
Time estimation was examined in 148 older good and poor sleepers in analogue and naturalistic sleep settings. On analogue tasks, both “empty” time and time listening to an audiobook were overestimated by both good and poor sleepers. There were no differences between groups. “Empty” time was experienced as “dragging.” In the sleep setting, most poor sleepers underestimated nocturnal sleep and overestimated awake times related to their own sleep problem: sleep onset vs. sleep maintenance insomnia. Good sleepers did the opposite. Severity of sleep problem and size of time estimation errors were unrelated. Greater night-to-night wake time variability was experienced by poor than by good sleepers. Psychological adjustment was unrelated to time estimations and to magnification or minimization of sleep problems. The results suggest that for poor sleepers who magnify their sleep problem, self-monitoring can be of benefit by demonstrating that the sleep problem is not as severe as believed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Conventional wisdom, clinical lore, and numerous published studies suggest that poor sleepers tend to overestimate the severity of their sleep problems. In support of this belief, a series of classic studies have shown that people who complain of insomnia generally overestimate the amount of time they spend awake during the night relative to polysomnographic data (nocturnal EEG); good sleepers do not do this (Borkovec, 1982; Hauri and Olmstead, 1983; Frankel et al., 1976). More recent investigations have also shown that self-report data about nocturnal awake times by poor sleepers differ from objective data derived from measures such as polysomnography (PSG) and actigraphy (e.g., Currie et al., 2003; Edinger and Fins, 1995; Tang and Harvey, 2003, 2004; Vallières and Morin, 2003; Vignola et al., 2002). In recognition of such findings, recent cognitive models of insomnia have incorporated errors in time perception as important in the experience and maintenance of insomnia (Fichten et al., 2001; Harvey, 2002).
It is not clear whether insomnia sufferers misperceive sleep-wake parameters specifically or whether their ability to estimate the passage of time generally is impaired. Furthermore, current guidelines question PSG as the gold standard for evaluating insomnia (Littner et al., 2003a; Reite et al., 1995) as well as the utility of actigraphy in providing good estimates of sleep parameters (De Souza et al., 2003; Littner et al., 2003b; Vallières and Morin, 2003). Problems with both measures relate to scoring criteria for determining when the individual is asleep or awake. This is particularly true of actigraphy, which measures activity rather than sleep (i.e., movement of the wrist), and can confuse sleep with lying in bed awake but unmoving. With respect to PSG, which is typically conducted in a sleep laboratory, both the artificiality of the setting as well as the electrodes worn during the night disturb sleep and influence sleep and wake times.
There are also important discrepancies in the literature which try to show that poor sleepers overestimate the magnitude of their insomnia problem. While sleep onset latency (SOL) data usually show that poor sleepers overestimate how long it takes them to fall asleep, older poor sleepers often underestimate wake time after sleep onset (WASO) compared to objective measures (Coates et al., 1983; Libman et al., 1997a; Lichstein and Johnson, 1991; Morin et al., 1994).
In view of difficulties with measures of objective criteria, discrepancies between SOL and WASO data, and the fact that we know little about how good sleepers differ from poor sleepers in their estimates of the passage of time, a second look at time misperception by poor sleepers is warranted. Does the phenomenon actually exist? Do good sleepers estimate time differently from poor sleepers? If so, what factors influence biases in time estimation? More information about how poor sleepers estimate time can cast further light on the differentiation of primary insomnia into psychophysiological insomnia and subjective/sleep state misperception subtypes (cf. Edinger and Krystal, 2003).
Some of the postulated reasons for distorted time perception include (a) measurement related factors (e.g., people with insomnia may experience being awake during EEG recorded Stage 2 sleep—Borkovec et al., 1981; Hauri and Olmstead, 1983), (b) cognitive factors (e.g., the subjective sense that time seems to pass more slowly during distressing and unpleasant bedtime experiences—Frankel et al., 1976), and (c) the most common view among clinicians, motivational factors which induce people with insomnia to magnify their sleep problem.
The methodology of the present investigation allows us to test a variety of mechanisms that may account for errors in time perception and estimation by people who sleep poorly. Here we use exclusively self-report tools to evaluate time estimation in both analogue and naturalistic sleep contexts. This eliminates confounds related to PSG and actigraphy. Of course, self-reports also have measurement problems. If, however, our data confirm those obtained using objective measures, then there is reason for confidence in the existing data. This methodology also permits us to (1) evaluate how good and poor sleepers evaluate time in analogue, sleep-like situations during the day and to examine the relationship between evaluations of actual time as well as its subjective speed (e.g., time drags); (2) compare different aspects of the sleep experience of both good and poor sleepers: total sleep times (TST), sleep onset latency (SOL), and wake time after sleep onset (WASO); (3) explore differences between those who follow the typical pattern of time estimation for their group, and those who deviate from this (e.g., poor sleepers who underestimate the severity of their problem and good sleepers who overestimate these). The self-report methodology also (4) allows us to test a variety of mechanisms that can account for different types of errors in time estimation and perception.
Hypothesis 1: Mechanisms which might explain errors in time perception and estimation people who have insomnia are poor estimators of time, regardless of context.
Findings are ambiguous in this area. It has been shown that people with insomnia overestimate not only time to sleep onset but even a 10 min adaptation period (Borkovec and Henning, 1978), and that poor sleepers overestimated a 12.5 min interval compared to good sleepers (Belleville and Morin, 2002). On the other hand, Bonnet (1990) found that people with insomnia could accurately estimate sleep onset to a daytime nap.
Hypothesis 2: Longer and shorter sleep and wake times are susceptible to different evaluation biases.
Poor sleepers, who sleep less and spend more time awake than their good sleeper counterparts, estimate different amounts of time. Although it has been suggested that longer wake times are more susceptible to bias (e.g., Harvey, 2002), there is surprisingly little evidence available on whether longer wake times are exaggerated and whether shorter sleep times are seen as even shorter. Interpretation is problematic in the majority of investigations which use a ratio (percentage of objective sleep time estimated) to evaluate accuracy. This is defined as estimated time divided by actual time multiplied by 100 (e.g., Edinger and Fins, 1995). This type of ratio precludes examination of the length of time estimated. For example, good sleepers may spend only approximately 5 min awake during the night, while poor sleepers may stay awake for up to 3 h 180 min. If each group overestimates by 100%, this will yield only 10 min for good sleepers and an unbelievable 6 h for the poor sleepers. Alternately, if both good and poor sleepers overestimate by 10 min, this means a 200% overestimation for the good sleepers but only 6% for the poor sleepers.
Hypothesis 3: Poor sleepers evaluate empty time as if it were filled with stimulus events.
Evidence from the perception literature shows that time intervals which contain stimulus events (filled durations) are overestimated compared to unfilled intervals (Coren and Ward, 1989; Fraisse, 1984). It is, therefore, possible that poor sleepers, many of whom have a tendency to worry during nocturnal wake times (e.g., Fichten et al., 2001), fill the empty time with noxious cognitive activities and, therefore, overestimate empty time compared to good sleepers.
Hypothesis 4: People with insomnia may confuse evaluations of the subjective speed of the passage of time with actual time duration.
The research literature shows that the passage of time during unpleasant experiences in general is perceived as dragging. Faster subjectively experienced time is associated with positive experiences (Gupta and Cummings, 1986; Thayer and Schiff, 1975), while listening to a boring rather than an interesting prose passage results in the perception that time is passing slowly (Hawkins and Tedford, 1976). Thus, poor sleepers, who are likely to fill empty time with negative cognitive activity, may see unfilled and nocturnal awake times as dragging and, therefore, overestimate their duration.
Hypothesis 5: Poor psychological adjustment and high arousal in poor sleepers cause biases in time estimations.
The literature shows that even in samples selected to exclude psychopathology, many individuals who have insomnia are likely to worry more and to experience more sub-clinical anxiety and depression (e.g., Borkovec, 1982; Coursey et al., 1975; Fichten et al., 2001, Tang and Harvey, 2004). People with insomnia have also been found to experience heightened autonomic arousal (Bonnet and Arand, 1997, 1998; Harvey, 2002). The literature on anxiety indicates that highly aroused individuals are likely to overestimate time. For example, Sarason and Stoops (1978) showed that highly test anxious individuals, when put into an anxiety inducing situation, overestimated both a 4 min waiting period as well as an 18 min performance period, compared to less anxious subjects. Our findings show that some individuals who sleep poorly are very upset about their sleep problem (highly distressed poor sleepers) while others take it in stride (low distress poor sleepers) (cf. Fichten et al., 1995). Findings on highly distressed individuals with insomnia indicate that, overall, they tend to experience more negative affect and have poorer scores on a large variety of measures of daytime psychological adjustment than do good sleepers or poor sleepers who are not distressed about their sleep problems (cf. Fichten et al., 2000; Fichten et al., 2001). Thus, it is possible that worry and high arousal may cause some people with insomnia to overestimate “unfilled” times during the day as well as sleep onset latencies and nocturnal wake times.
Hypothesis 6: Variability in nocturnal sleep and wake experiences causes biases in time estimations.
There is surprisingly little information available on the night-to-night variability of sleep and wake times among good and poor sleepers. In clinical practice, clients with insomnia frequently talk about good and bad nights and complain about not being able to anticipate how well they will sleep on any specific night. If, indeed, the nocturnal experiences of individuals who have insomnia are more variable than those of good sleepers, then biases in time estimation by people who have insomnia may be due to this greater variability in sleep and wake experiences.
In experimental psychology, the study of time estimation has been generally ignored. In the insomnia literature, errors due to overestimating time spent awake compared to objective criteria are generally lamented and treated as confounds. We believe that it is profitable to view poor sleepers’ “errors” in time estimation not as mere confounds but as important and legitimate targets for investigation and intervention.
Present Investigation
To evaluate whether poor sleepers generally magnify their sleep problems and whether their estimates of nocturnal wake and sleep times are generally more pessimistic than those of good sleepers we examined time estimation in good and poor sleepers in both analogue and naturalistic sleep settings.
In the analogue setting estimates were collected of (1) elapsed time [as measured by both direct reporting of time (i.e., minutes and seconds) as well as by a production technique (production of the time interval)] and (2) subjectively perceived pace of the passage of time (i.e., time passes slowly/quickly) during brief (2.5 min) intervals when subjects listened to an audiobook or a blank tape. We expected that time would be seen as passing more swiftly in the audiobook than in the blank tape conditions and expected poor sleepers to estimate blank tape intervals as longer and more likely to drag than good sleepers.
In the naturalistic setting participants reported on their sleep by completing a retrospective sleep questionnaire (last typical week) as well as seven consecutive days of self-monitoring using a daily sleep diary (last night). Self-reports of total sleep time (TST), sleep onset latency (SOL), and duration of wake time after sleep onset (WASO) were collected on both measures. Because daily self-monitoring is “closer” to the events in question, for the present investigation we made the assumption that self-monitoring data better represent actual times spent asleep and awake than retrospective questionnaire data, which are more likely to show bias effects.
If poor sleepers have a problem estimating empty time in general, then they should overestimate elapsed time in both analogue and naturalistic contexts. If, on the other hand, poor sleepers magnify their sleep problem, then their sleep and wake scores should show more pessimistic results on the retrospective sleep questionnaire than on the daily sleep diary, relative to good sleepers.
METHOD
Measures
Background Information Form
This modified version of a short questionnaire used in our previous studies on aging provides socioeconomic, personal and demographic descriptors (e.g., age, sex, marital status) (Fichten et al., 1995, 1998; Libman et al., 1997a, 1997b).
Structured Sleep History Interview
A modified version of the clinical instrument developed by Lacks (1987) provides information on exclusion criteria (e.g., sleep apnea, parasomnias, physical disorders, sleep phase disorder, medication use, use of hypnotics and sedatives). Most questions require a yes/no answer.
Sleep Questionnaire
This retrospective questionnaire has been used in previous investigations by our team (e.g., Fichten et al., 1995, 1998). It inquires about typical sleep experiences, including sleep parameters such as sleep onset latency, total sleep and wake times, and frequency (0–7 days/week) of: difficulty falling asleep, getting back to sleep after nocturnal awakenings, and falling asleep after waking up too early. It also inquires how frequently (0–7 days/week) each of these three sleep problems is accompanied by feelings of distress. The information provided allows (1) diagnosis of the presence or absence of difficulty initiating or maintaining sleep according to conventional research criteria (i.e., 30 min of undesired nocturnal awake time at least three times per week for a minimum of 6 months, cf. Fichten et al., 2000), to distinguish sleep onset and sleep maintenance problems, and to categorize individuals into good sleeper, poor sleeper, and “medium quality” sleeper groups. Our convergent validity data indicate significant and high correlations for a mixed sample of good and poor sleepers between corresponding scores on the Sleep Questionnaire and on 7 days of self-monitoring on the daily sleep diary. The significant differences between means found on several variables showed no systematic pattern (Libman et al., 2000).
Daily Sleep Diary
This one page modification of Lacks’ (1987, 1988) self-report instrument contains items which assess sleep quality (5-point scale) as well as the specific sleep parameters of interest in the present investigation: (1) sleep onset latency (SOL), (2) duration of nocturnal arousals (WASO), and (3) total sleep time (TST). Corresponding scores on the measure and on the Sleep Questionnaire are highly correlated (Libman et al., 2000).
Subjects
Participants were 148 older community resident volunteers (mean age = 69, range = 55–87), 51 men and 97 women, who met the selection criteria for our larger investigation of sleep, aging, and nondrug treatment of insomnia (Creti et al., 2005, Fichten et al., 1995, 1998; Libman et al., 1997a, 1997b; Libman et al., 1998). For this larger investigation, both good and poor sleepers were recruited from the community through media publicity consisting of press releases, presentations and mailings to seniors groups, and notices in community clinics and residences for older adults. Selection criteria for the volunteer participants were (a) age 55 and over, (b) community resident, (c) prescription sleep medication, if used, was currently taken less than three nights per week, (d) psychological status: currently not receiving psychiatric or psychological care, no evidence of psychopathology or depression, (e) physical status: absence of major illness or drug use directly associated with sleep disturbance, (f) no evidence of physically based sleep disturbance (e.g., sleep apnea), and (g) no evidence of parasomnias or sleep phase disorder (e.g., phase delay, phase advance, or deregulation of circadian cycles). Forty-one individuals were excluded from the original group of 189 who met the selection criteria because they failed to complete one week of self-monitoring on the daily sleep diary. Demographic information indicates that subjects were generally well educated and “middle class.” For example, 39% of participants indicated that they had completed university, 56% completed high school, while 5% had only an elementary school education. Similarly, participants were financially “comfortable;” on a 9-point scale (1 = “inadequate”, 5 = “adequate,” 9 = “more than adequate”): the mean score was 5.60 (SD = 1.68); only 18% of participants had scores in the inadequate range (1–4), 44% indicated that their income was adequate, and 38% indicated that their income was more than adequate (6–9) to meet their needs. None of the groups differed significantly on demographic variables or age and the sex ratio in all categories was approximately 2/3 female and 1/3 male.
Participants were classified into three distinct groups: poor sleepers were those who met the usual research criteria for the diagnosis of insomnia (i.e., 30 min of undesired awake time at least three times per week, problem duration at least 6 months, elevated distress about the sleep problem, cf. Fichten et al., 2000) and whose sleep questionnaire responses indicated problematic sleep on two additional items evaluating sleep difficulty. Good Sleepers were individuals who failed to meet the criteria for a diagnosis of insomnia and whose sleep questionnaire responses (on four items) indicated minimal difficulty with sleep and minimal distress about sleep problems. “medium quality” sleepers had elements of both good and poor sleep (see Fichten et al., 1995 for details).
52 participants were classified good sleepers and 37 as “medium quality” Sleepers. Although only 59 individuals met the stringent criteria for Poor Sleeper status, 82 (all poor sleepers and some medium quality sleepers) were diagnosed with Insomnia (difficulty initiating or maintaining sleep): 46 had sleep maintenance insomnia (problem getting back to sleep after waking in the middle of the night) and 36 had both this sleep problem as well as sleep onset insomnia (difficulty falling asleep). Poor sleepers had experienced insomnia for a mean of 17 years (range = 0.5–60).
Procedure
All subjects completed the structured sleep history interview, the sleep questionnaire, and the assessment test battery required by the larger investigation in our laboratory one week before the time estimation tasks. The test battery contained multiple measures of nocturnal and daytime functioning, including evaluations of psychological adjustment and personality (cf. Fichten et al., 1995, 2001). Participants were also provided with a package consisting of 7 daily sleep diary sheets to be returned 1 week later.
One hundred and forty-eight participants returned completed sleep diaries (a minimum of 4 of the 7 days). Twenty of these participants could not complete the analogue time estimation tasks because of scheduling constraints, hearing impairments, equipment failure, or lack of interest. Thus, analogue time estimation tasks were completed by only 128 subjects (46 men and 82 women) 46 good sleepers, 53 poor sleepers, and 29 medium quality sleepers. Testing was conducted on an individual basis during a single session while the participant was seated in a recliner, covered by a blanket, in a semi-darkened soundproofed empty room, with all time cues removed. We gave participants a description and a rationale for the time evaluation experimental tasks; these stressed our interest in the process of how people estimate time rather than in accuracy per se.
Analogue Time Estimation Tasks
Two and a half minute segments of a blank audiotape (blank) and of five different Louis Lamour (westerns) audiotaped novels (audiobook) were used in the time estimation tasks. All audiobook segments were different and started with the first paragraph of chapter one. The beginning and end of each stimulus duration were marked with a 1000 Hz tone.
All time estimation tasks were performed twice (i.e., two trials). Half of the subjects followed the order: blank tape/audiobook, while the rest followed the order audiobook/blank. Thus, subjects were presented with two trials on both types of stimuli (e.g., blank/audiobook/blank/audiobook); order of presentation was counterbalanced. All subjects engaged in three types of evaluations; all started with direct estimations of time, followed by the time production trials and the subjective speed of time trials.
Direct Estimations of Time
The goal of this task was to obtain direct estimates of elapsed time (minutes and seconds) after presentations of a 2.5 min audiobook segment and of a 2.5 min blank tape segment. After each stimulus presentation, subjects (1) estimated the duration of the stimulus [Estimation; “How long was the tape on?” (minutes and seconds); higher scores indicate the perception that the tape lasted longer].
Productions of Time
Because of conceptual difficulties with direct estimations of elapsed time (Coren and Ward, 1989; Fraisse, 1984), subjects were also asked to estimate duration through production of the stimulus interval (i.e., produce a duration of a specific interval). Participants listened to audiobook and to blank tape segments; in each case they were asked to stop the tape after 2.5 min had gone by (Production; lower scores indicate the perception that the tape lasted longer).
Subjective Speed of Time Tasks
A specific time interval can also seem to go by quickly or slowly (e.g., a “long” or a “short” 10 min). To assess the subjective speed of the passage of time, subjects listened to 2.5 min tapes both without being informed of the duration (subjective speed—uninformed) and after being informed that the tapes lasted 2.5 min (subjective speed—informed). For the subjective speed—uninformed task they answered a question adapted from Hawkins et al. (1988), “How quickly or slowly do you think time passed?” (1 = very slowly, 5 = very quickly). For the subjective speed—informed task, they were told, “Listen to this 2.5 min tape segment and tell me how long it seemed in minutes and seconds.” There were two trials of blank and audiobook tapes for each of these two tasks, again in counterbalanced order. Time passing quickly is reflected by higher scores on the subjective speed—uninformed task and by lower scores on the subjective speed—informed task.
RESULTS
Evaluations of Time in the Analogue Context
Relationships Among Measures While Listening to a Blank Tape
To ascertain the relationship between the various time evaluation tasks in the blank tape condition we computed Pearson product-moment correlations. Results indicate that Estimation and Production evaluations of time duration are significantly related, r(126) = −0.56, p < 0.001 (i.e., the two techniques seem to be measuring the same thing). Results on time estimation indicate that estimates of time duration were not related significantly to subjective speed ratings.
We also correlated scores on both time estimation and time production as well as on the two subjective speed evaluations in the blank tape condition with scores on 21 measures of personality, worry, cognitive arousal, negative thoughts, and psychological adjustment used in the larger investigation (Fichten et al., 1998); only 2 of the 84 coefficients were significant, suggesting chance results.
Differences Between Blank and Audiobook Conditions in Good and Poor Sleepers
Two different tasks—estimation and production—were used to evaluate subjects’ perceptions of the length of elapsed time while listening to 2.5 min of blank tape and 2.5 min of an audiobook segment. Because it is not clear whether Estimation and Production tasks yield similar findings, tests are generally duplicated for the two evaluation techniques. Most of the data were analyzed using a two-way mixed design analysis of variance (ANOVA) comparison [2 groups (good sleepers/poor sleepers) × 2 tape condition (audiobook/blank)], with Condition being a repeated measure. Data from the two trials were combined. Dependent measures were time estimation, time production, and the two subjective speed of time ratings.
“Objective” Evaluations of Time
It can be seen in Table I that findings from both good and poor sleepers show that the two techniques studied—time estimation and production—yielded similar results. ANOVA results indicate no significant differences between good and poor sleepers. 2.5 min audiobook segments were judged as lasting significantly longer than 2.5 min blank tape segments: F(1,97) = 8.65, p < 0.01, for Estimation, F(1,97) = 6.88, p < 0.01, for Production. No significant interactions were found. It is noteworthy that both good and poor sleepers overestimated time by a substantial amount—an average of 37% (i.e., approximately 1 min), with a range of 11–64%.
“Subjective” Evaluations of How Quickly Time Passed
The two ANOVA comparisons made to assess whether time seemed to drag or to pass quickly in the blank and audiotape conditions also yielded similar findings. Results on both the Uninformed and Informed tasks in Table II indicate that time seemed to pass significantly more quickly while listening to an audiobook rather than to a blank tape [Estimation: F(1, 97) = 16.59, p < 0.001; Production: F(1, 97) = 26.80, p < 0.001]. Again, there were no significant differences between good and poor sleepers, and no significant interactions.
Evaluations of Time During the Night: Sleep Questionnaire versus Daily Sleep Diary
As a first test of the commonly held assumption that Poor Sleepers magnify the extent of their sleep problems we examined whether discrepancies between estimates of total sleep and wake times measured using self-monitoring (daily sleep diary) and retrospective evaluation (sleep questionnaire) differed for good and poor sleepers. Because daily self-monitoring is “closer” to the events in question, we assumed that the daily sleep diary provides a better estimate of actual amounts of time awake and asleep than the retrospective sleep questionnaire. Therefore, if Poor Sleepers magnify their sleep problem, they were expected to have more pessimistic scores (i.e., underestimating their total sleep times and overestimating their total nocturnal awake times) on the sleep questionnaire than on the daily sleep diary, relative to good sleepers.
To test this assumption, we compared good and poor sleepers’ scores on total sleep time (TST) and total wake time using two-way ANOVAs [2 groups × 2 measures (daily sleep diary/sleep questionnaire)]. Because of the sample sizes, it was possible to eliminate four outlier scores from consideration: two of these were from the Good Sleeper and two from the Poor Sleeper sample. Elimination of outliers did not change the results of the ANOVA. Means and test results in Table III show not only significant Group main effects on both variables, but also highly significant interactions. In both cases, these show that Poor Sleepers “magnified” their problem relative to good sleepers on the sleep questionnaire. Moreover, it can be seen from the means in Table III that good sleepers overestimated how long they slept and underestimated how long they were awake, while the opposite was true of Poor Sleepers.
An additional test of the magnification hypothesis involved dividing the sample of individuals who had Insomnia. To increase power, here we used the whole sample of 82 individuals diagnosed with Insomnia. This was done because, as noted in the Method, only 59 of the 82 individuals with Insomnia met the very stringent criteria for Poor Sleeper status. All 82 participants diagnosed with Insomnia had problems getting back to sleep after waking up in the middle of the night (sleep maintenance insomnia). Only a subset of them, however, had difficulty falling asleep (sleep onset insomnia). If individuals who sleep poorly have a general problem with time estimation in bed, then both Insomnia groups would have been expected to overestimate their sleep onset latency. If the issue were one of magnification of one's sleep problem, then only the group with the sleep onset insomnia diagnosis would be expected to do this.
To evaluate the hypothesis that people with Insomnia magnify their problems, we compared time estimates made by diagnosed participants who did and who did not have sleep onset insomnia using two-way ANOVA comparisons [2 problem type (sleep onset insomnia/sleep maintenance insomnia only) × 2 measure (daily sleep diary/sleep questionnaire)]. Results in Table IV indicate that according to daily sleep diary scores, those diagnosed with sleep onset insomnia took close to 1 h to fall asleep while those diagnosed with sleep maintenance insomnia only took approximately 1/2 h. ANOVA results for sleep onset latency (SOL) in Table IV indicate a significant problem type main effect as well as a significant interaction. These show that participants with sleep onset insomnia overestimated the amount of time it took them to fall asleep by approximately 20 min (i.e., 37% overestimation) while those with sleep maintenance insomnia only underestimated how long it took them to fall asleep by almost 10 min (i.e., 29% underestimation). Means for good sleepers are provided for comparison; these indicate that similar to participants with sleep maintenance insomnia only, good sleepers, who took about 1/4 h to fall asleep, also underestimated sleep onset latency (SOL), but by only 2 min (i.e., 13% underestimation). Thus, the results support the specific sleep problem magnification hypothesis. Individuals who had only sleep maintenance insomnia underestimated sleep onset latency in the same way as good sleepers.
When it came to estimating wake time after sleep onset (WASO), with which both Insomnia groups had problems, it can be seen in Table IV that the significant measure main effect shows that both groups overestimated how long they were awake by a substantial margin. Good sleepers again underestimated how long they were up, also by a very substantial amount. There were no other significant findings on this comparison.
Table IV also shows that on total sleep time the two insomnia groups differed significantly, and that both the Measure main effect as well as the interaction were significant. Scores on the sleep questionnaire were more pessimistic than on the daily sleep diary and those with both types of insomnia reported sleeping less than those with sleep maintenance insomnia only on both measures. The significant interaction shows that participants who also had sleep onset insomnia underestimated TST by almost 1/2 h more than those who only had sleep maintenance insomnia. Again, good sleepers did the opposite; they slightly overestimated how long they slept.
Poor Sleepers do not differ from good sleepers on estimating the passage of time, per se. This is indicated by the absence of significant findings between good and poor sleepers on estimation of time in the analogue context and by the significant difference, shown in Table IV, between the two insomnia groups on SOL (i.e., like good sleepers, those who had only sleep maintenance insomnia underestimated SOL, while participants with sleep onset insomnia overestimated this). This conclusion is further buttressed by a series of generally small and nonsignificant Pearson product-moment correlation coefficients for Poor Sleepers between the key variables of the analogue study (i.e., time estimation, time production, and subjective speed of the passage of time scores in the blank tape condition) and (a) home based sleep parameters, such as SOL, TST, and WASO on both the sleep questionnaire and the daily sleep diary and (b) difference scores on these variables (sleep questionnaire−daily sleep diary scores).
Deconfounding Magnification of Problem and the Length of the Time Interval Being Estimated
So all of the findings point to the conclusion that Poor Sleepers magnify their sleep problems. But do they really? The means in Tables III and IV show an important confound: people who have a sleep problem and those who sleep well are estimating different amounts of sleep and wake times. To further evaluate whether differences in accuracy are due to the length of time estimated or to magnification, we set up a series of tests to attempt to deconfound the time duration variable.
The size and direction of the differences in Table IV suggest that longer times awake are more likely to be overestimated by a substantial amount and that shorter times awake are likely to be overestimated by a smaller margin or even underestimated. The reverse appears to be the case for TST. While the evaluations of wake and sleep times in Table IV appear to indicate that those who have a specific problem tend to magnify that problem, it is also evident in Table IV that, in all cases, the longer the “actual” awake time (or shorter the sleep time), the greater the overestimation.
To explore the relationship between length of time estimated and the extent of over and underestimation we examined correlations between “actual” duration of sleep and wake times (daily sleep diary) and the magnitude and direction of the estimation errors by examining difference scores (sleep questionnaire/daily sleep diary) on TST, WASO, and SOL. These relationships for the various groups are best seen in Figs. 1–3.

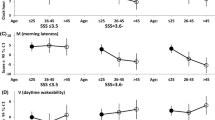
Sleep onset latency: over and underestimation by participants in the various groups.

Wake time after sleep onset: over and underestimation by participants in the various groups.

Total sleep time: over and underestimation by participants in the various groups.
On SOL (Fig. 1), the scatterplot and the Pearson product-moment correlation coefficient, r(49) = −0.504, p < 0.001, show that for good sleepers, the longer it takes to fall asleep, the greater the underestimation. The same is true of participants who have sleep maintenance insomnia only, r(44) = −0.733, p < 0.001. However, for those with sleep onset insomnia, the relationship, while still one of general underestimation, is much weaker, r(30) = −0.302, p < 0.05, and the scatterplot best resembles a triangle (i.e., the longer the “actual” sleep onset latency, the greater the size of both under and overestimations).
On WASO (Fig. 2), the scatterplot and the large significant correlation, r(48) = −0.971, p < 0.001, show that the longer good sleepers are “actually” awake, the larger the underestimation. Once more, the pattern of results for those who have sleep maintenance insomnia (i.e., all 82 subjects diagnosed with Insomnia) was very different. In this case, there appears to be no coherent pattern and the coefficient is both very small and nonsignificant, r(78) = −0.025, p > 0.05.
On TST (Fig. 3), for good sleepers the modest but significant negative correlation, r(50) = −0.424, p < 0.01, shows that longer times spent asleep are generally underestimated, although the scatterplot shows an inverted triangle (i.e., the shorter the actual TST, the more discrepant the estimates on the sleep questionnaire). Again, the scatterplot for those with Insomnia is less coherent and the correlation is small and nonsignificant, r(80) = −0.191, p > 0.05.
Resolving the Inconsistencies Between Findings on Means and Correlations
The correlations and the scatterplots in Figs. 1–3 appear to be inconsistent with the findings on means reported in Table IV. These latter suggest that, in general, longer wake times are overestimated and shorter wake times are underestimated and that shorter sleep times are underestimated and longer sleep times are overestimated. The scatterplots suggest the opposite.
Frequencies and Relative Size of Over and Underestimations
One possible reason for the inconsistency may reside in the relative sizes of over and underestimations and in the percentage of people who over and underestimate. To explore the relative sizes of over and underestimations of the various sleep parameters in good sleepers and in those with Insomnia we examined the number of participants who over and underestimated SOL, TST, and WASO. Results in Table V show that among the good sleepers, the vast majority (92%) underestimate WASO, and this by a large margin (about 1/2 h). Slightly more good sleepers underestimate (55%) than overestimate (45%) SOL. The amount of time by which they over and underestimate are also similar (about 8 min). People who have sleep maintenance insomnia only are, for the purposes of evaluation of SOL, good sleepers, and they follow the same pattern: 61% of them underestimated SOL and only 39% overestimated this sleep parameter. Again, while the size of the underestimation was somewhat greater than the size of overestimations, the difference in means was not substantial (about 11 min).
Good Sleepers are equally likely (50%) to over and to underestimate TST, although those who overestimate are likely to do so by a larger margin than those who underestimate (44 min vs. 25 min). Thus, the pattern of findings on frequencies of over and underestimation for good sleepers is similar to that found for means in Table IV. Indeed, it appears as though good sleepers have an optimistic expectation—a relatively short “norm”—about how long they are up and how long they sleep. The larger the discrepancy between this “norm” and their actual sleep and wake times, the greater the underestimation for SOL and WASO. The pattern on TST suggests that the shorter their actual sleep time, the more likely people are to provide either larger overestimations or larger underestimations.
When individuals experience problematic sleep, however, the pattern of findings is very different and shows that the majority of individuals with Insomnia overestimate wake times after sleep onset (69%) and underestimate sleep times (63%). In addition, the average size of the overestimations of awake times is approximately double the average size of underestimations. Similarly, the size of underestimation of total sleep times is approximately double the size of overestimations.
To try to better understand the findings on participants with Insomnia we examined the relative frequencies of individuals who magnified both aspects of their sleep problem (i.e., both overestimated WASO and underestimated TST) and those who minimized these. We did the same for good sleepers. It can be seen in Table VI that the largest group of individuals with Insomnia magnified both aspects of their sleep problem (n = 36, 48%) and that the smallest group (n = 8, 11%) minimized both aspects. It is noteworthy that similar numbers (15 and 16) over and underestimated both sleep parameters. Among good sleepers, none magnified both aspects of a sleep problem and approximately half minimized both. Chi-Square tests on these two sets of comparisons showed nonsignificant results for both the Insomnia, χ2(1) = .12, p > .05, and Good Sleeper groups, χ2(1) = 3.07, p > .05; these fail to support the idea that over or underestimation of WASO is related to estimation of TST.
What Distinguishes Individuals with Insomnia Who Behave Like Good Sleepers?
To examine what differentiates the minority of individuals with Insomnia who behave like good sleepers from the majority we correlated difference scores as well as sleep parameters from both the sleep questionnaire and the daily sleep diary with scores on the large number of measures used in the larger investigation which evaluated personality, worry, cognitive arousal, negative thoughts, psychological adjustment, daytime functioning, nocturnal distress, lifestyle, and demographic variables (cf. Fichten et al., 1995, 1998). These correlations were, almost exclusively, small and nonsignificant, suggesting that none of these variables distinguished those individuals who slept poorly but failed to magnify their sleep problems.
Variability of Wake and Sleep Times in Individuals with Insomnia and Good Sleepers
So, if psychological variables, relative frequencies of people, and the length of time being estimated do not explain the pattern of over and underestimations of sleep problems in those who have Insomnia, what does? A final possibility concerned the hypothesis that there is greater night-to-night variability in the sleep and wake experiences of those with Insomnia than in those who sleep well, and that the more variable the nocturnal experience, the greater the estimation error. To explore this notion we examined the standard deviations on SOL, WASO, and TST for the 7 nights that participants completed the daily sleep diary. The t-tests on mean scores show that the night-to-night variability on WASO (i.e., mean of the standard deviations) for those who have Insomnia (M = 0.91, SD = 0.47) is significantly greater than for good sleepers (M = 0.49, SD = 0.42), t(131) = 5.23, p < 0.001. Similarly, daily sleep diary SOL scores of those with sleep onset insomnia (M = 0.67, SD = 0.53) were significantly more variable than those of good sleepers (M = 0.18, SD = .21), t(85) = 5.97, p < 0.001. The comparison on TST of good sleepers (M = 0.83, SD = 0.43) and those with Insomnia (M = 0.95, SD = 0.21), although in the same direction, was not significant, t(131) = 1.43, p > 0.05.
To further examine whether the variability of daily sleep diary SOL, TST, and WASO scores was related to difference scores (sleep questionnaire−daily sleep diary), daily sleep diary standard deviation scores were correlated with difference scores for good sleepers and for each of the two Insomnia groups. Results show modest to strong negative correlations (range −0.176 to −0.789) between the variability of wake time scores (SOL and WASO) and the corresponding difference scores. None of the correlations involving TST were significant. Consistent with the “norming” notion, the largest (absolute) SOL, WASO, and TST coefficients were achieved in the Good Sleeper group, indicating that the more variable they are, the smaller the difference scores. Thus, although those with Insomnia do appear to have more variable nocturnal experiences, especially when it comes to wake times, the magnitude of the variability does little to explain the size of errors in time estimation.
DISCUSSION
Consistent with the findings of Bonnet (1990), the analogue study failed to show any distinctive time estimation problem on the part of individuals who have insomnia. On analogue tasks, both good and poor sleepers dramatically overestimated both 2.5 min of empty time as well as 2.5 min spent listening to an audiobook, with estimations in the audiobook condition being greater. Empty time was perceived as dragging relative to time spent listening to an audiobook. Again, there were no differences between good and poor sleepers, and Hypothesis 1 was not supported. There was also no indication that poor sleepers evaluate empty time as if it were filled with stimulus events. (Hypothesis 3). In addition, errors in estimates of time duration in the analogue context were not related significantly to home based scores on sleep parameters, to home based errors in time estimation, or to scores on measures of psychological adaptation and functioning.
Interestingly, the nocturnal sleep context also does not support a generalized tendency to overestimate duration of time on the part of poor sleepers. All poor sleeper participants had sleep maintenance insomnia, but only a subset of them had sleep onset insomnia. If poor sleepers have a general problem with time estimation, then both types of insomnia groups would be expected to overestimate their sleep onset latency. If the issue is, rather, one of magnification of one's sleep problem, then only the group with the sleep onset insomnia diagnosis would be expected to overestimate. The results, consistent with the magnification formulation, show that while those who had sleep onset insomnia overestimate how long it took them to fall asleep, individuals who had only sleep maintenance insomnia underestimated sleep onset latency in the same way as did good sleepers.
As the findings of Edinger and Fins (1995) indicate, mean scores may not tell the whole story. The results also show that while approximately half of the participants who had insomnia magnified both sleep and wake aspects of their problem, approximately 10% minimized both aspects. Of the rest, half magnified their sleep problem but minimized their wake problem and the other half did the converse. An interesting additional finding was that where the individual experienced one type of sleep problem, only that specific sleep problem was magnified. Among good sleepers, none magnified both sleep and wake aspects of a sleep problem and approximately half minimized both. Almost all others underestimated both their sleep and wake times.
With respect to Hypothesis 2 (longer and shorter durations of sleep/wake times are susceptible to different time estimation biases), the findings reported so far are inconclusive. In all cases longer wake and shorter sleep intervals were confounded with having a sleep problem. Nevertheless, analyses suggest that poor sleepers’ longer wake times and shorter sleep times do not explain the results.
To explore the relationship between length of time estimated and the extent of over and underestimation we examined correlations between the “actual” duration of sleep and wake times and the size and direction of estimation errors by examining difference scores (sleep questionnaire−daily sleep diary). Therefore, if the hypothesis that the reason that people who sleep poorly overestimate wake times is because the times are longer were to be correct (Hypothesis 2), then longer sleep onset latencies in both good and poor sleepers should have been overestimated. The results, best seen in the three figures, show that for good sleepers, the converse was true (i.e., the longer it takes to fall asleep, the greater the underestimation). The same was true of participants who have sleep maintenance insomnia but no sleep onset problem.
On wake time after sleep onset, again good sleepers underestimated longer wake times. For people with sleep maintenance insomnia the relationship between wake time and time estimation was nonsignificant. Again, these results are not consistent with the hypothesis that longer wake times are overestimated by people with insomnia.
As for total sleep time, for good sleepers there was a modest but significant negative correlation, showing that shorter times spent asleep were generally overestimated, while the relationship for people with insomnia was not significant. Thus, the results on sleep times, too, are inconsistent with the hypothesis that shorter sleep times are underestimated.
The findings on the relationship between time duration and over and underestimations, overall suggest that good sleepers have an optimistic expectation, a “norm” for how long they are asleep or awake during the night. Poorer sleep than the “norm” is, therefore, subject to estimation error. For poor sleepers there is no such norm, as suggested by the greater variability in their wake times. Their over and underestimations are generally not correlated with actual duration of sleep and wake parameters. These findings on poor sleepers are consistent with results reported by others, who also failed to show significant correlations between actual SOL, TST and WASO and the extent of over and underestimations (e.g., Edinger and Fins, 1995).
Variability of Sleep and Wake Times
It was suggested in Hypothesis 6 that there is greater night-to-night variability in the sleep and wake experiences of people who sleep poorly than among those who sleep well, and that it is these more variable nocturnal experiences that account for the errors in time estimation in people with insomnia. Although our data do show that poor sleepers experience greater night-to-night variability in nocturnal wakefulness than do good sleepers, correlations between variability and wake time difference scores showed only modest negative coefficients and none of the correlations involving sleep time were significant. Consistent with the “norming” notion, the highest coefficients were achieved in the good sleeper group.
Distress and Psychological Adjustment
Our previous studies have shown that many older people who experience poor sleep are not distressed by this (Fichten et al., 1995). Moreover, insomnia-related distress was related to poorer scores on numerous measures of psychological adjustment (Fichten et al., 2001). Therefore, we thought it possible that the size of magnification of poor nocturnal experiences would be related to scores on measures of personality, worry, cognitive arousal, negative thoughts, and psychological adjustment (Hypothesis 5). Consistent with others’ findings (Tang and Harvey, 2003), correlations between psychological variables and the size of estimation errors are not significant.
CONCLUSIONS
The findings suggest that many, but by no means all people who have insomnia magnify both sleep and wake aspects of their sleep problems when reporting on these in a retrospective, global manner. The data show that this tendency is not caused by problems related to estimating time in general, to the variability of the night-to-night sleep and wake experiences of individuals who have insomnia, to psychological variables (e.g., poorer psychological adjustment, negative thoughts during nocturnal awake times, neuroticism, nocturnal cognitive arousal, the tendency to worry), or to the length of time being estimated. Nor do the findings support the contention that the reason that poor sleepers overestimate wake times is that they fill empty wake times with self generated stimuli or that they confuse subjective speed of the passage of time with actual time duration. In fact, the only thing which seems to be implicated is the nature of one's sleep problem: overestimation of wake times is limited to the specific sleep problem experienced. Further research of the type indicated in Edinger and Krystal's (2004) review on subtyping primary insomnia is needed to determine what causes some poor sleepers to magnify their sleep problems and others to minimize these.
Several limitations of the present investigation must be noted. First, the sample is comprised of adults aged 55 and over, limiting the generalizability of the findings to younger age groups. It has long been known that older adults are likely to have problems with both sleep maintenance as well as sleep onset insomnia, while younger individuals usually have only sleep onset problems (e.g., Morin et al., 1993). Yet, it is precisely because of this characteristic of our sample that we were able to test some of the hypotheses. In addition, the analogue study dealt with only one time interval of 2.5 min. Although Rioux et al. (2004), using similar time durations, concluded that the typical sleep misperception in insomnia sufferers could not be explained by an altered sense of passage of time, longer or shorter intervals may have produced different results. The sleep parameters on the sleep questionnaire refer to the week prior to the week during which subjects completed the daily sleep dairy. Although our data show that test-retest correlations on the sleep questionnaire indicate reasonable temporal stability (r values range from 0.58 to 0.92) for the sleep questionnaire, it would have been preferable to have ratings on both measures reflect the identical 7-day period.
Clinical Implications
The findings suggest that many, but by no means all people who have insomnia magnify their sleep problems when reporting on these in a retrospective, global manner. As suggested by Edinger and Fins (1995), clinicians must not assume that all individuals with insomnia magnify the severity of their problem. Possibly, this characteristic is related to insomnia subtypes (Edinger and Krystal, 2003). In addition it will be important to find out which aspect of the sleep problem—wake or sleep time—is magnified. The pattern of the magnification may have important implications for diagnosis and treatment. For example, Edinger and Fins’ (1995) data and a recent study from our own laboratory involving diagnostic profiles in sleep apnea (Bailes et al., 2004) suggest that those poor sleepers who minimize their sleep complaint might profitably be investigated for a primary sleep disorder, such as sleep apnea or periodic limb movement disorder, or for other conditions characterized by nonrestorative sleep and daytime fatigue (e.g. chronic fatigue syndrome, depression).
People who do magnify aspects of their sleep problem, on the other hand, need to be made aware that their nighttime experience is not as bad as they believe it to be. Studies by Tang and Harvey (2003, 2004) show that demonstrating the discrepancy between actual and estimated scores corrected distorted perceptions and that visually juxtaposing the actual and estimated scores, rather than merely telling poor sleepers about these, also helped reduce sleep related anxiety and distress. Use of both a retrospective sleep questionnaire as well as a daily sleep diary during problem assessment may facilitate this process by bringing the added benefit of “reality testing” to the severity of perceived sleep problems.
REFERENCES
Belleville, G., and Morin, C. M. (2002). Are insomniacs poor judges of time? Retrospective and prospective estimates of time intervals in insomniacs and good sleepers. Sleep 25: Abstract Supplement.
Bailes, S., Baltzan, M., Alapin, I., Fichten, C. S., and Libman, E. (in press). Diagnostic indicators of sleep apnea in older women and men: A prospective study, Journal of Psychosomatic Research.
Bonnet, M. H. (1990). The perception of sleep onset in insomniacs and normal sleepers. In Bootzin, R. R., Kihlstrom, J. F., and Schacter, D. L. (Eds.), Sleep and cognition, American Psychological Association, Washington, pp. 149–157.
Bonnet, H. M., and Arand, D. (1997). Hyperarousal and insomnia: A review article. Sleep Med. Rev. 1(2): 97–108.
Bonnet, H. M., and Arand, D. (1998). Heart rate variability in insomniacs and matched normal sleepers. Psychosom. Med. 60: 610–615.
Borkovec, T. D. (1982). Insomnia. J. Consult. Clin. Psychol. 50(6): 880–895.
Borkovec, T. D., and Henning, B. L. (1978). The role of physiological attention focusing in the relaxation treatment of sleep disturbance, general tension, and specific stress reaction. Behav. Res. Ther. 16: 7–19.
Borkovec, T. D., Lane, T. W., and Van Oot, P. H. (1981). Short report: Phenomenology of sleep among insomniacs and good sleepers: Wakefulness experience when cortically asleep. J. Abnorm. Psychol. 90(6): 607–609.
Coates, T. J., Killen, J. D., Silverman, S., George, J., Marchini, E., Hamilton, S., and Thoresen, C. E. (1983). Cognitive activity, sleep disturbance, and stage specific differences between recorded and reported sleep. Psychophysiology 20: 243–250.
Coren, S., and Ward, L. M. (1989). Sensation and perception. In CorenS., and Ward, L. M. (Eds.), Sensation and perception, 3rd ed., Harcourt Brace Jovanovich, Toronto, pp. 371–389.
Coursey, R. D., Buchsbaum, M., and Frankel, B. L. (1975). Personality measures and evoked responses in chronic insomniacs. J. Abnorm. Psychol. 84(3): 239–249.
Currie, S., Malhotra, S., and Clark, S. (2003). Agreement among subjective, objective and collateral measures of insomnia in recovering alcoholics. Presentation at the Association for Advancement of Behavior Therapy (AABT) Conference, Boston.
De Souza, L., Benedito-Silva, A., Nogueira Pires, M., Poyares, D., Tufik, S., and Calil, M. H. (2003). Further validation of actigraphy for sleep studies. Sleep 26: 81–85.
Edinger, J. D., and Fins, A. I. (1995). The distribution and clinical significance of sleeptime misperceptions among insomniacs. Sleep 18: 232–239.
Edinger, J. D., and Krystal, A. D. (2003). Subtyping primary insomnia: Is sleep state misperception a distinct clinical entity? Sleep Med. Rev. 7(3): 203–214.
Fichten, C. S., Creti, L., Amsel, R., Brender, W., Weinstein, N., and Libman, E. (1995). Poor sleepers who do not complain of insomnia: Myths and realities about psychological and lifestyle characteristics of older good and poor sleepers. J. Behav. Med. 18(2): 189–223.
Fichten, C. S., Libman, E., Bailes, S., and Alapin, I. (2000). Characteristics of older adults with insomnia. In Lichstein, K. L. and Morin, C. M. (Eds.), Treatment of late life insomnia, Sage, NY, pp. 37–80.
Fichten, C. S., Libman, E., Creti, L., Amsel, R., Sabourin, S., Brender, W., and Bailes, S. (2001). Role of thoughts during nocturnal awake times in the insomnia experience of older adults. Cognitive Ther. Res. 25(6): 665–692.
Fichten, C. S., Libman, E., Creti, L., Amsel, R., Tagalakis, V., and Brender, W. (1998). Thoughts during awake times in older good and poor sleepers—The self-statement test:60+. Cognitive Ther. Res. 22(1): 1–20.
Fraisse, P. (1984). Perception and estimation of time. Am. Rev. Psychol. 35: 1–36.
Frankel, B. L., Coursey, R. D., Buchbinder, R., and Snyder, F. (1976). Recorded and reported sleep in chronic primary insomnia. Arch. Gen. Psychiat. 33: 615–623.
Gupta, S., and Cummings, L. L. (1986). Perceived speed of time and task affect. Percept. Motor Skills 63(2), 971–980.
Hauri, P., and Olmstead, E. (1983). What is the moment of sleep onset for insomniacs? Sleep 6(11): 10–15.
Häkkänen, J., and Summala, H. (2000). Sleepiness at work among commercial truck drivers. Sleep 23: 49–57.
Harvey, A. G. (2002). A cognitive model of insomnia. Behav. Res. Ther. 40: 869–982.
Hawkins, M. F., and Tedford, A. H. (1976). Effects of interest and relatedness on estimated duration of verbal material. Bull. Psychonom. Soc. 8: 301–302.
Hawkins, W. L., French, L. C., Crawford, D. B., and Engle, M. E. (1988). Depressed affect and time perception. J. Abnorm. Psychol. 97: 275–280.
Lacks, P. (1987). Behavioral treatment for persistent insomnia. Pergamon Press, New York.
Lacks, P. (1988). Daily sleep diary. In M. Hersen and A. S. Bellack (Eds.), Dictionary of behavioral assessment techniques, Pergamon, New York, pp. 162–164.
Lacks, P. (1988). Daily sleep diary. In M. Hersen and A. S. Bellack (Eds.), Dictionary of behavioral assessment techniques, Pergamon, New York, pp. 162–164.
Libman, E., Fichten, C. S., Weinstein, N., Tagalakis, V., Amsel, R., Brender, W., and Creti, L. (1998). Improvement and deterioration in sleep status of “younger” and “older” seniors: A longitudinal study. J. Ment. Health Aging 4(1): 183–192.
Libman, E., Creti, L., Amsel, R., Brender, W., and Fichten, C. S. (1997a). What do older good and poor sleepers do during periods of nocturnal wakefulness? The Sleep Behaviors Scale: 60+. Psychol. Aging 12(1): 170–182.
Libman, E., Creti, L., Levy, R. D., Brender, W., and Fichten, C. S. (1997b). A comparison of reported and recorded sleep in older poor sleepers. J. Clinical Geropsychol. 3(3): 199–211.
Libman, E., Fichten, C. S., Bailes, S., and Amsel, R. (2000). Sleep questionnaire vs. sleep diary: Which measure is better? Behavior and Sex Therapy Service, SMBD Jewish General Hospital. SqvsDiary.doc. Available e-mail: mc65@musica.mcgill.ca.
Lichstein, K. L., and Johnson, R. S. (1991). Older adults’ objective self recording of sleep in the home. Behav. Ther. 22: 531–548.
Littner, M., Hirshkowitz, M., Kramer, M., Kapenm, S., Mc Dowell, Anderson, W., Bailey, D., Berry, R. B., Davila, D., Johnson, S., Kushida, C., Loube, D. I., Wise, M., and Woodson, B. T. (2003a). Practice parameters for using polysomnography to evaluate insomnia. Sleep 26(6): 754–760.
Littner, M., Kushida, C., McDowell Anderson, W., Bailey, D., Berry, R. B., Davila, D., Hirshkowitz, M., Kapen, S., Kramer, M., Loube, D. I., Wise, M., and Johnson, S. (2003b). Practice parameters for the role of actigraphy in the study of sleep and circadian rhythms: An update for 2002. Sleep 26: 337–341.
Morin, C. M., Colecchi, C., Stone, J., Brink, D., and Sood, R. (1994). Cognitive-Behav. Ther. for insomnia. Convention Proceedings for the 28th Annual AABT, 65. San Diego, CA: AABT.
Morin, C. M., Kowatch, R. A., Barry, T., and Walton, E. (1993). Cognitive-Behav. Ther. for late-life insomnia. J. Consult. Clin. Psychol. 61(1): 137–146.
Perlis, M. L., Giles, D. E., Bootzin, R. R., Dikman, Z. V., Fleming, G. M., Drummond, S. P., and Rose, M. W. (1997). Alpha sleep and information processing, perception of sleep, pain, and arousability in fibromyalgia. Int. J. Neurosci. 89(3–4): 265–280.
Reite, M., Buysse, D., Reynolds, C., and Mendelson, W. (1995). The use of polysomnography in the evaluation of insomnia. Sleep 18: 58–70.
Rioux, I., Bastien, C. H., Morin, C. M., and Tremblay, S. (2004). Time estimation in chronic insomnia sufferers. Presentation at the Canadian Sleep Society 2nd Congress, Quebec.
Sarason, I. G., and Stoops, R. (1978). Test anxiety and the passage of time. J. Consult. Clin. Psychol. 46(1): 102–109.
Salin-Pascual, R. J., Roehrs, T. A., Merlotti, L. A., Zorick, F., and Roth, T. (1992). Long-term study of insomnia patients with sleep state misperception and other insomnia patients. Am. J. Psychiat. 149(7): 904–908.
Tang, N. K. Y., and Harvey, A. G. (2004). Correcting distorted perception of sleep in insomnia: A novel behavioral experiment. Behav. Res. Ther. 42: 27–39.
Tang, N. K. Y., and Harvey, A. G. (2003). An investigation of distorted perception of sleep in insomnia using actigraphy. Presentation at the Association for Advancement of Behavior Therapy (AABT) Conference, Boston.
Thayer, S., and Schiff, W. (1975). Eye-contact, facial expression, and the experience of time. J. Soc. Psychol. 95: 117–124.
Vallières, A., and Morin, C. M. (2003). Actigraphy in the assessment of insomnia. Sleep 26: 902–906.
Vignola, A., Bastien, C. H., and Morin, C. (2002). Evaluation neuropsychologique de la performance objective et subjective chez des aînés bon dormeurs et souffrant d'insomnie chronique. Poster session presented at the Quatrième journée scientifique du Réseau Santé Mentale, Montreal, Quebec.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fichten, C.S., Creti, L., Amsel, R. et al. Time Estimation in Good and Poor Sleepers. J Behav Med 28, 537–553 (2005). https://doi.org/10.1007/s10865-005-9021-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10865-005-9021-8