
Abstract
Children with autism make and accept fewer social initiations and spend more time playing alone than with typical peers. Interventions that capitalize on technology have proven to be particularly successful in improving social initiation skills because they increase motivation, maintenance, and generalization of new social behaviors (Nikopoulos and Keenan 2004). In the present study, a portable video modeling intervention (PVMI) was used to teach persistence in social initiations to four children with autism. Two hypotheses were tested: 1) that children with autism would effectively learn persistence in social initiations to peers by using a PVMI and that this skill would 2) generalize and be maintained across people and settings. Results indicated that children with autism could learn persistence in social initiations through the PVMI. These behavior changes generalized across peers and settings and were maintained after a 1-month follow-up period. Results are discussed in terms of the effectiveness of interventions such as a PVMI as potential learning tools for children with autism.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
One of the most pervasive obstacles in the treatment of children with autism is their failure to acquire appropriate social behavior (Schreibman 1988). While this is so with a wide range of social behaviors, beginning early in life with eye contact, joint attention, and basic exploratory play, it continues throughout childhood, occurring when other appropriate behaviors such as speech and language emerge (Lord and Paul 1997; Howlin and Rutter 1987). Additionally, when children with autism learn to play cooperatively with other children, they tend to lack the appropriate social initiation skills to begin a play interaction, and merely respond to others’ initiations (Pierce and Schreibman 1995).
A number of studies have been published demonstrating various strategies to teach social initiations to children with autism. These include teaching the children a variety of “ice breakers” or different types of initiations including greetings (i.e., “Good morning”; Charlop and Trasowech 1991), offering assistance (i.e., “Can I help you?”; Harris et al. 1990), giving compliments (i.e., “nice shoes!”; Apple et al. 2005). However, there has been no back up plan put in place with these social initiations in case the child did not get a response. This unfortunately means that if the child with autism did not get a response, the social exchange would end. Moreover, if the child made a bid to play with a peer, and that peer declined the bid, the child’s initiations and search for a playmate would be over. It thus seems necessary to look beyond the one phrase initiation and address the need to teach children with autism to continue their initiations and play bids, even in the face of initially being declined. We need to teach the child with autism persistence in initiating play bids to peers.
A number of procedures have been used to teach social initiations and may be appropriate to teach persistence to children with autism. Charlop-Christy and Martins (2001) used photographic schedules to enhance the social initiations of three children with autism. These schedules included pictures of daily activities with written captions underneath. For instance, one picture depicted a child arriving at his playgroup with the caption, “go say hi to ____” written beneath it. In this study, photographic activity schedules were successful in teaching five basic social initiations to the three children with autism.
In another study by Krantz et al. (1993) four children with autism were taught social initiations by using single line social initiation statements such as “John, do you want to swing outside today?” Participants were given manual guidance to read these sentences from cards and then the guidance was faded. Three of the four children with autism increased social interactions with peers and generalized the behavior across setting, time, teacher, and activity. In this study, the typical peer was prompted to reply positively to the child’s request to play, so the children with autism were never declined in their social initiation attempts. However, this does not mimic real world play scenarios, in which children will inevitably be socially declined from time to time.
There is now a robust literature on the use of video modeling in teaching social behaviors to children with autism. Video modeling has been successful in teaching conversational speech (Charlop and Milstein 1989; Sherer et al. 2001), play related statements (Taylor et al. 1999), perception of emotion (Corbett 2003) spontaneous requesting (Wert and Neisworth 2003), imaginative play (D’Ateno et al. 2003), and perspective-taking skills (Charlop-Christy and Daneshvar 2003; LeBlanc et al. 2003). However, only four video modeling studies to date have taught basic social initiation skills to children with autism and none have taught persistence in social initiations.
Charlop and Milstein (1989) reported on the successful use of video modeling to teach conversational skills, including social initiations, to three high functioning children with autism. All children rapidly acquired reciprocal conversational speech through a video modeling intervention, with improvements generalized to other people and topics. These effects were maintained over a 15-month follow-up period. More recently, Charlop et al. (2010) replicated and expanded upon this finding.
In addition, Nikopoulos and Keenan (2003, 2004) demonstrated decreased latency in socially initiating to researchers and increased appropriate play in children with autism using this approach. Nikopoulous and Keenan (2007) also found that video modeling was effective in building sequential social skills that included social initiations. While it is important to recognize that none of these studies taught child participants what to do if their peer was unresponsive, it seems promising to use video modeling to teach persistence in initiations of play bids to children with autism.
These studies suggest that video modeling has been associated with rapid acquisition rates and strong generalization results to teach social initiation behaviors to children with autism. Additionally, with current day technological advances, it seems that there are now means that are even more advantageous than traditional video modeling using TV or computer monitors. That is, with portable technology, video modeling can be done more easily, and be presented in a variety of environments. In other words, we can bring the technology to do video modeling to the children as opposed to bringing the children to the technology. Also, in this way, children with autism can practice persistence in social initiations in typical play settings around their peers without fear of social stigma.
The present study incorporated the use of an iTouch portable appliance to provide video modeling to four children with autism and teach them persistence in social initiations of bids to play with neurotypical peers. Persistence in making social initiations of bids to play was recorded as well as generalization of bid making across children and setting.
Method
Participants
Three boys and one girl (N = 4) with autism participated in this study during weekly sessions at an afterschool behavioral treatment program. All children had received a diagnosis of autism by outside agencies according to the DSM-IV (American Psychiatric Association 1994) criteria for autism and were deficient in social skills (e.g., few interactions with typical peers, few initiations of conversations) as described by their parents, therapists, and as indicated from their test results discussed below.
Mike was a 9 year 3 month old Iranian boy with an overall functioning age-equivalent of 8-3 on the Vineland Adaptive Behavior Scale (VABS; Sparrow et al. 2005). Language skills were age-appropriate as indicated by the Vineland. However, Mike often complained in a loud, disruptive voice when changes in routine occurred. Mike was unresponsive to initiations by other peers and adults to play.
Nick was an 8 year 3 month old Caucasian boy with an overall functioning age-equivalent of 7-3 on the VABS (VABS; Sparrow et al. 1984). Language characteristics included perseveration on video game characters and conversations about weapons. Nick responded to questions and intiations, but did not initiate.
Jake was an 8 year 2 month old Taiwanese boy, with an overall functioning age-equivalent of 6–7 on the VABS (Sparrow et al. 2005). His expressive language often consisted of incomplete sentences and he engaged in delayed echolalia. In addition, Jake exhibited behavioral characteristics that included perserveration on irrelevant topics and perseverative play with musical toys and vehicles during social activities. Jake interacted alone when other peers were present and did not socially initiate. He required prompting to respond to play requests from peers.
Kelly was a 7 year 2 month old Phillipina girl with an overall functioning age-equivalent of 5–9 on the VABS (Sparrow et al. 1984). Only English was spoken in her home. She exhibited high rates of non-compliance, delayed echolalia and stereotypy (hand flapping and body rocking). She did not initiate conversations or play with others. Kelly preferred to be left alone and play with cars and would often tell her therapists “no thank you” when asked to engage in games with other children.
Three typically developing children, none of whom were enrolled in the afterschool behavioral management program, served as confederate peers for all the children with autism in the study. Confederate 1 was the 8-year old typical sibling of Jake. He engaged in positive social interactions with both typical peers and children with autism and had age-appropriate cognitive and communication skills as reported by his mother. Confederate 2 was the 6-year old typical sibling of Nick. He usually participated in the social skills activities at the behavioral management program, was typically compliant with adult requests, and enjoyed playing a wide range of outdoor games and activities. Confederate 3 was the 5-year old typical sibling of Mike. He inconsistently complied with adult requests but enjoyed playing with the toys.
Setting
The children were taught persistence in social initiations in a playroom at an after-school behavior management program for children with autism. The playroom was furnished with chairs, a table, and an assortment of toys and games. Intervention was assessed in an outdoor play setting where the child had access to a variety of age-appropriate toys and games.
Generalization was assessed both in an indoor community recreation center near the after school behavioral program with familiar peers and at a public park with unfamiliar peers.
Maintenance of the target behavior was assessed at 1 and 2-month follow-ups in the outdoor play setting and generalization settings.
Materials
A video of the persistence in social initiation behavior was created using a flip camera and four undergraduate therapists who participated in a progressive video clip series (see Table 1). Persistence in social initiations of play bids, as defined in this study, consisted of a child approaching up to three peers to play after being socially declined. Three of the therapists were engaged in play activities (i.e. board games, imaginary play with tools) in different areas of an outdoor playground, while the fourth therapist approached these “peers” to play. In the first clip, a therapist approached a peer with a ball and asked, “Will you play with me?” The peer said, “Yes, I’ll play with you” and the two therapists began to play with the ball. In the second clip, the therapist approached a peer with a board game and asked, “Will you play with me?” The peer responded, “No, I’m busy.” The therapist then had to walk across the playground to a second peer and ask, “Will you play with me?” This time, the second “peer” said “Yes, let’s play” and the two actors began to play the board game. In the third clip, the therapist’s play request was declined on her first and second social initiation attempt. This meant that the therapist had to approach a third peer and ask her to play before being socially accepted.
These clips were then loaded onto an Apple iTouch™. It is important to note that the order in which these clips were shown varied so that participants did not learn persistence in social initiations as a chained behavioral sequence. That is sometimes the child would be shown Clip 2 first, sometimes clip 1 first, and so on. This will be discussed below.
Additional materials in this study were preferred games and toys of the target children, which were identified during baseline.
Procedure
Baseline
Participants were videotaped in 3-min increments in an outdoor play setting with three confederate peers and the two other participants in the intervention. First, the experimenter gave the direction “now it’s time to play, pick a toy and choose a friend to play with”. Then undergraduate therapists were instructed to prompt the peers to either accept or not accept the social initiation request of the target child if he or she asked a peer to play over 1 session (each session consisted of three trials). The Apple iTouch was in sight of the child, although no videos were loaded at this point in time. During baseline, there was no interference from other therapists or parents so that participants interacted how they typically did in that setting. Data were collected on the child’s persistence in social initiation behavior (see Table 1).
Portable Video Modeling Intervention (PVMI)
Training during the PVMI consisted of teaching the children all the steps, which made up the target persistence in social initiation behavior in a playroom. All three clips were presented on the screen of the iTouch, which were shown before each session. For the first few sessions of the intervention, the child was shown how to push the icons to start the videos until he or she did so independently. Then it was the child’s turn. After pushing the videos and watching them, the experimenter said, “Now it’s time to play, pick a toy and choose a friend to play with.” The child was then filmed for one session (consisting of three trials lasting 3 min each) in an outdoor play setting with three neurotypical peers and the other participants. If the child with autism asked a peer to play, the peer was prompted by a student therapist to either accept or not accept the social initiation request. Sometimes the first peer said “yes” when a child with autism asked him to play, other times the child with autism had to approach two or three peers before his play bid was accepted. By varying the occurrence of a peer accepting or declining the initiation request over the three trials, the child with autism learned that although one peer may say ‘no’ to his play bid, other peers may say ‘yes’. Criterion was reached once he or she was able to persist in asking up to three friends to play over two consecutive sessions (this would equal 100 % accuracy) without prior video modeling. If the child did not successfully persist in asking peers to play until he/she received an accepted play bid, the PVMI we presented again. This presenting the video and then assessing for learning was continued until criterion was met or discontinued after 15 video modeling sessions. Generalization and maintenance were assessed only once the child met criterion for the target behavior.
Generalization
PVMI training was completed once the target child engaged in the target behavior as depicted in the video clips, independent of the iTouch. The procedure for generalization was similar to baseline. For the generalization across settings probe, the child did not have access to the iTouch and the experimenter said, “now it’s time to play, pick a toy and choose a friend to play with.” Over a 3-min period in an indoor community recreational center with familiar peers and at a community park with unfamiliar peers, the child was given two generalization sessions to exhibit the target behavior. For each trial, the experimenter or an undergraduate therapist prompted peers to either accept or decline the social initiation request of the target child.
Follow-Up
To determine that the target behavior was maintained over time, probes were collected at 1 and 2 months after the intervention had been completed. The children were filmed for 3-min in the outdoor play setting with familiar peers, in the indoor community setting with familiar peers, and at the community park setting with unfamiliar peers. At the beginning of each trial, the experimenter said, “now it’s time to play, pick a toy and choose a friend to play with.” Data were collected on the percentage of successful play bids over three probes. For each trial, undergraduate therapists were instructed to prompt the peers to either accept or decline the social initiation request of the target child at the first, second, and third play bid.
Social Validation
The social validation of the treatment outcome of this study was assessed to determine the clinical significance of the child outcomes. Ten mothers of school-aged children who did not participate in the study were recruited from the behavioral treatment center the children in the study attended and the surrounding community. These mothers were given a questionnaire that consisted of 7-Likert scale items ranging on a scale from 1 (strongly disagree) to 7 (strongly agree) before watching baseline and follow-up videotapes of the children participating in the study. Examples of items included on the questionnaire are: “My child would want to play with this peer” and “The child demonstrates an interest in playing with his/her peers”. The social validity videos were selected at random from all possible videos of baseline and follow-up sessions. These videos were also shown in a counterbalanced order so that no child was presented in two consecutive videos. Pre- and post-treatment order was also counterbalanced. Pre- and post-treatment means were then analyzed to determine if there was a significant difference (see Table 2).
Procedural Reliability
Procedural reliability data were collected on the experimenter’s compliance with written procedures. Experimenter behaviors monitored included (a) providing a general prompt to the child with autism to watch the videos on the iTouch; (b) prompting the child through each step, if needed; and (c) providing the verbal prompt, “Pick a toy and choose a friend to play with”. During each observation period, the reliability observer recorded the occurrence or nonoccurrence of each experimenter behavior as written on the procedural plan. Procedural reliability estimates were calculated using the following formula: number of appropriate behaviors divided by the number of planned experimenter behaviors for each step, multiplied by 100 (Billingsley et al. 1980). Criterion for procedural reliability was 100 %, 95 %, and 98 % agreement for each of the three experimenter behaviors.
Inter-Observer Agreement
All sessions, which included baseline, intervention, generalization, and maintenance phases, were filmed and scored by the experimenter. An individual who was not aware of the proposed results scored 33 % of all sessions. The degree of inter-observer agreement was calculated by dividing the number of agreements, by the number of agreements plus disagreements, and then multiplying the result by 100. Reliability was 100 % across all children.
Results
Child Training, Generalization, and Follow-Up Data
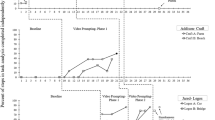
The percentage of opportunities correct for the target behavior during each session is shown in Fig. 1. During baseline, none of the participants persisted in their social initiations, although one participant demonstrated basic social initiation skills. That is, one child approached one peer to play, but was unable to approach subsequent peers after his social initiation bid was declined. After the PVMI was introduced, all four children met criterion for the persistence in social initiation behavior. In addition, although some children met criterion faster than others (sessions to criterion ranged from 4 to 10), all children demonstrated the target behavior at 100 % at 1 and 2 month follow-ups. Furthermore, the children were exhibited persistence in social initiation behavior ranging from 66 % to 100 % in at least one generalization setting after meeting criterion for the target behavior at 1 and 2-month follow-ups.

Percentage of persistence of play bids for each child during baseline, PVMI, Generalization, and follow-up
Nick’s data for persistence in social initiation play bids is presented in Panel A of Fig. 1. Nick did not demonstrate basic social initiation skills during baseline. However, once he was taught the target behavior using the PVMI, Nick reached criterion in 10 sessions. The training stimulus was then removed to test for generalization effects. Results from generalization indicated that Nick then generalized the target behavior in an indoor community setting at 100 % accuracy with familiar peers, and was successful at 66 % accuracy in an outdoor public park setting with unfamiliar peers. In this setting, Nick successfully asked two friends to play, but could not persist in initiating to a third peer. At 1 and 2-month follow-ups, Nick was able to persist in asking up to three peers to play at a rate of 100 % accuracy. He also demonstrated the target behavior with 100 % accuracy in the indoor community setting and 66 % accuracy in the public park setting at 1 and 2-month follow-ups.
Kelly’s data for persistence in social initiation play bids is presented in Panel B of Fig. 1. During baseline, Kelly was not able to demonstrate basic social initiation bids to peers. However, after implementing the PVMI, Kelly required 9 sessions to meet criterion for the intervention. In addition, Kelly generalized the target behavior in an indoor community setting with familiar peers with 100 % accuracy and a community park setting with unfamiliar peers at 66 % accuracy. At 1 and 2-month follow-ups, Kelly demonstrated that she had maintained the target behavior in the intervention setting with 100 % accuracy, the indoor community setting at 66 % accuracy, and the community park setting with 33 % accuracy.
As demonstrated in Panel C of Fig. 1, Mike inconsistently initiated to peers throughout the duration of baseline. However during treatment, Mike required only 4 sessions to reach criterion by asking up to three friends to play over two consecutive sessions. In addition, Mike generalized the target behavior in an indoor community setting with familiar peers with 100 % accuracy and at the community park setting with unfamiliar peers with 66 % accuracy. At 1 and 2-month follow-ups, Jake demonstrated that he had maintained the target behavior in the intervention setting with 100 % accuracy. He also maintained the target behavior in an indoor community setting at 100 % accuracy and community park setting at 66 % accuracy at 1 and 2-month follow-ups.
Jake’s data for persistence in social initiation play bids are presented in Panel D of Fig. 1. During baseline, Jake did not demonstrate social initiations. Nonetheless, Jake learned the target behavior within 6 sessions. Jake consistently generalized the persistence in social initiation behavior without the iTouch in an indoor community setting with familiar peers at 100 % accuracy. However like the other participants, Jake did not persist in asking three unfamiliar peers to play at a public park, resulting in a 33 % accuracy rate. At 1 and 2-month follow-ups, Jake demonstrated the target behavior at a rate of 100 % in the intervention setting, 66 % accuracy in the indoor community setting, and 33 % accuracy in the community park setting.
Social Validity of Treatment Goals
In order to evaluate the differences between pre- and post-treatment responses to the children by the 10 parents of children whom did not participate in the study, paired samples t tests were conducted for each child on each of the seven questionnaire items (see Table 2). All children were rated more favorably on post-treatment than on pre-treatment on every item, with these differences attaining statistical significance on all seven of the items for the individual children. Higher scores indicate a more favorable response. The greatest improvement for two of the three children was on the second item: “The child demonstrates an interest in playing with his/her peers.” The means and t-values for each question for each child are presented in Table 2 for Nick, Jake, Kelly, and Mike.
Discussion
The results of the present study indicated that a portable video modeling intervention (PVMI) successfully taught persistence in social initiation bids to four children with autism. All of the children in this study reached criterion for acquisition (100 % accuracy across two consecutive sessions) for the target behavior and maintained this skill at 100 % accuracy at 1 and 2-month follow-ups. Mike and Jake reached criterion for the target behavior after four and five treatment sessions respectively, while Nick and Kelly reached criterion after ten and nine sessions. All participants also demonstrated the target behavior with at least 66 % accuracy (persisting in asking two or three peers play) in at least one generalization setting.
The overall purpose of this study was to teach persistence in social initiations of play bids to children with autism through a PVMI. Despite the promise of instructional delivery via video modeling to teach social initiation skills, there have been no published video modeling studies that have taught persistence in social initiations prior to the present study (Nikopoulos and Keenan 2003, 2004). Therefore, this research builds upon existing social initiation literature by teaching children with autism how to persist in their play bids to peers. This skill is likely to have an important impact upon the social behavior of children with autism.
Rebuffs to social initiation bids are a normal part of social skill development. On a daily basis, neurotypical peers learn to deal with declined social initiation bids on the playground by moving on and asking subsequent peers to play. But while persisting in asking multiple peers to play may be learned more easily by a neurotypical child, this behavior is often difficult for a child with autism, due to their tendency to prefer to be alone. Intervention programs must therefore be specifically designed to teach persistence in social initiations to children with autism so that they can more effectively integrate with their peers in social settings. Furthermore, the importance of this skill is underlined by other findings, which suggest that when the social initiation rate of children with autism increases, then their overall social behavior improves significantly (Strain et al. 1979). The present study is another step in expanding the social initiation literature by teaching a more complex social initiation skill that is necessary for social success.
Past literature on video modeling has demonstrated its efficiency by showing rapid rates of acquisition of the target behavior (e.g. Charlop and Milstein 1989, Charlop-Christy et. al 2002). This finding has been shown in this study as well. The most sessions required to reach criterion was 10 and 9 sessions respectively by Nick and Kelly. It is possible that Nick needed more sessions because of behavior problems affecting his performance with the PVMI. Nick displayed off task behaviors of inattention, non-compliance, and tantrums. Despite these inappropriate behaviors, Nick eventually did meet criterion. Kelly often exhibited perseverative behaviors with musical toys and vehicles. When Kelly selected these toys to take to a peer and initiate a play bid, she initially failed to approach a peer and rather took the toy in a corner by herself and engaged in stereotypic behaviors with the toys. However, after the 5th PVMI session, Kelly began to exhibit more consistent persistence in social initiations.
Generalization of the target behavior across settings and peers was demonstrated by all of the children. However, results varied across participants for generalization to an untrained setting with unfamiliar peers. For example, all participants successfully generalized the target behavior at 100 % accuracy to an indoor community setting with familiar peers. However, a percentage correct of either 33 % or 66 % occurred at a public park with unfamiliar peers and no child persisted in socially initiating to a third peer in this setting. One possible reason for this may be because the children had no familiarity with the children at this park. This differed from the indoor community setting, in which the participants had previous success in their social initiation bids to confederate peers. These less robust generalization results are not uncommon in the literature of children with autism (e.g., Charlop-Christy et al. 2000). Future research should incorporate direct training of the target behavior with multiple peers and in multiple settings, which may increase the likelihood that the responses will generalize to novel settings and peers (Stokes and Baer 1977). This, in turn, could maximize the effectiveness and functionality of this behavior.
Furthermore, it is important to consider the clinical and social validity of teaching persistence in social initiations to children with autism. For instance, when developing interventions for children with autism, it is important to consider the social initiation skills of children without development disabilities. In neurotypical children, successful social initiations and subsequent peer interactions provide an important context and mechanism for the acquisition and elaboration of more complex social, language, and cognitive competencies. Even more, when neurotypical children have successful social initiations after being socially declined, they develop self-esteem and confidence in themselves and their social abilities. These patterns of social behavior begin develop early in the preschool years and continue to evolve throughout elementary school (Bijou 1978). It is therefore imperative to target persistence in social initiations in interventions for children with autism, given the importance of this social skill to typical child development.
Additionally, when developing interventions for children with autism, it is important to select skills that will be functional and reinforced by peers in the child’s life. Persistence in social initiation bids is such a skill in that it helps the child recognize that although one peer may decline a social bid to play, other peers may say yes. This allows for increased opportunities for social engagement and social skill growth in school and community settings. Given that many children with autism fail to develop social initiation skills, they often have limited social interactions and play opportunities. This deficit exacerbates the severe social withdrawal already common in many children with autism (Charlop-Christy and Kelso 2003). By teaching children with autism persistence in social initiations, they are more likely to have success in their play bids to peers, increasing the likelihood of social engagement and reinforcement of this social behavior.
The social validity is also important to consider with regards to the maintenance and generalization of skills. For example, when social behaviors are reinforced after training has ended, the likelihood that these behaviors will be maintained over time and generalize to other settings, behavior, and people is increased. Persistence in social initiations is such a skill given that when a child persists in their social initiations, peers are more likely to respond positively and reinforce that behavior. The present study supports this in that all children generalized the target skill across settings and people and maintained the skill at 1 and 2-month follow-ups.
The above findings demonstrate the potential of PVMI as an intervention tool for children with autism. Often parents report that their children with autism have a propensity for learning from videos (Heimann et al. 1995), especially those delivered via electronic screen media like the iTouch (Bernard-Opitz et al. 2001; Buggey 2005). An advantage of the PVMI over traditional video modeling is that it carries a certain “coolness” factor and represents a socially accepted intervention approach that can be used among neurotypical peers (Ward 2005). Additionally, the very nature of video modeling makes it ideal for teaching a variety of skills to this population. Not only do video media direct the child’s response to important cues for learning complex social behaviors (i.e. speaking slowly, providing eye contact to peers), but it also presented these behaviors as clearly sequenced steps. However, with PVMI over traditional video modeling, the relatively constrained viewing area of the iTouch enhances the frame of focus for the children with autism even more. This may facilitate participants to more readily to the relevant social stimuli and ignore irrelevant ones (Charlop-Christy and Daneshvar 2003; Sherer et al. 2001; Shipley-Benamou et al. 2002).
Teaching persistence in social initiations to children with autism using a PVMI also has some practical advantages over traditional video modeling research. First, it allows children with autism to use the intervention tool independent of adult assistance. Second, because of the compact size and convenience of having complex behavioral sequences on a portable device, the potential for learning can reach beyond traditional therapy settings and into natural social settings. This creates opportunities for more frequent and sustained usage of the intervention tool by children with autism both during and after the training program. Third, portable devices allow for parent programming in the home.
The limitations of this study suggest that results should be interpreted with these in mind. First, since this study was only conducted with four participants, the results may not be generalizable to children with autism as a whole. It is therefore important to replicate this study with more participants of different functioning levels. Replication is also necessary due to the discrepancy in learning and generalization rates between participants.
In everyday social situations, the behavior of persisting in social initiations is critical for successful social interactions (Haring and Lovinger 1989). While children with autism can be taught to make basic social initiations to others, they often have extreme difficulty reacting when a peer declines their initiation bid; the result is generally low social conversation and play rates among this population (Pierce and Schreibman 1995). Therefore, it is of upmost importance that future social skills research replicate the aim of the present study by teaching children with autism how to persist with other peers when their initial social initiation bid is declined. Additionally, the importance of creating social skills interventions that incorporate modern, portable, socially accepted, and user-friendly technology cannot be understated. A PVMI shows promise as an intervention tool for children with autism because it takes learning outside the therapy room and brings it into the child’s daily life. However, as portable technologies continue to evolve, more research must be done to uncover the full potential of this treatment approach.
References
American Psychiatric Association. (2004). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.
Apple, A., Billingsley, F., & Schwartz, I. (2005). Effect of video modeling alone and with self-management on compliment-giving behaviors in children with high-functioning ASD. Journal of Positive Behavior Interventions, 7, 33–46.
Bernard-Opitz, V., Sriram, N., & Nakhoda-Sapuan, S. (2001). Enhancing social problem solving in children with autism and normal children through computer-assisted instruction. Journal of Autism and Developmental Disorders, 31, 377–384.
Bijou, S. W. (1978). Behavior analysis of child development. Englewood Cliffs: Prentice-Hall.
Billingsley, F. F., White, O. R., & Munson, R. (1980). Procedural reliability: a rationale and an example. Behavioral Assessment, 2, 229–241.
Buggey, T. (2005). Video self-modeling applications with students with autism spectrum disorder in a small private school setting. Focus on Autism and Other Developmental Disabilities, 20, 52–63.
Charlop, M. H., & Milstein, J. P. (1989). Teaching autistic children conversational speech using video modeling. Journal of Applied Behavior Analysis, 22, 275–285.
Charlop, M. H., & Trasowech, J. E. (1991). Increasing autistic children’s daily spontaneous speech. Journal of Applied Behavior Analysis, 24, 247–761.
Charlop, M. H., Dennis, B., Carpenter M. H., & Greenberg, A. L. (2010). Teaching socially expressive behaviors to children with autism through video modeling. Education and Treatment of Children, 33, 371–393.
Charlop-Christy, M. H., & Daneshvar, S. (2003). Using video modeling to teach perspective taking to children with autism. Journal of Positive Behavior Interventions, 5, 12–21.
Charlop-Christy, M. H., & Kelso, S. E. (2003). Teaching children with autism conversational speech using a cue card/written script program. Education and Treatment of Children, 26.
Charlop-Christy, M. H. & Martins, M. P. (2001). Teaching children with autism using photographic activity schedules: A program to increase social behavior. Unpublished senior thesis. Claremont, CA. 472
Charlop-Christy, M. H., Le, L., & Freeman, K. A. (2000). A comparison of video modeling within vivo modeling for teaching children with autism. Journal of Autism and Developmental Disorders, 30, 537–477.
Charlop-Christy, M. H., Carpenter, M., Le, L., LeBane, L. A., & Kellet, K. (2002). Using the picture exchange communication system (PECS) with children with autism: Assessment of PECS acquisition, speech, social-communicative behavior, and problem behavior. Journal of Applied Behavior Analysis, 35, 213–231.
Corbett, B. A. (2003). Video modeling: a window into the world of autism. The Behavior Analyst Today, 4, 367–75.
D’Ateno, P., Mangiapanello, K., & Taylor, B. (2003). Using video modeling to teach complex play sequences to a preschooler with autism. Journal of Positive Behavior Interventions, 5, 5–11.
Haring, T. G., & Lovinger, L. (1989). Promoting social interaction through teaching generalized play initiation responses to preschool children with autism. Jash, 14, 58–67.
Harris, S. L., Handleman, J. S., Kristoff, B., Bass, L., & Gordon, R. (1990). Changes in language development among autistic and peer children in segregated and integrated preschool settings. Journal of Autism and Developmental Disorders, 20, 23–31.
Heimann, M., Nelson, K., Tjus, F., & ve Gillberg, A. (1995). Increasing reading and communication skills in children with autism through an interactive multimedia computer program. Journal of Autism and Developmental Disorders, 25, 89–120.
Howlin, P., & Rutter, M. (1987). Language development and disorders (Clinics in Developmental Medicine Nos. 101/102). In W. Yule & M. Rutter (Eds.), The consequences of language delay for other aspects of development. London: MacKeith Press/Blackwell.
Krantz, P. J., MacDuff, M. T., & McClannahan, L. E. (1993). Programming participation in family activities for children with autism: parent’s use of photographic activity schedules. Journal of Applied Behavior Analysis, 26, 137–138.
LeBlanc, L. A., Coates, A. M., Daneshvar, S., Charlop-Christy, M. H., Morris, C., & Lancaster, B. M. (2003). Using video modeling and reinforcement to teach perspective-taking skills to children with autism. Journal of Applied Behavior Analysis, 36, 253–257.
Lord, C., & Paul, R. (1997). Language and communication in autism. In D. J. Cohen & F. R. Volkmar (Eds.), Handbook of autism and pervasive developmental disorders (pp. 195–225). New York: Wiley.
Nikopoulos, C. K., & Keenan, M. (2003). Promoting social initiations in children with autism using video modeling. Behavioral Interventions, 18, 87–108.
Nikopoulos, C. K., & Keenan, M. (2004). Effects of video modeling on social initiations by children with autism. Journal of Applied Behavior Analysis, 37, 93–96.
Nikopoulos, C. K., & Keenan, M. (2007). Using video modeling to teach complex social sequences to children with autism. Journal of Autism and Developmental Disorders, 37, 678–693.
Pierce, K., & Schreibman, L. (1995). Increasing complex social behaviors in children with autism: Effects of peer-implemented pivotal response training. Journal of Applied Behavior Analysis, 28, 285–295.
Schreibman, L. E. (1988). Autism. Newbury Park: Sage Publications. 547social initiations in children with autism: effects of a tactile prompt. Journal of Applied Behavior Analysis, 35, 79–83.
Sherer, M., Pierce, K. L., Paredes, S., Kisacky, K. L., Ingersoll, B., & Schreibman, L. (2001). Enhancing conversational skills in children with autism via video technology. Which is better, “self” or “other” as a model? Behavioral Modification, 25, 140–158.
Shipley-Benamou, R., Lutzker, J. R., & Taubman, M. (2002). Teaching daily living skills to children with autism through instructional video modeling. Journal of Positive Behavior Interventions, 4, 165–175.
Sparrow, S., Balla, D., & Cicchetti, D. (1984). The vineland adaptive behavior scales: Interview edition. Expanded form. Circle Pines: American Guidance Service. choice. Journal of Experimental Child Psychology, 3, 159–167.
Sparrow, S. S., Cicchetti, D. V., & Balla, D. A. (2005). Vineland adaptive behavior scales: Survey form (2nd ed.). Circle Pines, MN: American Guidance Service.
Stokes, T. F., & Baer, D. M. (1977). An implicit technology of eneralization. Journal of Applied Behavior Analysis, 10, 349–367.
Strain, P. S., Kerr, M. M., & Ragland, E. U. (1979). Effects of peer-mediated social initiations and prompting reinforcement procedures on the social behavior of autistic children. Journal of Autism & Developmental Disorders, 9, 41–54.
Taylor, B. A., Levin, L., & Jasper, S. (1999). Increasing play-related statements in children with autism toward their siblings: effects of video modeling. Journal of Developmental and Physical Disabilities, 11, 253–571.
Ward, C. D. (2005). Commentary on Standen, P. J., & Brown, D. J., Virtual reality in the rehabilitation of people with intellectual disabilities Cyberpsychology & Behavior, 8, Review.
Wert, B. Y., & Neisworth, J. T. (2003). Effects of video self-modeling on spontaneous requesting in children with autism. Journal of Positive Behavioral Interventions, 5, 30–34.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Grosberg, D., Charlop, M. Teaching Persistence in Social Initiation Bids to Children with Autism Through a Portable Video Modeling Intervention (PVMI). J Dev Phys Disabil 26, 527–541 (2014). https://doi.org/10.1007/s10882-013-9362-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10882-013-9362-0