
Abstract
The relative influence of perceived familial addictive behaviors and personal gambling behaviors on adolescents’ self-perceptions of gambling problems was examined. Students from five high schools in Connecticut (N = 3,886) were surveyed. Of those between the ages of 14 and 17 who scored two or more on the South Oaks Gambling Screen—Revised for Adolescents (n = 532; 72% male; 43% Caucasian), 14.3% reported having a current or past problem with gambling. Wagering larger amounts in a single day, gambling on a daily basis, and perceived presence of a family member with a gambling problem were associated with increased odds of self-perception of a gambling problem. Thus, adolescents who may be less likely to be identified for prevention efforts (due to lack of engagement in high stakes gambling or the real/perceived absence of a problematic gambler in the home) appear less likely to perceive a gambling problem. To advance prevention and treatment strategies, the apparent discrepancy between adolescents’ self-perceptions and objective reports of problem gambling behaviors warrants further investigation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Adolescence is a developmental period marked by increased engagement in risk-behaviors including gambling (Chambers & Potenza, 2003; Jacobs, 2000). Although adolescent alcohol use has garnered more media attention, median rates of lifetime and past year gambling involvement (85% and 73%, respectively; National Research Council, 1999) exceed estimates of alcohol use in this population (Grunbaum et al., 2004; Johnston, O'Malley, Bachman, & Schulenberg, 2006). A smaller, yet significant, percentage of youth who gamble experience serious problems associated with their gambling such as disruptions of familial and peer relationships, difficulties in work and school environments, or involvement in criminal activities with subsequent legal complications (Hardoon, Gupta, & Derevensky, 2004; Jacobs, 2004; Lesieur & Klein, 1987; Shaffer & Hall, 2001; Shaffer, LaBrie, Scanlan, & Cummings, 1994; Wilber & Potenza, 2006). Based on their meta-analysis of adolescent gambling studies, Shaffer and colleagues (2001) concluded that 8.4% of adolescents experience moderate problems associated with their gambling, and over 3% experience more severe gambling-related problems during their lifetime.Footnote 1 A host of demographic and behavioral factors may signal greater risk for developing gambling problems, including being male, experiencing depression, heavier alcohol use, initiating gambling behavior at an early age, more diverse or frequent involvement in gambling, and wagering, winning or losing greater amounts of money (Desai, Maciejewski, Pantalon, & Potenza, 2005; Duhig, Maciejewski, Desai, Krishnan-Sarin, & Potenza, 2007; Hardoon & Derevensky, 2002; Jacobs, 2000; Lynch, Maciejewski, & Potenza, 2004; Welte, Barnes, Wieczorek, Tidwell, & Parker, 2004b). Familial factors, including genetic vulnerability (Potenza, Xian, Shah, Scherrer, & Eisen, 2005; Shah, Eisen, Xian, & Potenza, 2005; Slutske et al., 2000) and the environmental influence of real or perceived parental gambling behaviors (Hardoon et al., 2004; Jacobs, 2000; Jacobs, Marston, Singer, Widaman, Veizades, 1989; Lesieur & Klein, 1987; Vachon, Vitaro, Wanner, & Termblay, 2004) may also contribute to the development or maintenance of gambling problems among adolescents.
Based on recent census data (U.S. Census Bureau, 2000) and lower bound prevalence estimates for past-year problem gambling (Shaffer & Hall, 2001), over 750,000 youth between the ages of 13 and 18 in the United States have gambling problems and may benefit from treatment. Even adolescents whose gambling-related problems are considered less severe (as many as 2 million [Shaffer & Hall, 2001; U.S. Census Bureau, 2000]) may experience disruptions in psychosocial functioning that alter their developmental trajectory (Lynch et al., 2004), and may therefore benefit from therapeutic intervention. According to available estimates, however, as few as 1–2% of adolescents experiencing moderate to severe gambling problems actually present to treatment facilities or report having sought help (Ladouceur, Blaszczynski, & Pelletier, 2004; Steinberg, 2003; Wynne, Smith, & Jacobs, 1996). Of those who do seek help, most (over 80%) present with different problems initially (e.g., substance abuse), and their problematic gambling behavior is identified through the course of treatment (Steinberg, 2003). Multiple factors may contribute to this disparity (see Derevensky, Gupta, & Winters, 2003) including a lack of accurate awareness of the problematic nature of the behavior (Hardoon, Derevensky, & Gupta, 2003; Ladouceur et al., 2004).
Few studies have examined adolescents’ self-perceptions of gambling problem severity (Hardoon et al., 2003; Ladouceur et al., 2004; Wynne et al., 1996). Adolescents who acknowledge problem gambling behaviors when completing structured scales often do not report that they have a gambling problem. To date, only one study (Hardoon et al., 2003) has examined the discrepancy between scale-defined and self-reported measures of gambling problems in adolescents. The study found no statistically significant differences among individuals classified as having pathological gambling on the DSM-IV-J between groups defined by presence or absence of self-perceived pathological gambling (Hardoon et al., 2003); however, this study was limited due to the small numbers of subjects with pathological gambling (n = 33), particularly those acknowledging the behavior (n = 6). Nonetheless, the report described between-group differences that were not statistically significant, including findings suggesting that individuals who perceive themselves as having pathological gambling may engage in more forms of gambling, place maximum bets of greater monetary value, and initiate gambling at an earlier age. As indicated by the authors (Hardoon et al., 2003), more research is needed to examine factors influencing self-perception of youth gambling problems.
Although individual differences in gambling behavior may contribute to greater self-awareness of gambling problems, the behaviors do not occur in isolation. Negative consequences experienced as a result of gambling behaviors may be more salient than the behaviors themselves. Thus, the amount that any given gambling behavior contributes to the self-perception of a gambling problem may be diminished after taking into account the impact of negative consequences (i.e., level of gambling problem severity) on self-perception. Additionally, adolescents who perceive that family members in the home have gambling or substance use problems may judge their own behaviors and problems relative to these individuals. It is possible that juxtaposing their family members’ problematic behavior with their own behaviors leads individuals to view their behavior as normative. Alternatively, having viewed the destructive influence of their family members’ gambling or substance use problems on their home environment, they may be sensitized to the impact of addictive behaviors and thus be more likely to view their own behaviors as disordered.
The current study sought to extend prior research by examining perceived familial addictive behaviors and personal gambling behaviors as predictors of self-perception of gambling problems among adolescents who were identified as at-risk or problem gamblers. It was hypothesized that perception of having one or more family members with an addictive behavior would significantly predict self-perception of a gambling problem. It was also hypothesized that individuals who had engaged in a greater number of gambling activities (gambling diversity), who gambled more frequently, who had wagered a larger amount of money over the course of a single day (maximum daily wager), or who had placed a bet at an early age would be more likely to report a current or past gambling problem.
Method
Participants
Participants were 3,886 adolescents and young adults age 14–21 recruited from five public high schools in Connecticut in the fall of 1996. Demographically, the sample was generally representative of the regional high school student population from which it was drawn (Kloos, Tebes, & Steinberg, 1997). The vast majority of the sample (83.5%) endorsed having engaged in one or more gambling activities in their lives. Approximately 8.3% of participants were identified as at-risk gamblers and another 8.6% were considered to be problem gamblers at some point in their lifetime based on responses to the South Oaks Gambling Screen—Revised for Adolescents (SOGS-RA; Winters, Stinchfield, & Fulkerson, 1993). Although the percentage of youth whose responses were indicative of problem gambling is high relative to prior reports (the mean lifetime estimate of problem gambling among adolescents is 3.38%; Shaffer & Hall, 2001), the total percentage of youth meeting at-risk or problem gambling screening criteria (16.9%) is comparable to established norms (11.78%; Shaffer & Hall, 2001). Participants aged 18 and older were excluded from the analyses given their differential access to legal gambling venues, low representation in the larger sample, and potential influence on the generalizability of the findings to other high school students. Given the hypotheses, the sample was further limited to those individuals who were identified as lifetime at-risk or problem gamblers. Despite endorsement of gambling activity, 44 individuals who were classified as at-risk or problem gamblers provided inconsistent responses (e.g., I don’t gamble) to questions regarding age of first gambling experience and maximum amount of money ever wagered in a single day, which were used to generate predictor variables. An additional 10 individuals failed to provide a response on these two questions; thus, data from a total of 54 participants were excluded from the final sample.
The final sample (n = 532) was predominately male (72.0%; 27.8% female) and Caucasian (43.0%), with significant proportions acknowledging African American (10.9%), Hispanic (22.0%), Asian (8.8%) and “other” (13.7%) race/ethnicity. Consistent with the full sample, most students endorsed coming from two-parent (62.6%), middle income (68.6%) homes, and identified as Catholic (52.3%). As with the full sample, the percentage of at-risk gamblers and problem gamblers was approximately equal (48.9% and 51.1%, respectively), and just over 14% (n = 76) of the final sample reported having a current or past problem with gambling. Differences between the full sample and the final sample with respect to sex and ethnic/racial identity (i.e., the full sample contained a roughly equal number of male and female adolescents, and a greater percentage of individuals identified as Caucasian relative to the final sample) were anticipated given the focus on at-risk and problem gamblers (Griffiths, 1995; Stinchfield, 2000; Welte, Barnes, Wieczorek & Tidwell, 2004a; Welte et al., 2004b).
Assessments
The High School Gambling Survey (HSGS) was developed specifically for use in this study and includes both novel items as well as standardized measures of gambling problem severity. The HSGS is a self-report questionnaire that assesses demographic information, gambling-related negative consequences, perceived family history of gambling and drug problems, use of alcohol, tobacco and other drugs, quantity and frequency of gambling involvement, motives for gambling, and self-perception of problematic behaviors. Constructs relevant to the current study are described below.
Demographics and Age of First Bet
Individuals were asked to indicate their current age using one of four response options, each representing an inclusive two-year period (e.g., 14–15, 16–17). Participants were also asked to indicate if they were male or female and to specify the age at which they initiated gambling.
Gambling Problem Severity
The South Oaks Gambling Screening—Revised for Adolescents (SOGS-RA; Winters et al., 1993) assesses a variety of gambling behaviors and negative consequences. Participants were asked to indicate for each question if it was true in the past 12 months, true at any other time in your life, or never [true]. The modified version of the SOGS-RA demonstrated good internal consistency (Cronbach’s α = 0.83). Raw scores for current gambling problem severity were calculated by summing the number of items endorsed in the past 12 months. Similarly, raw scores for past gambling problem severity were calculated by summing the number of items endorsed at any other time. Individuals who reported any gambling activity and who had a raw score of 2 or 3 on the current or past measure of problem severity were labeled at-risk gamblers (Winters, Stinchfield, & Kim, 1995). Adolescents were considered to be problem gamblers if they reported engaging in at least one gambling behavior and had a past or current raw score of 4 or greater (Winters et al., 1995).
Family Member(s) with Addictive Behaviors
The perceived presence of one or more family members with a gambling problem was assessed via a single item: “How many members of the family you live with have ever had a gambling problem?” A similar question was used to assess the perceived presence of family members with alcohol and other drug problems.
Quantity, Frequency, and Diversity of Gambling Involvement
Gambling quantity was assessed via a single item, which asked participants to report the most money they had ever gambled in one day. Participants were also asked to indicate the frequency with which they engaged in various forms of gambling and related behaviors on a scale of never, less than monthly, monthly, weekly, or daily. Items were prefaced by “Have you ever...” and assessed casino gambling, sports betting, pari-mutuel betting, betting with a friend, placing bets through another person, gambling on school grounds, and wagering on more specific forms of gambling including jai alai, bingo, cards (non-casino), games of skill (non-casino), lottery, illegal numbers, slot machines, and pull tabs. A variable representing gambling diversity was created by computing the total number of gambling activities in which the participant had ever engaged.
Self-perception of Gambling Problems
The survey included a single item on self-perception of current or lifetime gambling problems: “Do you now or have you in the past ever had a gambling problem?” Participants were given the option of responding yes or no.
Procedure
Participation involved completion of the anonymous HSGS survey. The HSGS was administered during school hours in select classes. Students absent on the day of administration were thus excluded from the study. Passive consent procedures were used to secure permission from participants’ legal guardians, and verbal assent was given by individual participants at the time of the assessment. All procedures were approved by the Yale University School of Medicine Human Investigation Committee prior to data collection.
Data Management
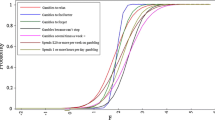
With the exception of gambling diversity, all other predictor variables (i.e., presence of one or more family members perceived to have a gambling or substance use problem, maximum daily wager, age of first bet, and peak frequency of gambling) were measured using ordinal scales. Response options for each variable were collapsed into two categories using a median split in order to eliminate problems associated with null cells (Tabachnick & Fidell, 2001). All dichotomous predictor variables were coded such that the category hypothesized to be associated with more severe gambling pathology was coded as 1. As such, adolescents who reported having one or more family members with a gambling problem or substance use problem, individuals who had placed a wager over $50, participants who had placed their first bet prior to age 12, and individuals who gambled on a daily basis were coded as 1. Responses denoting self-perception of a current or past gambling problem were coded as 1 to facilitate interpretation of odds ratios.
Data Analytic Plan
Logistic regression analysis was used to determine the unique contribution of familial factors and individual gambling behaviors to the prediction of self-perception of gambling problems. Sex, current age, and gambling problem severity were entered into the model to control for potential social and cognitive developmental differences and the influence of overall problem salience, respectively. Along with these variables, all predictor variables were entered simultaneously in the first step. Interaction terms between gambling problem severity scores and all other predictors were entered into the second step to explore whether the influence of the individual demographic, familial, and gambling behavior variables on gambling problem perception was moderated by overall gambling problem salience.
Results
Accounting for the influence of all other variables in the model, gambling problem severity (Wald χ 2(1) = 10.81, p = .001, OR = 3.11), presence of one or more family members perceived to have a gambling problem (Wald χ 2(1) = 20.52, p < .001, OR = 4.17), peak frequency of gambling engagement (Wald χ 2(1) = 11.80, p = .001, OR = 2.90), and maximum daily wager (Wald χ 2(1) = 4.43, p = .04, OR = 2.10) emerged as significant predictors of self-perception of a gambling problem. However, the presence of one or more family members perceived to have a substance use problem, total number of gambling activities (gambling diversity), and age of gambling onset were not reliably related to self-perception of a gambling problem (see Table 1 for relevant statistics for all predictors). Individuals whose responses on the SOGS-RA were indicative of problem gambling were approximately 3 times more likely than individuals identified as at-risk gamblers to endorse the self-perception of a gambling problem. Individuals with one or more family members perceived to have a gambling problem were over 4 times more likely to endorse having a gambling problem relative to individuals with no family members with a gambling problem. Individuals who engaged in daily gambling were nearly 3 times more likely than individuals who gambled less frequently to perceive that they had a gambling problem, and individuals who wagered over $50 in a single day were approximately twice as likely to endorse having a past or present gambling problem relative to those betting lesser amounts. The second step in the logistic regression analysis, containing the interaction terms between gambling problem severity score and the other predictors, was not statistically significant (p = .135). The overall model fit the data (Hosmer-Lemeshow χ 2(8) = 9.149, p = .330), and was a significant improvement over the null model (−2 log likelihood = 328.547, χ 2(17) = 106.268, p < .001), correctly classifying 87.5% of the cases.
Given the unique contribution of perceived familial gambling to the prediction of self-perception of gambling problems, additional analyses were conducted to determine if the proportion of adolescents who perceived having a gambling problem varied as a function of perceived familial gambling problems. A χ 2 test for independence revealed that the majority of adolescents who perceived having a gambling problem reported having one or more family members with a gambling problem (65.8%) whereas only a minority of adolescents who reported that they did not have a gambling problem reported the presence of a problematic gambler within the family (29.4%), χ 2(1, N = 529) = 38.172, p < .001. The magnitude of this effect was moderate according to Cohen’s (1988) conventions, Φ = .27.
Although perception of a family member with a substance use problem did not emerge as a significant predictor in the logistic regression model, reports of a family member with a gambling problem correlated significantly with reports of a family member with a substance use problem, r = 0.36, p < .001, consistent with high rates of co-occurrence of and shared genetic vulnerabilities for pathological gambling and alcohol dependence (Slutske et al., 2000; Potenza, 2007). Similarly, although gambling diversity did not significantly contribute to the prediction of self-perception of a gambling problem, a follow-up analysis focused on between-group differences revealed that individuals who perceived they had a gambling problem reported engaging in significantly more gambling activities on average (M = 8.83, SD = 3.08) than those who did not perceive having a problem (M = 7.17, SD = 2.73; t(529) = −4.818, p < .001).
Discussion
Consistent with study hypotheses, the presence of one or more family members perceived to have a gambling problem, maximum daily wager and peak gambling frequency were each associated with self-reported perception of a gambling problem. Contrary to study hypotheses, perception of familial substance use problems, greater gambling diversity and earlier age at gambling onset were not reliable predictors of self-perception of a gambling problem. Gambling problem severity did not moderate the relations between the primary predictor variables and self-perception of a gambling problem.
Perceived gambling problems in a family member was the most robust predictor of problem perception. This finding was supported by the χ 2 analysis, which indicated that the proportion of adolescents who perceived they had a problem with gambling differed as a function of perceived familial gambling problems. That is, the majority of adolescents who perceived they had a gambling problem also reported the presence of one or more family members with a gambling problem; the reverse was true for adolescents who did not perceive having a gambling problem (i.e., 70.6% reported having no family members with gambling problems). The reported presence of family members with substance use problems, however, did not reliably predict self-perception of a gambling problem. The fact that perception of one’s own gambling problem was significantly associated with the perception of having a problematic gambler (but not a substance abuser) in the home suggests that youth may use family members with gambling problems as a metric against which to judge the severity of their own problem.
Consistent with prior suggestions (Hardoon et al., 2003), having wagered over $50 in a single day was associated with increased odds of perceiving a gambling problem. Although information concerning disposable income was not available in this sample, adolescents typically have limited financial resources. To the extent that wagers correspond to losses, placing larger bets may lead to relative changes in wealth that cause significant distress and greater awareness of antecedent behaviors. Regarding peak frequency of gambling, participants who engaged in one or more forms of gambling on a daily basis were more likely to perceive that they had a gambling problem. Individuals who gamble daily may experience greater disruption to involvement in other activities leading to heightened awareness of the impact of their behaviors. More research is needed to identify mediating factors between gambling frequency and self-perception of gambling problems.
Predictions made regarding individual gambling history variables were not fully supported, however, as neither gambling diversity nor age of onset emerged as statistically significant predictors of self-perception of a gambling problem in this sample. It is worth noting, however, that an independent samples t-test revealed that individuals who perceived having a gambling problem reported significantly more gambling activities on average than those who did not perceive having a problem. Gambling diversity failed to predict gambling perceptions only in the context of the other predictors suggesting that other variables in the model account for the contribution of this variable to self-perception. The limited influence of gambling diversity in the regression model may also reflect the way in which the variable was computed. The variable for total number of gambling activities represents an individual’s entire gambling repertoire as opposed to only those games in which they regularly engage. It may be that gambling on multiple activities on an ongoing versus occasional basis would predict greater awareness of a gambling problem in the full model. Similarly, earlier age of gambling initiation may only predict greater self-awareness of gambling problems to the extent that it serves as a proxy for a longer period of active gambling. Unfortunately, neither current age nor age of gambling initiation was measured continuously in the current study. Thus, length of gambling history could not be calculated to explore this possibility.
Strengths and Limitations
The current study is the largest to date to examine the relation between perceived gambling problems and self-reported problem gambling behaviors. This large sample size permitted investigation of important areas that have not been possible in smaller samples. To our knowledge, this study is the first to systematically evaluate the relations between self-perception of gambling problems and the presence of family members perceived to have gambling and substance use problems, and examine problem perception among less severely disordered, at-risk gamblers.
Despite these relative strengths, the study has limitations that should be noted. The survey responses were self-reported and no collateral accounts were obtained to verify reported information. Thus, the extent to which stated behaviors reflect actual behaviors is unclear, and this seems particularly salient for gambling problem severity. While respondents may have under-endorsed gambling or other risk behaviors, it is also possible that they may have over-endorsed or misinterpreted items, and either possibility could lead to inappropriate classification as an at-risk or problem gambler (c.f., Ladouceur et al., 2000, 2005). Similarly, the extent to which perceived reports of familial gambling and substance use problems vary across individuals and reflect diagnostic cases is unclear. The family questions were further limited by a lack of specificity regarding environmental versus genetic influences. The questions assessed the total number of individuals living in the adolescent’s home that were thought to have a given problem, and may therefore have included non-biological parents, siblings, or extended relatives.
Conclusions and Future Directions
The current findings suggest that, among adolescents identified as problem gamblers, the presence of one or more problem gamblers in the home is associated with an increased likelihood of problem gambling acknowledgement by the respondent. Future research should evaluate the influence of parental involvement in and permissiveness of gambling on adolescents’ self-perception of gambling problems. The findings suggesting that both gambling on a daily basis and wagering larger amounts over the course of a single day similarly serve as self-salient cues of disordered gambling have important implications for prevention and intervention efforts. Understanding what factors influence adolescents’ perception of their problematic behavior is an important and essential first step to identifying appropriate prevention targets.
The results also have implications for reaching those least likely to seek treatment for problematic gambling. It appears that those most likely to perceive that their behavior is problematic are also the most likely to be identified as being in need of treatment. For example, adolescents with a positive family history of disordered gambling are a high-risk group and an appropriate program target, but all things being equal, these adolescents may be more likely to seek treatment than their counterparts who come from homes without a problematic gambling model. Likewise, adolescent problem gamblers who wager more on a given day or who gamble daily are more likely to be identified as targets for intervention due to the high profile nature of frequent, high-stakes gambling. At the same time, these individuals may be more likely than individuals who bet smaller amounts or bet infrequently to recognize they need to seek help. Thus, existing programs may only be identifying and targeting those individuals who would be more likely to seek out services on their own. Efforts to identify those who are at high risk but have a low likelihood of seeking treatment are particularly important if public health benefits are to be optimized.
Universal school-based screening could be used to identify youth experiencing gambling problems; however, limited financial and human resources may render this option impractical. Access to treatment services may also represent a limiting factor in many communities, and the cost of available treatments may represent an undue financial burden to many families (Rockloff & Schofield, 2004). Even when affordable treatment services are available, clinicians within the community who do not specialize in treatment of problem gambling may underestimate the incidence and severity of disordered gambling in this population, thus reducing the likelihood that the problem will be treated (Steinberg, 2003). Future prevention efforts may benefit from focusing on finding ways to reduce the burden of universal screening (e.g., develop computer-based, self-scoring screening programs) and on developing effective, low-cost interventions (e.g., personalized graphic feedback) that can be administered by non-clinically trained individuals. Empirical validation of these and other approaches are important in the development of effective adolescent problem gambling prevention strategies.
Notes
The term severity is used here to denote the number of consequences reported rather than how frequently these consequences are experienced or how disruptive they are to the individual’s level of functioning. Additionally, although the term problem gambling is sometimes used interchangeably or loosely with pathological gambling in the literature, a growing body of research suggests that these two constructs are not synonymous. Recently, Ladouceur, Ferland, Poulin, Vitaro, & Wiebe, (2005) found a 92.5% disparity between the number of youth in their sample that were identified as problem gamblers on the SOGS-RA (n = 93) and the number who met diagnostic criteria for pathological gambling during a clinical interview (n = 7). Though the gambling-related negative consequences experienced by youth who screen positive as problem gamblers may not cross the diagnostic threshold in all cases, it does not necessarily mean that the difficulties experienced by this group are benign.
References
Chambers, R. A., & Potenza, M. N. (2003). Neurodevelopment, impulsivity and adolescent gambling. Journal of Gambling Studies, 19, 53–84.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Erlbaum.
Derevensky, J. L., Gupta, R., & Winters, K. (2003). Prevalence rates of youth gambling problems: Are the current rates inflated? Journal of Gambling Studies, 19, 405–425.
Desai, R. A., Maciejewski, P. K., Pantalon, M. V., & Potenza, M. N. (2005). Gender differences in adolescent gambling. Annals of Clinical Psychiatry, 17, 249–258.
Duhig, A. M., Maciejewski, P. K., Desai, R. A., Krishnan-Sarin, S., & Potenza, M. N. (2007). Characteristics of adolescent past-year gamblers and non-gamblers in relation to alcohol drinking. Addictive Behaviors, 32, 80–89.
Griffiths, M. (1995). Towards a risk factor model of fruit machine addiction: A brief note. Journal of Gambling Studies, 11, 343–346.
Grunbaum, J. A., Kann, L., Kinchen, S., Ross, J., Hawkins, J., Lowry, R., et al. (2004). Youth risk behavior surveillance—United States, 2003. Morbidity and Mortality Weekly Report, 53(SS-2), 1–96.
Hardoon, K. K., & Derevensky, J. L. (2002). Child and adolescent gambling behavior: Current knowledge. Clinical Child Psychology and Psychiatry, 7, 263–281.
Hardoon, K. K., Derevensky, J. L., & Gupta, R. (2003). Empirical measures vs. perceived gambling severity among youth: Why adolescent gamblers fail to seek treatment. Addictive Behaviors, 28, 933–946.
Hardoon, K. K., Gupta, R., & Derevensky, J. L. (2004). Psychosocial variables associated with adolescent gambling. Psychology of Addictive Behaviors, 18, 170–179.
Jacobs, D. F. (2000). Juvenile gambling in North America: An analysis of long term trends and future prospects. Journal of Gambling Studies, 16, 119–152.
Jacobs, D. F. (2004). Youth gambling in North America: Long-term trends, future prospects. In J. L. Derevensky & R. Gupta (Eds.), Gambling problems in youth: Theoretical and applied perspectives (pp. 1–24). New York: Kluwer Academic/Plenum Publishers.
Jacobs, D. F., Marston, A. R., Singer, R. D., Widaman, K., & Veizades, J. (1989). Children of problem gamblers. Journal of Gambling Behavior, 5, 261–268.
Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2006). Monitoring the Future national survey results on drug use, 1975–2005: Volume I, Secondary school students (NIH Publication No. 06–5883). Bethesda, MD: National Institute on Drug Abuse.
Kloos, B., Tebes, J. K., & Steinberg, M. (1997). Gambling by Connecticut Public High School Students. A report prepared for the Connecticut Council on Problem Gambling. New Haven, CT: The Consultation Center.
Ladouceur, R., Blaszczynski, A., & Pelletier, A. (2004). Why adolescent problem gamblers do not seek treatment. Journal of Child and Adolescent Substance Abuse, 13, 1–12.
Ladouceur, R., Ferland, F., Poulin, C., Vitaro, F., & Wiebe, J. (2005). Concordance between the SOGS-RA and the DSM-IV criteria for pathological gambling among youth. Psychology of Addictive Behaviors, 19, 271–276.
Ladouceur, R., Bouchard, C., Rheaume, N., Jacques, C., Ferland, F., Leblond, J., & Walker, M. (2000). Is the SOGS an accurate measure of pathological gambling among children, adolescents and adults? Journal of Gambling Studies, 16, 1–24.
Lesieur, H. R., & Klein, R. (1987). Pathological gambling among high school students. Addictive Behaviors, 12, 129–135.
Lynch, W. J., Maciejewski, P. K., & Potenza, M. N. (2004). Psychiatric correlates of gambling in adolescents and young adults grouped by age at gambling onset. Archives of General Psychiatry, 61, 1116–1122.
Nagelkerke, N. J. D. (1991). A note on a general definition of the coefficient of determination. Biometrika, 78, 691–692.
National Research Council (1999). Pathological gambling: A critical review. Washington, D.C.: National Academy Press.
Potenza, M. N., Xian, H., Shah, K. R., Scherrer, J. F., & Eisen, S. A. (2005). Shared genetic contributions to pathological gambling and major depression in men. Archives of General Psychiatry, 62, 1015–1021.
Potenza, M. N. (2007). Impulse control disorders and co-occurring disorders: Dual diagnosis considerations. Journal of Dual Diagnosis, 3(2).
Rockloff, M. J., & Schofield, G. (2004). Factor analysis of barriers to treatment for problem gambling. Journal of Gambling Studies, 20, 121–126.
Shaffer, H. J., & Hall, M. N. (2001). Updating and refining prevalence estimates of disordered gambling behavior in the United States and Canada. Canadian Journal of Public Health, 92(3), 168–172.
Shaffer, H. J., LaBrie, R., Scanlan, K. M., & Cummings, T. N. (1994). Pathological gambling among adolescents: Massachusetts Gambling Screen (MAGS). Journal of Gambling Studies, 10, 339–362.
Shah, K. R., Eisen, S. A., Xian, H., & Potenza, M. N. (2005). Genetic studies of pathological gambling: A review of methodology and analyses of data from the Vietnam Era Twin (VET) Registry. Journal of Gambling Studies, 21, 179–203.
Slutske, W. S., Eisen, S., True, W. R., Lyons, M. J., Goldberg, J., & Tsuang, M. (2000). Common genetic vulnerability for pathological gambling and alcohol dependence in men. Archives of General Psychiatry, 57, 666–673.
Steinberg, M. A. (2003). Survey of Connecticut child and family treatment providers: Experience treating minors for a gambling problem and for the effects of family member’s gambling problem. Paper presented at the 17th National Conference on Problem Gambling, Louisville, KY.
Stinchfield, R. (2000). Gambling and correlates of gambling among Minnesota public school students. Journal of Gambling Studies, 16, 153–173.
Tabachnick, B. G., & Fidell, L. S. (2001). Using multivariate statistics (4th ed.). Needham Heights, MA: Allyn & Bacon.
U.S. Census Bureau (2000). Table QT-P2—Single years of age under 30 years and sex: 2000. Retrieved October 12, 2005, from http://factfinder.census.gov/servlet/QTTable?_bm=y&-geo_id=01000US&-qr_name=DEC_2000_SF1_U_QTP2&-ds_name=DEC_2000_SF1_U&-_lang=en&-_sse=on.
Vachon, J., Vitaro, F., Wanner, B., & Termblay, R. E. (2004). Adolescent gambling: Relationships with parent gambling and parenting practices. Psychology of Addictive Behaviors, 18, 398–401.
Welte, J. W., Barnes, G. M., Wieczorek, W. F., & Tidwell, M-C. (2004a). Gambling participation and pathology in the United States—A sociodemographic analysis using classification trees. Addictive Behaviors, 29, 983–989.
Welte, J. W., Barnes, G. M., Wieczorek, W. F., Tidwell, M-C. O., & Parker, J. C. (2004b). Risk factors for pathological gambling. Addictive Behaviors, 29, 323–335.
Wilber M. K., & Potenza M. N. (2006). Adolescent gambling: Research and clinical implications. Psychiatry 2006, 3(10), 40–48.
Winters, K. C., Stinchfield, R. D., & Fulkerson, J. (1993). Toward the development of an adolescent gambling problem severity scale. Journal of Gambling Studies, 9, 371–386.
Winters, K. C., Stinchfield, R. D., & Kim, L. G. (1995). Monitoring adolescent gambling in Minnesota. Journal of Gambling Studies, 11, 165–18.
Wynne, H., Smith, G., & Jacobs, D. (1996). Adolescent gambling and problem gambling in Alberta. A report prepared for the Alberta Alcohol and Drug Abuse Commission. Edmonton, Alberta: Wynne Resources, LTD.
Acknowledgements
The authors would like to gratefully acknowledge constructive comments made by Drs. Kelly D. Brownell and Teresa A. Treat to earlier versions of this manuscript. This manuscript was written in partial fulfillment of requirements for the degree of Master of Science. Preliminary results from this study were previously presented at the International Symposium on Problem Gambling and Co-Occurring Disorders in Mystic, Connecticut in October, 2004. The current study was supported in part through NIDA (R01 DA019039), the Veteran’s Administration (MIRECC VISN1 and REAP), and Women’s Health Research at Yale.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cronce, J.M., Corbin, W.R., Steinberg, M.A. et al. Self-perception of Gambling Problems among Adolescents Identified as At-risk or Problem Gamblers. J Gambl Stud 23, 363–375 (2007). https://doi.org/10.1007/s10899-006-9053-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-006-9053-1