
Abstract
Somatosensory evoked potentials (SSEPs) are utilized during aneurysm clipping to detect intraoperative ischemia. We assess the diagnostic accuracy of SSEPs in predicting perioperative stroke during aneurysm clipping. A retrospective review was conducted of 429 consecutive patients who underwent surgical clipping for ruptured and unruptured cerebral aneurysms with intraoperative SSEP monitoring from 2006 to 2013. The relationship between perioperative stroke and SSEP changes was analyzed by calculating the sensitivity, specificity, and area under a Receiving Operating Characteristic curve. Sensitivity and specificity were 42% and 90%, respectively. Area under the curve was 0.66 (95% confidence interval, 0.53–0.79). Reclassification of reversible temporary clip changes to correct for paradoxical classification of SSEP false positives raised the sensitivity from 42 to 65% (p = 0.041, Chi squared test). EEG (electroencephalography) changes increased the specificity (98% vs. 90%, p < 0.001, McNemar’s test), but not sensitivity (48% vs. 42%, p = 0.621, McNemar’s test) of SSEPs for perioperative stroke. A stepwise logistic regression model selected SSEP amplitude loss (p = 0.006, OR = 3.7 [95% CI 1.5–9.2]) and the SSEP change duration (p = 0.034, OR = 1.8 [95% CI 1.1–3.1]) as independent predictors of perioperative stroke. SSEP changes induced by temporary clipping were highly reversible compared to other SSEP changes (94% vs. 60%, p = 0.003, Fisher exact test), and typically responded to clip removal or readjustment. SSEP changes have high specificity and modest sensitivity for perioperative stroke. Stroke risk is a function of both the magnitude of SSEP amplitude loss and the duration of its loss. Given the modest sensitivity, patients may benefit from multimodal monitoring including motor-evoked potentials during cerebral aneurysm surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Perioperative stroke is a significant complication of cerebral aneurysm clipping procedures, causing significant morbidity and mortality in those patients [1]. Stroke deficits are often noticed on immediate postoperative exam and can be caused by temporary and permanent clip placements that result in vessel occlusion [2].
Intraoperative monitoring of somatosensory evoked potentials (SSEPs) has been used during open cerebral aneurysm surgery to detect the effects of anesthesia, temporary clipping, and surgical manipulation on postoperative neurological function [3,4,5,6,7,8,9,10,11,12]. A threshold existing between regional cerebral blood flow and the maintenance of electrical activity has been demonstrated in the non-human primate cortex [13]. When regional cerebral blood flow decreases below 16 mL 100 g−1min−1, cortical SSEP amplitude is significantly reduced [13]. Reduced cerebral blood flow will lead to reversible changes before becoming irreversible changes. The goal of SSEPs and other forms of intraoperative neuromonitoring is to detect reversible electrical changes as early as possible, in order to prevent irreversible ischemic damage. Infarction can occur if blood flow is reduced below 12 mL 100 g−1 min−1 [14]. Given this relationship, decreases in SSEP amplitude can be used to indicate an increased risk for perioperative ischemic complications such as stroke [15]. Significant changes from baseline SSEPs are regularly utilized to inform the surgical team of impending events. Currently, the alarm criteria used for warning the surgical team is defined by consistent and persistent amplitude decreases of ≥ 50% or latency increases by 10% compared to baseline values, which have been established in the literature [15,16,17,18]. The utility of SSEP monitoring for detecting cerebral ischemic events has been demonstrated in a variety of procedures including cerebral aneurysm clipping [3, 6, 19, 20].
The aim of this study is to evaluate the diagnostic accuracy of SSEPs for perioperative stroke prediction after cerebral aneurysm clipping surgery. We analyzed the sensitivity and specificity of various significant SSEP categories in predicting the occurrence of strokes. Understanding the diagnostic accuracy of SSEPs may allow for surgical administration of neuroprotective therapy for intraoperative stroke prophylaxis.
2 Methods
2.1 Standard protocol approvals, registrations, and patient consents
The study was approved by the IRB (Institutional Review Board) for retrospective review of data on human subjects at the University of Pittsburgh (MOD08120394-04/PRO08120394).
2.2 Study population
A retrospective chart review was conducted of patient medical records of ruptured and un-ruptured aneurysms that underwent aneurysm-clipping surgery at a UPMC (University of Pittsburgh Medical Center) facility between 2006 and 2013. Post-induction, pre-incision baseline and continuous intraoperative SSEP monitoring was recorded during the entirety of the surgical procedure. Overall, the inclusion criteria for participants were: (1) adult patients over the age of 18, (2) received surgical aneurysm clipping, (3) utilized intraoperative SSEP and EEG (electroencephalography) monitoring during surgery, (4) and had documentation of pre and post-operative neurological function. Data analysis for the purposes of this manuscript was performed after the procedures were completed. Upon review of previous medical records, if a patient who underwent aneurysm clipping did not have complete intraoperative SSEP monitoring records available for review or documentation of both pre- and postoperative neurological status, they were excluded from the study.
2.3 SSEP recordings and analysis
Baseline and continuous intraoperative SSEP recording was performed in the following manner as is described in detail elsewhere [21]. Independent, bilateral stimulation of the median or ulnar nerve at the wrist and bilateral stimulation of the tibial nerve at the ankle or head of the fibula, respectively, was performed. Stimulation parameters included an intensity range of 35–60 mA, pulse duration of 0.2–0.3 ms, and frequency of 2.31–2.45 Hz. Baseline SSEP data was recorded at the start of the procedure after the patient was anesthetized but always before incision and positioning. SSEP monitoring was performed throughout the entire operation and concluded at the time of skin closure [21].
2.4 Upper extremity SSEPs
Subdermal needle electrodes were utilized to stimulate either the medial or ulnar nerve bilaterally at the wrists. Three channels of upper extremity SSEP data were collected. The P3/FZ and P4/Fz channels were utilized to record cortical potentials, the Fz-CV2 channel recorded the subcortical SSEP, and the EPs-EPd channel recorded the peripheral nerve potential at the brachial plexus.
2.5 Lower extremity SSEPs
Similarly, subdermal needle electrodes were utilized to stimulate the posterior tibial or peroneal nerve bilaterally. Three channels of data were collected in response to tibial/peroneal nerve stimulation. The Pz/Fz and P4/P3 channels recorded the cortical SSEPs, and the Fz-CV2 channeled recorded the subcortical SSEP. The strength of the stimulus and other parameters were set similarly to those used for upper extremity SSEP generation.
2.6 Neurophysiologic monitoring alarm criteria
Intraoperative monitoring of bilateral upper and lower extremity SSEPs was performed throughout the surgery until skin closure. A significant SSEP change was defined as a consistent and persistent 50% reduction in primary somatosensory cortical amplitude and/or a greater than 10% prolongation in latency from baseline values that occurred in two consecutive averaged epochs [16, 17, 22]. To eliminate surgical interference, such as drilling or electrical noise, changes in SSEP latency and/or amplitude had to have occurred in at least two consecutive average epochs of minimum 128 trials/epoch. Following an SSEP change, intraoperative intervention such as clip readjustment, blood pressure management, EEG burst suppression, was based on surgeon preference.
2.7 Group discrimination
Perioperative stroke was defined as a new motor or sensory deficit present for more than 24 h after the procedure and not documented in the preoperative history and physical examination, in the patient medical records. For conscious patients, strength in the upper and lower extremities was graded from 0 to 5 according to the following definitions [23]:
-
0—No contraction
-
1—Flicker
-
2—Movement with gravity eliminated
-
3—Movement against gravity
-
4—Movement against gravity + resistance
-
5—Normal power
For unconscious patients, the motor response was graded according to the Glasgow Coma Scale (e.g. follows commands, localizes to pain, withdrawal from pain, flexion, extension, or no response) [24]. For the sensory exam, new postoperative numbness or paresthesias not present preoperatively were considered to be new-onset neurological deficits. Neurological exams for each patient were performed and documented by critical care fellows/advanced practice providers and neurosurgical house staff, under the direction of an attending physician. Clinical staff were not blinded to neuromonitoring results.
Neurological deficits were adjudicated by a new infarct on 72-h postoperative computed tomography (CT) scan or magnetic resonance imaging (MRI), which was documented in the imaging reports by a board-certified neuroradiologist. Only new-onset neurological deficits confirmed by neuroimaging results were counted as strokes for statistical analysis. Routine clinical assessments were performed until the time of discharge; however, clinical events after 72-h were not used for the purposes of our analysis. Silent strokes and new deficits without a neuroimaging correlate were not included in the overall stroke count.
Predictive values including sensitivity and specificity of changes in SSEPs to predict perioperative stroke were calculated after categorizing patients. Patients who had no significant change in SSEP amplitude and/or latency were categorized as having “no changes”. Those with significant changes in SSEPs were categorized as having at least an amplitude change of 50% or a latency change of 10% compared to baseline values. Significant SSEP changes were categorized as either reversible versus irreversible and as losses of response (complete or nearly complete loss in amplitude) versus change in response (sub-total loss in amplitude or latency change). For all reversible SSEP changes, we documented the time to improvement to baseline. For all irreversible SSEP changes, the time to improvement was calculated as the time from change-onset to the end of the procedure and for patients without an SSEP change, the change duration was recorded as 0 min. Furthermore, we documented if SSEP changes were induced by temporary clipping or not. Additional demographic and patient-specific information including age, gender, rupture status, Hunt and Hess score, and aneurysm location (anterior vs. posterior) were collected as well.
2.8 Statistical analysis
Sensitivity, specificity, negative predictive value, positive predictive value, and odds ratios (OR) were calculated for SSEPs in relation to perioperative stroke. An receiver operating characteristic (ROC) curve, with its area under the curve (AUC), was constructed to assess the trade-off between specificity and sensitivity of SSEPs. We calculated the AUC in relation to a number of variables (including EEGs, temporary-clip changes, loss of SSEP response, and irreversible changes), to evaluate their effect on the diagnostic accuracy of SSEPs. AUCs of various models were compared with a z-test, with 95% confidence intervals (95% CI) and standard errors estimated via exponential approximation [25]. Diagnostic test characteristics (i.e. sensitivity and specificity) of various models with the same outcome were compared with a McNemar’s test.
Furthermore, we evaluated the AUC for two separate definitions of stroke as outlined by Zhu et al. [26]. Using a conservative method, termed the ‘worst-case scenario’, we utilized the definition of stroke using 72-h radiographic evidence in patients with new-onset neurological deficits. True positives were defined as any patient with an SSEP change and a perioperative stroke. A false positive was regarded as a patient with significant changes in SSEPs who did not have a perioperative stroke. A false negative was regarded as a patient without SSEP changes who had a perioperative stroke. A true negative was regarded as a patient without SSEP changes who did not have a stroke. In a second more liberal method, termed the ‘best-case scenario’, we included all reversible temporary-clip SSEP changes to the total stroke count. This analysis was performed in order to evaluate the claim that the sensitivity of SSEP changes is artificially decreased by intraoperative rescue intervention in response to SSEP changes. By capturing these instances in the stroke definition, true positives are defined as any patient with an SSEP change and a perioperative stroke or any patient with a reversible temporary-clip induced SSEP change. Sensitivities between the best- and worst-case scenarios were compared with a Chi squared test.
To evaluate the SSEP features most important in the detection of perioperative stroke, we performed a stepwise logistic regression analysis with forward and backward selection of SSEP features including reversible and irreversible SSEP changes, SSEP loss of response, temporary-clip change, and duration of SSEP change. We also performed a series of multivariate logistical regression analyses to evaluate if SSEPs could predict perioperative stroke independent of potential confounders such as age, gender, rupture status, Hunt and Hess score, and aneurysm location (anterior vs. posterior). All statistical analysis was performed with Matlab R2018b (MathWorks, Natick, MA). Statistical significance was reached at p < 0.05, unless otherwise indicated.
3 Results
3.1 Participants
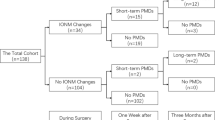
Data from a total of 429 patients (mean age 54 years) who underwent aneurysm clipping were included in this study. The majority (96%) of aneurysms were located in the anterior circulation (Table 1). Thirty percent of patients included presented with aneurysm rupture (130/429) and of these, 15 patients (12%) presented with Hunt and Hess score of 4 or 5.
3.2 Main outcomes
Of the total cohort, 33 patients (8%) developed a perioperative stroke and 55 patients (13%) had intraoperative SSEP changes (Table 2). The most common stroke presented in the frontal lobe of 15 patients (45%), as well as in the basal ganglia, which also presented in 15 patients (45%). Of the 33 strokes, intraoperative SSEP changes were negative for 19 strokes (58%). The most common location and highest incidence for SSEP-insensitive strokes occurred in the basal ganglia (11 strokes, 73%), The rate of SSEP-insensitive strokes in the parietal lobe was 71% (five of seven total parietal lobe strokes).
3.3 Diagnostic accuracy
There were a total of 55 SSEP changes of any kind (Table 3). For all SSEP changes, there were 355 true-negatives, 19 false-negatives, 41 false-positives, and 14 true-positives. The specificity, sensitivity, positive predictive value, and negative predictive value were 90%, 42%, 25%, and 95%, respectively. The stroke rate in patients without any SSEP change was 5% (19/374). The odds ratio for developing a perioperative stroke after any SSEP change was 6.4. AUC was 0.66 (0.53–0.79), as shown in Fig. 1a. Diagnostic accuracy of SSEPs was unchanged with age (AUC: 0.70, p = 0.584), gender (AUC: 0.68, p = 0.809), aneurysm rupture (AUC: 0.67, p = 0.892), Hunt and Hess score (AUC: 0.67, p = 0.864), and aneurysm location (AUC: 0.66, p = 0.984) added as covariates in the prediction of perioperative stroke.

a Receiver operating characteristic (ROC) curve (with 95% confidence interval) for SSEPs alone in predicting perioperative stroke. b Comparison of ROC curves for SSEPs in best and worst-case scenarios. The worst-case scenario utilizes stroke, defined by perioperative neurological deficits with a radiographic correlate, as the output. The best-case scenario counts reversible temporary clip SSEP changes in addition to perioperative stroke as the output. c Comparison of ROC curves for SSEPs alone, EEG alone, and a combination of both SSEPs and EEG
We then re-calculated the AUC of SSEPs for the best-case scenario, where the main outcome was considered to include all perioperative strokes and all reversible temporary clip SSEP changes (Fig. 1b). There were 54 total patients (13%) grouped into this more liberal stroke definition. This was performed in order to observe if the sensitivity of SSEPs increased in cases where intraoperative rescue intervention had a clear effect on SSEP reversal. We operated under the assumption that these cases would lead to perioperative stroke if no rescue intervention had been performed. Sensitivity under the best-case scenario was 65%, which was significantly higher than that of the worst-case scenario (p = 0.041, Chi squared test). The difference in AUCs between the best- and worst-case scenarios trended toward statistical significance (AUC: 0.80 vs. 0.66, p = 0.065, z-test).
Then, we considered the effect of EEG changes on the specificity and sensitivity of SSEPs for perioperative stroke. Two hypotheses were examined. First, we sought to examine if a change in both SSEPs and EEGs increased the specificity for stroke as compared to SSEPs alone. There were a total of 33 EEG changes, 15 (45%) of which occurred in patients who also had an SSEP change. Specificity was 98%, which was significantly higher than the specificity of SSEP changes alone (98% vs. 90%, p < 0.001, McNemar’s test). Next, we hypothesized that any intraoperative neuromonitoring change (SSEP or EEG, n = 73) was associated with an increase in sensitivity as compared to SSEP changes alone. Sensitivity of either an EEG or SSEP change was 48%, which was statistically similar to SSEP changes alone (48% vs. 42%, p = 0.621, McNemar’s test). The stroke rate in patients without any intraoperative neuromonitoring changes (SSEP or EEG) was 5%. There was no significant difference between the AUCs for predicting perioperative stroke with either SSEPs alone or with both SSEPs and EEGs (AUC: 0.66 vs. 0.68, p = 0.311, z-test). ROC curves for the two models are shown in Fig. 1c.
3.4 SSEP waveform analysis
To establish the most important waveform features in predicting perioperative stroke risk, we first examined the stroke rate as grouped by each SSEP variable. All waveform properties, including SSEP loss of response (p < 0.001), irreversible SSEP changes (p < 0.001), reversible SSEP changes (p < 0.001), temporary-clip SSEP changes (p = 0.029), were associated with an increased stroke rate, as evaluated by Chi square tests (Table 4). In patients with SSEP changes, the difference in SSEP change duration between patients with and without stroke trended toward statistical significance (median 36 vs. 13 min, p = 0.075, rank-sum test).
We then created a stepwise regression model with forward and backward selection including SSEP loss of response, SSEP change duration (input as z-scored continuous variable), reversible and irreversible SSEP changes, and temporary-clip SSEP changes as potential predictors. Of all features, SSEP change duration (p = 0.034, OR: 1.8 [95% CI 1.1–3.1]) and SSEP loss (p = 0.006, OR: 3.7 [95% CI 1.5–9.2]) were selected as the only independent predictors of perioperative stroke (Fig. 2a). Since duration was input as a z-scored variable, the odds ratio should be interpreted per increase in one standard deviation of SSEP change duration. If SSEP change duration was removed from the set of potential predictors, the stepwise regression selected SSEP loss (p < 0.001) and irreversible changes (p = 0.019) as independent predictors of stroke. Thus irreversible SSEP changes likely predict stroke as a function of SSEP change duration, given that irreversible SSEP changes last longer than reversible ones. Figure 2b demonstrates the stroke incidence as function of SSEP duration and SSEP loss. As shown, the stroke rate increases with SSEP change duration in patients with SSEP loss, but is relatively stable in patients without SSEP loss. Figure 2c demonstrates the OR for stroke as a function of SSEP change duration in patients with SSEP loss of response only (‘SSEP loss duration’). As shown, the OR steadily increases from OR = 7 to OR = 9 over the first 9 min, and then begins to more rapidly increase up to maximum of OR = 24 by 25 min.

a ORs of SSEP change duration and SSEP loss of response (with 95% confidence intervals) as evaluated by multivariate logistic regression. Asterisks (*) indicate statistically significant (p < 0.05) variables, which are visually depicted by those that do not cross OR = 1 (dashed line). b Stroke incidence (%) versus change SSEP duration (mins) as grouped by patients with and without SSEP loss of response. c OR of SSEP loss duration (with 95% confidence interval) for perioperative stroke
3.5 Rescue interventions
There were several stereotyped surgical interventions in response to SSEP changes intraoperatively (Table 5). The SSEP reversal rate of temporary clip changes was significantly higher than non-temporary clip changes (94% vs. 60%, p = 0.003, Fisher exact test). In response to temporary clip SSEP changes (n = 35), most commonly (n = 24) the surgeon attempted to remove the temporary clip to reverse the SSEP change, which was effective 92% (22/24) of the time. After temporary clip readjustment, SSEPs returned to baseline after a median of 3.3 (interquartile range 1.4–4.7) min, up to a maximum of 39 min. The causes of non-temporary clip SSEP changes (n = 20) were variable, and included intraoperative aneurysm rupture (n = 3), permanent-clip SSEP changes (n = 1), thrombus (n = 1), cerebral swelling (n = 1), and hypoxia (n = 1). Usually, however, there was no discernable cause (n = 13). Typical responses (with SSEP reversal rates) included EEG burst suppression (n = 5, 40% effective), increasing the mean arterial pressure (n = 5, 60% effective), and permanent clip readjustment (n = 2, 50% effective). Of note, burst suppression, blood pressure management, and clip readjustment were frequently used in combination with one another.
4 Discussion
Consistent with the current literature, perioperative stroke was a common complication following surgical clipping of cerebral aneurysms with an incidence rate of 8% in our study [6, 7, 9, 10, 27]. Cerebral hypoperfusion due to intentional temporary occlusion or permanent clipping of aneurysms and parent vessels and intra-operative aneurysm rupture with systemic hypotension are the most common causes of perioperative stroke following clipping [3, 5, 6, 9, 10]. A reduction in cerebral blood flow is often reflected in the cortical SSEP responses as a 50% reduction in amplitude or 10% increase in latency or disappearance of the response [3, 5,6,7].
Intraoperative SSEP changes during cerebral aneurysm clipping has a specificity of 90% in predicting perioperative strokes. The high specificity implies that SSEPs are invaluable in detecting intraoperative ischemia thereby warning the surgeon about the need for corrective and proactive interventions such as clip readjustment, EEG burst suppression, and/or increasing the mean arterial blood pressure. Our study shows that temporary-clip SSEP changes are highly reversible with clip readjustment, which may act to minimize the potential for a perioperative stroke. Furthermore, we note that both the complete loss of SSEP amplitude as well as the duration of the SSEP loss seem to portend a worse prognosis as compared to reversible SSEP changes or changes without complete amplitude loss (i.e. latency changes and sub-total amplitude loss). In specific regards to SSEP change duration, a recent study noted that an SSEP deterioration duration of longer than 11 min was associated with a higher rate of postoperative neurological deficits as compared to patients who had SSEP changes less than 11 min [28]. We present similar results, which demonstrate that the OR for perioperative stroke gradually increases from OR = 7 to OR = 9 between 0 and 9 min of SSEP deterioration, and then rapidly increases up to OR = 24 by 25 min. Given that temporary-clip SSEP changes typically return to baseline within one to five minutes after temporary clip readjustment, the surgical team may be better able to time clip removal with enough leeway to let SSEP changes return back to baseline before a large increase in OR.
The sensitivity of SSEP changes for perioperative stroke was 42%. The reason for the modest sensitivity of SSEPs is likely multifactorial. One potential explanation is the paradoxical categorization of SSEP changes, which are clearly reversed by intraoperative rescue intervention, as false positives, when they likely would have led to a stroke if no intervention been taken. These cases might be more appropriately categorized as true-positives, which would most directly affect the sensitivity of stroke detection in the sensory pathways. To test this hypothesis, we re-evaluated the sensitivity of SSEPs under the new classification scheme, whereby all reversible temporary-clip SSEP changes were counted as true positives, and showed that the sensitivity was improved from 42 to 65%. There is a strong chance that many of the reversible temporary-clip SSEP changes would have led to parietal or thalamic strokes if no intervention was taken. Thus, the low sensitivity of SSEPs in the parietal lobe (29%) are likely artificially due to paradoxical classification.
Despite a statistical improvement of the sensitivity after adjusting for paradoxical classification, the sensitivity was still only 65% in the best-case scenario. Our results mirror a recent meta-analysis, which showed that correction for paradoxical classification improved the sensitivity of SSEPs to from 63% [26]. Given the modest sensitivity and the substantial stroke rate (5%) among patients without SSEP changes, we emphasize the importance of multimodal monitoring during cerebral aneurysm surgery. Sensitivity is limited since SSEP monitoring is better utilized for predicting ischemia within the somatosensory cortex, specifically in the vascular territories of the middle and anterior cerebral arteries for median and tibial nerve stimulation respectively [3, 27]. Its reliability in predicting strokes purely in the motor cortex, subcortical regions, posterior circulation, and in the brain stem appears to be inadequate. As shown in Table 2, of the 30 strokes that occurred without concurrent SSEP changes, 22 (73%) of them occurred within the frontal lobe, basal ganglia, cerebellum, or the internal capsule, which are thought to be indiscernible by SSEP monitoring [6, 9, 10, 27]. Ischemic insults to motor areas can only be detected by SSEPs if an injury transcends into a sensory pathway. In our study, we were not able to discern a significant difference between the sensitivities of SSEPs with EEGs and SSEP monitoring alone. However, the use of motor evoked potentials in conjunction with SSEPs has been shown to improve the sensitivity of SSEPs from 59 to 92% [26]. Thus, the concurrent use of other monitoring techniques, such as transcranial motor evoked potentials may help to improve the accuracy and sensitivity of stroke prediction [18, 26].
In addition to the physiologic constraints that limit SSEP monitoring to the sensory pathways, there are additional technical constraints that limit the use of SSEPs alone. The advantage of intraoperative SSEPs is continuous monitoring that offers real-time resolution of cerebral ischemia. However, spatial resolution is limited and cannot be utilized to assess perforator arterial occlusion. SSEP changes should thus prompt the use of high spatial resolution imaging techniques such as digital subtraction angiography or indocyanine green videoangiography, which are useful in viewing small vessel patency [29, 30].
5 Conclusion
SSEP changes have high specificity and modest sensitivity for perioperative stroke. Use of a best-case scenario, in which reversible temporary-clip SSEP changes are counted as potential strokes, may improve the sensitivity of SSEPs for perioperative stroke. Given the high stroke rate among patients without either EEG or SSEP changes (5%), patients may benefit from other forms of multimodal monitoring, such as motor-evoked potentials, during cerebral aneurysm surgery. Perioperative stroke risk is a function of both the magnitude of SSEP amplitude loss and the duration of its loss. Temporary-clip SSEP changes are highly reversible, and typically respond to clip removal or readjustment.
References
Krayenbuhl N, et al. Symptomatic and silent ischemia associated with microsurgical clipping of intracranial aneurysms: evaluation with diffusion-weighted MRI. Stroke. 2009;40(1):129–33.
Jun T, et al. Preliminary study on safe thresholds for temporary internal carotid artery occlusion in aneurysm surgery based on motor-evoked potential monitoring. Surg Neurol Int. 2014;5:47.
Wicks RT, et al. Impact of changes in intraoperative somatosensory evoked potentials on stroke rates after clipping of intracranial aneurysms. Neurosurgery. 2012;70(5):1114–24. https://doi.org/10.1227/NEU.0b013e31823f5cf7.
Friedman W, et al. Evoked potential monitoring during aneurysm operation: observation after fifty cases. Neurosurgery. 1987;20(5):678–87.
Quiñones-Hinojosa A, et al. Transcranial motor evoked potentials during basilar artery aneurysm surgery: technique application for 30 consecutive patients. Neurosurgery. 2004;54(4):916–24.
Penchet G, et al. Use of intraoperative monitoring of somatosensory evoked potentials to prevent ischaemic stroke after surgical exclusion of middle cerebral artery aneurysms. Acta Neurochir. 2007;149(4):357–64.
Lopéz JR, Chang SD, Steinberg GK. The use of electrophysiological monitoring in the intraoperative management of intracranial aneurysms. J Neurol Neurosurg Psychiatry. 1999;66(2):189–96.
Little J, Lesser R, Luders H. Electrophysiological monitoring during basilar aneurysm operation. Neurosurgery. 1987;20(3):421–7.
Schramm J, et al. Surgical and electrophysiological observations during clipping of 134 aneurysms with evoked potential monitoring. Neurosurgery. 1990;26(1):61–70.
Buchthal A, Belopavlovic M, Mooij J. Evoked potential monitoring and temporary clipping in cerebral aneurysm surgery. Acta Neurochir. 1988;99(1–2):28–36.
Kashkoush AI, et al. Somatosensory evoked potentials during temporary arterial occlusion for intracranial aneurysm surgery: predictive value for perioperative stroke. World Neurosurg. 2017;104:442–51.
Kashkoush AI, et al. Perioperative stroke after cerebral aneurysm clipping: risk factors and postoperative impact. J Clin Neurosci. 2017;44:188–95.
Branston N, et al. Relationship between the cortical evoked potential and local cortical blood flow following acute middle cerebral artery occlusion in the baboon. Exp Neurol. 1974;45(2):195–208.
Morawetz RB, et al. Cerebral blood flow determined by hydrogen clearance during middle cerebral artery occlusion in unanesthetized monkeys. Stroke. 1978;9(2):143–9.
Nwachuku EL, Balzer J, Yabes JG, Habeych ME, Crammond DJ, Thirumala PD. Diagnostic value of somatosensory evoked potential changes during carotid endarterectomy: a systematic review and meta-analysis. JAMA Neurol. 2015;72(1):73–80.
Balzer JR, et al. Simultaneous somatosensory evoked potential and electromyographic recordings during lumbosacral decompression and instrumentation. Neurosurgery. 1998;42(6):1318–24 discussion 1324-5.
Chen ZY, Wong HK, Chan YH. Variability of somatosensory evoked potential monitoring during scoliosis surgery. J Spinal Disord Tech. 2004;17(6):470–6.
Guo L, Gelb AW. The use of motor evoked potential monitoring during cerebral aneurysm surgery to predict pure motor deficits due to subcortical ischemia. Clin Neurophysiol. 2011;122(4):648–55.
Skirboll S, Newell D. Noninvasic physiologic evaluation of the aneurysm patient. Neurosurg Clin N Am. 1998;9(3):463–83.
Holland N. Subcortical strokes from intracranial aneurysm surgery: implications for intraoperative neuromonitoring. J Clin Neurophysiol. 1998;15(5):439–46.
Thirumala PD, et al. Somatosensory-evoked potential monitoring during instrumented scoliosis corrective procedures: validity revisited. Spine J. 2014;14(8):1572–80.
York DH, Chabot RJ, Gaines RW. Response variability of somatosensory evoked potentials during scoliosis surgery. Spine (Phila Pa 1976). 1987;12(9):864–76.
Brigadier G. Aids to the examination of the peripheral nervous system. London: Crown Copyright. 70; 1943.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2(7872):81–4.
Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143(1):29–36.
Zhu F, et al. Intraoperative evoked potential monitoring for detecting cerebral injury during adult aneurysm clipping surgery: a systematic review and meta-analysis of diagnostic test accuracy. BMJ Open. 2019;9(2):e022810.
Mizoi K, Yoshimoto T. Permissible temporary occlusion time in aneurysm surgery as evaluated by evoked potential monitoring. Neurosurgery. 1993;33(3):434–40 discussion 440.
Wang M, et al. A prediction of postoperative neurological deficits following intracranial aneurysm surgery using somatosensory evoked potential deterioration duration. Neurosurg Rev. 2019. https://doi.org/10.1007/s10143-019-01077-5.
Felbaum D, et al. Real-time evaluation of anterior choroidal artery patency during aneurysm clipping. Cureus. 2016;8(2):e495.
Raabe A, et al. Near-infrared indocyanine green video angiography: a new method for intraoperative assessment of vascular flow. Neurosurgery. 2003;52(1):132–9 discussion 139.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kashkoush, A.I., Nguyen, C., Balzer, J. et al. Diagnostic accuracy of somatosensory evoked potentials during intracranial aneurysm clipping for perioperative stroke. J Clin Monit Comput 34, 811–819 (2020). https://doi.org/10.1007/s10877-019-00369-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-019-00369-x