
Abstract
This study evaluated the efficacy of a brief integrative multiple behavior intervention and assessed risk factors as mediators of behavioral outcomes among older adolescents. A randomized controlled trial was conducted with participants randomly assigned to either a brief intervention or standard care control with 3-month follow-up. A total of 479 students attending two public high schools participated. Participants receiving the intervention showed a significant reduction in quantity × frequency of alcohol use, and increases in fruit and vegetable consumption and frequency of relaxation activities, compared to those receiving the control, P’s = .01. No effects were found on cigarette and marijuana use, exercise and sleep. Effect sizes were small with alcohol use cessation effects reaching medium size. Intervention effects were mediated by changes in peer influenceability for alcohol use, and self-efficacy and self-image for health promoting behaviors. Findings suggest that the brief intervention resulted in health risk and promoting behavior improvements for adolescents, with outcomes mediated by several risk factors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
National health behavior surveillance indicates that significant proportions of older adolescents engage in behaviors that increase their likelihood of injury and death, as well as future chronic disease (Center for Disease Control and Prevention, [CDC] 2008). Common adolescent risk behaviors and problems include alcohol, tobacco and other drug use, physical inactivity, poor nutrition, inadequate sleep, and stress (CDC 2008; Ohayon et al. 2000; Rushton et al. 2002; Stuart 2006). Other US epidemiologic data indicate that the vast majority of adolescents simultaneously engage in multiple risk behaviors (Eaton et al. 2006).
Not surprisingly, interest in interventions targeting concurrent health behaviors has been growing (Atkins and Clancy 2004; Orleans 2004; Prochaska et al. 2008), with some stating that research on these types of interventions could offer the best way to advance public health practice and science (Nigg et al. 2002). Still, few studies have evaluated innovative prevention interventions that target multiple risk behaviors prevalent among American adolescents. A number of systematic reviews of research examining the effectiveness of brief interventions for reducing risk behaviors have concluded that brief motivational programs are effective in changing single risk behaviors, such as excessive alcohol consumption and cigarette smoking (Dunn et al. 2001; Heather 2002; Kaner et al. 2007; Solberg et al. 2008). An intriguing question is whether multiple health behavior content can be bundled and implemented within single, brief interventions. Brief integrative multiple behavior interventions would have a number of potential advantages over more intensive single behavior interventions, including greater cost-effectiveness and breadth of positive outcomes.
An emerging theoretical framework for planning brief multiple behavior interventions is the Behavior-Image Model (Werch 2007). Unlike common illness or risk-focused models, the Behavior-Image Model is a conceptual paradigm for developing asset-based, holistic health interventions emphasizing positive behavior and image content. The Behavior-Image Model is based on the hypothesis that activating existing or creating new images of others (i.e., social images or prototypes) and of our possible selves (i.e., future self-images) can link and motivate change in divergent health risk and health promoting behaviors. The Behavior-Image Model is also based on self-regulation theory of health (Scheier and Carver 2003), with interventions providing feedback on health behaviors to encourage public commitment to multiple concrete goals leading to improvements in both health risk and promoting behavior self-efficacy and change.
Recent studies have examined the effects of brief multiple behavior interventions that target positive social and self-images associated with engaging in health promoting behaviors like physical activity and healthy eating. Findings from these investigations indicate that youth exposed to image-based brief interventions consisting of a health behavior screen, one-on-one fitness consultation tailored to screen responses, and a goal plan for changing selected health habits demonstrated significant decreases in substance use and increases in one or more health promoting behaviors (Werch et al. 2003, 2005, 2007, 2008a, b). In the only controlled trial to date examining a fitness targeted brief multiple behavior intervention for high school aged adolescents, 604 students were randomized to receive either the brief intervention or minimal intervention control with 3- and 12-month follow-ups (Werch et al. 2005). At 3-month follow-up, adolescents given the integrative intervention showed significant differences in reductions in alcohol consumption behaviors and cigarette smoking, and increases in moderate physical activity. At 12-month follow-up cigarette smoking reductions were maintained, but alcohol and physical activity effects decayed. Unfortunately, this initial intervention trial was limited to evaluating physical activity and substance use outcomes. In addition, no studies were found evaluating multiple behavior interventions for adolescents that assessed mediators of health behavior change. Such analyses could provide valuable information for further tailoring and strengthening of future brief integrative interventions for youth.
The current investigation is only the second randomized trial to evaluate a brief integrative multiple behavior intervention among adolescents targeting fitness and health behavior images. We hypothesized that participating high school students receiving the brief intervention would show significant improvements on both health risk and promoting behaviors compared to those students receiving the standard care control. An exploratory analysis was also conducted examining theoretical risk factors associated with the Behavior-Image Model as possible mediators of behavioral outcomes resulting from the brief intervention. Risk factors included beliefs about the linkage between health risk and health promoting behaviors, perceived peer influence, self-image, and self-efficacy, representing the Behavior-Image Model’s key foci on creating behavior connections, peer and image influences, and self-regulatory processes.
Methods
Design
A randomized controlled trial was conducted using a within-school design at two schools. Participants were randomly assigned to either the brief intervention or standard care control group by computer generated random numbers stratified on baseline drug use (30-day alcohol, cigarette and/or marijuana drug use vs. non-use). Baseline data were collected during fall 2008 and post-intervention data were collected 3-months after intervention in spring 2009. Data were collected from participants assembled in small groups within participating schools by trained project staff following a standardized protocol. The research protocol was Institutional Review Board approved and required both written parental consent and youth assent prior to study participation.
Setting/participants
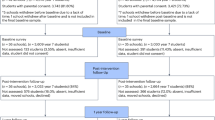
Participants included 479 students attending two public high schools in northeast Florida during fall 2008. Students in the 11th and 12th grades were invited to participate in the research project using formal presentations made in classrooms, cafeterias, auditoriums, and conference rooms regarding study aims, procedures, benefits and risks. Of the 512 adolescents recruited into the study, 93.6% (n = 479) participated in the baseline data collection, with 19 students grade-ineligible and 14 students absent from school. Data were not available to compare the similarity of the sample to other 11th and 12th grade students attending the participating schools. However, the study sample included more females (62% vs. 51%) and fewer white students (27% vs. 33%) than found in the entire population of students enrolled at participating schools. Table 1 details participant characteristics.
Intervention
The intervention, titled Project Active, included a 9-item life skills screen assessing target health behaviors, a one-on-one consultation with slides presenting positive image feedback tailored to screen results, a set of concrete behavioral recommendations for enhancing future fitness, and a personal fitness goal setting and commitment strategy linking positive image attainment with specific health behavior change. Intervention content and strategies were based on the Behavior-Image Model (Werch 2007). In particular, the consultation provided personalized feedback to screening responses on each of the target health behaviors, including the relationship between specific behaviors and favorable image achievement (e.g., I see you engage in at least 30 min of moderate physical activity on most days of the week. Congratulations, you are physically active!). Consultation content emphasized social images and future self-images associated with each of the health promoting behaviors, including moderate physical activity, vigorous exercise, healthy nutrition, sleep, and relaxation techniques, along with messages demonstrating how alcohol, cigarette and illegal drug use interferes with positive image attainment.
Immediately after the consult, participants received standardized recommendations to improve each of the health behaviors and linked these recommendations to positive image outcomes (“Practice at least one relaxation technique daily, if you want to be a stress free and calm young adult”). Lastly, after receiving recommendations, participants were provided with a goal plan and given instructions to check-off one or more health behaviors to improve in the next week within each of five image areas: (1) Being physically active, fit, athletic and vigorous; (2) Looking healthy and strong; (3) Being stress free and calm; (4) Being rested and energetic; and (5) Being alcohol, cigarette and illegal drug-free. Intervention content consisted primarily of printed text (screen, slides and goal setting) and scripted messages (recommendations and consultation) emphasizing words and phrases eliciting vivid images associated with target health behaviors.
The brief intervention was administered during regular school hours in designated study spaces. After randomization, trained personal fitness coaches implemented the intervention using fully scripted protocols. Fitness coaches consisted of nurses and certified health education specialists who received a two-day training that included demonstration, role-playing and feedback on how to implement each of the intervention components. The mean length of time to implement the combined screen, consultation, recommendations and goal setting strategies was approximately 30 min. Contamination was minimized by limiting materials students were given after the intervention to a copy of the goal plan.
Standard care control
The standard care control was a commercially available 15-page booklet titled: “What Everyone Should Know ABOUT WELLNESS” (Channing Bete Company 1992), which included information and illustrations about smoking, alcohol and drug use avoidance, exercise types and benefits, eating nutritious foods, managing stress, getting adequate sleep, and maintaining a positive attitude. Control material was implemented concurrently with the brief interventions within participating schools. Participants assigned to the standard care control were provided with the booklet, placed in a semi-quiet area in the schools, and given instructions to carefully read the booklet at their own pace. Students were observed to determine that they had adequate time to finish reading the booklet. Intervention and control participant interaction was minimized by using separate space within schools during treatment implementation, and by restricting the release of intervention materials that could be shared among participants after intervention implementation.
Main outcome measures
The Health and Fitness Survey (Werch et al. 2008b) was used to collect primary and secondary outcome measures. Measures used in this survey were adopted from those used in previous evaluations of brief multiple behavior interventions (Werch et al. 2007, 2008a). Primary health risk behavior measures included items assessing the frequency and quantity of alcohol, cigarette and marijuana use, scored as 30-day frequency (ranging from 1 = 0 days through 11 = 28–30 days) and 30-day quantity (ranging from 1 = 0 drinks/cigarettes/marijuana times used per day through 12 = 11 or more drinks/31 or more cigarettes/31 or more times using marijuana). These items originated from standardized national drug surveys and were multiplied to obtain a single quantity × frequency index (Bachman et al. 2008; Substance Abuse and Mental Health Services Administration [SAMHSA] 2007).
Primary health promoting behavior measures included exercise, which was assessed using the Leisure-Time Exercise Questionnaire (Godin and Shephard 1985). This measure was determined by multiplying the estimated rate of energy expenditure from reported frequency of participation and adding the two intensity measures (strenuous and moderate) to obtain a summed total score (i.e., 5 × moderate exercise frequency + 9 × strenuous exercise frequency) (U.S. Department of Health and Human Services [USDHHS] 2008). Nutrition was measured as servings of fruits and vegetables usually eaten each day in the past 30 days (ranging from 0 to 9 or more servings), based on public health recommendations (USDHHS and U.S. Department of Agriculture [USDA] 2005). Sleep was assessed using three items measuring number of hours of sleep each night in the past 30 days, how often do you get enough sleep, and number of days getting enough sleep, which were converted into a scale ranging from 0 (low) to 10 (high) and averaged (Cronbach’s alpha = .68). These items were adopted from previous research on sleep patterns (Groeger et al. 2004; Wolfson et al. 2003). Stress management was measured as mean frequency of use of four activities to help relax or prevent stress in the past 30 days, ranging from 1 = never to 4 = always (Cronbach’s alpha = .63). These items were adopted from a measure of health promotion for adolescents (Chen et al. 2003).
Secondary risk factors associated with the Behavior-Image Model (Werch 2007) and used in previous evaluations of brief integrative interventions (Werch et al. 2007, 2008a) included a measure of coupling beliefs assessing perceptions of whether or not alcohol and drugs interfere with five health promoting behaviors (each scored on a four-point Likert scale of yes to no); and self-image, measured as perceived similarity to the type of young adult who regularly practices activities to relax (scored on a four-point Likert scale of very similar to not at all similar). In addition, measures related to Social Cognitive Theory (Bandura 1986) used in previous studies evaluating brief multiple behavior interventions (Werch et al. 2003, 2005) were included in this study. These measures included self-efficacy, assessed as how sure participants felt they could always eat healthy and always practice stress management techniques regularly (each item scored on a four-point Likert scale of very sure to not sure), and peer influenceability measured as, "if friends wanted me to drink a lot of alcohol I would" (scored on a four-point Likert scale of agree a lot to disagree a lot).
Analysis
Analyses were performed using SPSS version 17.0. Preliminary analyses were conducted to determine whether advanced statistical methods were needed to address a possible nested characteristic of the data (i.e., participants clustered within schools). These analyses examined primary outcomes between units (i.e., schools), time and treatment groups. Only one-three-way interaction effect was found, therefore school setting was excluded as a factor to permit a more direct test of treatment by time effects. Repeated measures ANOVAs were used to test intervention effects over time. Outcome measures were combined to limit the number of tests conducted. In addition, we used Bonferroni-adjustments for family-wise comparisons within each behavior grouping, i.e., risk behaviors (P’s < .016) and health promoting behaviors (P’s < .012). Effect sizes were calculated using Morris’s formula (2008). Logistic regressions were then performed to examine intervention effects on improving, initiating, and stopping (for alcohol use only) those behaviors found to differ significantly based on ANOVA tests. The R 2 statistic was used to indicate effect sizes for regressions.
To assess possible mediators of intervention outcomes, only those risk factors associated with significant behavioral outcomes that were also found to differ significantly between treatment groups over time were included in the mediation analysis. The MATRIX mediation analysis approach was used for estimating indirect effects in multiple mediator models as described by Preacher and Hayes (2008). All variables were adjusted for baseline scores. Bootstrapping, a nonparametric resampling procedure, was used for testing mediation effects while controlling for gender. A 95% bias corrected and accelerated confidence interval was run for all analyses. Intervals not containing zero were interpreted as indicating a statistically significant indirect path and evidence of a mediated effect.
Results
Baseline, attrition and item response analyses
No differences were found on any of the socio-demographic or target health behavior measures between treatment groups at baseline (See Table 1). Most participants (94.1%) successfully completed the post-intervention data collection. Of those lost to follow up, 24 participants (85.7%) moved away from school and four (14.3%) were lost due to repeated absence from school, resulting in a total of 451 participants. No differences were found in the proportion of those who dropped out between treatment groups or participating schools.
Attrition analysis of baseline data indicated that dropouts were more likely than non-dropouts to drink (42.9% vs. 21.7%), smoke cigarettes (25.0% vs. 6.0%), skip school 1–2 times a month (25.0% vs. 14.2%), and be absent from school 1–2 times a month (57.1% vs. 27.1%), P’s < .05. Factorial ANOVA and loglinear tests showed no dropout by treatment group interactions on any of the demographic and targeted health behavior measures, with one exception. Dropouts from the control group used marijuana more frequently (m = 2.39, se = .32) than dropouts receiving the intervention (m = 1.00, se = .43), F(1,475) = 5.51, P = .02.
Item response analysis showed that at baseline, 98.2% strongly agreed or agreed they were willing to give honest answers to questions about their alcohol, drug use and other health habits on the outcome survey, and at post-intervention 98.9% strongly agreed or agreed they were willing to give honest answers. No differences were found on willingness to provide truthful responses between treatment groups, indicating little probability that social desirability influenced responses differentially across study arms. To further estimate the extent to which responses may have been unreliable due to participant lying or other factors, we included a bogus/fake drug (i.e., zanatel) among the list of substances that participants were asked if they used in the past 30 days. At baseline, one participant reported using the bogus/fake drug, and two students did so at post-intervention, suggesting that widespread error due to lying or sloppy completion of the data collection instrument was unlikely and did not differ across treatment groups.
Outcome analysis
Table 2 shows means, standard errors and effect sizes of health behavior measures by behavior type for treatment group and time. Significant treatment by time interaction effects were found on one risk behavior measure and two health promoting behavior measures. For risk behaviors, quantity × frequency of alcohol use in the past 30-days declined over time for students receiving the brief intervention and increased for those receiving the standard care control, F(1,447) = 7.46, P = .01. For health promoting behaviors, fruit and vegetable servings increased for participants receiving the brief intervention and decreased for participants receiving the standard care control, F(1,447) = 6.53, P = .01. Likewise, frequency of relaxation activities increased for students receiving the intervention and decreased for those receiving the control, F(1,449) = 6.43, P = .01. Effect sizes for all behavioral outcomes were small. No interaction effects were found for cigarette and marijuana use, exercise, and sleep behavior measures.
Table 3 shows the results of logistic regressions examining alcohol use, fruit and vegetable consumption, and relaxation activity improvement, initiation, and cessation. Regressions showed significant improvements on all three behaviors for those receiving the brief intervention, including significant reductions in alcohol use quantity (B = .61, P < .05), and increases in eating five or more servings of fruits and vegetables (B = .55, P < .05) and practicing relaxation activities (B = .51, P < .01). Those receiving the brief intervention were also less likely to initiate alcohol use (B = −.64, P < .05) and more likely to stop drinking at follow-up (B = 1.00, P < .05). Effects were small (R 2’s = .02) with the exception of alcohol use cessation, which was medium in size (R 2 = .07).
Mediation analysis
Significant treatment group by time interaction effects were found for five risk factors, including two factors for alcohol use, one for nutrition, and two for stress management, P’s < .05. These risk factors included measures of an alcohol coupling belief and peer influenceability to drink alcohol, healthy eating self-efficacy, and items measuring self-image and self-efficacy associated with practicing stress management activities. All risk factors improved over time for participants receiving the brief intervention, and most worsened over time for participants receiving the standard care control.
Table 4 shows the mediation of behavioral effects of the brief intervention through risk factor mediators. For all three behavioral outcomes (i.e., reduced alcohol use, increased fruit and vegetable consumption, and increased frequency of relaxation activities), total indirect effects were found indicating intervention effects on health behaviors were mediated by risk factors. Examination of specific indirect effects showed that a reduction in peer influenceability to drink (CI = .06, .29) was the only mediator of reduced alcohol use quantity × frequency, since its 95% CI did not contain zero. For health promoting behaviors, an increase in healthy eating self-efficacy (CI = .01, .18) mediated greater fruit and vegetable consumption, while both an increase in self-image associated with practicing activities to relax (CI = .01, .19) and stress management self-efficacy (CI = .03, .20) mediated greater frequency of practicing relaxation techniques.
Conclusions
This paper reported findings from only the second randomized controlled trial to evaluate a brief integrative multiple behavior intervention targeting physical activity and health behaviors among high school-aged adolescents, and the first to assess mediators of behavioral outcomes. Multiple behavior interventions are being increasingly recognized as important strategies for addressing concurrent health risks facing American adolescents (Atkins and Clancy 2004; Orleans 2004; Prochaska et al. 2008). Interventions based on the Behavior-Image Model targeting social and self-image represent an innovative approach to bundling multiple risk behavior content in brief formats.
Results from this study demonstrated that the brief intervention produced significant reductions in the quantity × frequency of alcohol use. In addition, the brief intervention reduced quantity of use and initiation of drinking, and increased stopping drinking. These results were small in size, with the exception of stopping drinking which was medium sized, suggesting the brief intervention might have its greatest effects for adolescents who are already drinking. These results support alcohol reductions found in previous brief integrative intervention trials, particularly among those adolescents already engaged in substance use (Werch et al. 2005, 2008b). While a reduction on cigarette smoking was also found among adolescents receiving the brief intervention, these effects were not significant because few adolescents in the study reported smoking cigarettes. However, non-significant increases in marijuana use were found for adolescents in both intervention and control groups. One possible reason for the lack of positive change on marijuana consumption was that the brief intervention did not address marijuana use specifically, but instead emphasized more general illegal drug use. In addition, differential attrition among marijuana users may have accounted in part for the lack of differences between groups on marijuana consumption.
Findings indicated the brief intervention also increased two health enhancing behaviors, fruit and vegetable consumption and frequency of relaxation techniques. Fruit and vegetable consumption increases are important because of their protective role in the prevention of chronic illness such as cardiovascular disease and cancer (Ness and Powles 1997; Key et al. 2004). A review of interventions aimed at increasing fruit and vegetable consumption among children found that most effective programs were multi-component interventions lasting at least 12-months in duration, resulting in an increase of 0.3 to 0.99 servings a day (Knai et al. 2006). The current study’s findings showed adolescents receiving the brief intervention increased their fruit and vegetable consumption by 0.74 servings a day. While this effect was small in size, this finding highlights the potential of a brief intervention for achieving outcomes similar in magnitude to those resulting from more complicated and lengthier programs.
In addition to healthy eating, greater numbers of adolescents receiving the brief intervention increased their frequency of relaxation techniques to manage stress. Although stress is associated with a number of physical and psychological problems experienced by adolescents (Fordwood et al. 2007; McMahon et al. 2003), it is unknown whether or not the small increase in relaxation techniques found in this study reduced stress symptoms among participating youth. Future research is needed evaluating brief interventions targeting broader stress management goals, such as increasing stress awareness and developing a range of coping strategies believed important in youth stress management (Kraag et al. 2009).
Results from the mediation analysis suggested various behavioral outcomes were mediated by different risk factors. Specifically, the brief intervention reduced alcohol use by reducing perceived peer influenceability to drink alcohol. Previous brief multiple behavior interventions have been shown to affect change on peer influenceability (Werch et al. 2003, 2005), further supporting its importance as a possible mediator of brief intervention effects on alcohol use. Peer influenceability was likely affected by intervention content based on the Behavior-Image Model illustrating peer prototypes and future self-images as avoiding alcohol consumption.
However, fruit and vegetable consumption and practicing relaxation activities were affected by the brief intervention through increasing self-efficacy to eat healthy and practice stress management, as well as enhancing self-image as one who regularly uses activities to relax. Previous research has linked self-efficacy to fruit and vegetable consumption among children (Thompson et al. 2007), while self-image improvements have been shown to result from image-based brief interventions (Werch et al. 2007, 2008b). It is possible that intervention content modeling favorable images of adolescents engaged in health promoting behaviors like healthy eating and practicing relaxation, and providing an opportunity to set goals for improving these behaviors, resulted in increases in self-efficacy and positive self-image.
Surprisingly, the brief intervention did not have a significant effect on increasing exercise as has previous brief multiple behavior interventions evaluated among adolescents (Werch et al. 2003, 2005). A small non-significant increase in exercise was seen in this study for those receiving the brief intervention. Given the low level of moderate physical activity practiced by adolescents in this study at baseline, an emphasis should be placed on presenting additional positive images associated with those engaged in moderate versus vigorous physical activity, and providing more concrete behavioral options for engaging in moderate physical activity in future brief interventions for adolescents.
This study was limited to a sample of adolescents from two public high schools in the southeastern US. Additional research is needed to evaluate integrative brief interventions with adolescents from more diverse high school settings, as well as with younger adolescents and children. By itself, this study should be viewed as an early step toward examining the effects of integrative brief image-based multiple behavior interventions on a number of critical health risk and health promoting habits of adolescents. This investigation was also limited to a three-month post-intervention follow-up. Longitudinal investigations are needed with extended follow-up periods to understand the sustainability of multiple behavior outcomes resulting from image-based brief interventions. Lastly, this study was limited to self-reported measures of health behavior without corroborating objective measures. The self-reported measures used in this study, however, have been used in previous research, and results from an analysis of item response indicated no treatment group variation in self-report bias due to social desirability or errors resulting from sloppy completion or deliberate falsification. Nevertheless, future studies evaluating integrative interventions would benefit from including prospective methods of collecting data more frequently, such as a daily diary method.
In conclusion, results from this study demonstrate that a brief integrative multiple behavior intervention resulted in improvements on three diverse health behaviors of adolescents. Positive changes on any one of these critical behaviors could have important implications for the enhancement of health and prevention of disease and injury among adolescents. Meanwhile, adolescents receiving the control showed a decline in all health behaviors, supporting the need for intervention during this important development period. In addition, this study generated critical data for better understanding possible mechanisms for changing multiple health behaviors, permitting more accurate tailoring of future intervention content and components for adolescents.
References
Atkins, D., & Clancy, C. (2004). Multiple risk factors interventions: Are we up to the challenge? American Journal of Preventive Medicine, 27(2 Suppl), 102–103.
Bachman, J. G., Johnston, L. D., & O’Malley, P. M. (2008). Monitoring the Future: Questionnaire responses from the nation’s high school seniors, 2006. Ann Arbor, MI: Institute for Social Research.
Bandura, A. (1986). Social foundations of thought and action: a social cognitive theory. Englewood Cliffs, NJ: Prentice-Hall.
Centers for Disease Control and Prevention. (2008). Youth risk behavior surveillance—United States, 2007. MMWR. Morbidity and Mortality Weekly Report, 57(SS-4), 1–131.
Channing Bete Company. (1992). What everyone should know ABOUT WELLNESS [Brochure]. South Deerfield, MA: Channing Bete Company, Inc.
Chen, M. Y., Wang, E. K., Yang, R. J., & Liou, Y. M. (2003). Adolescent health promotion scale: Development and psychometric testing. Public Health Nursing, 20(2), 104–110.
Dunn, C., Deroo, L., & Rivara, F. P. (2001). The use of brief interventions adapted from motivational interviewing across behavioral domains: A systematic review. Addiction, 96(12), 1725–1742.
Eaton, D. K., Kann, L., Kinchen, S., Hawkins, J., Harris, W. A., Lowry, R., et al. (2006). Youth risk behavior surveillance—United States, 2005. Journal of School Health, 76(7), 353–372.
Fordwood, S. R., Asarnow, J. R., Huizar, D. P., & Reise, S. P. (2007). Suicide attempts among depressed adolescents in primary care. Journal of Clinical Child and Adolescent Psychology, 36(3), 392–404.
Godin, G., & Shephard, R. J. (1985). A simple method to assess exercise behavior in the community. Canadian Journal of Applied Sport Sciences, 10(3), 141–146.
Groeger, J. A., Zijlstra, F. R., & Dijk, D. J. (2004). Sleep quantity, sleep difficulties and their perceived consequences in a representative sample of some 2000 British adults. Journal of Sleep Research, 13(4), 359–371.
Heather, N. (2002). Effectiveness of brief interventions proved beyond reasonable doubt. Addiction, 97(3), 293–294.
Kaner, E. F., Beyer, F., Dickinson, H. O., Pienaar, E., Campbell, F., Schlesinger, C., et al. (2007). Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database of Systematic Reviews, 2, CD004148.
Key, T. J., Schatzkin, A., Willett, W. C., Allen, N. E., Spencer, E. A., & Travis, R. C. (2004). Diet, nutrition and the prevention of cancer. Public Health Nutrition, 7(1A), 187–200.
Knai, C., Pomerleau, J., Lock, K., & McKee, M. (2006). Getting children to eat more fruit and vegetables: A systematic review. Preventive Medicine, 42(2), 85–95.
Kraag, G., Van Breukelen, G. J., Kok, G., & Hosman, C. (2009). ‘Learn Young, Learn Fair’, a stress management program for fifth and sixth graders: Longitudinal results from an experimental study. Journal of Child Psychology and Psychiatry and Allied Disciplines, 50(9), 1185–1195.
McMahon, S. D., Grant, K. E., Compas, B. E., Thurm, A. E., & Ey, S. (2003). Stress and psychopathology in children and adolescents: Is there evidence of specificity? Journal of Child Psychology and Psychiatry and Allied Disciplines, 44(1), 107–133.
Morris, S. B. (2008). Estimating effect sizes from pretest-posttest-control group design. Organizational Research Methods, 11(2), 364–386.
Ness, A. R., & Powles, J. W. (1997). Fruit and vegetables, and cardiovascular disease: A review. International Journal of Epidemiology, 26(1), 1–13.
Nigg, C. R., Allegrante, J. P., & Ory, M. (2002). Theory-comparison and multiple- behavior research: Common themes advancing health behavior research. Health Education Research, 17(5), 670–679.
Ohayon, M. M., Roberts, R. E., Zulley, J., Smirne, S., & Priest, R. G. (2000). Prevalence and patterns of problematic sleep among older adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 39(12), 1549–1556.
Orleans, C. T. (2004). Addressing multiple behavioral health risks in primary care: Broadening the focus of health behavior change research and practice. American Journal of Preventive Medicine, 27(2 Suppl), 1–3.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891.
Prochaska, J. J., Spring, B., & Nigg, C. R. (2008). Multiple health behavior change research: An introduction and overview. Preventive Medicine, 46(3), 181–188.
Rushton, J. L., Forcier, M., & Schectman, R. M. (2002). Epidemiology of depressive symptoms in the National Longitudinal Study of Adolescent Health. Journal of the American Academy of Child and Adolescent Psychiatry, 41(2), 199–205.
Scheier, M. F., & Carver, C. S. (2003). Goals and confidence as self-regulatory elements underlying health and illness behavior. In L. D. Cameron & H. Leventhal (Eds.), The self-regulation of health and illness behaviour (pp. 17–44). New York, NY: Routledge.
Solberg, L. I., Maciosek, M. V., & Edwards, N. M. (2008). Primary care intervention to reduce alcohol misuse ranking its health impact and cost effectiveness. American Journal of Preventive Medicine, 34(2), 143–152.
Stuart, H. (2006). Psychosocial risk clustering in high school students. Social Psychiatry and Psychiatric Epidemiology, 41(6), 498–507.
Substance Abuse and Mental Health Services Administration. (2007). 2008 National survey on drug use and health. Retrieved from http://www.oas.samhsa.gov/nsduh/2k8MRB/2k8Q.pdf.
Thompson, V. J., Bachman, C. M., Baranowski, T., & Cullen, K. W. (2007). Self-efficacy and norm measures for lunch fruit and vegetable consumption are reliable and valid among fifth grade students. Journal of Nutrition Education and Behavior, 39(1), 2–7.
U.S. Department of Health and Human Services. (2008). 2008 Physical Activity Guidelines for Americans. Retrieved from http://www.health.gov/paguidelines/pdf/paguide.pdf.
U.S. Department of Health and Human Services, U.S. Department of Agriculture. (2005). Dietary Guidelines for Americans, 2005. Retrieved from http://www.health.gov/dietaryguidelines/dga2005/document/pdf/DGA2005.pdf.
Werch, C. (2007). The Behavior-Image Model: A paradigm for integrating prevention and health promotion in brief interventions. Health Education Research, 22(5), 677–690.
Werch, C., Bian, H., Moore, M. J., Ames, S., DiClemente, C. C., Thombs, D., et al. (2008a). Brief multiple behavior health interventions for older adolescents. American Journal of Health Promotion, 23(2), 92–96.
Werch, C., Bian, H., Moore, M. J., Ames, S., DiClemente, C. C., & Weiler, R. M. (2007). Brief multiple behavior interventions in a college student health care clinic. Journal of Adolescent Health, 41(6), 577–585.
Werch, C., Moore, M., Bian, H., DiClemente, C. C., Ames, S. C., Weiler, R. M., et al. (2008b). Efficacy of a brief image-based multiple-behavior intervention for college students. Annals of Behavioral Medicine, 36(2), 149–157.
Werch, C., Moore, M., DiClemente, C. C., Bledsoe, R., & Jobli, E. (2005). A multihealth behavior intervention integrating physical activity and substance use prevention for adolescents. Prevention Science, 6(3), 213–226.
Werch, C., Moore, M., DiClemente, C. C., Owen, D. M., Jobli, E., & Bledsoe, R. (2003). A sport-based intervention for preventing alcohol use and promoting physical activity among adolescents. Journal of School Health, 73(10), 380–388.
Wolfson, A. R., Crowley, S. J., Anwer, U., & Bassett, J. L. (2003). Changes in sleep patterns and depressive symptoms in first-time mothers: Last trimester to 1-year postpartum. Behavioral Sleep Medicine, 1(1), 54–67.
Acknowledgments
This investigation and manuscript would not have been possible without the financial support from the National Institute on Alcohol Abuse and Alcoholism (Grant number: AA9283) and the National Institute on Drug Abuse (Grant numbers: DA018872 and DA019172). We also wish to thank the many school administrators, staff, teachers, parents, guardians, and students who made this project possible through their kind support and participation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Werch, C.E., Bian, H., Carlson, J.M. et al. Brief integrative multiple behavior intervention effects and mediators for adolescents. J Behav Med 34, 3–12 (2011). https://doi.org/10.1007/s10865-010-9281-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10865-010-9281-9