
Abstract
Global life satisfaction has been linked with long-term health advantages, yet how life satisfaction impacts the trajectory of long-term health is unclear. This paper examines one such possible mechanism—that greater life satisfaction confers momentary benefits in daily life that accumulate over time. A community sample of working adults (n = 115) completed a measure of life satisfaction and then three subsequent days of ecological momentary assessment surveys (6 times/day) measuring affect (i.e., emotional valence, arousal), and perceived stress, and also provided salivary cortisol samples. Multilevel models indicated that people with higher (vs. lower) levels of life satisfaction reported better momentary affect, less stress, marginally lower momentary levels and significantly altered diurnal slopes of cortisol. Findings suggest individuals with high global life satisfaction have advantageous daily experiences, providing initial evidence for potential mechanisms through which global life satisfaction may help explain long-term health benefits.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Life satisfaction is typically defined as a global assessment of one’s past, current, or future quality of life based on a comparison with subjective standards (Shin & Johnson, 1978). Such measures are increasingly utilized in large scale survey studies of health and well-being; for example, the Behavioral Risk Factor Surveillance System uses the item, “In general, how satisfied are you with your life?” Cross-sectional studies have found that greater life satisfaction is related to better health behaviors (Grant et al., 2009) and overall physical health (Pressman & Cohen, 2005; Salovey et al., 2000). Longitudinal studies demonstrate that life satisfaction predicts better physical health (Rauma et al., 2014; Siahpush et al., 2008), reduced risk of mortality and greater longevity (Chida & Steptoe, 2008; Xu & Roberts, 2010), and fewer mobility limitations and disabilities (Collins et al., 2008; Koivumaa-Honkanen et al., 2004).
Despite these compelling relationships between global life satisfaction and health, the mechanisms for how life satisfaction impacts long-term health are less clearly defined (Diener & Chan, 2011). Theories point to life satisfaction impacting momentary processes or daily experiences, such as how one feels moment to moment or how engaged one is with their surroundings, but this proposition has not yet been carefully tested. Moreover, it is unclear if the impact of life satisfaction is observed across all moments, or if it is especially important for those moments that confer potential risk—responding to stressful experiences. This paper examines two potential pathways through which life satisfaction may impact long-term health. First, whether individuals higher in life satisfaction experience better indicators of well-being in daily life, including more positive and less negative affect, increased psychological engagement, reduced stress, and healthier cortisol function, than those lower in life satisfaction. Second, if the effects of being exposed to a stressor are less negative for those with higher levels of life satisfaction (i.e., a buffering effect). Doing so would help establish plausible pathways through which global life satisfaction may impact health over time.
Global life satisfaction
Life satisfaction is the primary cognitive component of subjective well-being that reflects one’s judgments about life (Diener et al., 1985), and is separable from its trait affective component (i.e., positive and negative affect) that reflects emotive states (Diener et al., 1999). Judgments about life are dependent on current appraisals of internal self-imposed standards, past experiences, personal values, and comparisons with others (Diener et al., 1999). Appraisals can be made about satisfaction with one’s life in general or specific life domains (Diener, 1994). We focus on general appraisals of life satisfaction, also called global life satisfaction, to assess a construct that conveys similar meaning across individuals. That is, global assessments are based on perceptions of what a person deems necessary for their overall satisfaction (Kilpatrick & Cantril, 1960; Schwarz & Strack, 1999), whereas domain-specific assessments test the importance of a particular facet of life on satisfaction levels and may vary in relevance for each individual. Global life satisfaction can be measured with the Self-Anchoring Striving Scale (SASS; Kilpatrick & Cantril, 1960). Using the SASS, respondents anchor themselves on current and predicted/future life satisfaction (Kilpatrick & Cantril, 1960).
Global life satisfaction and daily health
Despite well-established links between global life satisfaction and health, little is known about whether global life satisfaction predicts indicators of well-being in daily life, including momentary affect, stress, and physiology. These putative indicators of well-being in daily life are important to understand because they may serve as two intermediary pathways between global life satisfaction and observed long-term benefits. First, that those who have more positive judgments about their life will exist in more positive hedonic states (Diener, 1994), which may provide cumulative health effects over time. In daily life, this may translate into experiencing better momentary affective states, less stress, and showing less indication of physiological stress. Although evidence from daily life is sparse, broadly consistent with this view, adults with higher levels of global life satisfaction report lower levels of perceived life stress (Hamarat et al., 2001). Second, that global life satisfaction may buffer against the negative effects of stress (Suldo & Huebner, 2004; Veenhoven, 2008). That is, events typically associated with stress (e.g., having an argument) produce less pronounced stress responses among those with higher versus lower global life satisfaction. Again, broadly consistent with this view, spouses of hospice patients perceived care giving tasks to be less stressful if they had higher (versus lower) levels of global life satisfaction (Haley et al., 2003).
Along with more adaptive psychological and emotional processes, individuals with higher global life satisfaction may have more regulated (healthier) physiological processes (Sapolsky, 1999). For instance there is existing evidence that, typically observed at relatively long time scales, global life satisfaction is related to healthier physiological processes such as cardiovascular and neuroendocrine processes (e.g., Brummett et al., 2009; Diener & Chan, 2011). The hypothalamic pituitary adrenal (HPA) axis is a regulatory physiological system that helps maintain good health by releasing a hormone called cortisol in a natural diurnal pattern consisting of a morning peak and a decline across the day; cortisol also is released through this system in response to stress (Van Cauter, 1990). In the event that the HPA axis does not release cortisol in the normative diurnal slope and/or has an elevated or blunted cortisol output in response to stress, it may be indicative of dysregulated physiological processes and poor health (Holt-Lunstad and Steffen, 2007; Matthews et al., 2006). We propose that global life satisfaction may promote healthier HPA axis functioning (i.e., average levels, regulated diurnal cycle, and/or stress-specific cortisol output), thus creating physiological conditions in daily life that could lead to long-term positive health.
Indicators of daily well-being, momentary affect, perceptions of stress, and cortisol output are responsive to environmental stimuli (e.g., stressful events) and change within and across days (e.g., Almeida et al., 2009; Smyth et al., 1998; Watson, 1988). In turn, these indicators are related to health. For example, negative momentary mood is related to more health complaints (Watson, 1988) and greater engagement in poor health behaviors (Jones et al., 2007). Daily stress is associated with concurrent and subsequent health problems (Almeida et al., 2009; DeLongis et al., 1988). In order to capture and characterize these dynamic processes, we use Ecological Momentary Assessment (EMA; Shiffman et al., 2008; Smyth & Stone, 2003). EMA obtains data in participants’ natural environments, typically relying on multiple brief assessments over fairly short intervals (e.g., 3-6 times per day; Smyth & Heron, 2012). EMA also allows for the integration of subjective self-reports and objective assessments (e.g., salivary cortisol), providing a dynamic picture of participants’ daily experiences and well-being (e.g., Hanson et al., 2000; Smyth et al., 1998; van Eck et al., 1996). Accordingly, EMA is used for this study to examine how global life satisfaction relates to momentary indicators of daily well-being, including affect, stress, as well as the ambulatory biomarker salivary cortisol, collected in daily life.
The present paper
We examined whether varying levels of global life satisfaction predicted within-person variations in affect, stress, and physiological functioning in daily life in a community sample of working adults. Two hypotheses were tested: (1) those with higher (vs. lower) levels of global life satisfaction will have better daily indicators of well-being (i.e., better momentary affect, lower stress, and more regulated momentary and diurnal cortisol output); and (2) global life satisfaction will mitigate the impact of daily stressors (i.e., moderate momentary stress-related reactivity) on momentary indicators of well-being.
Method
Participants
Data comes from a larger study looking to understand factors that influence the interplay of stress, mood, health, and job characteristics (e.g., workplace engagement) in working adults. Working adults provided an excellent test for examining the impact of global life satisfaction on momentary indicators of well-being, as they were generally healthy (not selected for acute or chronic illness), had a full range of potential daily stressors (e.g., home, work, etc.), yet were homogenous in the sense of removing important potential confounds (e.g., unemployment, severe poverty, etc.). A community sample of employed adults (n = 115) was recruited from a mid-sized city in the Northeast US to participate (additional details in Procedures section). Participants were aged 19–63 (M = 41.23, SD = 11.87), were mostly women (75.7 %), were mostly White (76.1 %), had a range of incomes (20.7 % low income, 52.3 % middle income, 27.0 % high income; see below), mostly had some college education (48.7 % with at least a college degree, and another 40.9 % with some college education), were somewhat likely to be married (53.0 %), and somewhat likely to have children at home (49.6 %). Participants were excluded if they were unemployed or held a non-traditional work schedule (i.e., employment h outside of 6:00 am to 7:00 pm on week days), were not fluent in English, self-reported initiating psychological or psychiatric treatment (or major treatment changes) in the past 3 months, or were pregnant.
Materials
Baseline assessment
Demographic information was collected at baseline. Participants indicated their sex, age, race, marital status, and if they had children at home. Participants reported their income from nine categorical options recoded as the following: low (<$10,000–$29,999), middle ($30,000–$74,999), and high ($75,000–$150,000 or greater). Participants also indicated their highest level of education, which was recoded into the following categories: high school or less (high school but did not graduate; or high school degree or GED), some college (vocational certificate; associate’s degree; or some college), and B.A. or higher (graduated college; or went to graduate school).
To serve as an additional statistical control, participants completed the physical limitations subscale of the Health Survey-Short Form 36 (SF-36; McHorney et al., 1993). The SF-36 assesses the state of individuals’ health and any impairments they have experienced for a range of physical and social activities in the past 4 weeks. The physical functioning subscale uses ten items (α = .80) on a three-point scale: 1 (Limited a Lot), 2 (Limited a Little), and 3 (Not Limited at All) to assess whether participants report being able to perform common types of physical activities, including vigorous activities (e.g., “Does your health now limit you in climbing several flights of stairs?”). All items were recoded onto a 0-100 scale, with items averaged together such that higher scores indicated greater physical limitations. Other measures were included in this study but were not relevant to the present analyses.
Life satisfaction
The Self-Anchoring Striving Scale (SASS; Cantril, 1965) was used to assess global life satisfaction. The SASS contains two items that ask participants to indicate, using steps of a ladder, their current and anticipated satisfaction with their life. For the present analyses, we use the current life satisfaction item as our predictor as some work suggests the future satisfaction item can be interpreted as a measure of optimism (cf. Bjornskov, 2010; Gallagher et al., 2013). For current life satisfaction participants answer, “On which step of the ladder would you say you personally feel you stand at this time, assuming that the higher the step the better you feel about your life, and the lower the step the worse you feel about it? Which step comes closest to the way you feel?” Responses ranged from 0 (worst possible life) to 10 (best possible life). Although only the results for the current life satisfaction item are presented, the current and future satisfaction items had a moderately high correlation (r = .60, p < .001), as has been found in previous work (e.g., Gallagher et al., 2013). Moreover, the results for the future life satisfaction item and a combined current and future scale produce a very similar set of results as presented below; these full results are available upon request.
Ecological momentary assessment
After completing the baseline materials, participants were trained on using a supplied mobile device (Z22 Palmpilot, Palm Inc., Sunnyvale, CA) to collect EMA data. Devices were programmed using a free, open-source software package (Experience Sampling Program, http://www.experience-sampling.org/; see Barrett & Barrett, 2001) designed to collect information about momentary affect and perceived stress, among other measures. Participants were prompted to input data six times each day (see details below). For affect (Russell, 1980), as an indicator of emotional valence, participants indicated separately how happy and sad they were at the time of the prompt; sad was reverse coded prior to combining (across all measurements, r = .45, p < .001). As an indicator of arousal, participants indicated separately how interested and tired they were at the time of the prompt; tired was reverse coded prior to combining (across all measurements, r = .33, p < .001). All affect questions were answered on a 0 (Not at All) to 6 (Very Much) scale. For perceived stress, participants responded to a modified version of the 4-item Perceived Stress Scale (PSS; Cohen et al., 1983; Cohen & Williamson, 1988), adapted to assess if participants were currently feeling stressed (e.g., “At the time of the prompt, did you feel difficulties piling up so you cannot overcome them?”). Participants responded to the perceived stress items using a 0 (Not at All) to 4 (Very Much) scale. Across all measurement occasions, the PSS showed acceptable reliability (Cronbach’s α = .68). Finally, as a measure of stressor occurrence, participants indicated yes/no as to if a series of eight hassles (six pre-determined hassles; e.g., argument, traffic, and two spots to indicate others) had occurred since the last prompt. For analysis, if any hassle was reported, the moment was coded as having had a stressor. These measures are similar to those used in prior studies examining momentary health in daily life (e.g., Atienza et al., 2001; King et al., 1994; Smyth et al., 2014).
Salivary measure of cortisol
After each EMA prompt, participants provided a saliva sample for cortisol analysis. Saliva was collected using standard salivettes (Sarstedt AG & Co, Nümbrecht, Germany), small plastic tubes containing a synthetic swab that participants place in their mouths (~90 s or until saturated with saliva) and then replace in the tube. Participants were given a bag of six salivettes for each day of data collection, and were asked to label each tube with the time and date after they provided the saliva sample. Participants were asked to refrigerate their salivettes after collection. The saliva samples were sent to a technical lab (Dresden, Germany) to assay cortisol using standard methods. Given the non-normal distribution observed in cortisol, cortisol values were log-transformed prior to analysis. To control for time-varying influences on cortisol, participants also indicated in the EMA whether or not in the past 30 min they ingested caffeine, smoked cigarettes, and/or drank any alcoholic beverages, and whether or not they were eating or drinking at the time of the prompt. As an additional person-level control, participants indicated at the baseline assessment if they were currently taking oral contraceptives.
Procedure
All materials and procedures were approved by the relevant Institutional Review Boards. Participants were recruited through calls by trained research staff selecting numbers at random from a local telephone reverse directory, and through public listings on university e-mail news alerts and regional event websites. Upon initial contact, participants were provided with information about the study and screened for eligibility. Eligible participants were scheduled for an initial appointment on a Wednesday evening, during which they gave informed consent, responded to the baseline questionnaires, and were trained on the use of the EMA device and on providing saliva samples. For the next three consecutive days (i.e., Thursday through Saturday), participants carried mobile devices with them and responded to EMA prompts during all h between waking and sleeping (pre-specified by participants). Auditory alarms on the mobile device signaled participants to complete six surveys each day at semi-random intervals (stratifying waking h into roughly equal intervals); at the end of each EMA assessment, participants were also provided with an on-screen reminder to collect a saliva sample. A follow-up visit was scheduled for the Monday after EMA data and saliva collection ended for participants to return all study materials, which were checked by the experimenter for completion. All participants were paid $100 for completing the study protocol, and an additional $20 was awarded for completing >94 % (i.e., 17 + out of 18) EMA survey prompts.
Analytic plan
Multilevel analyses were performed using PROC MIXED in SAS 9.3 to account for the two-level data structure, with observations (Level 1) nested within individuals (Level 2). Multilevel analyses are typically recommended for EMA and similar data (Schwartz & Stone, 1998) and, importantly, are robust to missing data that can occur due to differing levels of compliance within and across participants. Individuals were expected to vary on their mean levels of momentary reports (Level 1); thus, random intercepts were specified to account for individual differences in momentary affect, perceived stress, and cortisol levels. As is typically recommended (e.g., Schwartz & Stone, 1998), we assumed that the residuals across momentary assessments were not independent, but rather that assessments closer in time were more related to each other than assessments spaced temporally farther apart. Thus, we specified a spatial power covariance structure for the R matrix modeling time continuously as the number of min that had elapsed since midnight of the first day of data collection for each participant.
The multilevel models tested whether current life satisfaction (assessed as a between-person Level 2 variable) predicted differing levels of affect (valence and arousal), perceived stress, and momentary cortisol, which were all assessed at the within-person level (Level 1). In addition to these within-person variables, the effect of life satisfaction also was examined on two types of between-person (Level 2) outcomes related to the occurrence of stress and the slope of cortisol throughout the day. For stress occurrences, a mean average was calculated of all moments across all days of measurements for whether a stressor had occurred; the resulting variable is thus a proportion of moments a participant reported experiencing a stressor. This stress occurrences variable was then regressed on global life satisfaction.
In order to estimate daily cortisol slope, a time of day variable was created using six 3-h blocks coinciding with the window of time each EMA survey was completed (i.e., higher values correspond to later times in the day). Of note, we used this time interval approach to calculate cortisol slopes as this was how time was accounted for as a predictor in the multilevel models. We also explored a precise assessment of time of day—the number of min that had elapsed since midnight—in the models. The time interval and precise time estimates of the cortisol slope were (as expected) highly similar, r = .98, p < .001, and produced similar results in relation to life satisfaction. Thus for presentation and consistency purposes, we present the data from the time interval approach. This time interval variable was then regressed on cortisol for each of the 3 days of data collection (to estimate three daily cortisol slopes for each person). In addition, in order to control for the influence of ingesting caffeine, smoking cigarettes, drinking alcohol, and eating or drinking anything on cortisol, these factors were also included in the regression models estimating the slope within each day. Next, for each person, the three daily slopes were averaged together to create a mean within-person cortisol slope for each participant; this mean cortisol slope variable was then regressed on global life satisfaction. Finally, we also conducted exploratory analyses to see if the slope of cortisol for each day followed a quadratic (non-linear) trend. Therefore, we performed additional analyses in which we estimated daily cortisol slopes as a function of the time of day interval and time of day interval squared (again, estimates using the precise time of day approach vs. the time interval approach produced similar results). For the vast majority of the regression analyses estimating the slope, time of day squared was not a significant predictor, thus suggesting that the cortisol data did not follow a quadratic trend. Also, global life satisfaction did not significantly predict these quadratic slopes for either the interval or precise time of day measure. Thus, we do not consider a quadratic trend of cortisol in further analyses.
For Hypothesis 1, global life satisfaction was entered in the multilevel models as a continuous variable. Results reveal the extent to which between-person differences in global life satisfaction predict average levels of momentary affect, perceived stress, and cortisol in daily life. Global life satisfaction was also tested in multivariate regression models to predict differences in the person averages for stress occurrences and cortisol slope.
For Hypothesis 2, whether or not a stressor/hassle had occurred since the last prompt was also included in the multilevel models used to test the first hypothesis, as well as the interaction between global life satisfaction and a stressor occurrence. The interaction term is of primary interest for our buffering hypothesis as it reveals if the contemporaneous association between experiencing a stressor and momentary affect, perceived stress, and cortisol is moderated by between-person differences in global life satisfaction.
Two time related effects were controlled for in the multilevel models—time of day interval and whether it was a workday or not—so as to rule out time of day and day of week effects that could account for observed results. Additionally, demographic variables were controlled for across all models (i.e., both the multilevel models and the regression models examining person averaged stress occurrence and cortisol slope). Demographic indicators including sex, age, race, income, education, marital status, and having children at home were included so as to better examine the independent effect of global life satisfaction outside of variables that could be related to well-being indicators in daily life. Income and education were recoded and entered as dichotomous variables testing for the effect of low and middle levels of income and education, respectively. We also controlled for reported physical limitations (using the SF-36). We note that the observed relationships between life satisfaction and affect, perceived stress, and cortisol were largely similar regardless of whether these control variables were included; we have retained the control variables in the presented analyses. Finally, in the models testing for momentary cortisol effects, we additionally controlled for whether participants were taking oral contraceptives (assessed at baseline), and if they had recently ingested caffeine, smoked cigarettes, drank alcohol, and/or ate or drank anything (assessed at each EMA) as these variables have known influences on cortisol levels. As cortisol levels typically attenuate throughout the day, we additionally examined the effect of global life satisfaction by time in the momentary cortisol model.
Results
Preliminary analyses
Participants reported a moderately high overall level of current life satisfaction (M = 7.13, SD = 1.61). For the EMA measures, 1766 momentary assessments were collected (an average of ~16 of 18 possible assessments). Given that we adopted a strict timing control approach in which participants only had up to 5 min to complete an EMA before being timed out and coded as missing, these numbers suggest good compliance with the EMA portion of the research protocol. On average, participants reported moderate to high levels of affect valence (M = 4.81, SD = 0.67), moderate levels of affect arousal (M = 3.87, SD = 0.86), and moderate levels of perceived stress (M = 1.81, SD = 0.53). Across all measurements, a stressor was rated as occurring for 31 % of EMAs (M = 0.31, SD = 0.18). For cortisol, 1514 momentary assessments (M = 13.76/18 possible assessments) were collected. In terms of timing, 95 % of assessments were collected within 15 min (based on participants’ self-report of time) of the start of an EMA, with the remaining being completed within 30 min. Given that there was a lag of a few min to complete the EMA and then an additional few minutes to collect the saliva, these data again suggest good levels of compliance. We observed the following average levels of (log) cortisol across assessments (M = 0.53, SD = 0.19) and average slope across days (M = −0.14, SD = 0.10).
H1: Global life satisfaction and affect, stress, and cortisol
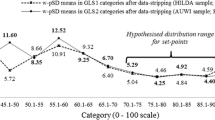
Hypothesis 1 tested whether the between-person differences in life satisfaction predicted within-person levels of momentary affect, perceived stress, and cortisol in daily life using multilevel models. As presented in Table 1, global life satisfaction had a consistent effect predicting more positive emotional valence (p < .001), greater arousal (p = .030), less perceived stress (p < .001), and marginally lower momentary levels of cortisol (p = .055) (see also Fig. 1).

Momentary levels of cortisol at each time interval by levels of global life satisfaction
Multivariate regressions also examined whether global life satisfaction predicted person-averaged levels of stress occurrences and daily cortisol decline throughout the day (i.e., cortisol slope). As shown in Table 2, across all measurements global life satisfaction showed a statistical trend towards a smaller proportion of moments with stressors (p = .058). For cortisol throughout the day, global life satisfaction significantly related to average cortisol slope (across the 3 days; p = .046; see Fig. 1).
H2: Life satisfaction as a buffer
Hypothesis 2 examined if life satisfaction buffered the effect that experiencing a stressor had on momentary affect, perceived stress, and cortisol. In other words, whether the within-person associations between experiencing a stressor and the outcomes of interest were moderated by between-person life satisfaction. The models testing for within-person differences in momentary affect, perceived stress, and cortisol in daily life as a function of life satisfaction were re-run (see Hypothesis 1), but also included were the stressor occurrence variable (indicating whether or not a hassle/stressor had occurred since the last prompt), and the interaction of stressor occurrence and global life satisfaction. As shown in Table 1, global life satisfaction did not interact with the stressor occurrence variable to predict any of the momentary affect, perceived stress, or cortisol variables (ps > .175).
Exploratory analyses
Age may be related to global life satisfaction, or may moderate the observed associations between life satisfaction and affect, perceived stress, and cortisol. In our sample, age was unrelated to life satisfaction (r = .05, p = .56). We re-ran the analyses tested in Hypothesis 1 but also included an interaction term between age and life satisfaction. The age by life satisfaction interaction was not significant for affect, stress, and cortisol (ps > .211).
We also tested if typical levels of emotional valence and/or arousal in daily life accounted for the relationship between life satisfaction and cortisol. We created a person mean for valence and arousal (i.e., an average of all valence measures for the entire measurement period for each participant) and entered these two terms into the model testing the effect of life satisfaction on cortisol described in Hypothesis 1. Neither person-averaged valence nor arousal were significant predictors of average cortisol (ps > .658), and life satisfaction was a significant predictor of average cortisol (p = .021).
Discussion
As has been well-established in prior research, high global life satisfaction is linked with a range of positive health outcomes; yet research exploring potential mechanisms that may explain such linkages is lacking (Diener & Chan, 2011). The present study contributes to the understanding of global life satisfaction by using EMA and ambulatory physiological measurements to test whether global life satisfaction was related to momentary indicators of well-being in daily life. As predicted, individuals with high levels of global life satisfaction experienced better momentary experiences—better affect (more positive mood states, and more arousal as indexed by items assessing interest and engagement), less perceived stress, a trend towards lower momentary cortisol levels, and a statistically significant (but weak) association with the diurnal slope of cortisol—than those with lower levels of life satisfaction. Contrary to expectations, global life satisfaction did not buffer individuals from the negative effects of acute stressful occurrences in daily life.
The associations of life satisfaction with the momentary well-being indicators provide evidence consistent with the hedonic profile (Diener, 1994), such that individuals with higher global life satisfaction generally report feeling better in daily life. As suggested by theory, this may be attributed to adaptive cognitions such that people with higher global life satisfaction have more positive judgments (or appraisals) and self-assessments (or perceived personal resources), which promote healthy psychological and physical functioning (Lazarus & Folkman, 1984; Smith et al., 1993). In contrast, individuals with lower global life satisfaction may engage in maladaptive perseverative cognitions, such as repetitive thoughts or worries, which can give way to poor health via repeated and/or extended stress responses (Brosschot, 2010; Smyth et al., 2013).
The cortisol analyses showed that global life satisfaction was marginally related (p = .055) to lower average momentary cortisol levels (presumptively reflecting healthier HPA axis functioning) in daily life; this relationship was significant in secondary statistical models with additional controls. Global life satisfaction was also significantly positively associated with the diurnal slope of cortisol, although this relationship was small in magnitude. As HPA axis functioning is related to a number of other biological processes (e.g., metabolic and immune processes), these data suggest a plausible biological link between global life satisfaction and long-term health outcomes. This finding also helps demonstrate effects using objective measures of physiological functioning that are not reliant on self-report measures, thus reducing concerns about demand characteristics and other reporting biases that may be related to global life satisfaction. Global life satisfaction was (significantly but rather weakly) related to cortisol slope throughout the day, yet the study’s assessment schedule may not have been ideal to test for effects across the full day. That is, ideally, cortisol would also be measured shortly after waking given that a typical cortisol slope has a curvilinear pattern with an initial surge followed by sharp decreases after waking, followed by flatter declines later in the day (Van Cauter, 1990). Our initial measurements did not take place for up to a few hours after waking, thus missing the waking rise; a potentially important period of daily HPA function (Nader et al., 2010). Future work should measure cortisol closer to waking and with a greater density of samples so as to better test how global life satisfaction is related to the cortisol awakening response and diurnal slope.
No participants in the current study exhibited very low levels of global life satisfaction. This may result from the self-selected enrollment process used for recruiting participants into the present study; possibly, individuals who are truly suffering (i.e., deeply unsatisfied with their life) are less likely to seek out participation in research studies or do not have regular employment, which was an eligibility requirement for the study. Yet, even those with slightly lower levels of global life satisfaction appear to experience worse momentary well-being indicators, suggesting that even small differences in life satisfaction may predict differential experiences in daily life. In line with past research (Gallup, 2009), there appears to be a benefit to reporting high global life satisfaction. For example, those with more global life satisfaction reported lower stress levels in daily life. There may be a virtuous cycle whereby those with more positive, happy outlooks in general have more positive (and/or less negative) daily experiences that promote better affect and lower perceived stress over time. Individuals with high global life satisfaction also may engage in more, and derive more satisfaction from, positive health behaviors (e.g., exercise; Grant et al., 2009). These processes may cumulatively translate to long-term health outcomes; for example, levels of affect and stress in daily life can predict future health complaints and poor health behaviors (Almeida et al., 2009; DeLongis et al., 1988; Jones et al., 2007).
Some prior work suggests that global life satisfaction may have beneficial effects because it buffers against potential deleterious effects of (generally globally assessed) stress (Suldo & Huebner, 2004; Veenhoven, 2008); our study tested this proposition by examining whether global life satisfaction moderated the impact of acute stress on a range of momentary well-being indicators. Global life satisfaction did not moderate the impact of acute stressors on momentary states in the present data. Thus, it may be that global life satisfaction does not contribute to health by increasing resiliency to acute stressors; rather, those with high global life satisfaction may be better able to cope with stress over time, with benefits from global life satisfaction accruing from ‘enrichment’. For example, having more positive affect and less negative affect on a daily basis may give individuals with higher global life satisfaction an advantage over time; individuals with more positive affect have better long term health outcomes, including lower rates of morbidity and mortality (Pressman & Cohen, 2005). Interestingly, including person-average affect indicators in our model did not attenuate the relationship between life satisfaction and average levels of cortisol; we note, however, that this is a very crude test of the potential role of affect (e.g., as potential mediator). Future work should use more sophisticated approaches (e.g., inclusion of time-varying estimates of life satisfaction, sophisticated lag analyses, etc.) to better understand these relationships.
Limitations and future directions
Our measure of global life satisfaction and, particularly, our approach to measuring affect were relatively non-standard. Future work should certainly replicate (and extend) these findings using alternative measures (e.g., satisfaction with life scale [Diener et al., 1985]). This is the first study of which we are aware to show associations between global life satisfaction and well-being in daily life; as such, there are many possible subsequent research questions. For instance, it is important to consider the role of personality traits. In particular, there may be a synergistic effect between traits linked with negative health outcomes, such as neuroticism (Shipley et al., 2007) or ruminative thinking (Petrie et al., 2001; Thomsen et al., 2004), and lower global life satisfaction whereby psychological and physiological health and well-being are compromised. On the contrary, more adaptive traits shown to predict good health, such as conscientiousness (Roberts et al., 2007), optimism (Carver & Scheier, 2014), and proactive coping styles (Juth et al., 2015), may interact with high global life satisfaction yielding multiplicative health benefits. Future work could examine the interplay between these and other dispositions with global life satisfaction in shaping daily health and well-being.
The same working (Thursday and Friday) and non-working (Saturday) days were measured across all participants so as to standardize assessment schedules; yet this leaves experiences on other days unknown. Given the potentially complex relationships between affect, stress and physiological functioning, future work may more explicitly explore transitional periods and spillover effects (e.g., as individuals go from work to home).
Despite using a global assessment of life satisfaction that was obtained prior to micro-longitudinal momentary assessments, these data do not allow us to confidently determine the causal direction between global life satisfaction and momentary indicators of well-being in daily life. Nonetheless, this study is the first of which we are aware to show an association between global life satisfaction and momentary well-being in daily life. These novel findings, combined with the existing evidence linking global life satisfaction to health outcomes longitudinally (Chida & Steptoe, 2008; Collins et al., 2008; Koivumaa-Honkanen et al., 2004; Xu & Roberts, 2010), may provide the necessary evidentiary basis to move research forward in new directions (e.g., developing and testing interventions to enhance life satisfaction).
Conclusion
Using EMA to capture naturalistic experiences, this study applied a novel methodological approach to contribute to the current examinations of global life satisfaction as it relates to momentary indicators of well-being in daily life. It is the first to show relationships between global life satisfaction and better momentary experiences in daily life using both self-reported and objective measures, including more positive emotional valence and greater arousal, less stress, and putatively healthier physiological functioning (HPA axis functioning as indexed by cortisol). Additionally, these findings are consistent with a potential mechanistic pathway through which global life satisfaction confers its relatively well-documented long-term health benefits; these data suggest that one of the ways that global life satisfaction may bring about those positive outcomes is through the cumulative effect over time of better affect, stress, and cortisol in daily life.
References
Almeida, D. M., McGonagle, K., & King, H. (2009). Assessing daily stress processes in social surveys by combining stressor exposure and salivary cortisol. Biodemography and Social Biology, 55, 219–237. doi:10.1080/19485560903382338
Atienza, A. A., Collins, R., & King, A. C. (2001). The mediating effects of situational control on social support and mood following a stressor: A prospective study of dementia caregivers in their natural environments. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 56, S129–S139. doi:10.1093/geronb/56.3.S129
Barrett, L. F., & Barrett, D. J. (2001). Computerized experience-sampling: How technology facilitates the study of conscious experience. Social Science Computer Review, 19, 175–185. doi:10.1177/089443930101900204
Bjornskov, C. (2010). How comparable are the Gallup world poll life satisfaction data? Journal of Happiness Studies, 11, 41–60.
Brosschot, J. (2010). Markers of chronic stress: Prolonged physiological activation and (un)conscious perseverative cognition. Neuroscience and Biobehavioral Reviews, 35, 46–50. doi:10.106/j.neubiorev.2010.01.004
Brummett, B. H., Boyle, S. H., Kuhn, C. M., Siegler, I. C., & Williams, R. B. (2009). Positive affect is associated with cardiovascular reactivity, norepinephrine level, and morning rise in salivary cortisol. Psychophysiology, 46, 862–869.
Cantril, H. (1965). The Pattern of Human Concerns. New Brunswick, NJ: Rutgers University Press.
Carver, C. S., & Scheier, M. F. (2014). Dispositional optimism. Trends in Cognitive Sciences, 18, 293–299. doi:10.106/j.tics.2014.02.003
Chida, Y., & Steptoe, A. (2008). Positive psychological well-being and mortality: A quantitative review of prospective observational studies. Psychosomatic Medicine, 70, 741–756. doi:10.1097/PSY.0b013e31818105ba
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385–396.
Cohen, S., & Williamson, G. (1988). Perceived stress in a probability sample of the United States. In S. Spacapam & S. Oskamp (Eds.), The social psychology of health: Claremont Symposium on applied social psychology. Newbury Park, CA: Sage.
Collins, A. L., Goldman, N., & Rodríguez, G. (2008). Is positive well-being protective of mobility limitations among older adults? Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 63, 321–327.
DeLongis, A., Folkman, S., & Lazarus, R. S. (1988). The impact of daily stress on health and mood: psychological and social resources as mediators. Journal of Personality and Social Psychology, 54, 486–495. doi:10.1037/0022-3514.54.3.586
Diener, E. (1994). Assessing subjective well-being: Progress and opportunities. Social Indicators Research, 31, 103–157. doi:10.1007/BF01207052
Diener, E., & Chan, M. Y. (2011). Happy people live longer: Subjective well-being contribute to health and longevity. Applied Psychology: Health and Well-Being, 3, 1–43. doi:10.1111/j.1758-0854.2010.01045.x
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49, 71–75. doi:10.1207/s15327752jpa4901_13
Diener, E., Suh, E. M., Lucas, R. E., & Smith, H. L. (1999). Subjective well-being: Three decades of progress. Psychological Bulletin, 125, 276–302. doi:10.1037/0033-2909.125.2.276
Gallagher, M. W., Lopez, S. J., & Pressman, S. D. (2013). Optimism is universal: Exploring the presence and benefits of optimism in a representative sample of the world. Journal of Personality, 81, 429–440. doi:10.1111/jopy.12026
Gallup. (2009). World poll methodology. Technical Report. Washington, DC: Gallup.
Grant, N., Wardle, J., & Steptoe, A. (2009). The relationship between life satisfaction and health behavior: A cross-cultural analysis of young adults. International Journal of Behavioral Medicine, 16, 259–268. doi:10.1007/s1252
Haley, W. E., LaMonde, L. A., Han, B., Burton, A. M., & Schonwetter, R. (2003). Predictors of depression and life satisfaction among spousal caregivers in hospice: Application of a stress process model. Journal of Palliative Medicine, 6, 215–224. doi:10.1089/109662103764978461
Hamarat, E., Thompson, D., Zabrucky, K. M., Steele, D., & Matheny, K. B. (2001). Perceived stress and coping resource availability as predictors of life satisfaction in young, middle-ages, and older adults. Experimental Aging Research, 27, 181–196. doi:10.1080/036107301750074051
Hanson, E. J. S., Maas, C. J. M., Meijman, T. F., & Godaert, G. L. R. (2000). Cortisol secretion throughout the day, perceptions of the work environment, and negative affect. Annals of Behavioral Medicine, 22, 316–324. doi:10.1007/BF02895668
Holt-Lunstad, J., & Steffen, P. R. (2007). Diurnal cortisol variation is associated with nocturnal blood pressure dipping. Psychosomatic Medicine, 69, 1097. doi:10.1097/PSY.0b013e318050d6cc
Jones, F., O’Connor, D. B., Conner, M., McMillan, B., & Ferguson, E. (2007). Impact of daily mood, work hours, and iso-strain variables on self-reported health behaviors. Journal of Applied Psychology, 92, 1731–1740. doi:10.1037/0021-9010.92.6.1731
Juth, V., Dickerson, S. S., Zoccola, P. M., & Lam, S. (2015). Understanding the utility of emotional approach coping: Evidence from a laboratory stressor and daily life. Anxiety, Stress, and Coping, 28, 50–70. doi:10.1080/10615806.2014.921912
Kilpatrick, F., & Cantril, H. (1960). Self-anchoring scaling: A measure of individuals unique reality worlds. Journal of Individual Psychology, 16, 158–173.
King, A. C., Oka, R. K., & Young, D. R. (1994). Ambulatory blood pressure and heart rate responses to the stress of work and care giving in older women. The Journal of Gerontology, 49, M239–M245. doi:10.1093/geronj/49.6.M239
Koivumaa-Honkanen, H., Koskenvuo, M., Honkanen, R. J., Viinamäki, H., Heikkilä, K., & Kaprio, J. (2004). Life dissatisfaction and subsequent work disability in an 11-year follow-up. Psychological Medicine, 34, 221–228. doi:10.1017/S0033291703001089
Lazarus, R. S., & Folkman, S. (1984). Stress, Appraisal, and Coping. New York: Springer.
Matthews, K., Schwartz, J., Cohen, S., & Seeman, T. (2006). Diurnal cortisol decline is related to coronary calcification: CARDIA study. Psychosomatic Medicine, 68, 657–661. doi:10.1097/01.psy.0000244071.42939.0e
McHorney, C. A., Ware, J. E., & Raczek, A. E. (1993). The MOS 36-item short-form health survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Medical Care, 31, 247–263.
Nader, N., Chrousos, G. P., & Kino, T. (2010). Interactions of the circadian CLOCK system and the HPA axis. Trends in Endocrinology and Metabolism, 21, 277–286. doi:10.1016/j.tem.2009.12.011
Petrie, K. J., Sivertsen, B., Hysing, M., Broadbent, E., Moss-Morris, R., Eriksen, H. R., et al. (2001). Thoroughly modern worries: The relationship of worries about modernity to reported symptoms, health and medical care utilization. Journal of Psychosomatic Research, 51, 395–401. doi:10.1016/S0022-3999(01)00219-7
Pressman, S. D., & Cohen, S. (2005). Does positive affect influence health? Psychological Bulletin, 131, 925–971. doi:10.1037/0033-2909.131.6.925
Rauma, P. H., Koivumaa-Honkanen, H., Williams, L. J., Tuppurainen, M. T., Kröger, H. P., & Honkanen, R. J. (2014). Life satisfaction and bone mineral density among postmenopausal women: Cross-sectional and longitudinal associations. Psychosomatic Medicine, 76, 709–715. doi:10.1097/PSY.0000000000000114
Roberts, B. W., Kuncel, N. R., Shiner, R., Caspi, A., & Goldberg, L. R. (2007). The power of personality: The comparative validity of personality traits, socioeconomic status, and cognitive ability for predicting important life outcomes. Perspectives on Psychological Science, 2, 313–345. doi:10.1111/j.1745-6916.2007.00047.x
Russell, J. A. (1980). A circumplex model of affect. Journal of Personality and Social Psychology, 39, 1161–1178. doi:10.1037/h0077714
Salovey, P., Rothman, A. J., Detweiler, J. B., & Steward, W. T. (2000). Emotional states and physical health. American Psychologist, 55, 110–121. doi:10.1037/0003-066X.55.1.110
Sapolsky, R. M. (1999). The physiology and pathophysiology of unhappiness. In D. Kahneman, E. Diener, & N. Schwarz (Eds.), Well-Being: The Foundations of Hedonic Psychology (pp. 453–469). New York, NY: The Russell Sage Foundation.
Schwartz, J., & Stone, A. (1998). Strategies for analyzing ecological momentary assessment data. Health Psychology, 17, 6–16. doi:10.1037/0278-6133.17.1.6
Schwarz, N., & Strack, F. (1999). Reports of subjective well-being: Judgmental processes and their methodological implications. In D. Kabneman, E. Diener, & N. Schwarz (Eds.), Well-being: The Foundations of Hedonic Psychology (pp. 61–84). New York: Russell Sage Foundation.
Shiffman, S., Stone, A. A., & Hufford, M. R. (2008). Ecological momentary assessment. Annual Review of Clinical Psychology, 4, 1–32. doi:10.1146/annurev.clinpsy.3.022806.091415
Shin, D. C., & Johnson, D. M. (1978). Avowed happiness as an overall assessment of the quality of life. Social Indicators Research, 5, 475–492. doi:10.1007/BF00352944
Shipley, B. A., Weiss, A., Der, G., Taylor, M. D., & Deary, I. J. (2007). Neuroticism, extraversion, and mortality in the UK Health and Lifestyle Survey: A 21-year prospective cohort study. Psychosomatic Medicine, 69, 923–931. doi:10.1097/PSY.0b013e31815abf83
Siahpush, M., Spittal, M., & Singh, G. K. (2008). Happiness and life satisfaction prospectively predict self-rated health, physical health, and the presence of limiting, long-term health conditions. American Journal of Health Promotion, 23, 18–26. doi:10.4278/ajhp.061023137
Smith, C. A., Haynes, K. N., Lazarus, R. S., & Pope, L. K. (1993). In search of the “hot” cognitions: Attributions, appraisals, and their relation to emotion. Journal of Personality and Social Psychology, 65, 916–929. doi:10.1037/0022-3514.65.5.916
Smyth, J., & Heron, K. (2012). Health psychology. In M. Mehl & T. Conner (Eds.), Handbook of Research Methods for Studying Daily Life (pp. 569–584). New York, NY: Guilford.
Smyth, J., Ockenfels, M. C., Porter, L., Kirschbaum, C., Hellhammer, D. H., & Stone, A. A. (1998). Stressors and mood measured on a momentary basis are associated with salivary cortisol secretion. Psychoneuroendocrinology, 23, 353–370. doi:10.1016/S0306-4530(98)00008-0
Smyth, J., & Stone, A. (2003). Ecological momentary assessment research in behavioral medicine. Journal of Happiness Studies, 4, 35–52. doi:10.1023/A:1023657221954
Smyth, J., Zawadzki, M., & Gerin, W. (2013). Stress and health: A structural and functional analysis of chronic stress. Social and Personality Psychology Compass, 7, 217–227. doi:10.1111/spc3.12020
Smyth, J., Zawadzki, M., Santuzzi, A., & Filipkowski, K. (2014). Examining the effects of perceived social support on momentary mood and symptom reports in asthma and arthritis patients. Psychology & Health, 29, 813–831. doi:10.1080/08870446.2014.889139
Suldo, S. M., & Huebner, E. S. (2004). Does life satisfaction moderate the effects of stressful life events on psychopathological behavior during adolescence? School Psychology Quarterly, 19, 93–105. doi:10.1521/scpg.19.2.93.33313
Thomsen, D. K., Mehlsen, M. Y., Olesen, F., Hokland, M., Viidik, A., Avlund, K., et al. (2004). Is there an association between rumination and self-reported physical health? A one-year follow-up in a young and an elderly sample. Journal of Behavioral Medicine, 27, 215–231. doi:10.1023/B:JOBM.0000028496.41492.34
Van Cauter, E. (1990). Diurnal and ultradian rhythms in human endocrine function: Aminireview. Hormone Research in Paediatrics, 34, 45–53. doi:10.1159/000181794
van Eck, M., Berkhof, H., Nicolson, N., & Sulon, J. (1996). The effects of perceived stress, traits, mood states, and stressful daily events on salivary cortisol. Psychosomatic Medicine, 58, 447–458. doi:10.1037/a0032736.
Veenhoven, R. (2008). Healthy happiness: Effects of happiness on physical health and the consequences for preventive health care. Journal of Happiness Studies, 9, 449–469. doi:10.1007/s10902-006-9042-1
Watson, D. (1988). Intraindividual and interindividual analyses of positive and negative affect: Their relation to health complaints, perceived stress, and daily activities. Journal of Personality and Social Psychology, 54, 1020–1030. doi:10.1037/0022-3514.54.6.1020
Xu, J., & Roberts, R. E. (2010). The power of positive emotions: It’s a matter of life or death—Subjective well-being and longevity over 28 years in a general population. Health Psychology, 29, 9–19. doi:10.1037/a0016767
Acknowledgments
Partial support for the collection of data was provided by the Gallup Organization.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Joshua M. Smyth, Matthew J. Zawadzki, Vanessa Juth, and Christopher N. Sciamanna declares that they have no conflict of interest.
Human and animal rights and Informed consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all patients for being included in the study
Rights and permissions
About this article

Cite this article
Smyth, J.M., Zawadzki, M.J., Juth, V. et al. Global life satisfaction predicts ambulatory affect, stress, and cortisol in daily life in working adults. J Behav Med 40, 320–331 (2017). https://doi.org/10.1007/s10865-016-9790-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10865-016-9790-2