
Abstract
Religiousness has been observed to have a beneficial relationship with blood pressure, however, specific aspects of religiousness that interact with physiological mechanisms to influence this relationship are not known. This study explored laboratory cardiovascular reactivity (blood pressure, heart rate) to psychological stress among middle aged community dwelling individuals grouped by religious motivation (Intrinsic, Pro-religious, Non-religious). Measures of personality, cynical hostility, aggression, sense of coherence, and compassion were administered. Results indicated that the Pro-religious group demonstrated dampened reactivity compared to the other research groups. However, the Pro-religious also demonstrated a less positive psychological profile (e.g., greater cynicism, aggression, and neuroticism; less compassion and sense of coherence) and poorer self-reported health compared with the Intrinsic group and behavioral observations demonstrated that the Pro-religious were unreliable in keeping appointments and appeared rushed during the experiment. These findings indicate a complicated interface between personality, coping, and religious motivation in response to stressors and emphasize the need for naturalistic and longitudinal investigations of individuals who vary in terms of religious motivation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The rate of publication of empirical investigations of the relationship between religiousness/spirituality (R/S) and health has increased in recent years. Masters (2007) observed that in the 5 years between 1975 and 1979, fewer than 100 published articles were located that dealt with this topic, i.e., less than 20 per year; whereas for the seven years between 2000 and 2006, more than 650 were identified, approximately 93 per year. Another development has been an increased emphasis on understanding the nuances of the R/S-health relationship. Though large epidemiological studies have been, and remain, vitally important to establishing the size and robustness of the relationship, recent work has begun probing specific areas of health in relation to particular aspects of R/S (i.e., what aspects of R/S relate to what indices of health/illness?). The present study continues this trend.
One area that has received significant attention addresses the relations between various indicators of R/S and cardiovascular functioning and disease. Chida et al. (2009) provided the first meta-analytic demonstration that R/S was negatively associated with cardiovascular mortality in healthy population studies. Masters (in press) published a narrative review of the cardiovascular-R/S literature across many indicators of both cardiovascular disease (e.g., cardiovascular mortality, recurrent coronary artery disease, recovery from cardiac surgery) and R/S (e.g., religious service attendance, denomination, degree of orthodoxy, impact on health behaviors). He found evidence of a broad protective effect for R/S across diverse populations and R/S constructs. Particularly interesting for development of explanatory models was a strong association between R/S and lack of engagement in risky health behaviors. Specifically, higher levels of R/S predicted less likelihood of smoking and only moderate consumption of alcohol. But it is noteworthy that these behaviors did not completely explain the R/S-cardiovascular health relationship. Other discussed mechanisms included religiously based social support, greater adherence to medical treatment regimens, participation in a healthy lifestyle that includes engagement in positive health behaviors (e.g., exercise), and the influence of psychological pathways relevant to R/S (e.g., forgiveness, compassion, sense of coherence, hope, optimism, self-regulation and self-control, conscientiousness, and reduced anger or hostility) on cardiovascular outcomes. A recent line of work investigated relations between R/S and personality constructs. Conscientiousness (Kern & Friedman, 2008) and neuroticism (Lahey, 2009) have reasonably well established relations with health and longevity. Evidence indicates that intrinsic religiousness (see below) is associated positively with conscientiousness and agreeableness and negatively with neuroticism (McCullough et al., 2003; Saroglou & Fiasse, 2003; Saroglou & Muñoz-García, 2008; Saucier & Skrzypinska, 2006; Bergin et al., 1987). McCullough and Willoughby (2009) noted that agreeableness and conscientiousness form the personality substrates of self-control and their review suggests that self-control and self-regulation are pathways through which religion influences health outcomes.
R/S and hypertension
Hypertension is a particularly important indicator of cardiovascular dysfunction and a major risk factor for premature death, myocardial infarction (MI), stroke, congestive heart failure, vision loss, and erectile dysfunction and is a leading cause of kidney failure (American Heart Association, 2011). Approximately one in three U.S. adults has hypertension with the risk doubling for each 20/10 mmHg increase over 115/75 mmHg (Heart Disease and Stroke Statistics 2010 Writing Group, 2010). There is some evidence, however, of a positive relationship between religiousness and lower blood pressure. In a national sample of U.S. adults age 20 years and over, Gillum and Ingram (2006) found that those who attended religious services weekly or more than weekly had lower adjusted hypertension prevalence compared to those who never attended. Seeman et al. (2003) reviewed the literature and determined that there was an overall relationship between religious involvement and lower blood pressure but they also cautioned that many studies used nonrepresentative samples and were cross-sectional. A noticeable limitation is that many of these studies operationalized religiousness on the basis of service attendance or similar unidimensional measures that do not account for the rich multidimensionality of R/S and thus fail to enlighten regarding possible psychological pathways between aspects of R/S and blood pressure. This limitation in earlier studies was brought into sharper focus by the findings of a recent report (Buck et al., 2009). This team investigated blood pressure and hypertension in light of several dimensions of religiousness among over 3,000 individuals included in the Chicago Community Adult Health Study. They found a complex pattern of results wherein the specific findings depended on the particular R/S variable and blood pressure outcome (i.e., systolic, diastolic, hypertension) under consideration. Surprisingly, attendance was not related to outcomes, perhaps due to the relatively young composition of the sample. Of particular interest for our present purposes, belief in the social benefits of attendance (similar to extrinsic religiousness to be discussed later) predicted increased systolic blood pressure. An earlier study by Hixson et al. (1998), however, found a direct beneficial relationship for intrinsic religiosity on blood pressure.
McEwen (1998, 2007) developed the construct of allostasis, i.e., a process by which living organisms maintain biological homeostasis in the face of challenges of both physical and psychological origin. Failure to maintain homeostasis leads to deleterious effects on health. Laboratory based cardiovascular reactivity studies are designed to assess allostasis via assessment of the activity of the cardiovascular system, namely changes in blood pressure and heart rate, in individuals who encounter psychological stressors. McEwen (1998) and Appelhans and Luecken (2006) discuss the intricate connections between cardiac function and the autonomic nervous system and note that the cardiovascular system is the best-studied allostatic system. Further, evidence indicates that exaggerated cardiovascular reactivity to psychological stress is a predictor of preclinical states (e.g., left ventricular mass and blood pressure) and in some cases primary hypertension (Treiber et al., 2003).
R/S and cardiovascular function
To test mechanistic hypotheses regarding R/S and cardiovascular function more directly a small number of studies investigated R/S as a predictor of cardiovascular reactivity to psychological stress. Masters et al. (2004) found that older adults characterized by extrinsic religious motivation demonstrated exaggerated blood pressure reactivity to psychological stressors whereas older intrinsically religious adults experienced a protective effect. Lawler and Younger (2002) studied younger and middle aged adults and similarly found a beneficial effect for intrinsic religiousness for diastolic blood pressure reactivity. Tartaro et al. (2005) found reduced cortisol and blood pressure reactivity among those who had a greater composite R/S scale score. Edmondson et al. (2005) found that higher levels of religious well-being predicted smaller systolic blood pressure reactivity to an interview stressor whereas higher levels of spiritual well-being and existential well-being predicted lower heart rate reactivity. Finally, Bernston et al. (2008) investigated R/S and autonomic cardiac control in a representative sample of 229 participants aged 50–68 years. Findings demonstrated that an R/S composite, but not religious service attendance, predicted cardiac autonomic regulation, parasympathetic cardiac control, and sympathetic cardiac control but not cardiac autonomic balance. Significant relations held after entry of demographic, health behavior, and personality variables into the regression and the effects could not be accounted for by psychological characteristics such as loneliness, perceived stress, social support, hostility, depression, or general satisfaction with others. It was further demonstrated that cardiac autonomic regulation and R/S predicted (negatively) MI and that the relationship between R/S and MI was mediated by autonomic regulation. Though the study was cross-sectional, it provides support for the possibility that R/S may contribute to cardiac health through a high level of cardiac autonomic regulation that may signify enhanced neuroregulatory control of the heart.
An important concern in laboratory reactivity studies pertains to the nature of the stressor and, in particular, the undesirable likelihood that the laboratory stimulus may rarely or perhaps never occur in the real world. This led to recommendations to use more ecologically valid laboratory stressors, such as social or interpersonal stressors (e.g., Larkin et al., 1998). Cardiovascular responses to laboratory tasks that are less interpersonal may not be closely related to responses to tasks that have a larger interpersonal component (Lassner et al., 1994; Smith & O’Keefe, 1988), yet interpersonal events are central to the experience of stress for many people and are the most robust predictor of psychosocial risk in epidemiological studies (Adler & Matthews, 1994). Interpersonal stressors are also highly salient for tests of R/S and reactivity because of the significant emphasis within religious systems on human relationships as exemplified by commandments to, for example, offer a cup of water to anyone in need, love your neighbor as yourself, and even love your enemy. The Christian New Testament teaches that the greatest spiritual gift is love and Williams (1989) suggested that similar teachings across religions may provide the basis for religion to have a dampening effect on reactivity to interpersonal provocation.
Religious motivation
Intrinsic and extrinsic religiousness were briefly mentioned above. These constructs, as characterized by Allport (1950) and operationalized by Allport and Ross (1967) have a substantial history in the psychology of religion. Allport and Ross hypothesized that religious service attendees are not a homogeneous group but their religious motivation may be characterized as being either intrinsic, extrinsic, both, or neither. This work was further clarified by Gorsuch (1994) who defined intrinsic religiousness as: “…the motivation for experiencing and living one’s religious faith for the sake of the faith itself. The person’s religion is an end unto itself, a goal pursued in the absence of external reinforcement” (p. 317). Thus, intrinsically religious individuals embrace a religious creed, internalize it, and attempt to follow it. Attendance at church for the intrinsically religious may be thought of as motivated by desire for spiritual growth in the faith. Extrinsic religiousness, on the other hand, is characteristic of individuals whose motivation for religious involvement is mostly in service of something other than the religion itself, such as enhancing their sense of security or social connections. The ‘mostly’ in the sentence above (and on items that measure extrinsic religious motivation) is important. Certainly intrinsically religious individuals also experience increased security or social connections as a result of their religious involvement but these are not the primary motivating factors in their involvement; they are beneficial but incidental outcomes. This distinction resonates throughout many historical writings on the topic. For example, the Book of Job tells the story of Job, a religious man who is accused by the adversary of being a believer whose faith will diminish if he does not continue to reap the earthly rewards to which he is accustomed. The accusation is, essentially, that Job is extrinsically religious. Similarly William James (1902) discussed firsthand direct religion (intrinsic) versus secondhand institutional religion (extrinsic).
It would seem, based on the definitions and operationalizations cited above, that one could not logically strongly endorse both intrinsic and extrinsic religious motivation simultaneously but there are individuals who do just this and they have become known as the pro-religious. Thus some researchers, including a couple investigating health variables, have investigated groups consisting of the intrinsically religious (high intrinsic, low extrinsic), extrinsically religious (high extrinsic, low intrinsic), pro-religious (high on both), and non-religious (low on both scales) (e.g., Donahue, 1985; Richards, 1991; Smith et al., 2004; Turner-Musa & Wilson, 2006). Little is known about the pro-religious individuals though what research has been done indicates that when dependent variables are religious in nature the pro-religious tend to score similarly to the intrinsically religious. Noting the difficulty distinguishing between pro-religious and intrinsically religious individuals, Hood et al. (1990) utilized an isolation tank methodology (i.e., participant sat in a 10 inch deep hydrated magnesium sulfate solution inside a soundproof tank) and found that intrinsically religious participants were generally more likely to report experiences in religious terms whereas the pro-religious were more likely to report experiences in religious terms only when prompted to do so. Extrinsically religious persons were unlikely to report religious experiences regardless of whether or not they were prompted.
When dependent variables measure something that is not identifiably religious (e.g., self-rated health, dogmatism, cynical hostility) however, there is a consistent tendency for intrinsic and non-religious individuals to score similarly and different from the extrinsic and pro-religious (Donahue, 1985). Further, most research found that intrinsically religious individuals score better on measures of psychological functioning than do extrinsically religious individuals. Previous studies using these religious motivation constructs, or aspects thereof, investigated relations with constructs central to social psychological research (e.g., prejudice, obedience, happiness) and clinical phenomena (e.g., fear of death, anxiety) but health research has been quite limited.
Purpose of the study
The general purpose of this study was to advance specific understanding of the relations between particular aspects R/S and certain physiological processes relevant to health outcomes. Specifically, the study was designed to examine the relations between religious motivation and laboratory based cardiovascular reactivity among a sample of middle to older age adults. Based on results from previous studies in our lab (Masters et al., 1997, 2004) and inference from other research (Chida & Hamer, 2008), it was predicted that there would be a relationship between religious motivation and cardiovascular reactivity such that those characterized by intrinsic and non-religious motivation would demonstrate better cardiovascular reactivity profiles to psychological stress compared with the extrinsic and pro-religious participants. Included in the study were measures of personality variables (NEO Five-Factor Inventory) and characterological constructs (e.g., hostility, aggression, compassion, sense of coherence) that served as covariates to more clearly illuminate the role of religious motivation and also provided informative descriptive and interpretive data regarding the religious motivation groups.
Method
Recruitment and participants
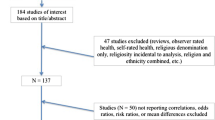
All recruitment and laboratory procedures were approved by the appropriate Institutional Review Board. Participants were self-selected in response to advertisements in local newspapers, physician offices, posted flyers, a monthly (over eight months) announcement in a university employee electronic newsletter, and invitations solicited at meetings of targeted groups consisting primarily of individuals in the required age range. Initial telephone interviews screened respondents on the basis of age and general health. To be included individuals were required to be between the ages of 40 and 70 yrs and be free of any diagnosis of cardiovascular disease, stroke, or hypertension. Eligible individuals were mailed a packet of materials including a brief consent form, the Age Universal Intrinsic/Extrinsic—Revised scale (Gorsuch & McPherson, 1989), 27-item Cook-Medley Hostility Scale (Barefoot et al., 1989), and Buss-Perry Aggression Questionnaire (Buss & Perry, 1992) along with a postage paid return address envelope. Individuals who returned the questionnaires were classified into groups based on religious motivation (Intrinsic, Extrinsic, Pro-religious, Non-religious, see below) and invited to the cardiovascular laboratory to participate in the next phase of the study. Four Non-religious participants declined to participate further once they received the mailed questionnaires. Surprisingly only 7 participants who returned the questionnaires qualified for the Extrinsic group and thus this group was not considered further in the study.
At the laboratory individuals over 60 years were screened for cognitive impairment using the Mini-Mental State Examination (Folstein et al., 1975). Only those who scored 24 or above were eligible for further participation (Hill & Bäckman, 1995). One participant was excluded on this basis and 4 additional participants were excluded because of very high blood pressure readings during baseline assessment (above 165/100, see below). The final sample consisted of 131 participants distributed as follows: 46 Intrinsic, 41 Pro-religious, and 44 Non-religious. They ranged in age from 40 – 70 years (M = 49.99, SD = 6.58) and were mostly Caucasian (85%) with 12% African American. Thirty percent were male and 62% were either married or living with their partner. Thirty seven percent identified as Catholic, 24% as some form of Protestant, 24% as having no religious affiliation, and the rest being Jewish (.8%), Buddhist (1.6%), or other (11.3%).
Measures
Intrinsic/Extrinsic-Revised Scale
Gorsuch and McPherson (1989) designed this 14-item scale to be a more psychometrically robust measure of the intrinsic and extrinsic religious motivation constructs first measured by Allport and Ross’ Religious Orientation Scale (1967). Specific changes include a response format revised to be consistent across all items, inclusion of reverse scored items on the intrinsic scale to counterbalance for acquiescence, and wording edited to be generally applicable across education levels. Factor analyses by the scale developers supported the intrinsic/extrinsic constructs and the final I/E-R consists of separate intrinsic (8 items) and extrinsic (6 items) scales. Alpha reliabilities in the original report were .83 for the intrinsic scale and .65 for the extrinsic. In our sample these coefficients were .82 for intrinsic and .81 for extrinsic. Participants responded to each item indicating whether they strongly agree, tend to agree, are not sure, tend to disagree, or strongly disagree. To make the scale more reader friendly across religious groups we changed the wording of three items substituting “religious services” for “church”. A prototypic item from the intrinsic scale is “My whole approach to life is based on my religion” and prototypic items for the extrinsic scale are “What religion offers me most is comfort in times of trouble and sorrow” or “I go to religious services mainly because I enjoy seeing people I know there.” Scores on each scale were averaged (per item) and individuals were classed into religious motivation groups based on splits made at the midpoint (not median) of the respective scales. Midpoint division has been previously recommended (Donahue, 1985) and serves to promote comparison across samples in different studies and reduces some degree of arbitrariness in scores. Thus classifications were as follows: (a) Intrinsic = average of intrinsic items > 3 and average of extrinsic items < 3; (b) Extrinsic = average of intrinsic items < 3 and average of extrinsic items > 3; (c) Pro-religious = average of both intrinsic and extrinsic items > 3; and d) Non-religious = average of both intrinsic and extrinsic items < 3.
Cook-Medley Hostility Scale
The Cook-Medley Hostility Scale is a 27-item self report measure used to assess various forms of hostility including cynicism, hostile attributions, hostile affect, aggressive responding, and social avoidance (Barefoot et al., 1989). Individuals scoring high on this scale have been shown to have little confidence in others and they perceive others as dishonest, unsocial, and mean (Cook & Medley, 1954). The cynicism component of the hostility scale has further been found to be associated with health problems such as coronary heart disease (Miller et al., 1996). Graham (2006) reported that the Cook-Medley Hostility Scale has been found to be internally consistent (α = .86) and that it has good test–retest reliability (α = .84). In the current study, Cronbach’s α = .69.
Buss-Perry Aggression Questionnaire
The Buss-Perry Aggression Questionnaire is a 29-item self report measure that assesses physical aggression, verbal aggression, anger, and hostility (Buss & Perry, 1992). The developers made reference to the tripartite division (cognitive, affective, and instrumental) of the Buss-Perry Scale and its extension to the personality trait of aggression. The Buss-Perry Aggression Questionnaire has been found to be internally consistent, with total score α = .89 and the total score α for this study = .90. The test–retest reliability over a 9-week period has been reported at .80 for the total scale.
NEO five-factor inventory
The NEO five-factor inventory (NEO-FFI) is a well-established self report measure of personality traits corresponding to the five factor model of personality. The NEO-FFI is a shortened version of the NEO Personality Inventory-Revised (NEO PI-R) and consists of 60 items assessing five domains of personality: (1) neuroticism, (2) extraversion, (3) openness, (4) conscientiousness, and (5) agreeableness. Introversion/extraversion and agreeableness may be key personality variables when looking at the way individuals respond to certain stressors (Miller et al., 1999). The NEO-FFI is highly correlated with the NEO PI-R (correlations ranging between .75 and .89) and it has been found to be internally consistent with values ranging from .74 to .89 (Costa & McCrae, 1992). The Cronbach’s α for this study were .90 for neuroticism, .77 for extraversion, .77 for openness, .78 for conscientiousness, and .82 for agreeableness.
Functional Assessment in Chronic Illness Therapy: Spiritual Well-Being: Expanded Scale (FACIT-SP-EX)
This 23-item self report measure (Brady et al., 1999) builds on the original 12-item Functional Assessment in Chronic Illness Therapy – Spiritual Well-Being – Expanded Scale (FACIT-SP) and was used in this study to measure compassionate attitude based on a subscale consisting of 4 items initially assembled by Steffen and Masters (2005). These are “I feel compassion for others in the difficulties they are facing,” “I feel love for others,” “I feel loved,” and “I feel connected to other people.” Respondents rated how much they agreed with the previous statements by choosing a number on a 5-point Likert type scale of 1 (not at all), 2 (a little bit), 3 (somewhat), 4 (quite a bit), and 5 (very much). Steffen and Masters reported factor analytic support for this 4 item scale and internal consistency estimates in their two studies of, Cronbach’s α = .77 and .78 respectively. The Cronbach α in the present study = .78.
Sense of Coherence Scale
The Sense of Coherence Scale (SOC) was developed by Antonovsky (1987) and consists of a 29 item, five-facet, semantic differential questionnaire. Respondents select a response on a seven-point semantic differential scale with two anchoring phrases. There are 11 comprehensibility, 10 manageability, and 8 meaningfulness items that are summed to arrive at one overall score. Thirteen items are worded negatively and reverse scored. A high score on the SOC expresses a strong sense of coherence. Individuals with a high sense of coherence believe that life is under control, has meaning, and is part of a grand plan and may, therefore, experience less psychological stress. Sense of coherence was formally defined as “a global orientation that expresses the extent to which one has a pervasive, enduring though dynamic feeling of confidence that (1) stimuli deriving from one’s internal and external environments in the course of living are structured, predictable, and explicable; (2) the resources are available to one to offset the demands posed by these stimuli; and (3) these demands are challenges worthy of investment and engagement” (Antonovsky, 1987, p. 19). Antonovsky (1993) summarized the psychometric properties of the SOC as determined from studies around the world. Cronbach’s alpha measures of internal consistency ranged from .82 to .95. The SOC has also been found to have test–retest correlations over a 2 yr period of .54. Finally, evidence from factor analytic studies indicates that the scale best measures one core global orientation construct. In the present study Cronbach’s α = .91.
Evaluation of the confrontation stressor and self-reported health
Participants were asked 4 questions regarding their perception of the confrontation stressor: (1) How realistic was this role-play situation? (2) How realistic was the stress you experienced during the role-play situation? (3) How stressful would encountering this situation be in real life? and (4) How likely is it that you would encounter this situation in real life? Responses were made on a 1 – 10 scale with anchors of “very unlikely (unrealistic)” and “very likely (realistic)”. Finally, participants were asked to rate how they would describe their health in the last month on a scale ranging from one (poor) to five (excellent).
Procedures
Baseline
Participants were instructed to abstain from caffeine (coffee, tea, soda) for 12 h and refrain from smoking cigarettes for at least 1 h prior to their appointment. They were also asked to refrain from any strenuous exercise anytime during the day of their lab session and to consume a light snack 2 h before their appointment. Upon entering the laboratory participants were verbally informed about the study and completed another informed consent document. Participants were then asked to identify the most important person in their lives (e.g., grandchild, wife, husband, son, daughter, etc.) and they completed the NEO-Five Factor Inventory, Sense of Coherence Scale, FACIT-SP-EX compassion scale, and were fitted with a non-invasive automated blood pressure cuff (Accutorr Plus, DataScope, Mahwah, NJ). Upon completion of these scales they entered a 10 min baseline period during which they reviewed National Geographic magazines. Measures of blood pressure (BP) and heart rate (HR) were taken 150 s and 30 s before the end of this baseline and averaged to provide a baseline measure.
Reactivity manipulations
The first of two reactivity manipulations was then introduced (counterbalanced order). All participants completed both tasks consisting of a cognitive stressor (mental arithmetic) and an interpersonal challenge (confrontational role play; preparation for the role play was also treated as a stressor). Verbal behavior was controlled by having participants speak for equal time intervals on both tasks.
The mental arithmetic task required participants to perform three 1 min serial subtraction problems (Cacioppo et al., 1995). They were left alone in the room but told to work as quickly as possible and that their performance would be tape recorded to be compared with others in the study. A visible cassette tape recorder was activated at this time. Measures of BP and HR were triggered at 30 s and 150 s into the task with the two readings averaged to produce a single stressor score for each variable. Immediately following the task participants entered another 10 min baseline period as described above.
The interpersonal challenge (Masters et al., 2004) required participants to role play confrontation with an insurance adjustor who had recently denied payment for a medically necessary intervention (bone marrow transplantation) for the person they had earlier identified as being most important to them. They were told that the coverage was denied because of the expense and because no local providers were authorized by the insurance company to perform bone marrow transplantation even though competent and experienced physicians capable of performing the procedure practice in the area. Participants had 5 min to prepare for the role-play. BP and HR were recorded at 150 s and 30 s before the end of this preparation time and the obtained scores were averaged. They next role-played this scenario for 180 s by placing a phone call to a research assistant they had not seen or met who took on the role of an insurance adjuster. The research assistant was trained and provided with a script of suggested responses (e.g., “You can’t expect me to get personally involved,” “You know, you get what you pay for,” “You just have to play the cards you have been dealt”) and rules (e.g., acting cold, being impersonal). During the role play, measures of BP and HR were taken at 30 s and 150 s. The average of these two scores then produced a single stressor score for this variable. At the conclusion of this task, participants completed 4 questions that assessed their perception of the confrontation stressor and were then paid $20 for their participation.
Data analysis
Preliminary data analysis
Preliminary data analyses using one-way analysis of variance (ANOVA) were conducted to detect differences between the three religious motivation groups (Intrinsic, Pro-religious, and Non-religious) at baseline on measures of BP and HR. Then, consistent with recommendations regarding choice of reactivity indices (Llabre et al., 1991) and previous publications in the field (e.g., Smith et al., 1997; Masters et al., 2004) change scores were calculated by subtracting the appropriate baseline score from the during stressor task score.
Primary data analysis
The reactivity change scores were subjected to a series of 3 × 3 mixed ANOVAs with Religious Motivation as the between-subjects independent variable with three levels and Type of Stressor as a within-subjects independent variable with three levels (cognitive stressor, stress during speech preparation, and stress during speech). Separate analyses were performed for each dependent measure change score (systolic blood pressure [SBP], diastolic blood pressure [DBP], and heart rate [HR]). Examination of these analyses focused on the interaction effects of Religious Motivation and Type of Stressor as well as the main effects of Religious Motivation. Because we were not interested in the main effect of Type of Stressor, when significant Type of Stressor x Religious Motivation interaction effects were not found, consistent with analytic recommendations in the field for improved reliability (Kamarck & Lovallo, 2003; Schwartz et al., 2003), change score data were aggregated across the three stressors and subsequently a one-way ANOVA with Religious Motivation as the independent variable and aggregated reactivity change scores as the dependent variable was conducted. Post-hoc tests were performed to determine group mean differences. Following these analyses, an analysis of covariance (ANCOVA) was conducted with measures of hostility, aggression, compassion, sense of coherence, and personality as covariates.
Exploratory secondary data analyses
To better understand characteristics of the different religious motivation groups exploratory descriptive and inferential analyses were performed with Religious Motivation as the independent variable and scores on the measures of aggression, hostility, personality, sense of coherence, compassion, perception of the confrontation stressor, and self-reported health in the last month as dependent variables. A series of one-way ANOVAs with follow-up Tukey Least Significant Difference (LSD) tests were conducted. Several behavioral observations were also recorded.
Results
Baseline comparisons
Three one-way ANOVAs were conducted to explore baseline differences between the religious motivation groups on measures of SBP, DBP, and HR. The groups did not differ (all ps > .05) on any initial baseline measures (see Table 1).
Cardiovascular reactivity outcomes
SBP
A 3 (Religious Motivation) × 3 (Type of Stressor) mixed-model ANOVA conducted on SBP revealed a non-significant interaction effect, F(4, 248) = 1.77, p = .136. Reactivity change scores were subsequently aggregated across stressors and tested for the effect of Religious Motivation using one-way ANOVA. This revealed a significant effect for Religious Motivation, F(2, 124) = 6.66, p = .002. Post-hoc comparisons using the Tukey LSD method indicated that the mean reactivity score for the Pro-religious group (M = 6.80 Δ mmHg, SD = 8.87) was significantly less than for the Intrinsic (M = 12.42 Δ mmHg, SD = 8.54; d = .65) and the Non-religious (M = 12.98 Δ mmHg, SD = 7.84; d = .74) group mean scores. Mean aggregate change scores are presented in Table 2 and mean aggregate raw scores are found in Table 1.
DBP
The 3 × 3 mixed-model ANOVA for DBP reactivity did not reveal a significant interaction effect for Religious Motivation by Type of Stressor, F(4, 246) = .203, p = .937. Subsequent one-way analysis of the effect of Religious Motivation on the aggregate scores also revealed a non-significant finding, F(2,123) = .751, p = .474, though the pattern found for SBP, of the Pro-religious group having lower levels of reactivity, was again observed (see Table 2).
HR
The findings for HR are similar. The 3 × 3 mixed-model ANOVA did not reveal a significant interaction effect of Religious Motivation and Type of Stressor, F(4, 248) = .747, p = .561. The one-way effect of Religious Motivation on the aggregate scores approached significance, F(2, 124) = 2.82, p = .064. Again it was the Pro-religious group that demonstrated the least reactivity (see Table 2).
Analysis of covariance
To test for the influence of potential covariates on the significant between groups effect for Religious Motivation on SBP measures of cynical hostility, aggression, personality, compassion, and sense of coherence were entered as covariates into a one-way Analysis of covariance (ANCOVA) with Religious Motivation as the independent variable. The significant differences for Religious Motivation remained and none of the covariates reached significance, though Compassion approached it (p = .08).
Exploratory secondary analyses
Because relatively little descriptive research has been conducted on these religious motivation groups, and to better interpret the present findings, we gathered descriptive data on several personality and characterological variables. Did they differ on variables that may influence stress reactivity and more generally may influence their overall approach to life in ways that may have other health ramifications? Means and standard deviations for all variables are shown in Table 3.
Personality
A series of one-way ANOVAs with Religious Motivation as the independent variable and scales of the NEO-FFI as the dependent variables were conducted. The Intrinsic group demonstrated significantly less neuroticism than either the Pro-religious or Non-religious, F(2, 127) = 5.17, p = .007; and greater extraversion than the Non-religious, F(2, 127) = 4.26, p = .015. Both the Pro-religious and Intrinsic groups demonstrated significantly higher agreeableness scores than the Non-religious, F(2, 126) = 6.07; p = .003. No significant differences were found for openness or conscientiousness though in each case the Intrinsic group tended to have the higher score.
Hostility and aggression
One-way ANOVAs performed on the Cook-Medley Hostility Scale and the Buss-Perry Total Aggression score also yielded significant results. Regarding cynical hostility, the Intrinsic group scored lower than both the Pro-religious and Non-religious on the Cook-Medley, F(2, 128) = 4.85, p = .009, and for aggression the Intrinsic group scored lower than the Non-religious on the Buss-Perry, F(2, 127) = 4.43, p = .014.
Compassion and sense of coherence
One way ANOVAs performed on the FACIT-SP-EX compassion scale and the Sense of Coherence scale also demonstrated significant findings. In both cases the Intrinsic group achieved higher scores than both the Pro-religious and Non-religious, F(2, 128) = 8.96, p = .000; F(2, 128) = 8.42, p = .000, respectively.
Evaluation of the confrontation stressor and self-reported health
Overall participants perceived the confrontation stressor as moderately realistic (M = 6.93, SD = 2.48) and similarly rated the realism of the experienced stress (M = 6.55, SD = 2.54). The Religious Motivation groups did not differ on these measures. But there were significant differences in terms of how stressful it would be to encounter this situation in real life, F(2, 126) = 4.65, p = .011 with both the Intrinsic and Non-religious groups finding it more stressful than the Pro-religious (see Table 3). The groups demonstrated a trend toward differences in terms of how likely they believed they would be to encounter this situation in real life, F(2, 126) = 2.55, p = .08, again with the Pro-religious (M = 5.45, SD = 2.76) scoring lower than the Intrinsic (M = 6.02, SD = 2.86) and Non-religious (M = 6.79, SD = 2.51). Intrinsic participants rated their health in the last month as significantly better than the Pro-religious, F(2, 128) = 3.12, p = .04.
Behavioral observations
Several serendipitous behavioral observations were made during the conduct of this study pertaining to the Pro-religious group. First, 20 participants who returned initial surveys and qualified for the study from that group could not subsequently be contacted to schedule a research appointment despite repeated efforts, whereas this virtually never happened for the Intrinsic and Non-religious groups. They failed to return e-mails and even had phones that were disconnected. Second, completion of data collection was delayed several weeks because research assistants had a very difficult time getting the Pro-religious participants to keep their appointments. These appointments were often rescheduled several times but in many cases they ultimately resulted in the subjects never coming to the lab. Interestingly, once appointments were scheduled these individuals insisted that they wanted to complete the study but with regularity no-showed or canceled appointments only to reschedule at a later date. Finally, research assistants, who were blind to experimental condition, commented that “these last participants” (i.e., the Pro-religious) seemed rushed and not as invested in the research project as the other (i.e., Intrinsic, Non-religious) participants.
Discussion
This study was designed to examine differences in cardiovascular reactivity to laboratory stress between different religious motivation groups of middle aged adults. Also included were measures of personality and relevant characterological traits that provided descriptive information of the groups. We predicted that the Intrinsic and Non-religious groups would show the least amount of cardiovascular reactivity to laboratory stressors but, contrary to predictions, the Pro-religious group actually demonstrated the least reactivity. Pro-religious individuals, as classified in this study, had to score above the mid-point on both intrinsic and extrinsic scales of religious motivation. Many previous investigations have demonstrated generally worse psychological functioning related to extrinsic religiousness (Masters & Bergin, 1992; Smith et al., 2003) and one study demonstrated exaggerated cardiovascular reactivity among older adults characterized as extrinsically religious (Masters, et al., 2004), a component of pro-religiousness. Though no previous studies had directly investigated reactivity among Pro-religious individuals, a previous unpublished study in our lab (Masters et al., 1997) revealed that Pro-religious college students scored higher than Intrinsic students on measures of cynical hostility (a finding supported in the present study). Given the previously established positive relationship between hostility and reactivity (Chida & Hamer, 2008) and the presence of extrinsic religious motivation in the composition of pro-religiousness, we expected greater reactivity from the Pro-religious group.
It is not clear why the Pro-religious group demonstrated the lowest levels of cardiovascular reactivity but several intriguing observations are worthy of further exploration. First it may be that individuals characterized by Pro-religious motivation derive benefits associated with both intrinsic (e.g., sense of meaning, belief, sense of coherence) and extrinsic (e.g., social contacts, religious comfort) religious motivations and that these characteristics allow them to be well-defended when facing stressful events. Arguing against such an interpretation, however, are the findings that the Pro-religious group demonstrated higher levels of cynical hostility and lower levels of sense of coherence and compassion than did the Intrinsic group.
The behavioral observations noted earlier are important to consider. They seem to suggest an interpersonal pattern characterized by failure to follow through on obligations and what appeared to be a somewhat indifferent attitude toward the task that the Pro-religious participants volunteered to complete. In this regard it is interesting that the Pro-religious group indicated they would find the confrontation situation less stressful than either the Intrinsic or Non-religious participants were they to encounter it in their real life. These related findings suggest that the Pro-religious group may be less empathic than the other groups but no self report measures of empathy were employed in this study. The differences regarding compassion, however, lend a measure of support to this hypothesis. It is also notable that the Pro-religious group scored higher than either the Intrinsic or Non-religious on neuroticism. Chida and Hamer (2008) in their meta-analysis of reactivity studies found that neuroticism was associated with decreased cardiovascular reactivity but delayed (i.e., worse) cardiovascular recovery. They hypothesized that individuals characterized by higher levels of neuroticism may, as a result of experiencing chronic arousal, have exhausted underlying physiological pathways thus resulting in decreased reactivity though this hypothesis is clearly speculative.
We must consider whether the behaviors/characteristics exhibited by the Pro-religious individuals generalize and are typical of their daily lives, the routine ways they function in stressful situations, or if they are idiosyncratic to the research environment. Presently there is no way to confidently answer this question. Martin Orne (1962) many years ago began his classic discussions on the social psychology of the experiment and noted the unique situations that research participants find themselves in and how they often react to them in an active and reasonable manner but one that might not be what the experimenter intended. It is certainly possible that what we saw from these participants is characteristic of them only when they are involved in a task that is peripheral to their lives, has no lasting importance to them, and for which they are guaranteed payment. Nevertheless, their interactions were clearly different than those of the other groups. Their extra-laboratory behavior and psychological test scores suggest at least the possibility that this style of interacting is present in other contexts as well. They may simply fail to thoroughly engage in a careful way many tasks, including potential stressors, presented to them. Whether, when compared with the other groups, the behavioral pattern demonstrated by the Pro-religious of reduced reactivity and a less positive self reported psychological profile is ultimately a predictor of better or worse psychological functioning, naturally occurring cardiovascular reactivity, and health outcomes cannot be known at present. A previous study (Masters & Knestel, 2011), however, demonstrated that Pro-religious individuals rated themselves as less healthy and having higher body mass indexes than Intrinsic individuals and similarly in the present study we found that the Pro-religious rated their health over the past month as worse than the Intrinsic participants.
Another surprising finding in the current investigation was the absence of the Extrinsic religious motivation group. The project was designed to include four religious motivation groups and an earlier study (Masters & Knestel, 2011) determined that the local population consisted of approximately 22% individuals who could be classified as extrinsic. Further, Masters et al. (2004) had no trouble recruiting younger and older extrinsically religious individuals for a similar study. In the present study, however, only 3.3% of the returned I/E-R questionnaires displayed an extrinsic profile. Our recruitment methods were reasonably comprehensive. We have no adequate explanation for the failure of extrinsically motivated individuals to respond but encourage further investigation.
There are several limitations of this study that deserve consideration. First, as just mentioned, the failure to recruit extrinsically religiously motivated participants eliminated any chance to include them in comparisons of the religious motivation groups. Thus a major goal of this study, i.e., the inclusion of all four religious groups, was not achieved. Second, some may question the use of the religious group paradigm and suggest, instead, that the intrinsic and extrinsic scales be examined individually without regard to religious motivation grouping. Though the psychometric examinations necessary to support, on that basis alone, the formation of the religious groups have not been performed we, like many previous investigators cited throughout, believe that there is merit in considering individuals classified according to this structure and that the results of this and previous investigations suggest that this continues to be a fruitful method of investigation. It is quite unlikely, for example, that we would have accurately been able to relate the behavioral differences we observed to the intrinsic and extrinsic scales in the absence of employing the religious motivation grouping. Space does not permit a detailed discussion of the philosophic and analytic issues involved with this possible concern but we recommend that future investigations employ a variety of methods of analysis of the intrinsic and extrinsic constructs. Third, all laboratory reactivity studies suffer from the limitations inherent in attempting to create in the laboratory stressful situations that have relevance to real world experiences. This is a topic that, in itself, is worthy of much more critique and analysis but is beyond what can be done in this report. We also note our sample was geographically restricted and included oversampling of Catholic participants and undersampling of other religious affiliations relative to the U.S. population (Pew Research Center, 2008). The sample was also largely Caucasian and female. We do not know how these restrictions may limit the generalizability of our findings.
Our results portray the puzzling finding that Pro-religious individuals demonstrate dampened cardiovascular reactivity in the laboratory though simultaneously exhibit psychological profiles that appear less healthy than those found for the Intrinsically religiously motivated. Little is known regarding how individuals who are variously religiously motivated respond to stress in real world situations or how they adjust psychologically to their environments. Further, the likelihood that individuals evolve through different religious motivation groups as their lives develop is strong. Thus, in addition to better controlled laboratory studies that include not only reactivity to psychological stressors but recovery as well, we further recommend longitudinal and naturalistic evaluation of religiously motivated individuals in terms of their ability to cope with stress and engage their world and how this influences their health status.
References
Adler, N., & Matthews, K. A. (1994). Health psychology: Why do some people get sick and some stay well? Annual Review of Psychology, 45, 229–259.
Allport, G. W. (1950). The individual and his religion: A psychological interpretation. New York: Macmillan.
Allport, G. W., & Ross, J. M. (1967). Personal religious orientation and prejudice. Journal of Personality and Social Psychology, 5, 432–443.
American Heart Association. (2011). Why blood pressure matters. Retrieved March 30, 2011 from http://www.heart.org/HEARTORG/Conditions/HighBloodPressure/WhyBloodPressureMatters/Why-Blood-Pressure-Matters_UCM_002051_Article.jsp.
Antonovsky, A. (1987). Unraveling the mystery of health. San Francisco: Jossey-Bass Pub.
Antonovsky, A. (1993). The structure and properties of the sense of coherence scale. Social Science and Medicine, 36, 725–733.
Appelhans, B. M., & Luecken, L. J. (2006). Heart rate variability as an index of regulated emotional responding. Review of General Psychology, 10, 229–240.
Barefoot, J. C., Dodge, K. A., Peterson, B. L., & Dahlstrom, W. G. (1989). The Cook-Medley Hostility Scale: Item content and ability to predict survival. Psychosomatic Medicine, 51, 46–57.
Bergin, A. E., Masters, K. S., & Richards, P. S. (1987). Religiousness and mental health reconsidered: A study of an intrinsically religious sample. Journal of Counseling Psychology, 34, 197–204.
Bernston, G. G., Norman, G. J., Hawkley, L. C., & Cacioppo, J. T. (2008). Spirituality and autonomic cardiac control. Annals of Behavioral Medicine, 35, 198–208.
Brady, M.J., Peterman, A.H., Finchett, G., & Cella, D. (1999). The expanded version of the Functional Assessment of Chronic Illness Therapy-Spiritual Well-Being Scale (FACIT-Sp-Ex): Initial report of psychometric properties. Paper presented at the Annual Meeting of the Society of Behavioral Medicine, San Diego, CA.
Buck, A. C., Williams, D. R., Musick, M. A., & Sternthal, M. J. (2009). An examination of the relationship between multiple dimensions of religiosity, blood pressure, and hypertension. Social Science and Medicine, 68, 314–322.
Buss, A. H., & Perry, M. (1992). The Aggression Questionnaire. Journal of Personality and Social Psychology, 63, 452–459.
Cacioppo, J. T., Malarkey, W. B., Kiecolt-Glaser, J. K., Uchino, B. N., Sgoutas-Emch, S. A., Sheridan, J. F., et al. (1995). Heterogeneity in neuroendocrine and immune responses to brief psychological stressors as a function of autonomic cardiac activation. Psychosomatic Medicine, 57, 154–164.
Chida, Y., & Hamer, M. (2008). Chronic psychosocial factors and acute physiological responses to laboratory-induced stress in healthy populations: A quantitative review of 30 years of investigations. Psychological Bulletin, 134, 829–885.
Chida, Y., Steptoe, A., & Powell, L. H. (2009). Religiosity/spirituality and mortality. Psychotherapy and Psychosomatics, 78, 81–90.
Cook, W. W., & Medley, D. M. (1954). Proposed hostility and pharisaic-virtue scales for the MMPI. The Journal of Applied Psychology, 38, 414–418.
Costa, P. T., Jr., & McCrae, R. R. (1992). Neo PI-R professional manual. Lutz, FL: Psychological Assessment Resources, Inc.
Donahue, M. J. (1985). Intrinsic and extrinsic religiousness: Review and meta-analysis. Journal of Personality and Social Psychology, 48, 400–419.
Edmondson, K. A., Lawler, K. A., Jobe, R. L., Younger, J. W., Piferi, R. L., & Jones, W. H. (2005). Spirituality predicts health and cardiovascular responses to stress in young adult women. Journal of Religion and Health, 44, 161–171.
Folstein, M. G., Folstein, S. E., & McHugh, P. R. (1975). Mini-mental state: A practical method of grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12, 189–198.
Gillum, R. F., & Ingram, D. D. (2006). Frequency of attendance at religious services, hypertension, and blood pressure: The Third National Health and Nutrition Examination Survey. Psychosomatic Medicine, 68, 382–385.
Gorsuch, R. L. (1994). Toward motivational theories of intrinsic religious commitment. Journal for the Scientific Study of Religion, 33, 315–325.
Gorsuch, R. L., & McPherson, S. E. (1989). Intrinsic/extrinsic measurement: I/E-Revised and single-item scales. Journal for the Scientific Study of Religion, 28, 348–354.
Graham, J. R. (2006). MMPI-2: Assessing personality and psychopathology (4th ed.). New York: Oxford University Press.
Heart Disease and Stroke Statistics 2010 Writing Group. (2010). Heart disease and stroke statistics–2010 update: A report from the American Heart Association. Circulation, 121, e46–e215.
Hill, R. D., & Bäckman, L. (1995). The relationship between the Mini-Mental State Examination and cognitive functioning in normal elderly adults: A componential analysis. Age and Ageing, 24, 440–446.
Hixson, K. A., Gruchow, H. W., & Morgan, D. W. (1998). The relation between religiosity, selected health behaviors, and blood pressure among adult females. Preventive Medicine, 27, 545–552.
Hood, R. W., Morris, R. J., & Watson, P. J. (1990). Quasi-experimental elicitation of the differential report of religious experience among intrinsic and indiscriminately pro-religious types. Journal for the Scientific Study of Religion, 29, 164–172.
James, W. (1902). The varieties of religious experience. New York: Random House.
Kamarck, T. W., & Lovallo, W. R. (2003). Cardiovascular reactivity to psychological challenge: Conceptual and measurement considerations. Psychosomatic Medicine, 65, 9–21.
Kern, M. L., & Friedman, H. S. (2008). Do conscientious individuals live longer? A quantitative review. Health Psychology, 27, 505–512.
Lahey, B. B. (2009). Public health significance of neuroticism. American Psychologist, 64, 241–256.
Larkin, K. T., Semenchuk, E. M., Frazer, N. L., Suchday, S., & Taylor, R. L. (1998). Cardiovascular and behavioral response to social confrontation: Measuring real-life stress in the laboratory. Annals of Behavioral Medicine, 20, 294–301.
Lassner, J. B., Matthews, K. A., & Stoney, C. M. (1994). Are cardiovascular reactors to asocial stress also reactors to social stress? Journal of Personality and Social Psychology, 66, 69–77.
Lawler, K. A., & Younger, J. W. (2002). Theobiology: An analysis of spirituality, cardiovascular responses, stress, mood, and physical health. Journal of Religion and Health, 41, 347–362.
Llabre, M. M., Spitzer, S. B., Saab, P. G., Ironson, G. H., & Schneiderman, N. (1991). The reliability and specificity of delta versus residualized change as measures of cardiovascular reactivity to behavioral challenges. Psychophysiology, 28, 701–711.
Masters, K. S. (2007). Religiosity/spirituality and behavioral medicine: Investigations concerning the integration of spirit with body. Journal of Behavioral Medicine, 30, 287–289.
Masters, K. S. (in press). Religion, spirituality, and cardiovascular disease. In S. Waldstein, K. Kaatzel, & W. Kop (Eds.). Handbook of cardiovascular behavioral medicine. Springer: New York.
Masters, K. S., & Bergin, A. E. (1992). Religious orientation and mental health. In J. F. Schumaker (Ed.), Religion and mental health (pp. 221–232). London: Oxford University Press.
Masters, K. S., Hill, R. D., Kircher, J. C., Lensegrav Benson, T. L., & Fallon, J. A. (2004). Religious orientation, aging, and blood pressure reactivity to interpersonal and cognitive stressors. Annals of Behavioral Medicine, 28, 171–178.
Masters, K. S., Ives, D. E., & Shearer, D. S. (1997). Religious orientation as a mediator of hostility. Paper presented at the 105th annual convention of the American Psychological Association, Chicago, IL.
Masters, K. S., & Knestel, A. (2011). Religious orientation among a random sample of community-dwelling adults: Relations with health status and health-relevant behaviors. The International Journal for the Psychology of Religion, 21, 63–76.
McCullough, M. E., Tsang, J., & Brion, S. (2003). Personality traits in adolescence as predictors of religiousness in early adulthood: Findings from the Terman longitudinal study. Personality and Social Psychology Bulletin, 29, 980–991.
McCullough, M. E., & Willoughby, B. L. B. (2009). Religion, self-regulation, and self-control: Associations, explanations, and implications. Psychological Bulletin, 135, 69–93.
McEwen, B. S. (1998). Protective and damaging effects of stress mediators. New England Journal of Medicine, 338, 171–179.
McEwen, B. S. (2007). Physiology and neurobiology of stress and adaptation: Central role of the brain. Physiological Review, 87, 873–904.
Miller, G. E., Cohen, S., Rabin, B. S., Skoner, D. P., & Doyle, W. J. (1999). Personality and tonic cardiovascular, neuroendocrine, and immune parameters. Brain, Behavior, and Immunity, 13, 109–123.
Miller, T. Q., Smith, T. W., Turner, C. W., Guijarro, M. L., & Hallet, A. J. (1996). A meta-analytic review of research on hostility and physical health. Psychological Bulletin, 119, 322–348.
Orne, M. T. (1962). On the social psychology of the psychological experiment: With particular reference to demand characteristics and their implications. American Psychologist, 17, 776–783.
Pew Research Center. (2008). US religious landscape survey: The Pew Forum on Religion and Public Life; 2008. Retrieved December 23, 2008 from http://religions.pewforum.org/.
Richards, P. S. (1991). Religious devoutness in college students: Relations with emotional adjustment and psychological separation from parents. Journal of Counseling Psychology, 38, 189–196.
Saroglou, V., & Fiasse, L. (2003). Birth order, personality, and religion: A study among young adults from a three-sibling family. Personality and Individual Differences, 35, 19–29.
Saroglou, V., & Muñoz-García, A. (2008). Individual differences in religion and spirituality: An issue of personality traits and/or values. Journal for the Scientific Study of Religion, 47, 83–101.
Saucier, G., & Skrzypińska, K. (2006). Spiritual but not religious? Evidence for two independent dispositions. Journal of Personality, 74, 1257–1292.
Schwartz, A. R., Gerin, W., Davidson, K. W., Pickering, T. G., Brosschot, J. F., Thayer, J. F., et al. (2003). Toward a causal model of cardiovascular responses to stress and the development of cardiovascular disease. Psychosomatic Medicine, 65, 22–35.
Seeman, T. E., Dubin, L. F., & Seeman, M. (2003). Religiosity/spirituality and health: A critical review of the evidence for biological pathways. American Psychologist, 58, 53–63.
Smith, T. B., McCullough, M. E., & Poll, J. (2003). Religiousness and depression: Evidence for a main effect and the moderating influence of stressful life events. Psychological Bulletin, 129, 614–636.
Smith, T. W., Nealey, J. B., Kircher, J. C., & Limon, J. P. (1997). Social determinants of cardiovascular reactivity: Effects of incentive to exert influence and evaluate threat. Psychophysiology, 34, 65–73.
Smith, T. W., & O’Keefe, J. L. (1988). Cross-situational consistency of cardiovascular reactivity. Biological Pathways, 27, 237–243.
Smith, M. H., Richards, P. S., & Maglio, C. J. (2004). Examining the relationship between religious orientation and eating disturbances. Eating Behaviors, 5, 171–180.
Steffen, P. R., & Masters, K. S. (2005). Does compassion mediate the intrinsic religion-health relationship? Annals of Behavioral Medicine, 30, 217–223.
Tartaro, J., Luecken, L. J., & Gunn, H. E. (2005). Exploring heart and soul: Effects of religiosity/spirituality and gender on blood pressure and cortisol stress responses. Journal of Health Psychology, 10, 753–766.
Treiber, F. A., Kamarck, T., Schneiderman, N., Sheffield, D., Kapuku, G., & Taylor, T. (2003). Cardiovascular reactivity and development of preclinical and clinical disease states. Psychosomatic Medicine, 65, 46–62.
Turner-Musa, J. O., & Wilson, S. A. (2006). Religious orientation and social support on health- promoting behaviors of African American college students. Journal of Community Psychology, 34, 105–115.
Williams, R. (1989). The trusting heart. New York: Times Books.
Acknowledgments
The authors wish to thank Ralph W. Emerson IV and Stephanie A. Hooker for their assistance on this project. This research was supported by funding from the College of Arts and Sciences, Syracuse University.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Masters, K.S., Knestel, A. Religious motivation and cardiovascular reactivity among middle aged adults: is being pro-religious really that good for you?. J Behav Med 34, 449–461 (2011). https://doi.org/10.1007/s10865-011-9352-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10865-011-9352-6