
Abstract
The aims of this project were to map the location and density of gambling machines in Britain; to explore whether geographic areas with higher densities of machines exist and to examine the socio-economic characteristics of these areas relative to others. Using geospatial analysis of premises records, we identified 8861 Machine Zones which were areas with a 400 meter radius around gambling machine venue and 384 High Density Machine Zones (HDMZ) with 1 or more gambling machine per hectare. There was a significant correlation between machine density and socio-economic deprivation. HDMZs had greater levels of income deprivation, more economically inactive people and a younger age profile than other areas; 37 % of those living in HDMZs were economically inactive compared with 33 % of those in non-machine areas. HDMZs were in seaside locations but also New Towns or satellite towns to major urban areas. Area affluence explains some of this pattern; of the New Towns with HDMZs, 78 % were in New Towns with a high proportion of low income areas. We therefore concluded that the distribution of gambling machines in Great Britain, in line with other international jurisdictions, displays a significant association with areas of socio-economic deprivation. The profile of the resident population living in HDMZs mirrors the profile of those most at-risk of experiencing harm from gambling. This spatial pattern has important implications for assessing the relationship between gambling availability and gambling-related harm, and for the future development of policy, harm-prevention and treatment strategies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Commercial gambling has proliferated throughout many countries in the world over the last three decades (Shaffer and Hall 2001). Great Britain, arguably, has one the most accessible gambling markets in the world with provisions for gambling ranging from lottery tickets sold in most local shops, to gambling machines located in a variety of venues, to casinos, bookmakers and online gambling. As opportunities for gambling have multiplied, concerns about the public health impacts associated with this behaviour and the impact on rates of problem and pathological gambling have increased.
As with other forms of addictive behaviors, such as tobacco and alcohol consumption, problems associated with gambling have a social and geographical gradient, with those living in areas of greater deprivation, who are economically inactive and with lower incomes being more likely to experience harm (Orford et al. 2010; Wardle et al. 2011b). This suggests that there is both a social and geographical patterning of gambling-related harm which is likely to be complex and involve both individual factors (composition) and social factors (context), such as access and availability of gambling, and socio-economic and demographic characteristics and circumstances (Pearce et al. 2008). Although considerable research has been conducted on the individual determinants of problem gambling far less is known about contextual influences (Welte et al. 2006).
Increasing recognition of contextual issues has encouraged focus on the interplay between individuals and environment and, in particular, on the relationship between access to gambling opportunities and impact on behaviour (Korn and Shaffer 1999; Pearce et al. 2008; Orford 2010). Welte (2004, 2007) demonstrated that gambling problems were higher among those who lived in close proximity to a casino, whilst examination of machine density in Australia showed that high machine density accounted for 77 % of the variation in gambling expenditure per adult (Storer and Stubbs 2007). Many studies have focused on the relationship between gambling machine availability and player behaviour. Internationally, machines are associated with high rates of at-risk and problem gambling as well as high rates of help-seeking among players (Storer et al. 2009). Research from Australia and Canada has suggested that they are frequently clustered in areas of high socio-economic deprivation and are associated with higher rates of problems among individuals from lower socio-economic groups (Livingstone 2001; Abbott et al. 2004; Wheeler et al. 2006).
In Britain, there has been no systematic evaluation of the distribution of gambling opportunities and their spatial patterning. This is an increasingly glaring omission as changes in the way that gambling venues were approved and licensed were introduced with the Gambling Act 2005. British policy, directed by the Department for Culture, Media and Sport, is now largely based on the principles of consumer choice and market competition, albeit with the stipulation that vulnerable people should be protected from harm (DCMS 2005). Free market principles dominate policy relating to supply for gambling opportunities, with little consideration of how the geographic distribution of the latter may impact upon the prevalence and incidence of problem gambling.
This has lead to increasing debate about the perceived clustering of gambling opportunities—particularly machines—in areas of greatest socio-economic deprivation. Critics have pointed to the changing profile of some local High Streets to argue that there is increasing geographical clustering of machine gambling venues and that this exposes local populations to augmented risk of harm (Light 2007; Orford 2010; Harman 2011). The objective of this study was to contribute to this debate by taking an important first step and mapping the location and density of gambling machines in Great Britain. Put simply, we need to know if and how machines cluster in certain areas before we can examine the impact of this.
Gambling machines are of particular policy interest because of their association with gambling-related harm, a clear social gradient of participation and their availability. This has led to researchers describing their international distribution as based on principles of regressive ‘harm production’ (Livingstone and Adams 2010). Aside from lottery tickets and scratchcards, gambling machines are the most accessible form of land based gambling in Britain, with around 135,000 gambling machines in the market (Gambling Commission 2011). The British Gambling Prevalence Survey 2010 showed that the prevalence of playing gambling machines was significantly higher among those who were unemployed, had low personal income and/or were living in areas of greatest deprivation (Wardle et al. 2011b). As noted in other jurisdictions, a majority of those presenting for treatment for gambling problems are heavily involved in machine play (Wheeler et al. 2006; GamCare 2010).
The aims of this study were to (a) map the location and estimated density of gambling machines in Britain, (b) identify whether geographic areas with higher densities of machines exist and, if so, (c) to explore the socio-economic characteristics of those areas relative to others.
Methods
Identifying the Number of Gambling Machines at Different Venues
There is no central register which records the number of gambling machines present at different venues in Britain. Therefore, data about the location and density of gambling machines were collected in two stages:
-
1.
Data showing the location of all regulated British gambling venues as at December 2010 was obtained from the UK’s Gambling Commission (GC). This database contained full address and postcode information for licenses issued to venues. This includes all bookmakers, bingo clubs, amusement arcades/family entertainment centres and casinos (i.e., venues where machines may be present). The GC does not regulate gambling machines in pubs and restaurants. Therefore, a separate listing of licensed pub/restaurant premises with gambling machines was purchased from a commercial supplier.
Some gambling venues hold more than one license for gambling machines and 165 licenses had no spatial location record. Taking these into account, analysis was based on 29,711 premise locations.
-
2.
Estimates of the number of machines at each venue type were made based on (a) regulatory information about the maximum number of machines allowed per venue, (b) consultation with specific industry sectors and (c) a field validation process. For example, a pub with gambling machines licensed within its alcohol license is allowed a maximum of two machines per premise. Bookmakers are permitted to have four machines per premise and the Association of British Bookmakers confirmed that, space permitting, most use their full allocation.
The sector for which little information was available was amusement arcades, known as Adult Gaming Centres (AGCs). In AGCs, limits on machine numbers applies only to higher-stake machine categories, whereas lower category machines are unlimited in number. A field validation study was conducted by NatCen Social Research to obtain a meaningful estimate of machine numbers for AGCs.
NatCen interviewers visited 65 AGCS to count the number of machines at each. The venues were purposively selected from the GC’s license database. Consultation with the GC suggested that the number of machines per venue was likely to vary based on location. Quotas were set on different AGC types categorised by geographic location. These were urban/central, periphery or smaller urban areas, medium or small towns, seaside resorts and transport hub locations. The number and type of AGCs included in the validation study broadly reflected the distribution of all licensed AGCs in Great Britain. Data from the field validation study were collated and the results used in analysis. Estimates of the average number of machines per venue type are shown in Table 1.Footnote 1
Information from these two stages were combined to provide estimates of the average number of machines in a given location based on venue type (see Wardle et al. 2011a for full details).
Analysis
Visualising Machine Density
The average number of machines per premise license type was assigned to each premise. The average number of machines for each Output Area (OA)Footnote 2 was calculated by aggregating machine number estimates for all venues found within each OA. The average number of machines per person in each OA was also calculated by dividing the average number of machines by the population of the OA using 2001 Census data. Weighted kernel density estimation techniques were used (using ArcGIS spatial analyst tools) to produce continuous data surfaces indicating higher densities of machines per resident head of population.
Identifying Machine Zones and High Density Machine Zones
In order to compare the socio-economic characteristics of areas both with and without gambling machines, a geographic ‘buffer’ zone of 400 m was drawn around each machine gambling venue. There is no recognised standard of the distance from a gambling venue which represents greater or lesser access to gambling. Studies in Australia, Canada and the USA have used various distances with radii ranging from 300 m to 16 km (Wilson et al. 2006; Robitaille and Herjean 2008; Welte and Barnes 2007). Given the more compact and densely populated nature of Great Britain, a distance of 16 km was not judged appropriate. UK Planning Policy Statement 6 states that 300 m between facilities within a town centre represents easy walking distance (ODPM 2005). Furthermore, a 400 m radius was required to be able to include socio-economic data for Lower Super Output AreasFootnote 3 in a nearest-neighbour analysis. Therefore, a radius of 400 m from any venue with a gambling machine was judged to be a reasonable definition of a ‘machine zone’ (MZ). There were 8,861 ‘machine zones’ in total, with many becoming contiguous with neighbouring zones.
Once MZs were identified, the number of machines per zone was calculated by estimating the number of machines at each venue within that zone. These data were used to calculate the average number of machines per hectare within MZs.
There is no standard definition of what constitutes a ‘high-density’ of gambling machines. Plotting the distribution of average number of machines per hectare within MZs showed that one standard deviation from the mean gave an average density of 1 machine per hectare. Using this density threshold, 386 MZs were classified as ‘high-density’ (4.3 % of all MZs). This grouped machine zones into two types: high density machine zones (HDMZs), with an average of 1.9 machines per hectare, and non high density MZs (nhd-MZs) with a density below this threshold, with an average 0.3 machines per hectare.
Socio-Economic Characteristics and Statistical Testing
Once nhd-MZs and HDMZs were identified, headline statistical values were calculated for income (based on Income Domain scores from the Index of Multiple Deprivation, 2007), economic inactivity, occupation group, ethnicity and age (using Census data), based on the OA/Lower-Super OA population-weighted centroids falling within their boundaries.Footnote 4 Where no such centroid fell within an nhd-MZ/HDMZ, it was excluded from analysis, leaving a total of 7,243 MZs. Chi square tests were computed on variable counts within a 5 × 5 matrix, defined by quintiles, of zone density against the various indicators.
Results
Geographic Location of High Density Machine Zones
Unsurprisingly, HDMZs tended to be found in seaside locations: a third of HDMZs were located within one mile of the coastal boundary, reflecting the traditional concentration of amusement arcades in seaside towns. However, HDMZs were also present in urban locations and specifically in periphery and satellite towns to major urban centres. For example, towns like Crawley, Feltham, Luton and Watford around Central London contained HDMZs, though not Central London itself. This pattern was replicated in Manchester, Newcastle, Birmingham, Liverpool and Glasgow, whereby the areas surrounding each city contained some HDMZs but none were evident within the central urban area of the cities themselves. Adjusting estimates to take into account population density did not alter the observed distribution; HDMZs are high density relative to both the geographic space and the resident population in which they are located. HDMZs were also disproportionately located in New Towns. Of the 27 New Towns created by the 1946 New Town Act, 18 contained HDMZs.
Socio-Economic Characteristics of HDMZs
Areas with gambling machines were likely to have a slightly younger population than areas outside machines zones; 27.6 % of the total population in nhd-MZs were aged 16–34 compared with 23.4 % of those living in non-machine areas. This difference was more pronounced when looking at HDMZs where 29.9 % of the population was in this age group (p < 0.01).
This pattern was replicated for most of the socio-economic characteristics considered (see Table 2). Compared with non-machine areas, nhd-MZs had a higher proportion of non-white ethnic groups, a lesser proportion of residents in managerial/professional occupations and a greater percentage of economically inactive residents. When looking at HDMZs, differences were more pronounced. These areas had the highest proportion of economically inactive people (37.0 %), higher percentages of residents in elementary jobs (14.8 %) and, likewise, the lowest proportion of those in managerial/professional occupations (p < 0.01). In England, HDMZs had significantly higher income deprivation scores compared with non-machine areas. In Wales, all machine zones, whether high density or otherwise, had higher income deprivation scores than non-machine areas (p < 0.01).
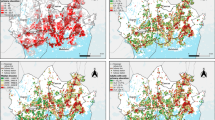
A clear relationship between income deprivation and HDMZs was evident. By and large, HDMZs were located in areas of greatest income deprivation. However, HDMZs tend not to be present in very central urban areas but are more likely to be found in urban fringe or suburban locations. This is evident when looking at Greater London (Fig. 1), with the observed pattern being replicated across Great Britain.

High density machine zones and income deprivation in Greater London (Darker shading means greater income deprivation)
However, these patterns were not universal. Not all areas with the greatest levels of income deprivation had a HDMZ and not all HDMZs were located in the most income deprived areas. Some were situated in areas that may be considered relatively affluent comparative to the surrounding area. See for example the cluster of HDMZs in South West Manchester (Fig. 2).

High density machine zones and income deprivation in Greater Manchester (Darker shading equals greater income deprivation)
Seaside Resorts, New Towns and Income
HDMZs were disproportionately present in both seaside locations and New Towns,Footnote 5 though again not universally. Further investigation was undertaken to explore whether income levels may be associated with this distribution. Seaside resortsFootnote 6 and New Towns were subdivided into two types: those with a HDMZ and those without. A further categorisation was made based on whether each settlement had more than half of its OAs within the lowest 20 % of income areas. These were classified as areas with a ‘high’ percentage of low income areas.
Results showed that 84 % of seaside resorts with a high percentage of low income areas had a HDMZ. Of HDMZs in seaside locations 61 % were in areas with a higher proportion of low income areas. The same pattern was observed for New Towns: 74 % of New Towns with a high percentage of low income areas also had a HDMZ and HDMZs were found disproportionately in this category of New Town (78 %).
Discussion
Understanding the distribution of gambling machines is an important, but sorely neglected, public health issue. International research has shown that a relationship between exposure to gambling—especially machines—and risk of harm exists, although this relationship is complex and may vary according to regulatory environment. Gambling machines are one of the most highly accessible forms of gambling available in Great Britain, and are disproportionately popular among youth and other vulnerable groups, such as those who are unemployed or live in deprived areas (Wardle et al. 2011b). Analysis demonstrated a strong correlation between machine density and socio-economic deprivation and highlighted a specific geographic patterning of distribution. HDMZs had higher income deprivation, more economically inactive residents and a younger population profile. However, this pattern was not universal and HDMZs were also evident in some relatively affluent areas. This suggests that factors other than those related to income deprivation or the socio-demographic profile of residents may be relevant when considering gambling machine distribution. Resident population density, however, was not one of them. A number of machine hotspots had a disproportionately high number of machines per head of resident population. Therefore it does not appear that machines are simply clustering proportionately to the size of the resident population; other factors must be driving this distribution.
As expected, seaside resorts had high densities of gambling machines but somewhat unexpectedly, so did New Towns and suburban centres to major urban areas. Income deprivation was clearly correlated with this distribution. However, taking a more relational approach to understand this spatial patterning may also be fruitful. Our analysis necessarily took a static approach when analysing the relationship between place (machine zones) and people (residents within machine zones). However, we recognise that the relationship between place and people is both relational and dynamic through space and time (Cummins et al. 2007; Rainham et al. 2010). Given the centralised location of gambling venues in business, recreational and retail areas, these dynamic relations are even more pertinent as different groups of people populate these spaces at different times. Going forward, it will be important to consider how factors such as local culture and heritage, structure and infrastructure or differing uses of space by population sub-groups combine to influence the distribution of gambling venues. For example, pre-existing culture, heritage and tourism are likely to provide explanatory factors for the distribution of HDMZs in seaside locations, though they do not comprehensively explain why some seaside resorts have high densities and others do not. It is likely that local policies and priorities (for example, those related to regeneration), economic diversification and local norms may provide additional explanations, along with the socio-demographic and economic characteristics of the local area. With regard to New Towns, these areas are likely to be focal centres for work, entertainment and recreation meaning that these spaces are used by a variety of people at different points. Greater understanding is needed about who, out of this broader population base, is actually using the gambling provisions. In short, the impact of increased gambling machine availability may extend far beyond the local resident population living within 400 m from a venue and reach to transient populations who use the same spaces for work and recreation. These patterns need to be investigated and understood at a local level.
Whilst greater understanding is needed about factors governing distribution, it is clear that these factors are converging to produce areas where the local resident population is disproportionately exposed to gambling machines and that the residents of these areas tend to have poorer socio-economic outcomes. It is broadly accepted that place and context can influence human behaviour and that geographic and other inequalities can propagate the risk of experiencing adverse health outcomes. There is a significant literature on the associations between lower socio-economic status, neighborhood deprivation and the concentration of alcohol, tobacco and fast food outlets (Scribner et al. 2000; Chuang et al. 2005; Macdonald et al. 2006; Ellaway et al. 2010). This current research suggests that gambling opportunities display similar patterning and, related to this, the experience of gambling-related harm—like obesity and high alcohol consumption—may have a geographical aspect. Such a relationship encourages that a more holistic perspective be applied to understanding problem gambling, one which includes wider policy and regulatory environments alongside the characteristics and behaviour of individual players.
To date, such a broad perspective has received relatively little attention, in the UK at least, with policy focusing on individual and psycho-social parameters of consumer choice and responsibility. Only recently has the role of regulatory and legislative changes received broader attention in relation to its (potential) impact upon the unequal distribution of gambling opportunities. As Wheeler et al. (2006) note, in other areas of ‘addictive’ health behaviours policy often trails research and this appears to be the case with gambling. Crucially, whilst there is widespread acceptance of problem gambling as a psychiatric disorder and a recognition its prevalence should be minimised, a public health based approach to policy in Britain has not been adopted. Finally, further understanding the geo-spatial patterning of gambling opportunities and the place-specific drivers of this distribution has a highly practical application. This relates to the potential development of geographically-targeted interventions relating to both prevention and education initiatives and the provision of treatment services, facilitating the focus of scarce resources where they are needed most.
Limitations
There are a number of issues to consider when reviewing this study. Firstly, machine densities were calculated using average weighted estimates per venue type as no register which records the number of machines at each venue exists. For certain venue types (pubs, bookmakers) we can be confident that the average estimate is a close reflection of reality based on confirmation with the industry sector and statutory provisions. For some venues, specifically Amusement Arcades there will be greater variation because the number of machines permissible was linked to the venue size. A field validation study was conducted to determine what estimates should be used in analysis. However, it is possible that there is some error around this estimate, which should be borne in mind. For example, the field validation study showed that the mean number of machines in per AGC was 38.2, with a standard deviation of 26 meaning there was a large variation around this figure. However, much of this variance was accounted for by large seaside AGCs which tend to have more floor space and therefore more machines. Excluding seaside AGCs gives a mean of 34.1 machines per AGC and standard deviation of 13.8. We were not able to determine from the venue data available to us which venues had greater floor space and therefore more machines and which had smaller floor space and therefore fewer machines. As such, we used the mean figure in our analysis. There may be a few specific examples of areas being incorrectly identified as high density because of this. However, examination of our methods and use of different thresholds does not suggest that this alters the overall patterns observed. Estimates of the number of machines per venue are one source of error that might be evident with our approach. The other source of error relates to geocoding of venue postcodes to Output Areas. We are confident that there is limited error relating to this as gambling venues are generally found in built-up areas where the spatial extent of a unit postcode is small (it will often summarise fewer than 5 buildings with multiple occupation) and its centroid will therefore represent the ground truth location of a building to a fine degree of accuracy. Therefore, the main source of likely error relates to our estimates of the number of machines per venue, though data were checked, triangulated against multiple sources and, in the case of AGCs, subject to field validation to improve accuracy. Secondly, the definition of what constitutes a high density machine zone is an arbitrary threshold; there is no standard definition. Our threshold was determined based on examination of the distribution of the average number of machines per area. It is possible that using a different threshold may give slightly different results to those reported here. Finally, around 1,600 MZs were excluded from analysis because no population-weighted LSOA/OAs fell within their boundary. Inspection of those omitted does not suggest that the overall relationships would have been different had these MZs been included, though the specific estimates may vary.
Notes
Full technical details about how the number of machines per venue were estimate are given in Wardle et al. 2011a. Alternatively, please contact the authors for a copy or further discussion of methods.
Output Areas are continuous area units covering the UK, built for and used to represent census-based and other demographic statistics. They are demographically designed to have similar population sizes and be as socially homogenous as possible and they allow for finer resolution of data analysis. In 2001 the minimum threshold population was 100.
Lower Super Output Areas (LSOAs) are akin to Output Areas (OAs). They are built from blocks of Output Areas and have a mean population of 1,500.
Population-weighted OA centroids are point locations of OA situated towards where the majority of people within that area live `on the ground'.
Defined as the 27 British towns created under the New Towns Act 1946 or rapidly expanded under its provisions or the replacement 1964 Act.
This used the 74 largest resorts in England by population based on Department for Communities and Local Government benchmarking study; no equivalent listing exists for Wales or Scotland.
References
Abbott, M., Volberg, R., Bellringer, M., & Reith, G. (2004). A review of research on aspects of problem gambling: Final report. Auckland: AUT University.
Chuang, Y. C., Cubbin, C., Ahn, D., Winkleby, M. A. (2005). Effects of neighbourhood socioeconomic status and convenience store concentration on individual level smoking. Journal of Epidemiology and Community Health, doi:10.1136/jech.2004.029041.
Cummins, S., Curtis, S., Diez-Roux, A. V., & Macintyre, S. (2007). Understanding and representing ‘place’ in health research: A relational approach. Social Science and Medicine, 65(9), 1825–1838.
Department for Culture, Media and Sport. (2005). Gambling Act: 2005. London.
Ellaway, A., Macdonald, L., Forsythe, A., & Macintyre, S. (2010). The socio-spatial distribution of alcohol outlets in Glasgow city. Health & Place, 16(1), 167–172.
Gambling Commission. Industry Statistics 2011. Birmingham: Gambling Commission.
GamCare. (2010). Statistics 2009/2010. http://www.gamcare.org.uk/publications.php. Accessed 27 March 2012.
Harman, H. (2011). The problem of betting shops blighting our high street. http://www.harrietharman.org/uploads/d2535bc1-c54e-6114-a910-cce7a3eff966.pdf. Accessed 25 Jan 2012.
Korn, D. A., & Shaffer, H. J. (1999). Gambling and the health of the public: Adopting a public health perspective. Journal of Gambling Studies, 15(4), 289–365.
Light, R. (2007). The Gambling Act 2005: Regulatory containment and market control: The Gambling Act 2005. Modern Law Review, 70(4), 626–653.
Livingstone, C. (2001). The social economy of Poker Machine Gambling in Victoria. International Gambling Studies, 1(1), 45–65.
Livingstone, C., & Adams, A. (2010). Harm promotion: Observations on the symbiosis between government and private industries in Australasia for the development of highly accessible gambling markets. Addiction, 106(1), 3–8.
Macdonald, L., Cummins, S., & Macintyre, S. (2006). Neighbourhood fast food environments and area deprivation—substitution or concentration? Appetite, 49(1), 251–254.
Office of the Deputy Prime Minister. (2005). Planning policy statement 6: Planning for town centres. London: Annex A.
Orford, J. (2010). An unsafe bet: the dangerous rise of gambling and the debate we should be having. Oxford: Wiley.
Orford, J., Wardle, H., Griffiths, M. D., Sproston, K., & Erens, B. (2010). The role of social factors in gambling: Evidence from the 2007 British Gambling Prevalence Survey. Community, Work and Family, 13(3), 257–271.
Pearce, J., Mason, K., Hiscock, R., & Day, P. (2008). A national study of neighbourhood access to gambling opportunities and individual gambling behaviour. Journal of Epidemiology and Community Health, 62, 862–868.
Rainham, D., McDowell, I., Krewshi, D., & Sawada, M. (2010). Conceptualising the healthscape: Contributions of time geography, location technologies and spatial ecology to place and health research. Social Science and Medicine, 70(5), 668–676.
Robitaille, E., & Herjean, P. (2008). An analysis of the accessibility of video lottery terminals: The case on Montreal. International Journal of Health Geographics. doi:10.1186/1476-072X-7-2.
Scribner, R. A., Cohen, D. A., & Fisher, W. (2000). Evidence of a structural effect for alcohol outlet density: A multilevel analysis. Alcohol Clinical Experimental Research, 24(2), 188–195.
Shaffer, H., & Hall, M. N. (2001). Updating and refining prevalence estimates of disordered gambling behavior in the US and Canada. Canadian Journal of Public Health, 92, 168–172.
Storer, J., Abbott, M., & Stubbs, J. (2009). Access or adaptation? A meta analysis of surveys of problem gambling prevalence is Australia and New Zealand with respect to the concentration of electronic gaming machines. International Gambling Studies, 9(3), 225–244.
Storer, J., & Stubbs, J. (2007). Submission to statutory review of the gaming machines Act 2001. Sydney.
Wardle, H., Keily, R., Thurstain-Goodwin, M., Astbury, G. (2011a). Machines Research 1: Mapping the social and economic characteristics of high density machine locations. Responsible Gambling Fund (Available from authors on request).
Wardle, H., Moody, A., Spence, S., Orford, J., Volberg, R., Griffiths, M., et al. (2011b). British gambling prevalence survey 2010. London: The Stationery Office.
Welte, J. W. (2004). The relationship of ecological and geographic factors to gambling behaviour and pathology. Journal of Gambling Studies, 20(4), 405.
Welte, J. W., & Barnes, G. M. (2007). Type of gambling and availability as risk factors for problem gambling: A tobit regression analysis by age and gender. International Gambling Studies, 7(2), 183–198.
Welte, J. W., Wieczoeck, W. F., Barnes, G. M., & Tidwell, M. C. O. (2006). Multiple risk factors for frequent and problem gambling: Individual, social and ecological. Journal of Applied Social Psychology, 36, 1548–1568.
Wheeler, B. W., Rigby, J., & Huriwai, T. (2006). Pokies and poverty: Problem gambling risk factor geography in New Zealand. Health and Place, 12(1), 86–96.
Wilson, D. H., Derevensky, J., Gilliland, J., Gupta, R., & Ross, N. (2006). Video lottery terminal access and gambling among high school students in Montréal. Canadian Journal of Public Health, 97(3), 202–206.
Acknowledgments
We wish to acknowledge the support of the Responsible Gambling Fund who sponsored a program of research into gambling machines in Britain, of which the work reported in this paper was part.
Conflict of interest
Heather Wardle and NatCen has received funding for a number of research projects from the Responsible Gambling Fund, a charitable body who funds its research programme based on donations from the gambling industry. NatCen has also undertaken work for an online gambling company to help them improve their social responsibility practice. Ruth Keily and Gaynor Astbury have received funding from the Responsible Gambling Fund as well as other commercial clients not related to the gambling industry. Gerda Reith has received joint funding from the Responsible Gambling Fund and the ESRC. She is also a member of the Responsible Gambling Strategy Board which advises the Responsible Gambling Fund about research issues.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wardle, H., Keily, R., Astbury, G. et al. ‘Risky Places?’: Mapping Gambling Machine Density and Socio-Economic Deprivation. J Gambl Stud 30, 201–212 (2014). https://doi.org/10.1007/s10899-012-9349-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-012-9349-2