
Abstract
Mindfulness refers to the ability to be aware of and attentive to internal and external events, without becoming overwhelmed or feeling the need to react automatically. Recent studies indicate that this ability is associated with the following factors: mental health, psychological functioning, and stress reduction. Although questionnaires have been developed to measure mindfulness, so far these have not been adapted for use within the Italian population. Thus, the aim of our studies was to investigate the reliability and validity of an Italian version of the Five Facet Mindfulness Questionnaire (FFMQ; Baer et al. Assessment, 13, 27–45, 2006). The FFMQ is a self-report measure that is based on a five-facet model (i.e., Observe, Describe, Act with Awareness, Nonjudge, and Nonreact). In the first study, internal consistency, factor structure, and concurrent validity analyses were carried out on a sample of 559 volunteers. The second study entailed test–retest analyses on a different sample of 43 students. The results showed that the Italian FFMQ: (a) has a similar factor structure to the original English version; (b) has good to excellent internal consistency as a whole (alpha = 0.86) with sub-scale consistency ranging from 0.65 to 0.81, and test–retest stability for the total score being 0.71; (c) has good concurrent validity as demonstrated by significant correlations between the FFMQ scores and a number of self-report measures related to mindfulness. Our findings support both the adaptation of the FFMQ to the Italian context as well as the conceptualization of mindfulness in multi-faceted terms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In recent decades the construct of mindfulness has received increased attention. In general terms, it refers to the ability to attend to experiences occurring in the present moment in both a non-evaluative and accepting way (Brown and Ryan 2003; Kabat-Zinn 1990; Linehan 1993a). As Kabat-Zinn (1990) pointed out mindfulness is the opposite of mind-blindness, i.e., the tendency to behave automatically and mechanically, as if ‘on autopilot’. Similarly, Langer (1989) defined mindlessness as the inclination to perceive reality through experience-based preconceptions. On the contrary, mindfulness allows experience of reality to unfold in the present and to thus be considered from different points of view. Being ‘mentally present’ therefore means being aware and accepting of one’s activities and mental states, as they reveal themselves in the moment.
The construct of mindfulness has its origin in Eastern spiritual traditions, specifically, in Buddhist meditation practices (Mace 2008). In recent decades, traditional mindful meditation practices have been adapted for secular use. Mindful based interventions have now been widely available in medical and mental-health settings. These interventions include mindfulness-based stress reduction techniques which have been adapted based on Kabat-Zinn’s work (MBSR; Kabat-Zinn 1982, 1990), Linehan’s dialectical behavior therapy for borderline personality disorders (DBT; Linehan 1993a, b), mindfulness-based cognitive therapy (MBCT; Segal et al. 2002), acceptance and commitment therapy (ACT; Hayes et al. 1999) and other variations of these methods. A number of studies have indicated that the mindful stance is related to psychological well-being (Black et al. 2011; Brown and Ryan 2003; Dekeyser et al. 2008; Rasmussen and Pidgeon 2011), and mindfulness-based interventions reduce psychological symptoms and act as a protective factor for psychological distress. Beneficial effects, for example, have been observed on the reduction of symptoms such as anxiety, depression, self-harm, impulsive and aggressive behaviors, as well as physical symptoms and sensory pain (Dunn et al. 2012; Farb et al. 2012; Grossman et al. 2004; Mace 2008). In general, symptom-reduction has been observed across a wide range of clinical populations, suffering from both mental and physical disorders (Baer 2003; Grossman et al. 2004; Hartmann et al. 2012; Hayes et al. 2004; Kearney et al. 2012; Mace 2008; Robins and Chapman 2004; van der Lee and Garssen 2012).
Several studies have focused on the empirical validation of mindfulness scales that consider the underlying components of mindfulness (Baer et al. 2004; Brown and Ryan 2003; Cardaciotto et al. 2008; Lau et al. 2006). The authors have emphasized that psychometrically sound measures of mindfulness are necessary for an understanding of the mechanisms and consequently the beneficial effects. Baer et al. (2006) administered the five mindfulness questionnaires available at the time to a large student sample, in order to develop a reliable and valid measure of mindfulness. These scales included the Mindful Attention Awareness Scale (MAAS; Brown and Ryan 2003), the Freiburg Mindfulness Inventory (FMI; Buchheld et al. 2001), the Kentucky Inventory of Mindfulness Skills (KIMS; Baer et al. 2004), the Cognitive and Affective Mindfulness Scale (CAMS; Feldman et al. 2004; Hayes and Feldman 2004), and the Mindfulness Questionnaire (MQ; later denominated the Southampton Mindfulness Questionnaire, Chadwick et al. 2008). After carrying out a factor analysis on the combined pool of items, the authors retained 39 items and proposed a hierarchical factor structure, characterized by a general factor for mindfulness and five secondary facets. The resulting questionnaire was named Five Facet Mindfulness Questionnaire (FFMQ; Baer et al. 2006), and the five facets identified were described as:
-
Observe (8 items)—Attending to sensory stimuli that mainly derive from external sources and the body as well as related cognitions and emotions.
-
Describe (8 items)—Labeling internal experiences with words.
-
Act with Awareness (8 items)—An ongoing attention to, and awareness of present activity and experience.
-
Nonjudge (8 items)—Having a non-evaluative attitude towards one’s thought and emotional processes while focusing on inner experiences, rather than taking on a critical stance.
-
Nonreact (7 items)—Assuming a stance that implies being able to perceive thoughts and feelings, especially when they are distressing, but without feeling compelled to react or being overwhelmed.
More recent studies have supported the validity of the FFMQ for the assessment of mindfulness and its correlates, in both clinical and non-clinical samples across different languages and cultural backgrounds (Baer et al. 2008; Bohlmeijer et al. 2011; Bränström et al. 2010; Carmody and Baer 2008; Deng et al. 2011; Fernandez et al. 2010; Heeren et al. 2011; Lilja et al. 2011; Sugiura et al. 2011; Veehof et al. 2011). However, more research is called for to investigate the extent to which Baer et al.’s (2006) findings can be generalized to different samples. In Italy the wide-spread interest for mindfulness is suggested by the numerous clinical contexts in which it is practiced and taught. At the same time, research on the construct and its applications is rare. In fact, only two empirical studies have been published to date (Fossati et al. 2011, 2012), as a PUBMED and PsycINFO search by means of the cue words ‘mindfulness’ and ‘Italian’ confirmed. Both studies administered translated versions of the questionnaires on mindfulness with the aim to investigate the relationship between mindfulness and personality disorders in non-clinical adolescents (Fossati et al. 2011) and adult outpatients (Fossati et al. 2012). As the authors had pedicted, both studies found that high levels of mindfulness were negatively associated with characteristics of personality disorders.
The main objective of the present study was to address the aforementioned lack of valid measures of mindfulness in Italy, with the intent to also contribute to the cross-cultural adaptation of the FFMQ. Two studies were carried out to investigate the validity and reliability of the Italian translation of the FFMQ. Study 1 examined the factor structure, internal consistency and concurrent validity of the questionnaire in a sample of undergraduate psychology students and a normative adult sample. Study 2, analyzed the test–retest reliability of a smaller sample of 43 University students who had not participated in the first study.
Study 1
Method
The FFMQ was translated into Italian and administered along with other self-report measures to a large Italian sample of students and adults.
The Translation of the FFMQ
The adaptation of the FFMQ to an Italian population included a translation and a subsequent back-translation procedure (Brislin 1980; Geisinger 2003; Van de Vijver and Hambleton 1996). Several authors (L. B., C. G., G. A.) translated the original English version of the FFMQ from English to Italian. Then, a bilingual author (A. T.), who was blind to the original questionnaire, re-translated this version back into English. Finally, the two English versions were compared in order to resolve inconsistencies.
Participants
The initial sample consisted of 636 Italians: 355 were undergraduate University students; 281 were non-student adult volunteers, who were recruited in order to extend the age range of the sample. After eliminating subjects with missing data on one or more items of the FFMQ, the sample size was reduced to 559. This final sample ranged in age from 18 to 64 years (M = 33.0; SD = 12.1); The majority (70.7 %) of the participants were femaleFootnote 1. All were Italian citizens and identified themselves as Italian and Caucasian.
Procedure
All participants were handed the questionnaires along with a brief description of the study and an informed consent form. The student sample was recruited through an online service of the University of Milano-Bicocca. The non-student sample was collected by using a strategy similar to that of the snowball sampling, i.e., a small group of students (not included in the student sample) asked other people (relatives, friends, and acquaintances) to take part in the study by anonymously completing the questionnaires (envelopes were provided for each participant so as to keep the answers unavailable to the students who collected the questionnaires). Each student recruited at least ten participants as part of a homework assignment in a personality assessment undergraduate course.
All participants were volunteers and filled out the questionnaires anonymously. The students involved in the study, either as participants or as recruiters, received class credit in exchange for participation. The non-student volunteer participants did not receive any compensation for their participation.
Measures and Predictions
To validate the Italian version of the FFMQ we included measures adopted by Baer et al. (2006) in their original validation study. Validated Italian measures were used and when these were unavailable, the scales were translated and subsequently back-translated.
The Five Facets Mindfulness Questionnaire (FFMQ; Baer et al. 2006)
The FFMQ is a 39 item self-report instrument developed in order to measure five aspects on a 5-point Likert scale, ranging from 1 (never or very rarely true) to 5 (very often or always true), with higher total scores reflecting a greater degree of mindfulness. According to Baer et al.’s (2006) original study, the FFMQ measures one general mindfulness factor and five secondary facets (Observe, Describe, Act with Awareness, Nonjudge, and Nonreact). In that study, Cronbach’s alphas ranged from 0.75 to 0.91 for all scales, except for Nonreact, that had an alpha value of 0.67. Each sub-scale correlated significantly and in the expected directions with other mindfulness questionnaires, related constructs, self-report well-being measures, and with the absence of psychopathological symptoms. An exception was the factor Observe, which had no significant correlation with Nonjudge and correlated positively with measures of dissociation, psychological symptoms, absent-mindedness and thought suppression (Baer et al. 2006). Similar results have been found across different languages and cultures (Deng et al. 2011; Heeren et al. 2011; Lilja et al. 2011; Sugiura et al. 2011). However, when a subsample of experienced meditators was examined, Observe correlated positively and significantly with Nonjudge, thus suggesting that in people with no experience in meditation, attending to experiences may be associated with judging them (Baer et al. 2006, 2008).
The Toronto Alexithymia Scale (TAS-20; Bagby et al. 1993)
The TAS-20 is often referred to as the gold standard method for assessing alexithymia. Participants are asked to rate 20 items on 5-point Likert scale, with higher total scores indicating an increase in alexithymia. In this study we used the Italian version of the TAS-20 (Bressi et al. 1996), which has high Cronbach alphas in both clinical and non-clinical groups (0.82 and 0.75 respectively) and a high test–retest reliability over 2 weeks (r = 0.86). Mindfulness implies observing and labeling one’s mental processes and feelings, we therefore predicted a negative correlations between the TAS-20 and our Italian version of the FFMQ, in particular with the Observe and Describe sub-scales.
The Big Five Questionnaire-2 (BFQ-2; Caprara et al. 2007)
The BFQ-2 is a self-report measure of personality traits and behavioral preferences. For this study, we selected only the items measuring Mental Openness and Emotional Stability. These two dimensions are valid and reliable measures of a tendency to accept experience (Mental Openness) and the ability to cope with negative emotions (Emotional Stability) according to Caprara et al. (2007). Given that mindfulness is associated with lower levels of negative affect and a greater ability to observe inner feelings and external stimuli, we expected positive correlations between the FFMQ and these BFQ-2 scales. In particular, the Nonreact facet and the Emotional Stability scale were expected to be positively correlated, since they both describe the ability to come to terms with distressing feeling, thoughts and situations without being overwhelmed by them.
The Trait Meta-Mood Scale (TMMS; Salovey et al. 1995)
The TMMS is a 30-item self-report measure of emotional awareness and understanding. Items are rated on a 5-point Likert scale, with higher scores reflecting greater attention to emotions, as well as the ability to regulate emotions. Salovey et al. (1995) obtained an adequate to good internal consistency for the total scores and for each sub-scale. Further, the scale was reported to be significantly associated with less life-satisfaction and with fewer depressive episodes (Martinez-Pons 1997). The scale was adapted into Italian through a back-translation procedure since an Italian version was not available. We predicted positive correlations between the TMMS and the FFMQ. In particular we expected to replicate the results of Baer et al. (2006), who found positive correlations with the Observe and Describe facets, as these entail identifying external and internal experiences and labeling them.
The Difficulties in Emotion Regulation Scale (DERS; Gratz and Roemer 2004)
The DERS is a 36-item self-report measure that assesses significant difficulties in emotion regulation. Items are rated on a 5-point Likert scale, with higher scores reflecting greater difficulties. For this study we used an Italian validated version (Giromini et al. 2012), which showed adequate to excellent internal consistency (alpha values ranged from 0.77 to 0.92) and test–retest reliability (ICCs ranged from 0.49 to 0.73), and good validity (significant correlations with related constructs were found, and a clinical vs. non-clinical sample comparison yielded significant differences with large effect sizes). Because the mindfulness construct includes awareness and acceptance of emotions, we expected negative correlations between the DERS and the FFMQ.
Scale of Dissociative Activities (SODAS; Mayer and Farmer 2003)
The SODAS is a self-report measure of dissociation, with items being rated on a 5-point Likert scale. Higher scores reflect acting without awareness, a lack of perception of inner experience, memory disruptions and perception of unreality. According to Mayer and Farmer (2003) the SODAS has good internal consistency (an alpha value equal to 0.95) and test–retest reliability (r = 0.77), and is significantly correlated with other measures of dissociation. Italian versions of the SODAS were also not available. The scale was therefore adapted by means of the back-translation procedure. Dissociation, as measured by the SODAS, implies lack of awareness of actions and inner experiences. We therefore predicted a negative correlation with the FFMQ, especially in the case of the Act with Awareness sub-scale that refers to the ability to exercise constant awareness during activities.
White Bear Suppression Inventory (WBSI; Wegner and Zanakos 1994)
The WBSI is a 15-item self-report measure of thought suppression. Studies have shown that its internal consistency is good (alpha value of ’89) and test–retest reliability is satisfactory (r = 0.80) (Muris et al. 1996). Because no validated Italian versions of the WBSI was available, we adapted it to Italian by means of the back-translation procedure. Negative correlations between the WBSI and the FFMQ were expected, especially in relation to the Nonjudge sub-scale that describes accepting thoughts and feelings without critical judgment, while the WBSI measures attempts to suppress or avoid internal experiences.
Results
FFMQ Scores
Descriptive statistics for the FFMQ scores are indicated in Table 1. All scores were normally distributed. Age was modestly correlated with the Describe, r = −0.09, p = 0.04, and Act with Awareness facets, r = 0.09, p = 0.04. Male participants scored a little lower on Observe, M = 24.1 (SD = 5.8) vs. M = 25.3 (SD = 5.3), t(279.5Footnote 2) = −2.3, p = 0.02, d = 0.16, and slightly higher on Nonjudge, M = 28.8 (SD = 5.7) vs. M = 27.2 (SD = 5.9), t(554) = 2.9, p < 0.01, d = 0.27 than female participants. None of the other FFMQ scores were significantly correlated with age, nor were other significant gender differences observed. Correlations among the FFMQ sub-scales and between the sub-scales and the total FFMQ score are shown on Table 2. Similar to Baer et al.’s (2006) findings, the five facets were not strongly correlated amongst themselves while all facets correlated positively with the total FFMQ score. Finally, in line with previous findings among nonmeditating samples (Baer et al. 2006, 2008; Lilja et al. 2011; Sugiura et al. 2011) the sub-scale Observe was negatively correlated with the Nonjudge and Act with Awareness sub-scales.
Factorial Structure
Baer et al. (2006) suggested a hierarchical model, in which Observe, Describe, Act with Awareness, Nonjudge and Nonreact were defined as facets of an overall mindfulness construct. To test if such a model was also replicated in our Italian sample, we conducted a confirmatory factor analysis (CFA), using a correlation matrix of individual items as input, and a maximum likelihood estimation method (Hu et al. 1992). This analysis was conducted using structural equation modeling by means of Lisrel 8.50 (Jöreskog and Sörbom 2001).
To evaluate the goodness of fit of the model, four indices were considered with particular attention: (1) the root mean square error of approximation (RMSEA); (2) the comparative fit index (CFI); (3) the nonnormed fit index (NNFI); (4) the ratio of the value of chi-square to its degrees of freedom (chi2/df). In detail, the following criteria were considered: the RMSEA had to be around 0.05 for a close fit, 0.08 for a fair fit, and 0.10 for a marginal fit (Browne and Cudeck 1993), the CFI and NNFI had to be 0.90 or higher for a good fit (Bentler and Bonett 1980), and the chi2/df had to be close to 2.00 for a good fit, and lower than 5.00 for a quite promising fit (Watkins 1989).
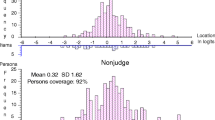
According to these criteria, the CFA performed on the Italian version of the FFMQ replicated the factorial structure obtained by Baer et al. (2006) rather well. Indeed, the RMSEA indicated a fair to close fit (RMSEA = 0.072; 90 % confidence interval = 0.069–0.075), the CFI and NNFI were not far from the threshold value of 0.90 (CFI = 0.83; NNFI = 0.82), and the chi2/df was quite promising to good (chi2/df = 3.918). Furthermore, all factor loadings were ≥0.30 (for details see Fig. 1).

Factorial structure of the Italian FFMQ Obtained from CFA (N = 559). Note. The coefficients that describe the loadings of the five facets on the broad mindfulness construct are maximum likelihood estimates. Maximum likelihood estimates of item loadings on facets are also provided. For ease of presentation, error terms for items are omitted. r reversed item
Internal Consistency
To determine the internal consistency of the Italian version of the FFMQ, Cronbach’s alpha was calculated for both the total and for each sub-scale score. As shown in Table 3, the results indicate that the FFMQ has a high internal consistency, with Cronbach’s alpha = 0.86 for the total score, and acceptable values for the sub-scales, i.e., alpha ≥0.74Footnote 3. It should be pointed out however, that two items (i.e., item 33 “Usually when I have distressing thoughts or images, I just notice them and let them go” and item 11 “I notice how food and drinks affect my thoughts, bodily sensations, and emotions”) obtained low—albeit significant—correlations (i.e., <0.2) with the total FFMQ score.
Concurrent Validity
To provide data on the concurrent validity of the Italian version of the FFMQ, correlations between the FFMQ scores and the above-indicated questionnaires, measuring related constructs were investigated. The values of Cronbach’s alpha for each measure included in this analysis was higher than 0.70. Results are presented in Table 4. As in the study of Baer et al. (2006), our results indicate that four of the five facets of the FFMQ (i.e., Describe, Act with Awareness, Nonjudge and Nonreact) correlated positively with measures related to mindfulness (e.g., emotional stability), and negatively with the scales that assess aspects which may be regarded as mind-blinded or mindless. As predicted, the facet Act with Awareness was negatively correlated with the dissociation scale, and the sub-scale Nonjudge correlated with a tendency to dissociation and thought suppression. The Describe facet was negatively associated with alexithymia and positively with emotional awareness. As expected, the highest correlation of the Nonreact facet was found with the scale assessing emotional stability. Our results also replicated those of Baer et al. (2006), by finding that the Observe facet apart from correlating positively with mental openness and emotional awareness, was also associated in a positive direction with dissociation and thought suppression.
Study 2
Method
To assess the test–retest reliability of the Italian FFMQ, a second sample was obtained.
Participants
Participants were 43 undergraduate Psychology University students who had not participated in Study 1 and who compiled the questionnaires in exchange for class credit. Ages ranged from 19 to 48 years (M = 23.5; SD = 6.0); 81.4 % were female.
Procedure
During a psychology class, students were invited to complete the FFMQ, indicating their University ID number. All were informed that participation was voluntary and that written consent was required before taking part in the study. Of these students, 43 agreed to complete the FFMQ again 4 weeks later. Class credit was given in exchange for participation.
Results
The intraclass correlation coefficient (ICC) for the total FFMQ was 0.71. The ICCs for the sub-scales were: 0.63 for Observe; 0.81 for Describe; 0.71 for Act with Awareness; 0.65 for Nonjudge; 0.63 for Nonreact. According to the suggested benchmarks (Cicchetti 1994; Cicchetti and Sparrow 1981; Fleiss 1981), the test–retest of the Italian FFMQ is good to excellent.
General Discussion
A widespread interest in the construct and practice of mindfulness during recent decades encouraged the development of different empirical methods for its assessment. In particular, mindfulness-related techniques in Italy are beginning to be applied to clinical contexts and validated instruments for its assessment are thus required. As a consequence, the main objective of this study was to investigate the validity and reliability of the Italian version of the FFMQ. Two studies were conducted: the first aimed to examine the factorial structure, the internal consistency and the convergent validity of the questionnaire; the second to assess test–retest reliability.
Results, overall, supported both the adaptability of the FFMQ to the Italian context and the concept of mindfulness as a multi-dimensional construct. The factor structure of the Italian version replicated the one obtained by Baer et al. (2006). In fact, the internal consistency and test–retest stability were adequate to excellent, and most of the scores correlated in the expected direction with a number of theoretically-related constructs. In other words, all five facets identified by Baer et al. (2006), appeared to be distinct, valid and reliable features of mindfulness.
The dimensions of the FFMQ were associated with other constructs selected for the evaluation of the convergent validity. As in Baer et al. (2006), the ability to observe internal and external sensations and experiences was associated with emotional intelligence, while the capacity to express one’s inner experience in words (Describe) was, as expected, associated negatively with alexithymia and positively with emotional intelligence. Not surprisingly, the capacity to be mindful of ongoing activities (Act with Awareness) was negatively associated to dissociation. Finally, the scale assessing a non-judgmental stance towards feelings and thoughts (Nonjudge) was negatively associated with emotion dysregulation, thought suppression and dissociative tendencies. Also, as expected, the propensity to assume a stance that implies observing but without feeling compelled to react to distressing experiences (Nonreact) was positively related to emotional stability.
The sub-scale Observe was associated to a lesser extent to mindfulness as a whole (the total score of the FFMQ) than the other four facets, and a negative, albeit modest, association of the ability to Observe was found with the mindfulness-related dimensions of Acting with Awareness and Non-Judging. Furthermore, Observe was positively associated with the self-reported measures of dissociation and thought suppression. This finding was however in line with Baer et al. (2006), who hypothesized that the content of the Observe factor, with its attention to external stimuli and body-experiences, differs from the other factors, which tend to refer to cognition, emotions, behaviors, and/or attention. They further suggested that the Observe factor may be more sensitive to meditation experience than others. Indeed, according to Baer et al.’s (2006) findings, the sub-scale Observe is highly correlated with a general mindfulness factor, but only if the FFMQ is administered to experienced meditators. Thus, our Observe-related results may be in part explained by the lack of an experienced meditator sample in our studies. It should be noted, in any case, that Observe clearly emerged from the factor analysis, showed good internal consistency and test–retest stability, and did show significant correlations (in the expected direction) with both mindfulness (i.e., with the FFMQ total scores) and emotional intelligence (i.e., with the TMMS scores).
A number of limitations for both our studies should also be highlighted. First, our studies only included self-report measures which may lead to misleading interpretations of the items. Second, the divergent validity of the FFMQ was not addressed. Third, three of the scales administered to investigate the concurrent validity of the Italian FFMQ have not yet been cross-validated with the Italian population. Fourth, given that in study 1, participants were asked to complete several questionnaires concerning relatively similar constructs, respondent fatigue may have occurred. Therefore, more research on Italian samples, and in particular, with participants who have experience in meditation or mindfulness techniques is warranted.
Despite the limitations and uncertainties of our present studies, the results provide a contribution to mindfulness research, suggesting that the FFMQ is adaptable to the Italian context, as well as provide further support for Baer et al. (2006)’s multi-dimensional model of mindfulness.
Notes
Three records were missing gender information and 3 were missing ages.
Since homoscedasticity could not be assumed, the Welch-Satterthwaite method was used to adjust the degrees of freedom.
According to Nunnally (1978) values of 0.70 or higher are considered acceptable.
References
Baer, R. A. (2003). Mindfulness training as a clinical intervention: a conceptual and empirical review. Clinical Psychology: Science and Practice, 10, 125–143.
Baer, R. A., Smith, G. T., & Allen, K. B. (2004). Assessment of mindfulness by self-report: the Kentucky Inventory of Mindfulness Skills. Assessment, 11, 191–206.
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13, 27–45.
Baer, R. A., Smith, G. T., Likins, E., Button, D., Krietemeyer, J., Sauer, S., et al. (2008). Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment, 15, 329–342.
Bagby, R. M., Taylor, G. J., & Parker, J. D. A. (1993). The twenty-item Toronto Alexithymia scale-II: convergent, discriminant, and concurrent validity. Journal of Psychosomatic Research, 38, 33–40.
Bentler, P. M., & Bonett, D. G. (1980). Significance tests and goodness of fit in the analysis of covariance structures. Psychological Bulletin, 88, 588–606.
Black, D. S., Semple, R. J., Pokhrel, P., & Grenard, J. L. (2011). Component processes of executive function-mindfulness, self-control, and working memory and their relationships with mental and behavioral health. Mindfulness, 2, 179–185.
Bohlmeijer, E., ten Klooster, P. M., Fledderus, M., Veehof, M., & Baer, R. (2011). Psychometric properties of the five facet mindfulness questionnaire in depressed adults and development of a short form. Assessment, 8, 308–320.
Bränström, R., Kvillemo, P., Brandberg, Y., & Moskowitz, J. T. (2010). Self-report mindfulness as a mediator of psychological well-being in a stress reduction intervention for cancer patients: a randomized study. Annals of Behavioral Medicine, 39, 151–161.
Bressi, C., Taylor, G. J., Parker, J. D. A., Bressi, S., Brambilla, V., Aguglia, E., et al. (1996). Cross validation of the factor structure of the 20-Item Toronto Alexithymia Scale: an Italian multicenter study. Journal of Psychosomatic Research, 41, 551–559.
Brislin, R. W. (1980). Translation and content analysis of oral and written material. In H. C. Triandis & J. W. Berry (Eds.), Handbook of cross-cultural psychology (Vol. 1, pp. 389–444). Boston: Allyn & Bacon.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84, 822–848.
Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & J. S. Long (Eds.), Testing structural equation models (pp. 136–162). Beverly Hills: Sage.
Buchheld, N., Grossman, P., & Walach, H. (2001). Measuring mindfulness in insight meditation (Vipassana) and meditation-based psychotherapy: the development of the Freiburg Mindfulness Inventory (FMI). Journal for Meditation and Meditation Research, 1, 11–34.
Caprara, G. V., Barbaranelli, C., Borgogni, L., & Vecchione, M. (2007). Big Five Questionnaire—2 (BFQ-2). Firenze: Giunti O.S. Organizzazioni Speciali.
Cardaciotto, L., Herbert, J. D., Forman, E. M., Moitra, E., & Farrow, V. (2008). The assessment of present-moment awareness and acceptance: the Philadelphia Mindfulness Scale. Assessment, 15, 204–223.
Carmody, J., & Baer, R. A. (2008). Relationship between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. Journal of Behavioral Medicine, 31, 23–33.
Chadwick, P., Hember, M., Symes, J., Peters, E., Kuipers, E., & Dagnan, D. (2008). Responding mindfully to unpleasant thoughts and images: reliability and validity of the Southampton Mindfulness Questionnaire (SMQ). British Journal of Clinical Psychology, 47, 451–455.
Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychological Assessment, 6, 284–290.
Cicchetti, D. V., & Sparrow, S. S. (1981). Developing criteria for establishing the interrater reliability of specific items in a given inventory. American Journal of Mental Deficiency, 86, 127–137.
Dekeyser, M., Raes, F., Leijssen, M., Leysen, S., & Dewulf, D. (2008). Mindfulness skills and interpersonal behaviour. Personality and Individual Differences, 44, 1235–1245.
Deng, Y., Liu, X., Rodriguez, M. A., & Xia, C. (2011). The Five Facet Mindfulness Questionnaire: psychometric properties of the Chinese version. Mindfulness, 2, 123–128.
Dunn, C., Hanieh, E., Roberts, R., & Powrie, R. (2012). Mindful pregnancy and childbirth: effects of a mindfulness-based intervention on women’s psychological distress and well-being in the perinatal period. Archives of Women’s Mental Health, 15, 139–143.
Farb, N. A., Anderson, A. K., & Segal, Z. V. (2012). The mindful brain and emotion regulation in mood disorders. Canadian Journal of Psychiatry, 57, 70–77.
Feldman, G. C., Hayes, A. M., Kumar, S. M., & Greeson, J. M. (2004). Development, factor structure, and initial validation of the Cognitive and Affective Mindfulness Scale. Unpublished.
Fernandez, A. C., Wood, M. D., Stein, L. A., & Rossi, J. S. (2010). Measuring mindfulness and examining its relationship with alcohol use and negative consequences. Psychology of Addictive Behaviour, 24, 608–616.
Fleiss, J. L. (1981). Statistical methods for rates and proportions (2nd ed.). New York: Wiley.
Fossati, A., Feeney, J., Maffei, C., & Borroni, S. (2011). Does mindfulness mediate the association between attachment dimensions and Borderline Personality Disorder features? A study of Italian non-clinical adolescents. Attachment and Human Development, 13, 563–578.
Fossati, A., Vigorelli Porro, F., Maffei, C., & Borroni, S. (2012). Are the DSM-IV personality disorders related to mindfulness? An Italian study on clinical participants. Journal of Clinical Psychology.
Geisinger, K. F. (2003). Testing and assessment in cross-cultural psychology. In J. R. Graham, J. A. Naglieri, & I. B. Weiner (Eds.), Handbook of psychology (Vol. 10). Assessment psychology (pp. 95–118). New Jersey: Wiley.
Giromini, L., Velotti, P., de Campora, G., Bonalume, L., & Zavattini, G. C. (2012). Cultural adaptation of the difficulties in Emotion Regulation Scale: reliability and validity of an Italian version. Journal of Clinical Psychology, 68(9), 989–1007.
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26, 41–54.
Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness-based stress reduction and health benefits: a meta-analysis. Journal of Psychosomatic Research, 57, 35–43.
Hartmann, M., Kopf, S., Kircher, C., Faude-Lang, V., Djuric, Z., Augstein, F., et al. (2012). Sustained effects of a mindfulness-based stress-reduction interventions in type 2 diabetic patients: design and first results of a randomized controlled trial (The Heidelberger Diabetes and Stress-Study). Diabetes Care, 35, 945–947.
Hayes, A. M., & Feldman, G. (2004). Clarifying the construct of mindfulness in the context of emotion regulation and the process of change in therapy. Clinical Psychology: Science and Practice, 11, 255–262.
Hayes, S. C., Strosahl, K., & Wilson, K. G. (1999). Acceptance and commitment therapy: An experiential approach to behavior change. New York: Guilford.
Hayes, S. C., Masuda, A., Bissett, R., Luoma, J., & Guerrero, L. F. (2004). DBT, FAP, and ACT: how empirically oriented are the new behaviour therapy technologies? Behavior Therapy, 35, 35–54.
Heeren, A., Douilliezc, C., Pescharda, V., Debrauwerea, L., & Philippota, P. (2011). Cross-cultural validity of the Five Facets Mindfulness Questionnaire: adaptation and validation in a French-speaking sample. Revue Européenne de Psychologie Appliqué, 61, 147–151.
Hu, L. T., Bentler, P. M., & Kano, Y. (1992). Can test statistics in covariance structure analysis be trusted? Psychological Bulletin, 112, 351–362.
Jöreskog, K., & Sörbom, D. (2001). LISREL 8.51 for Windows. Computer software. Lincolnwood: Scientific Software International, Inc.
Kabat-Zinn, J. (1982). An outpatient program in behavioural medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. General Hospital Psychiatry, 4, 33–47.
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of your mind and body to face stress, pain, and illness. New York: Delacorte.
Kearney, D. J., McDermott, K., Malte, C., Martinez, M., & Simpson, T. L. (2012). Association of participation in a mindfulness program with measures of PTSD, depression and quality of life in a veteran sample. Journal of Clinical Psychology, 68, 101–116.
Langer, E. J. (1989). Mindfulness. Cambridge: Perseus Books.
Lau, M. A., Bishop, S. R., Segal, Z. V., Buis, T., Anderson, N. D., Carlson, L., et al. (2006). The Toronto Mindfulness Scale: development and validation. Journal of Clinical Psychology, 62, 1445–1467.
Lilja, J. L., Frodi-Lundgren, A., Hanse, J. J., Josefsson, T., Lundh, L. G., Sköld, C., et al. (2011). Five Facets Mindfulness Questionnaire—reliability and factor structure: a Swedish version. Cognitive Behaviour Therapy, 40, 291–303.
Linehan, M. M. (1993a). Cognitive-behavioral treatment of borderline personality disorder. New York: Guilford.
Linehan, M. M. (1993b). Skills training manual for treating borderline personality disorder. New York: Guilford.
Mace, C. (2008). Mindfulness and mental health: Therapy, theory and science. London: Routledge.
Martinez-Pons, M. (1997). The relation of emotional intelligence with selected areas of personal functioning. Imagination, Cognition, and Personality, 17, 3–13.
Mayer, J. L., & Farmer, R. F. (2003). The development and psychometric evaluation of a new measure of dissociative activities. Journal of Personality Assessment, 80, 185–196.
Muris, P., Merckelbach, H., & Horselenberg, R. (1996). Individual differences in thought suppression. The White Bear Suppression Inventory: factor structure, reliability, validity and correlates. Behavioural Research and Therapy, 34, 501–513.
Nunnally, J. C. (1978). Psychometric theory. New York: McGraw-Hill.
Rasmussen, M. K., & Pidgeon, A. M. (2011). The direct and indirect benefits of dispositional mindfulness on self-esteem and social anxiety. Anxiety, Stress and Coping, 24, 227–233.
Robins, C. J., & Chapman, A. L. (2004). Dialectical behavior therapy: current status, recent developments, and future directions. Journal of Personality Disorders, 18, 73–89.
Salovey, P., Mayer, J. D., Goldman, S. L., Turvey, C., & Palfai, T. P. (1995). Emotional attention, clarity, and repair: Exploring emotional intelligence using the Trait Meta-Mood Scale. In J. W. Pennebaker (Ed.), Emotion, disclosure, and health (pp. 125–154). Washington, DC: American Psychological Association.
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2002). Mindfulness based cognitive therapy for depression: A new approach to preventing relapse. New York: Guilford.
Sugiura, Y., Sato, A., & Ito, Y. (2011). Development and validation of the Japanese version of the Five Facet Mindfulness Questionnaire. Mindfulness, 3, 85–94.
Van de Vijver, F., & Hambleton, R. K. (1996). Translating tests: some practical guidelines. European Psychologist, 1, 89–99.
van der Lee, M. L., & Garssen, B. (2012). Mindfulness-based cognitive therapy reduces chronic cancer-related fatigue: a treatment study. Psychooncology, 21, 264–272.
Veehof, M. M., ten Klooster, P. M., Taal, E., Westerhof, G. J., & Bohlmeijer, E. T. (2011). Psychometric properties of the Dutch Five Facet Mindfulness Questionnaire (FFMQ) in patients with fibromyalgia. Clinical Rheumatology, 30, 1045–1054.
Watkins, D. (1989). The role of confirmatory factor analysis in cross-cultural research. International Journal of Psychology, 24, 685–701.
Wegner, D. M., & Zanakos, S. (1994). Chronic thought suppression. Journal of Personality, 62, 615–640.
Conflict of Interest
Caterina Giovannini declares that there is no conflict of interest; Luciano Giromini declares that there is no conflict of interest; Laura Bonalume declares that there is no conflict of interest; Angela Tagini declares that there is no conflict of interest; Margherita Lang declares that there is no conflict of interest; Gherardo Amadei declares that there is no conflict of interest.
Experiment Participants
The study protocol and informed consent have been approved by the Institutional Ethic Committee and meets the standards required.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Giovannini, C., Giromini, L., Bonalume, L. et al. The Italian Five Facet Mindfulness Questionnaire: A Contribution to its Validity and Reliability. J Psychopathol Behav Assess 36, 415–423 (2014). https://doi.org/10.1007/s10862-013-9403-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10862-013-9403-0