the retained sample may have differed from that of the non-retained sample.
Second, as with nearly all community studies, the research was based on a self-report methodology that required participants to recall their gambling over the previous 12 months. Although use of this method is very hard to avoid, it does have known limitations. One of these is the issue of recall bias, in which reports of activities during a specific period do not necessarily correspond to that period. For example, it is possible that when young people were asked to report what activities they had undertaken in the previous 12 months, some may have referred to a longer period. If there had been any within individual inconsistencies in the frames used for recall, this could partially account for some of the inconsistency in gambling habits reported between survey points.
Third, this study is limited by the fact that the sample is relatively small and only contained very few respondents with gambling-related problems. Thus, it was not possible to conduct a detailed analysis of the stability of classifications of risk as based on the PGSI. Finally, while the sample was drawn using an appropriate sampling strategy, it is recognised that young people who take part in telephone surveys may differ significantly from those who do not. The prevalence of gambling problems in the original sample of 15–16 year old was significantly lower than almost every school-based survey conducted in Australia over the last decade. While it is not inconceivable that the school surveys may also be subject to biases in the opposite direct (i.e., inflation of prevalence rates due to less random selection methods), there remains the possibility this telephone survey was unable to sample many young people with a stronger interest in gambling. For these reasons, it is important that analyses of this nature be replicated in future prevalence studies wherever this is possible so as to investigate the reliability of these findings.
Finally, this study is also only of a largely descriptive nature and it would be important to supplement studies of this nature with qualitative interviews of some participants to gain insights into young people’s motivations for gambling and their reasons for changing their gambling habits over time. Although legal accessibility clearly plays a role in increasing participation from adolescence to adulthood, subsequent changes (e.g., including the gradual stabilisation of participation rates) could be investigated further. One possibility in that many young people become involved in other life activities (e.g., study and work) which reduces the amount of leisure time available for trying new forms of gambling. Alternatively, it may be that the experience of gambling itself leads to a more realistic assessment of the long-term profitability of gambling so that it no longer appears as attractive.
Notes
Many young people in this age group gain access to adult forms of gambling via older peers, relatives or by using credit cards.
Full copies of the percentages and graphical presentation of trends can be obtained from the first author upon request.
References
Abbott, M. W., & Clarke, D. (2007). Prospective problem gambling research: Contribution and potential. International Gambling Studies, 7, 123–144.
Abbott, M., McKenna, B., & Giles, L. (2000). Gambling and problem gambling among recently sentenced males in four New Zealand prisons. Wellington: Department of Internal Affairs.
Australian Bureau of Statistics (ABS). (2009). http://www.abs.gov.au/ausstats/abs@.nsf/Products/1306.4~2009~Main+Features~People?OpenDocument#PARALINK9.
Burnett, J., Ong, B., & Fuller, A. (1999). Correlates of gambling by adolescents. In J. McMillen & L. Laker (Eds.), Developing strategic alliances: Proceedings of the 9th annual conference of the National Association for Gambling Studies (pp. 84–92). Queensland: Gold Coast.
Delfabbro, P. H. (2000). Gender differences in Australian gambling: a critical summary of sociological and psychological research. Australian Journal of Social Issues, 35, 145–157.
Delfabbro, P. H., & Le Couteur, A. (2010). A decade of gambling research in Australia and New Zealand (1992-2009): Implications for policy, regulation and harm minimization. Adelaide: Independent Gambling Authority of South Australia.
Delfabbro, P. H., & Le Couteur, A. (2011). A decade of gambling research in Australia and New Zealand (1992-2010): 5th Edition. Implications for policy, regulation and harm minimization. Adelaide: Independent Gambling Authority of South Australia.
Delfabbro, P. H., & Thrupp, L. (2003). The social determinants of gambling in South Australian adolescents. Journal of Adolescence, 26, 313–330.
Delfabbro, P. H., Lahn, J., & Grabosky, P. (2005). Adolescent gambling: A report on recent ACT research. Canberra: ACT Gambling and Racing Commission.
Delfabbro, P. H., Winefield, A. H., & Anderson, S. (2009). Once a gambler- always a gambler- longitudinal analysis of adolescent gambling patterns. International Gambling Studies, 9, 151–164.
Derevensky, J. L., & Gupta, R. (2000). Prevalence estimates of adolescent gambling: a comparison of the SOGS-RA, DSM-IV-J, and the GA 20 questions. Journal of Gambling Studies, 16, 227–251.
Derevensky, J., Gupta, R., & Winters, K. (2003). Prevalence rates of youth gambling problems: are the current rates inflated? Journal of Gambling Studies, 19, 405–425.
Dickson, L., Derevensky, J., & Gupta, R. (1999). The prevention of gambling problems in youth: a conceptual framework. Journal of Gambling Studies, 18, 97–159.
Dowling, N., Jackson, A. C., Thomas, S. A., & Frydenberg, E. (2010). Children at risk of developing problem gambling. Melbourne: Gambling Research Australia.
Ferris, J., & Wynne, H. (2001). The Canadian Problem Gambling Index (CPGI): Final report. Ottawa, ON: Canadian Centre on Substance Abuse.
Fisher, S. E. (1992). Measuring pathological gambling in children: The case of fruit machines in the UK. Journal of Gambling Studies, 8, 263–285.
Fisher, S. E. (1993). Gambling and pathological gambling in adolescents. Journal of Gambling Studies, 9, 277–287.
Fisher, S. (1995). Adolescent slot machine dependency and delinquency: Questions on a question of methodology. Journal of Gambling Studies, 11, 303–310.
Fisher, S. E. (1999). A prevalence study of gambling and problem gambling in British adolescents. Addiction Research, 7, 509–538.
Griffiths, M. D. (2011). Adolescent gambling. In B. B. Bradford & M. Prinstein (Eds.), Encyclopedia of adolescence (Vol. 3, pp. 11–20). San Diego: Academic.
Griffiths, M. D., & Sutherland, I. (1998). Adolescent gambling and drug use. Journal of Community and Applied Social Psychology, 8, 423–427.
Gupta, R., & Derevensky, J. L. (1998). Adolescent gambling behavior: A prevalence study and examination of the correlates associated with problem gambling. Journal of Gambling Studies, 16, 227–251.
Hardoon, K., & Derevensky, J. (2002). Social influences involved in children’s gambling behaviour. Journal of Gambling Studies, 17, 191–215.
Hardoon, K., Gupta, R., & Derevensky, J. (2004). Psychosocial variables associated with adolescent gambling. Psychology of Addictive Behaviours, 18, 170–179.
Haworth, B. (2005). Longitudinal gambling study. In G. Coman (Ed.). Proceedings of the 15th annual national association for gambling studies conference (pp. 128–154). Melbourne: Alice Springs.
Jackson, A. (1999). The impacts of gambling on adolescents and children. Report prepared for the Department of Human Services, Victoria.
Jacobs, D. F. (1987). Effects on children of parental excess in gambling. Paper presented at the Seventh International Conference on Gambling and Risk Taking, Reno, NV.
Ladouceur, R., & Mireault, C. (1988). Gambling behaviour among high school students in the Quebec area. Journal of Gambling Behaviour, 4, 3–12.
Ladouceur, R., Dubé, D., & Bujold, A. (1994). Gambling among primary school students. Journal of Gambling Studies, 10, 363–370.
Lesieur, H., & Klein, R. (1987). Pathological gambling among high school students. Addictive Behaviours, 12, 129–135.
McCormack, A., Shorter, G., & Griffiths, M. D. (2013). An empirical study of gender differences in online gambling. Journal of Gambling Studies. doi:10.1007/s10899-012-9341-x.
Mentzoni, R. A., Laberg, J. C., Brunborg, G. S., Molde, H., & Griffiths, M. D. (2012). Effects of sequential win occurrence on subsequent gambling behavior and urges. Gambling Research, 24(1), 31–38.
Moore, S., & Ohtsuka, K. (1997). Gambling activities of young Australians: Developing a model of behavior. Journal of Gambling Studies, 13, 207–236.
Moore, S., & Ohtsuka, K. (2001). Youth gambling in Melbourne’s West: Changes between 1996 and 1998 for Anglo-European background and Asian background school based youth. International Gambling Studies, 1, 87–102.
National Gambling Impact Study Commission. (1999). National gambling impact study commission report. Washington, DC: National Gambling Impact Study Commission.
National Research Council. (1999). Committee on the social and economic impact of pathological gambling, committee on law and justice, behavioral, and social sciences and education. Washington, DC: National Academy Press.
Shaffer, H. J., & Hall, M. N. (1996). Estimating the prevalence of adolescent gambling disorders: A quantitative synthesis and guide toward standard gambling nomenclature. Journal of Gambling Studies, 12, 193–214.
Shaffer, H., & Hall, M. (2001). Updating and refining prevalence estimates of disordered gambling behaviour in the United States and Canada. Canadian Journal of Public Health, 92, 168–172.
Shaffer, H., & Korn, D. (2002). Gambling and related mental disorders: A public health analysis. Annual Review of Public Health, 23, 171–212.
Slutske, W. S., Jackson, K. M., & Sher, K. J. (2003). The natural history of problem gambling from age 18 to 29. Journal of Abnormal Psychology, 112, 263–274.
South Australian Department for Families and Communities. (2005). Gambling prevalence in South Australia. Adelaide: Department for Families and Communities.
South Australian Department for Health. (2008). Young people’s gambling in South Australia: Interim report 1. Adelaide: South Australian Department for Health.
South Australian Department for Health. (2009). Young people’s gambling in South Australia: Interim report 2. Adelaide: South Australian Department for Health.
South Australian Department for Health. (2010). Young people’s gambling in South Australia: Interim report 3. Adelaide: South Australian Department for Health.
Stinchfield, R. (2000). Gambling and correlates of gambling among Minnesota public school students. Journal of Gambling Studies, 16, 153–173.
Stinchfield, R., Cassuto, N., Winters, K., & Latimer, W. (1997). Prevalence of gambling among Minnesota public school students in 1992 and 1995. Journal of Gambling Studies, 13, 25–48.
Vitaro, F., Arseneault, L., & Tremblay, R. (1999). Impulsivity predicts problem gambling in low socio-economic status adolescent males. Addiction, 94, 565–575.
Volberg, R., & Moore, W. (1999). Gambling and problem gambling among adolescents in Washington State: A six-year replication study 1993 to 1999. Olympia: Washington State Lottery.
Volberg, R., Gupta, R., Griffiths, M. D., Olason, D., & Delfabbro, P. H. (2010). An international perspective on youth gambling prevalence studies. International Journal of Adolescent Medicine and Health, 22, 3–38.
Wallisch, L. (1993). Gambling in Texas: 1992 Texas survey of adolescent gambling behavior. Austin, Texas: Texas Commission on Alcohol and Drug Use.
Wallisch, L. (1996). Gambling in Texas: 1995 Texas survey of adolescent gambling behavior. Austin, Texas: Texas Commission on Alcohol and Drug Use.
Winters, K. C., Stinchfield, R. D., & Fulkerson, J. (1993). Toward the development of an adolescent gambling problem severity scale. Journal of Gambling Studies, 9, 63–84.
Winters, K. C., Stichfield, R. D., & Kim, L. G. (1995). Monitoring adolescent gambling in Minnesota. Journal of Gambling Studies, 11, 165–183.
Winters, K. C., Stinchfield, R. D., Botzet, A., & Anderson, N. (2002). Prospective study of youth gambling behaviours. Psychology of Addictive Behaviors, 16, 3–9.
Winters, K. C., Stinchfield, R. D., Botzet, A., & Slutske, W. S. (2005). Pathways of youth gambling problem severity. Psychology of Addictive Behaviors, 19, 104–107.
Wynne, H. J., Smith, G. J., & Jacobs, D. F. (1996). Adolescent gambling and problem gambling in Alberta. Edmonton, Canada: Alberta Alcohol and Drug Abuse.
Yeoman, T., & Griffiths, M. D. (1996). Adolescent machine gambling and crime. Journal of Adolescence, 19, 99–104.
Acknowledgments
This paper was supported and funded by the Independent Gambling Authority of South Australia. Data for the study was extracted and compiled for analysis by the S.A. Department of Families and Communities.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Delfabbro, P., King, D. & Griffiths, M.D. From Adolescent to Adult Gambling: An Analysis of Longitudinal Gambling Patterns in South Australia. J Gambl Stud 30, 547–563 (2014). https://doi.org/10.1007/s10899-013-9384-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-013-9384-7