
Abstract
The purpose of this study was to examine the psychometric properties of the Chinese 9-item Problem Gambling Severity Index (PGSI) derived from the 31-item Canadian Problem Gambling Index (CPGI) originally developed by Ferris and Wynne (2001). Exploratory factor analysis (EFA; n = 386; Group A data) and confirmatory factor analysis (CFA; n = 387; Group B data) on the Chinese student and community data (Mean age = 25.36 years) showed that a unifactorial model fitted the data with good reliability score (Cronbach’s alpha = 0.77). The concurrent validity of the PGSI-C was good in terms of the Chinese data matching the expected correlation between PGSI-C and other variables or scales such as SOGS, gambling frequency, gambling urge, gambling cognitions, depression, anxiety, and stress. The scale also reported good discriminant and predictive validity. In sum, the PGSI-C has good psychometric properties and can be used among Chinese communities to identify at-risk problem gamblers. Implications and suggestions for future research are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Gambling is commonly recognised as an act of betting a sum of money on the outcome of an event or game that is largely determined by chance (Bolen and Boyd 1968). There are many forms of gambling, most commonly pari-mutuels (dog and horse tracks, Jai Alai, off-track-betting parlours), casinos (slot machines, table games), lotteries, bookmaking, card rooms, bingo and the stock market (Illinois Institute for Addiction Recovery 2007). When gamblers win or lose, a range of readily perceptible cognitions, emotions, and behaviours are evoked. In turn, they drive a vicious cycle of excessive gambling with detrimental consequences such as financial debt, work and health issues, and strained relationships (Loo et al. 2008). At present, gambling is legal in many countries and readily accessible to individuals that meet the minimum requirement for age limit, which differs according to state or country. The availability of gambling venues perpetuates the frequency and severity of gambling-related social issues and has raised concerns among practitioners and governmental authorities. Hence, accurately defining and measuring problem gambling are important steps in gaining understanding of this addictive behaviour.
To date, most researchers have concurred that the term problem gambling (PG) refers to gambling behaviour that is severe enough to create negative outcomes for the problem gambler, immediate family, and social networks (Brooker et al. 2009; Raylu and Oei 2002). Similarly, in this study, problem gambling will be used in a broader sense to define the situation where an individual is experiencing gambling problems that causes disruption to the individual’s functioning that may extend to affect family members and social networks (Lesieur and Blume 1987). The term pathological gambling will be used to define individuals who meet the diagnostic criteria in the Diagnostic and Statistical Manual, Fourth Edition, Text Revision (DSM-IV-TR; American Psychiatric Association 2000). Thus, pathological gambling is more serious or extreme in comparison to PG. For the purpose of this study, gambling problems are conceptualized on a latent continuum of duration and severity.
Building up from these conceptual frameworks, several evidence-based instruments such as the South Oaks Gambling Screen (Lesieur and Blume 1987), DSM criteria (American Psychiatric Association 2000), Canadian Problem Gambling Index (Ferris and Wynne 2001), and Victorian Gambling Screen (Wenzel et al. 2004) have been developed to measure problem and pathological gambling. These scales report good psychometric properties when used among Western populations of various age ranges and are valuable tools for clinicians to determine an individual’s PG severity. A comparative evaluation on PG measurements suggested that the Canadian Problem Gambling Index (CPGI) demonstrated the most valid and reliable psychometric properties to measure PG prevalence among Western population (McMillen and Wenzel 2006). This was also confirmed by another Australian national review on PG measurements and related issues (Neal et al. 2004). The CPGI has been used effectively in community health settings, student samples, and also among diverse populations (Arthur et al. 2008; Young and Stevens 2008). The CPGI is also a preferred scale in Canada, as well as in Australian community prevalence research in Queensland (Queensland Treasury 2006), Tasmania (Roy Morgan Research 2006), and Victoria (McMillen et al. 2004).
The predecessors of CPGI such as SOGS and DSM-IV have been used widely in gambling research and validated among various population groups from countries such as Hong Kong and Singapore (Arthur et al. 2008; Tang et al. 2007, 2010). However, there has been substantial evidence that criticises the use of SOGS in community prevalence studies as SOGS was originally developed for clinical use and it tended to overestimate PG prevalence (McMillen and Wenzel 2006; Young and Stevens 2008). Questions arose concerning the suitability of SOGS in different ethnic groups, particularly with regards to items on money problems (Stinchfield 2002).
The CPGI, on the contrary, was originally developed to assess the prevalence of PG among general population research and defined PG as a less severe albeit destructive gambling pattern that may or may not include pathological gambling behaviour (Ferris and Wynne 2001). As a whole the CPGI consists of 31 items (including demographics) measuring gambling involvement, PG assessment, and PG correlates (Ferris and Wynne 2001). However, only nine items are scored, which is collectively named the Problem Gambling Severity Index (PGSI) under the CPGI. Although many studies uses the term CPGI synonymously with PGSI; for clarity reasons, PGSI will be used in this study to identify the scored 9-items scale. Factor analysis of the 9-items of PGSI on a Canadian sample resulted in a unifactorial model (Brooker et al. 2009). For example, items in the PGSI included “Have you bet more than you could really afford to lose?” and “Have you felt that you might have a problem with gambling?” The parsimonious factor replicated the unifactorial model of PGSI in the original Canadian report that used a different dataset, lending support to the construct validity of PGSI (Ferris and Wynne 2001).
Reflecting from past research, there are many social costs and harmful effects that occur due to PG that affects both problem gamblers and their significant others (Raylu and Oei 2002). It has also been argued that there are fundamental differences in the development of PG, perpetuation of gambling problems, and help-seeking behaviour between individuals from the West and Chinese individuals (Loo et al. 2008; Raylu and Oei 2004). These differences can be attributed to historical, geological, political, cultural, and social environments in which the individual lives in. As the characteristics of Chinese problem gamblers are in some ways different to those of gamblers in Western societies (Vong 2007), they must be taken into consideration when conducting assessments, planning treatments, and developing support services to help them.
Chinese individuals were selected as the focus of this study for various reasons. In 1998 there were approximately 1.3 billion Chinese worldwide, and while the vast majority lived in mainland China, 37 million lived elsewhere (Parker et al. 2001). Representing 22% of the planet’s population, Chinese people are the largest ethnic group in the world (Tseng et al. 1995). It is perhaps one of the largest groups of migrants around the world, with many individuals being of Chinese descent. It is also not uncommon to encounter anecdotal media coverage on pathological gambling among Chinese individuals with speculations of prostitution and drug-dealing to repay debts, and parental neglect of young children stemming from gambling addiction (Blaszczynski et al. 1998). Moreover, empirical evidence of PG among the Chinese does suggest that gambling is a popular recreational activity and prevalence rates are higher in this population in comparison to Western populations (Blaszczynski et al. 1998; Chen et al. 1993; Loo et al. 2008; Victorian Casino and Gaming Authority 2000). Gambling remains popular among Chinese Diaspora due to the fact that it is an acceptable form of social activity in the community (Hobson 1995; Lai 2006; Raylu and Oei 2004). In fact, social gambling is expressed as a form of entertainment, often occurring during festivities such as Chinese New Year, birthdays, or weddings.
Hence, it is arguably important to examine the validity of using the same assessment scale to measure PG across different populations. To date, scale validation has not been done on individuals from other ethnicity using translated versions of PGSI. Particularly, psychometric analysis has yet to be conducted on Chinese individuals using Chinese-translated version of PGSI. In the current study, the aim is to examine the factor structure of the Chinese-translated version of PGSI (i.e., PGSI-C) and to further investigate its validity and reliability among Chinese community and student sample. The evaluation of the psychometric properties of PGSI-C will extend our understanding of its application and suitability in Chinese populations.
Method
Participants
The participants consisted of 801 Chinese participants from Taiwan (i.e., Taiwanese Chinese). All 801 participants can read and write in Chinese language (i.e., Mandarin). There were 396 males and 360 females (45 missing data). The mean age was 25.36 years (SD = 10.25) with an age range of 18 to 74 years. In relation to employment status, 69.50% of participants were students; while 20.10% were employed full-time and 5.10% were employed part-time. The remainder participants were either job hunting (1.70%), under disability pension (2.50%), or retired (1.10%).
Measures
As part of a larger project, the materials included a demographics form and a set of self-report questionnaires. All measures without existing validated Chinese versions were translated into Chinese from English and back-translated (i.e., reverse translation) again to check for consistency and face validity. A bilingual psychologist and graduate student who underwent both Western and Chinese education completed the translations. The scales were also checked by two bilingual clinical psychology PhD candidates who were blind to the study to ensure accuracy of translation. Pilot tests were conducted on 10 university students to verify the semantic integrity of each item and to ensure ease of understanding. The preceding steps were then repeated for highlighted items after pilot testing. Discrepancies between the versions were thoroughly discussed and resolved until a translated version was found to have semantic equivalence.
The Chinese validated version of the Depression, Anxiety, and Stress Scale (DASS; Norton 2007) will be utilised in this study as these variables have been found to be positively related to PG (Petry 2005a). SOGS (Lesieur and Blume 1987) and gambling frequency will be also be measured. The Chinese version of Gambling Urge Scale (GUS-C; Oei et al. 2007b) and Gambling Related Cognitions Scale (GRCS-C; Oei et al. 2007a) will also be used as a measure of gambling urge and erroneous cognitions, respectively.
The Problem Gambling Severity Index (PGSI; Ferris and Wynne 2001)
The PGSI is a 9-item measure of PG, derived from the 31-item CPGI. Five items of PGSI originated from SOGS, 2 items from DSM-IV, and 2 items were developed for the PGSI. It uses a 4-point rating scale ranging from “0—Never” to “3—Almost always.” Items are totalled and the total of 0 identifies a non-gambler, 1–2 identifies a low-risk gambler, 3–7 identifies a moderate-risk gambler, and 8 or more identifies a problem gambler. The Cronbach’s alpha was good, at 0.84, with a test-retest reliability of 0.78 (Ferris and Wynne 2001). The PGSI has good criterion-related validity because it matches up fairly well with the DSM-IV and the SOGS, correlating at 0.83 with both measures (Ferris and Wynne 2001).
South Oaks Gambling Screen (SOGS; Lesieur and Blume 1987)
South Oaks Gambling Screen (SOGS; Lesieur and Blume 1987) is the most commonly used 20-item self-administered instrument for assessing “pathological gambling,” which was developed based on DSM-III criteria. Cronbach’s alpha was 0.97 and the test-retest reliability was 0.71 (Lesieur and Blume 1987). This 20-item scale uses yes/no responses and scores ranges from 0 to 20. A score of 0 indicates no problem gambling, 1–4 indicates at risk gambling behaviour or possible problematic gambling, and a score of 5 or more indicates problem gambling. In Chinese samples, the Cronbach’s alpha was 0.75 with good construct validity (Blaszczynski et al. 1998).
Gambling Frequency
The gambling frequency questions consisted of four items measuring frequency of gambling in (1) gaming machines, (2) table games, (3) animals such as horse racing, and (4) other forms of gambling such as bingo, lottery, and sports betting. Responses were measured on a 5-point scale ranging from “1—Never,” “2—monthly or less,” “3—2 to 4 times a month,” “4—2 to 3 times per week,” to “5—4 or more times per week.”
The Gambling Related Cognitions Scale (GRCS; Oei et al. 2007a)
The GRCS is a 23-item scale measuring erroneous gambling cognitions and included items such as “I have some control over predicting my gambling wins.” The responses were measured on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree) with higher scores indicating more cognitive distortions held by the individual. The Chinese version of the GRCS reported a Cronbach’s alpha 0.95 and ranged from 0.83 to 0.89 for the five factors. The GRCS-C also reported good concurrent, predictive, and discriminant validities.
The Gambling Urge Scale (GUS; Oei et al. 2007b)
The 6-item questionnaire measured gambling urges and included items such as “All I want to do now is to gamble.” Participants responded on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree) with higher scores indicating a stronger urge to gamble. The Cronbach’s alpha for the Chinese version was reported to be 0.87 and has adequate concurrent, predictive, and criterion validities.
Depression, Anxiety, and Stress Scale (DASS; Lovibond and Lovibond 1995)
This 21-item scale (rated on a 4-point scale ranging from 0 “did not apply to me at all” to 3 “applied to me very much or most of the time”) assesses symptoms of depression, anxiety and stress. The scale showed a high internal consistency (α = 0.94, 0.87 and 0.91 for the subscales of depression, anxiety and stress respectively) (Antony et al. 1998). In a Chinese sample, the Cronbach’s alpha for the three subscales were also high (α depression = .85; α anxiety = .87; α stress = .82) and the Chinese version showed good criterion and predictive validities (Oei et al. 2008).
Procedure
As a part of a larger study, university participants from Taiwan were recruited from universities in Southern Taiwan and Northern Taiwan. Ethical clearances were provided by the respective organisational ethics committee and all procedures were carried out accordingly. The university participants were recruited from these departments: (1) Nursing, (2) General Education, (3) Mechanical Engineering, (4) Electrical Engineering, (5) Recreation Administration, (6) Business Administration, and (7) Medicine. The community participants were recruited from Southern and Northern Taiwan by word-of mouth and community contacts with companies. Voluntary participation was followed by an introduction to the research study, explanation on informed consent, and freedom to withdraw participation. No personal identification information was requested and privacy was assured. Paper and pencil questionnaires were administered individually and participants were thanked and debriefed upon completion. All participants were reimbursed with TWD 100.00 (i.e., approximately AUD 4.00) and average time taken to complete the questionnaire was 30 min.
Results
Preliminary Data Analysis
All data cleaning and descriptive analyses were conducted using SPSS version 17. Data cleaning included checking accuracy of data entry, missing values, and assumptions of multivariate analysis. Using a z score larger than 3.29 criterion (P < 0.001), 16 univariate outliers were identified and removed from analyses (Tabachnick and Fidell 2007). Using a P < 0.001 criterion for Mahalanobis distance, 12 multivariate outliers were identified and removed from further analyses. Mean substitution was used to handle missing data for all variables, which had fewer than 5% of missing items. Visual screening of the histogram and statistical tests indicated that there was some univariate kurtosis and skewness. Data was positively skewed and hence, logarithm transformation was performed (Tabachnick and Fidell 2007). All analyses were conducted with both non-transformed and transformed data—as no substantive differences were found only the non-transformed results are reported.
Before conducting Exploratory Factor Analysis (EFA), approximately 50% of the total sample was randomly selected for the analysis using SPSS select cases (split-half) option (Group A; n = 386). The remaining 50% of the sample was reserved for the Confirmatory Factor Analysis—CFA (Group B; n = 387). Analyses revealed that the two samples did not differ significantly from one another in gender, age, employment status, depression, anxiety, stress, gambling urge, gambling cognitions, and problem gambling. Using the CPGI cut-offs (Ferris and Wynne 2001), 42.7% of participants were classified as non-gamblers, 21.1% were low-risk gamblers, 27.2% were moderate-risk gamblers, and 9% were problem gamblers.
Differences in Problem Gambling and Gambling Correlates Between Student and Community Sample
Multivariate Analysis of Variance (MANOVA) was conducted to assess mean differences in the PG and correlates between students and community sample. As shown in Table 1, significant differences between the two groups were evident in three of the assessed variable: DASS-depression, DASS-anxiety, and DASS-stress. Differences between groups were not evident in the gambling-related measures. Students scored higher in depression, anxiety, and stress as compared to community participants.
Exploratory Factor Analysis (EFA) of The Chinese Version of TRS with Group A Data
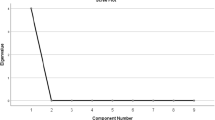
Principal components extraction (PCA) was used prior to principal axis factoring (PAF) to estimate number of factors and factorability of the correlation matrices. PAF was chosen for EFA because it conforms to the factor analytic model where common variance is analysed with unique and error variance removed; thus, maximizing the variance extracted (Tabachnick and Fidell 2007). The Kaiser-Meyer-Olkin measure of sampling adequacy indicated that the sample was factorable (KMO = 0.801). Bartlett’s test of Sphericity was 797.05 (P < .0001) and the diagonal values of the anti-image correlation matrix indicated that all correlations were above the recommended 0.5 (Brace et al. 2009), suggesting that the correlation is not an identity matrix. The factor correlation matrix indicated the items are interrelated, verifying that oblique rotation is more appropriate than orthogonal rotation. Among other methods of oblique rotation, the direct oblimin rotation is the most recommended method (Kline 1994). The initial criteria utilised to retain substantive factors included (a) eigenvalues over 1 and examination of the scree plot, (b) loading of at least 0.40 on one factor (i.e., 20% variance overlap between variable and factor), (c) no factors with fewer than three items, and (d) conceptual consistency and meaningfulness with other items on the factors.
An examination of the scree plot and the initial pattern matrix (extraction of initial eigenvalues greater than 1) revealed that a 1-factor solution fits the data. All items loaded on this factor and confirm the unifactorial solution. Therefore, analyses were executed again using PAF. The final 1-factor solution accounted for 37.51% of extracted variance (eigenvalue = 3.40).
Confirmatory Factor Analysis of the Chinese Version of TRS
A series of confirmatory factor analysis (CFA) via AMOS 17.0 were conducted on the Chinese data (Group B sample; n = 387) to determine the model that best fit the data. The measures of model fit used to evaluate how well the observed data fit the proposed model were:
-
(a)
Chi-square statistics (non-significant χ 2 is desired but this test is sensitive to sample size and violations of normality (Blunch 2008); hence, other fit indices will be used also)
-
(b)
Chi-square/degrees of freedom (df) value being less than 4, indicating good fit (Field 2000)
-
(c)
Comparative fit index or CFI (>0.90 indicating good fit)
-
(d)
The goodness-of-fit index or GFI (>0.90 indicating good fit)
-
(e)
The root mean square error of approximation or RMSEA (0.08 indicating reasonable error of approximation)
First, a CFA was conducted to assess whether the 1-factor structure of PGSI obtained in the Canadian sample (i.e., Brooker et al. 2009) should be retained (Model 1). This structure is the same as the results obtained in the EFA conducted in the current study. All nine items loaded on a single factor. Initially, CFA results indicated that all of the fit indices were less than acceptable, χ 2 (27) = 171.55, P < .001; χ2 /df = 6.35; CFI = 0.81; GFI = 0.91; and RMSEA = 0.12 (see Table 2 for model comparisons). However, modification indices suggested freeing covariance between eight error terms. Conceptually valid covariance was added between items 1 and 2, items 2 and 3, items 3 and 4; and items 5 and 8. In other words, these items were allowed to co-vary in Model 2. A subsequent model (i.e., Model 2) freeing these four paths were found to have a better fit than the constrained model. Although the chi-square (χ 2) value for overall model fit was significant suggesting a lack of fit between the hypothesised model and the data; due to the sensitivity of χ 2 in large samples, other fit indices were assessed (Kline 1994). Model fit indices were in the acceptable range, χ 2 (23) = 80.14, P < .001; χ2 /df = 3.49; CFI = 0.92; GFI = 0.96; and RMSEA = 0.08 (see Table 2). Chi-square difference tests showed that the overall model fit was comparably better for the non-constrained model (Model 2) than the constrained model (Model 1), (Δχ 2 (1) = 91.41, P < .001). Given the significant improvement in overall fit, the model allowing the covariances was considered the acceptable model. The factor structure for PGSI-C is shown in Fig. 1.

Confirmatory factor analysis (CFA) of PGSI-C based on the Chinese sample
Gender Differences
Results of an independent samples t-test revealed that there was a significant gender difference in the PGSI-C total score, t = 3.40, df = 724, P = 0.001. Males (M = 2.61, SD = 3.26) reported higher PGSI-C score than females (M = 1.86, SD = 2.70). The mean difference between genders was 0.75 and the 95% confidence interval for the estimated population mean difference is between 0.31 and 1.18. There was a medium effect size (Cohen’s d = 0.25).
Reliability Analysis and Concurrent Validity for the PGSI-C Factor Structure
The Cronbach’s alpha of the 9-item PGSI-C was high (α = 0.77). Table 3 lists: (1) The Pearson correlations between TRS-C and the concurrent validity indicators, and (2) The coefficient of determination referred to as R squared or the proportion of variance shared by two variables; which are both measures of effect size. Pearson correlation values of ±0.1 represent a small effect, ±0.3 represent a medium effect, and ±0.5 is a large effect (Field 2009). The total score of PGSI-C were significantly positively correlated with other measures of PG, namely SOGS (large effect size) and gambling frequency (medium effect size). Significantly positive correlations were also evident between PGSI-C and gambling urge (small effect size), gambling-related cognitions (medium effect size), depression (small effect size), anxiety (small effect size), and stress (small effect size).
Discriminant Validity of PGSI-C
Discriminant analysis was performed to examine whether PGSI-C discriminated between non-problem gamblers and possible problem gamblers. Based on SOGS scores and cut-offs consistent with past research (Oei et al. 2007a; Rosenthal 2003), participants were divided into Group C (SOGS total = 0, N = 314) and Group D (SOGS total = 4 or above, N = 116). The discriminant analysis used SOGS grouping as the dependant variable (DV), and PGSI-C, age, and gender as the predictor variable (IVs). Age and gender were controlled for in the analysis due to the significant difference found in these variables in past research (e.g., Clarke et al. 2006). Univariate ANOVAs showed that non-problem gamblers and possible problem gamblers differed significantly on age and PGSI-C, but not gender. However, a single discriminant function was calculated and the value of this function was significantly different for both groups (Wilk’s Lambda = 0.60, χ 2 = 197.68, df = 3, P < 0.001). The correlations between predictor variables and the discriminant function suggested that PGSI-C is an excellent predictor of PG suggesting that individuals high on PGSI-C scored higher on SOGS (R = 0.99). Overall, the discriminant function successfully predicted outcome for 83.7% of cases, with accurate predictions being made for 91% of the participants who are non-problem gamblers and 63.6% of the participants who are possible problem gamblers.
Predictive Validity of PGSI-C
Multiple regression analyses were conducted to investigate the predictive validity of PGSI-C (i.e., how well PGSI-C predicts PG). Similarly, age and gender were controlled for in the analysis due to the significant difference found in these variables in analyses reported above. Hierarchical multiple regression analysis was completed with SOGS as the DV, and both age and gender (Step 1) and the PGSI-C total (Step 2) as the IV. The model explained 28.1% of the variance (Adjusted R 2 = 0.281, P < 0.001) with approximately 1.6% accounted for by both age and gender, and 26.5% accounted for by PGSI-C. Participants who scored higher on SOGS are more likely to score higher on PGSI-C (see Table 4).
Discussion
The current study examined the psychometric properties of the Chinese translated version of PGSI (i.e., PGSI-C). Consistent with past evaluations of the original version of PGSI (Brooker et al. 2009; Ferris and Wynne 2001), the results reported here provided support for the unifactorial structure of PGSI. The PGSI-C has the same factor structure as the English version of PGSI. Findings from this study also suggest that the PGSI-C has good reliability and validity in measuring PG among the Chinese. The results showed significant positive correlations with SOGS, gambling frequency, gambling urge, gambling-related cognitions, depression, anxiety, and stress—all of which indicated good concurrent validity. The PGSI-C reported good reliability (Cronbach’s alpha) for the total score. Differences between student and community sample were not evident in the gambling-related measures. However, differences were evidenced in DASS. Students scored higher in depression, anxiety, and stress as compared to community participants. There was a significant gender difference with males reporting higher PGSI-C score than females. This finding is consistent with previous studies on Chinese communities where males reported higher PG rates as compared to females (Blaszczynski et al. 1998; Raylu and Oei 2004).
Consistent with past research on PG (Lesieur and Blume 1987; Oei et al. 2007a, b), there were positive correlations between PGSI-C and all gambling-related measures (i.e., SOGS, gambling frequency, gambling urge, and gambling cognitions). It is important to note that with the exception of SOGS that evidenced a large effect size, the gambling-related measures showed small to medium effect sizes. Furthermore, examination of the validity analyses showed that there were significant positive correlations (albeit, small effect sizes) between PGSI-C with depression, anxiety, and stress; which are consistent with past research on PG (Petry 2005a). These results should be interpreted with caution as small effect sizes in a smaller sample size may yield different results. Future research could also benefit from a replication with clinical samples.
Results obtained from the discriminant analysis revealed that the PGSI-C can differentiate between non-problem gamblers and possible problem gamblers. Total scores of PGSI-C in the two groups of participants were significantly different suggesting that problem gamblers reported higher PGSI-C score. The PGSI-C have been found to have excellent predictive validity, as the multiple regression analyses showed that an individual’s score on PGSI-C can significantly predict SOGS score. Higher PGSI-C predicted higher SOGS score. These findings provides support for the notion that PGSI-C can discriminate and predict the occurrence of PG in the community (Brooker et al. 2009).
All findings in this study should be interpreted in light of the limitations of this study. The participants were recruited using convenient sampling method as opposed to random sampling (e.g., using census data) where every member of the population has an equal opportunity of being selected. For obvious reasons, such research will require national collaborative effort and significant funding. As the majority of participants were young adults, the higher participation rates in this sample as compared to prevalence rates of past research (e.g., Fong and Ozorio 2005; Wong and So 2003) is a reflection of the consistent finding that gambling problems are more prevalent in young adults than older adults (Petry 2005b; Shaffer and Hall 1996). However, the current study provided good support for PGSI-C despite the detail that the participants reported here may not be an accurate representation of the respective general population. As with all survey research, we relied on self-reported PG involvement, which is dependent on demand characteristics and recall bias. Cross-sectional data was used in this study instead of longitudinal data and therefore did not assess the consistency of PGSI-C as time progresses. It will be interesting to examine the test-retest reliability of PGSI-C in future investigations.
In sum, the construct of PG as measured by PGSI-C can be represented by a unifactorial model. This finding is supported by the fact that PGSI-C has good model fit in both exploratory and confirmatory factor analysis; and also good reliability and validity indicators. Future research on PGSI-C can potentially explore whether the results reported here will be replicated in other Chinese samples from different countries such as China, Singapore, and Malaysia where gambling is prevalent and popular among the locals. The same unifactorial structure between samples (Canadian and Chinese) suggests that PGSI can be regarded as a stable instrument across these populations and can be utilised to compare findings in the literature. Future psychometric evaluations of the PGSI will be essential when utilised in other populations, but the results reported here did provide a hint of positive expectation of a similar unifactorial structure, which is an important criteria when used in comparison research. The current study concludes that the application of Western theoretical and measurement models of PG is helpful and provides a foundation or starting point in understanding Chinese individuals. The PGSI-C can potentially be used among Chinese undergraduates and community samples to identify Chinese at-risk gamblers and/or problem gamblers.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders: DSM-IV-TR (4th, text revision edn.). Washington, DC: American Psychiatric Association.
Antony, M. M., Bieling, P. J., Cox, B. J., Enns, M. W., & Swinson, R. P. (1998). Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychological Assessment, 10(2), 176–181.
Arthur, D., Tong, W. L., Chen, C. P., Hing, A. Y., Sagara-Rosemeyer, M., Kua, E. H., et al. (2008). The validity and reliability of four measures of gambling behaviour in a sample of Singapore university students. Journal of Gambling Studies, 24(4), 451–462.
Blaszczynski, A., Huynh, S., Dumlao, V. J., & Farrell, E. (1998). Problem gambling within a Chinese speaking community. Journal of Gambling Studies, 14(4), 359–380.
Blunch, N. L. (2008). Introduction to structural equation modelling using SPSS and AMOS. Los Angeles: Sage.
Bolen, D. W., & Boyd, W. H. (1968). Gambling and the gambler: A review and preliminary findings. Archives of General Psychiatry, 18(5), 617–629.
Brace, N., Kemp, R., & Snelgar, R. (2009). SPSS for psychologists. Hampshire: Palgrave Macmillan.
Brooker, I. S., Clara, I. P., & Cox, B. J. (2009). The Canadian Problem Gambling Index: Factor structure and associations with psychopathology in a nationally representative sample. Canadian Journal of Behavioural Science, 41(2), 109–114.
Chen, C. N., Wong, J., Lee, N., Chan-Ho, M. W., Lau, J. T. F., & Fung, M. (1993). The Shatin community mental health survey in Hong Kong: II Major findings. Archives of General Psychiatry, 50(2), 125–133.
Clarke, D., Abbott, M., Tse, S., Townsend, S., Kingi, P., & Manaia, W. (2006). Gender, age, ethnic and occupational associations with pathological gambling in a New Zealand urban sample. New Zealand Journal of Psychology, 35(2), 84–91.
Ferris, J., & Wynne, H. (2001). The Canadian problem gambling index: Final report. Ottawa (ON): Canadian Centre on Substance Abuse.
Field, A. (2000). Discovering statistics using SPSS (3rd ed.). London: Sage.
Field, A. (2009). Discovering statistics using SPSS (3rd ed.). London: Sage.
Fong, D. K., & Ozorio, B. (2005). Gambling participation and prevalence estimates of pathological gambling in a far-east city: Macao. UNLV Gaming Research & Review Journal, 9, 15–28.
Hobson, J. S. P. (1995). Macao: Gambling on its future. Tourism Management, 16(3), 237–243.
Illinois Institute for Addiction Recovery. (2007). Addiction information. Retrieved from http://www.addictionrecov.org/aboutgam.htm.
Kline, P. (1994). An easy guide to factor analysis. London: Routledge.
Lai, D. W. L. (2006). Gambling and the older Chinese in Canada. Journal of Gambling Studies, 22(1), 121–141.
Lesieur, H. R., & Blume, S. B. (1987). The South Oaks Gambling Screen (SOGS): A new instrument for the identification of pathological gamblers. American Journal of Psychiatry, 144(9), 1184–1188.
Loo, J. M. Y., Raylu, N., & Oei, T. P. S. (2008). Gambling among the Chinese: A comprehensive review. Clinical Psychology Review, 28(7), 1152–1166.
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33(3), 335–343.
McMillen, J., Marshall, D., Ahmed, E., & Wenzel, M. (2004). 2003 Victorian longitudinal community attitudes survey. Canberra, Australia: The Centre for Gambling Research, Australian National University.
McMillen, J., & Wenzel, M. (2006). Measuring problem gambling: Assessment of three prevalence screens. International Gambling Studies, 6(2), 147–174.
Neal, P., Delfabbro, P. H., & O’Neill, M. (2004). Problem gambling and harm: Towards a national definition. Melbourne: National Gambling Research Program Working Party.
Norton, P. J. (2007). Depression Anxiety and Stress Scales (DASS-21): Psychometric analysis across four racial groups. Anxiety, Stress & Coping: An International Journal, 20(3), 253–265.
Oei, T. P. S., Lin, J., & Raylu, N. (2007a). Validation of the Chinese version of the Gambling Related Cognitions Scale (GRCS-C). Journal of Gambling Studies, 23, 309–322.
Oei, T. P. S., Lin, J., & Raylu, N. (2007b). Validation of the Chinese version of the Gambling Urges Scale (GUS-C). International Gambling Studies, 7, 101–111.
Oei, T. P. S., Lin, J., & Raylu, N. (2008). The relationship between gambling cognitions, psychological states, and gambling: A cross-cultural study of Chinese and Caucasians in Australia. Journal of Cross-Cultural Psychology, 39(2), 147–161.
Parker, G., Gladstone, G., & Chee, K. T. (2001). Depression in the planet’s largest ethnic group: The Chinese. American Journal of Psychiatry, 158(6), 857–864.
Petry, N. M. (2005a). Pathological gambling: Etiology, comorbidity, and treatment. Washington, DC: American Psychological Association.
Petry, N. M. (2005b). Prevention: Focus on gambling in youth and young adults. In N. M. Petry (Ed.), Pathological gambling: Etiology, comorbidity, and treatment (pp. 269–278). Washington, DC: American Psychological Association.
Queensland Treasury. (2006). Queensland household gambling survey 2003–04. Brisbane: Queensland Government.
Raylu, N., & Oei, T. P. S. (2002). Pathological gambling: A comprehensive review. Clinical Psychology Review, 22(7), 1009–1061.
Raylu, N., & Oei, T. P. S. (2004). Role of culture in gambling and problem gambling. Clinical Psychology Review, 23(8), 1087–1114.
Rosenthal, R. J. (2003). Distribution of the DSM-IV criteria for pathological gambling. Addiction, 98(12), 1674–1675.
Roy Morgan Research. (2006). The fourth study into the extent and impact of gambling in Tasmania with particular reference to problem gambling: Follow-up to the studies conducted in 1994, 1996, and 2000. Hobart, Tasmania: Gambling Support Bureau, Department of Health and Services.
Shaffer, H. J., & Hall, M. N. (1996). Estimating the prevalence of adolescent gambling disorders: A quantitative synthesis and guide toward standard gambling nomenclature. Journal of Gambling Studies, 12(2), 193–214.
Stinchfield, R. (2002). Reliability, validity, and classification accuracy of the South Oaks Gambling Screen (SOGS). Addictive Behaviors, 27(1), 1–19.
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics (5th ed.). Boston: Pearson.
Tang, C. S., Wu, A. M. S., & Tang, J. Y. C. (2007). Gender differences in characteristics of Chinese treatment-seeking problem gamblers. Journal of Gambling Studies, 23(2), 145–156.
Tang, C. S., Wu, A. M. S., Tang, J. Y. C., & Yan, E. C. W. (2010). Reliability, validity, and cut scores of the South Oaks Gambling Screen (SOGS) for Chinese. Journal of Gambling Studies, 26(1), 145–158.
Tseng, W. S., Lin, T. Y., & Yeh, E. K. (1995). Chinese societies and mental health. Hong Kong: Oxford University Press.
Victorian Casino and Gaming Authority. (2000). The impact of gaming on specific cultural groups report. Melbourne, Victoria.
Vong, F. (2007). The psychology of risk-taking in gambling among Chinese visitors to Macau. International Gambling Studies, 7(1), 29–42.
Wenzel, M., McMillen, J., Marshall, D., & Ahmed, E. (2004). Validation of the Victorian gambling screen. Melbourne: Centre for Gambling Research (CGR), ANU.
Wong, I. L. K., & So, E. M. T. (2003). Prevalence estimates of problem and pathological gambling in Hong Kong. American Journal of Psychiatry, 160(7), 1353–1354.
Young, M., & Stevens, M. (2008). SOGS and CGPI: Parallel comparison on a diverse population. Journal of Gambling Studies, 24(3), 337–356.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Loo, J.M.Y., Oei, T.P.S. & Raylu, N. Psychometric Evaluation of the Problem Gambling Severity Index-Chinese Version (PGSI-C). J Gambl Stud 27, 453–466 (2011). https://doi.org/10.1007/s10899-010-9221-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-010-9221-1