
Abstract
Background
Implantable cardioverter defibrillators (ICD) are life-saving device therapy, and patients often carry devices for decades with interim pulse generator exchanges. Inappropriate shocks are associated with impaired quality of life and increased mortality, but available data on their incidence and etiology outside of clinical trials is limited and usually restricted to the lifespan of a singular device. We hypothesized that the incidence in clinical practice is underestimated and aimed this study to retrospectively assess the long-term incidence and etiology of inappropriate shocks in a real-world cohort of patients with multiple ICDs over a long follow-up period.
Methods
Patients with ICDs implanted between 1998 and 2012 in two Swiss cardiology departments and at least one device exchange in the same department thereafter were included in this cohort. Retrospective analysis with follow-up until 2016 was conducted to assess incidence and etiology of inappropriate ICD shocks.
Results
Two hundred forty-nine ICDs were implanted in 100 patients (mean age: 60.1 ± 11.7; 80% male). Over a mean follow-up time of 11.2 (± 3.6) years, 555 shocks occurred in 55 patients. One hundred twenty-three (22%) shocks in 23 (23%) patients were inappropriate. Supraventricular arrhythmia and oversensing were the most frequent causes of inappropriate shock. Patients with younger age or previous supraventricular arrhythmias were at increased risk of inappropriate shocks. Patients with inappropriate shocks during the lifespan of their first ICD were at increased risk for inappropriate shocks in subsequent devices.
Conclusions
Inappropriate shocks are an underestimated and frequent problem in clinical practice with an incidence that may exceed numbers of previously reported clinical trials with shorter follow-up periods. Patients at increased risk for inappropriate shocks need careful evaluation of potential therapeutic optimization strategies including pharmacological treatment, device programming, electrophysiological ablation, device downgrading, and telemonitoring.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Cardiovascular diseases are the most common causes of death in the early twenty-first century, and cardiac arrhythmias are estimated to constitute up to 30% of worldwide cardiovascular mortality [1]. After the first successful human application of an implantable cardioverter defibrillator (ICD) in 1980, several landmark studies confirmed reduced mortality and morbidity after ICD implantation in patients at high risk for ventricular arrhythmias [2,3,4,5,6,7]. Currently, 1% of the total population in Europe is estimated to harbor a potential indication for future ICD implantation [8, 9]. A feared complication of ICD implantation are inappropriate shocks, defined as shocks delivered in the absence of ventricular tachycardia and associated with impaired quality of life, earlier battery depletion, and increased mortality [10, 11]. With increasing numbers of patients with ICDs and multiple pulse generator exchanges, estimating long-term incidence and clinical predictors of inappropriate ICD shocks is becoming crucial in everyday routine clinical practice in order to evaluate risk-to-benefit ratio of ICD implantation, facilitate patient-informed decision-making, and identify patients at high risk that might benefit from potential pharmacological, interventional, or device-programming interventions to minimize inappropriate ICD therapy. However, available data on the long-term incidence of inappropriate ICD shocks outside of clinical trials is sparse and heterogeneous within: in a meta-analysis of contemporary trials, inappropriate ICD therapy was estimated to occur in 10 to 24% of patients [12]. Furthermore, the follow-up time in clinical studies is usually restricted to the lifespan of a singular device, hence not reflecting real-life patients carrying ICD devices for decades. Additionally, whether patients suffering from an inappropriate shock during the lifespan of their first ICD are at increased risk for inappropriate shocks in subsequent devices might seriously influence risk-to-benefit evaluation at timepoints of pulse generator exchanges. We hypothesized that the incidence of inappropriate shocks in patients with ICDs may be higher in clinical practice than in previous trials, and aimed this study to retrospectively assess the long-term incidence and etiology of inappropriate shocks in a real-world cohort of patients with ICDs and at least one pulse generator exchange.
2 Methods
2.1 Patient population
Patients with primary transvenous ICD implantations between 1998 and 2012 and at least one pulse generator exchange were included for analysis in two collaborating Swiss healthcare centers (University Heart Center Zurich and Zurich Regional Health Center Wetzikon). In both departments, systematic data collection was started around 1998, and in order to achieve a sufficient follow-up time exceeding the lifespan of singular ICD device for a minimum of 4 years, patients with primary implantations after 2012 were excluded. Patients were identified and recruited via the respective clinics informational system and followed up until January 2016. In all patients, indication for ICD implantation complied with international guidelines at the timepoint of implantation. Patients were eligible, if device and patient characteristics at the time of first device implantation and device exchange were available. Device settings were programmed according to current evidence-based guidelines at the timepoint of implantation and were changed at the discretion of the responsible attending physician. At least one documented device interrogation for every implanted pulse generator was mandatory for patient enrollment, with scheduled ICD controls being performed in 3- to 6-month intervals. Patients with missing ICD interrogation data for more than 6 months were considered lost to follow-up.
2.2 Data acquisition
Baseline and follow-up data was collected by thorough investigation of all electronic or paper-based patient history at the time of the first ICD implantation, and at every follow-up visit until January 2016. ICD readouts and 12 lead electrocardiograms were used for shock classification. An inappropriate shock (IAS) was defined as a shock delivered by the ICD in the absence of ventricular tachycardia or ventricular fibrillation. Since detailed programming parameter settings were not available for all patients at all follow-up visits, these parameters were not analyzed.
2.3 Statistical analysis
Mean values and standard deviations (SD) were chosen for continuous variables. Numbers and percentages (%) were given for categorical variables. For patients, only percentages were noted, since exactly 100 patients were finally included. The Kaplan-Meier method and Log-rank tests were performed to illustrate the time to first appropriate/inappropriate shock and compare subgroups for cumulative event rates. The Cox proportional hazards regression analysis was used to determine clinical variables associated with increased risk of inappropriate shocks, with univariate analysis being performed primarily with all baseline variables. Subsequently, a multivariate analysis was performed for variables with a p value < 0.1 in the univariate analysis. For examination of time-dependent occurrence of inappropriate shocks by ICD implantation date, ICD implantations were divided into two groups by median calendar implantation date, and a log-rank test was conducted. The Mann-Whitney U test was used to compare incidences of inappropriate shocks in subsequent ICDs in patients with/without inappropriate shock in their first ICD. A p value of < 0.05 was considered significant. For computed statistical analysis, the IBM SPSS Statistics version 23 Software (SPSS, Inc., Chicago, Illinois) was used.
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
3 Results
3.1 Patient population
One hundred eighteen patients underwent an ICD implantation between 1998 and 2012 and had experienced at least one pulse generator exchange. Eighteen patients were excluded due to missing device interrogation data during follow-up, insufficient baseline characteristics, or downgrading to a pacemaker at the timepoint of the first pulse generator exchange. Of the remaining 100 patients included in the analysis, 80% were male with a mean age of 60.1 (± 11.7) years at the time of first ICD implantation, 61% suffered from ischemic heart disease, 80% had impaired left ventricular systolic function, 41% experienced supraventricular arrhythmias before ICD implantation, and 51% were implanted with primary prevention indication. Devices were exclusively implanted in the pectoral region and manufactured by St. Jude Medical (St. Paul, Minnesota), Boston Scientific (Natick, Massachusetts), Medtronic (Minneapolis, Minnesota), Biotronik (Berlin, Germany), Ventritex (Sunnyvale, California), or Guidant (St. Paul, Minnesota). Baseline patient characteristics are summarized in Table 1.
3.2 Device implantation and exchanges
Within a cumulative follow-up period of 1123.1 years, 249 ICDs were implanted, of which 149 replaced previously implanted aggregates. All patients received one pulse generator exchange, and 41% received two or more exchanges. Battery depletion was the indication in 72.5%, and an upgrade to cardiac resynchronization therapy was the indication in 15.4%, while electrode dysfunction and infection were indications for a device exchange in less than 10% (9.4%) of patients. One hundred sixty-five of the 249 implanted ICDs were dual chamber ICDs. The most common manufacturers used were Medtronic (36.9%), Boston Scientific/Guidant (28.9%), and St. Jude Medical (23.7%). The mean time to ICD device exchange was 4.4 (± 2.1) years.
3.3 Incidence of inappropriate shocks
During a mean follow-up of 11.2 (± 3.6) years, 555 shocks occurred in 55 (55%) patients. The amount of inappropriate shocks was 123 (22.2%) occurring in 23 patients, while the amount of appropriate shocks was 432 (77.8%) occurring in 45 patients. Cumulative event rates of first inappropriate shock were 6% at 1 year, 13% at 2 years, 16% at 5 years, 21% at 8 years, and 23% at 10 years (Fig. 1). Of the 23 patients suffering from inappropriate shocks, 19 (83%) patients experienced more than one inappropriate shock and 12 (52.2%) patients experienced both appropriate and inappropriate shocks. The mean number of years until occurrence of first shock after the first ICD implantation was 1.8 (± 1.7) years for inappropriate and 2.2 (± 2.1) years for appropriate shock. Eighty-seven percent of patients received their first inappropriate shock within 6 years after primary ICD implantation, while almost half of all patients experienced an appropriate shock within 10 years of follow-up. The mean number of inappropriate shocks was 1.23 (± 3.3) for all patients and 5.4 (± 5.0) for patients with inappropriate shocks. The cumulative incidence of inappropriate ICD shocks for all patients was 1 inappropriate shock in 10 years of ICD exposure.

Kaplan-Meier curve for first inappropriate ICD shock
3.4 Etiology of inappropriate shocks
The main cause of inappropriate shock was supraventricular arrhythmia misdiagnosed as ventricular tachycardia (74.8% of inappropriate shocks), with atrial fibrillation being the most frequent subtype (Fig. 2). Oversensing of T waves and sinus tachycardia represented the second and third most frequent causes (14.6 and 12.2%). Oversensing due to lead defect was responsible for 9.8%, and atrioventricular-node re-entry tachycardia was responsible for 8.9% of inappropriate shocks. Analysis of the 31 ICDs delivering inappropriate shocks revealed, that 64.5% of all ICDs delivered inappropriate shocks due to supraventricular arrhythmias, and 32% delivered inappropriate shocks due to oversensing.

Mechanism of inappropriate shock (123 inappropriate shocks = 100%)
3.5 Variables associated with inappropriate shocks
We additionally performed uni- and multivariate proportional Cox regression analysis to identify clinical predictors of inappropriate shock during long-term follow-up (Table 2). An age < 65 years and secondary prevention ICD implantation indication significantly correlated with an increased risk, while a history of ischemic heart disease was associated with a reduced risk of inappropriate shocks in univariate analysis. However, in multivariate analysis, only an age < 65 years and documented supraventricular arrhythmia before implantation remained statistically significant predictors for inappropriate shocks (Table 2). In addition, factors associated with inappropriate shocks were also calculated in a per ICD analysis using the cox proportional hazards regression model. An age < 65 years (HR 2.8, 95%CI 1.3–6.3, p = 0.011) and documented supraventricular arrhythmias before implantation (HR 2.7, 95%CI 1.3–5.6, p = 0.008) were again significantly associated with an increased risk of inappropriate shock both in uni- and multivariate analysis. There was no difference in time to first inappropriate shock in patients with single versus dual chamber ICD in our study. To examine differences in inappropriate shock incidence according to device implantation date, we separated implanted ICDs (n = 249) to the median calendar implantation date (11.1.2006) and compared cumulative event rates of inappropriate shocks with Kaplan-Meier analysis, wherein no significant difference was observed.
3.6 Inappropriate shocks in subsequent devices
Fourteen patients experienced inappropriate shocks during the lifespan of their first ICD. Of these, five patients (35.7%) also suffered from inappropriate shocks in subsequent ICD devices, while only nine of 86 patients (10.5%) without inappropriate shocks during the lifespan of their first ICD experienced inappropriate shocks in later ICDs. The cumulative number and incidence of subsequent inappropriate shocks in subsequent devices were significantly higher in patients suffering from inappropriate shocks during the lifespan of their first ICD compared to patients experiencing no inappropriate shocks (p = 0.012 and p = 0.015, respectively). The cumulative event rate of inappropriate shocks was also significantly higher (p = 0.025) in patients with inappropriate shocks in their first ICD in the Kaplan-Meier analysis, but the continuous hazard assumption was not met. Patients with an inappropriate shock in their first ICD had a threefold higher mean incidence of inappropriate shocks during the remaining follow-up (0.3 vs 0.1 inappropriate shocks per year for patients with/without inappropriate shock in their first ICD device, p = 0.015).
4 Discussion
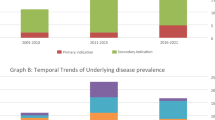
Our study with patients in clinical practice provides a long-term follow-up of an average 11.2 (± 3.6) years with an incidence of inappropriate shocks in 23% of ICD patients, which is considerably higher than reported in previous major clinical trials with shorter follow-up periods. The PainFREE Rx II trial reported an incidence of inappropriate shocks of 9% after 0.9 years of follow-up [13], while the multicenter automatic defibrillator implantation trial II (MADIT-II) reported an incidence of 12% after a 2-year follow-up in patients with ischemic cardiomyopathy [5], and the sudden cardiac death in heart failure trial (SCD-HeFT) including patients with dilated cardiomyopathy reported 17% after 3.8 years of follow-up [7]. Of note, a prolonged follow-up period generally appears to correlate with a higher reported incidence of inappropriate shocks in these studies, reflecting the continuously growing number of affected patients over time (Fig. 3). Unsurprisingly, the reported incidences of inappropriate shocks in context of the respective follow-up periods correlate well with the cumulative event rates during long-term follow-up in our study (6% at 1 year, 13% at 2 years, 16% at 5 years). Therefore, we suggest that the incidence of inappropriate shocks has previously been correctly reported concerning the observed periods, but clearly underestimated in the long-term because of the limited follow-up time of previous studies. In routine clinical practice reality, we often encounter patients carrying ICD’s for decades, and therefore, their long-term risk for an inappropriate shock may be estimated to be higher than in previous studies and around 20% based on our study results. This may affect risk-to-benefit evaluation of device therapy and patient-informed decision-making. On the other hand, our study may overestimate the incidence of inappropriate shocks due to the smaller patient population in comparison to larger clinical studies; however, the estimated incidence of inappropriate shock per ICD year was 0.1 in our study, which is within the reported estimated incidence of the prospective ADVANCE III trial with a much larger patient population [14].

The incidence of appropriate shocks was 45% in our study during a mean follow-up of 11.2 (± 3.6) years, which is similar to reported frequencies in trials from an equivalent time period [12], confirming valid, guideline compliant patient selection for ICD implantation. Also similar to previous studies, supraventricular arrhythmia misclassified as ventricular tachycardia was the main cause of inappropriate shock (74.8%) in our study with atrial fibrillation presenting the predominant etiology [11, 18, 19]. Despite an otherwise frequent cause of inappropriate shocks in ICD patients [20], sinus tachycardia represented the cause of only 12.2% of inappropriate shocks in our study, possibly reflecting the relatively high mean age of the population (60.1 ± 11.7 years), the high amount of beta blocker medication (90% of patients) and adequate ICD programming. While T wave oversensing accounted for 14.6% of all inappropriate shocks in our study, oversensing due to lead defects accounted for 9.8%, which is also comparable to previous studies [21, 22]. Higher shock zones, delayed therapy, telemonitoring, and various discriminating algorithms have been successfully introduced in the last decades to reduce inappropriate shocks due to supraventricular tachycardias and oversensing, but according to our study, they still remain the most significant mechanisms resulting in a substantial amount of inappropriate shocks in clinical practice [23,24,25,26]. Patients with younger age (age < 65 years: HR 5.1, CI 1.4–18.0, p = 0.012) and a history of supraventricular arrhythmia before ICD implantation (HR 2.5, CI 1.0–6.0, p = 0.041) were at increased risk for inappropriate shocks in our multivariate analysis, which is also consistent with previous studies [11, 19]. Younger ICD patients are known to be more prone to lead defects and sinus tachycardia due to their activity level [27], which may explain their excess risk of inappropriate shocks. Accordingly, all patients receiving an inappropriate shock for oversensing or sinus tachycardia in our study were below 65 years old. This highlights the importance of identifying patients at higher risk for inappropriate shocks before device implantation or during regular follow-up visits in order to identify possible optimization strategies in pharmacological treatment, device programming, electrophysiological ablation of arrhythmias, and telemonitoring. In addition, our study demonstrated an increased risk of inappropriate shocks in subsequent ICDs for patients who already experienced inappropriate shocks with their first device, warranting careful evaluation of potential optimization strategies but also ICD indication in the context of relevant comorbidities and life expectancy at the timepoint of a pulse generator exchange in this patient population.
Our study has several limitations. The number of included patients is small, which is partly overcome by a long follow-up period, and reported incidences match extrapolated expectations based on large studies with a much shorter follow-up. Additionally, the missing device programming parameters due to our retrospective study design reflect a shortcoming prohibiting any interpretation of our results concerning device settings. Finally, we cannot rule out underreporting of events in the cohort.
5 Conclusions
Inappropriate shocks remain an underestimated and frequent problem in ICD patients in clinical practice with an incidence that may exceed numbers of previously reported clinical trials with shorter follow-up periods. Affected patients or high-risk individuals need a holistic approach with evaluation of pharmacological treatment, device programming, electrophysiological ablation, telemonitoring, and even ICD indication at the time of indicated pulse generator exchange. We expect declining frequencies of inappropriate shocks in future ICD patients—not only because of ongoing technological improvements in detection and discrimination algorithms but also due to recent advances in device programming optimization and the advent of telemonitoring.
Abbreviations
- ICD:
-
Implantable cardioverter-defibrillator
- IAS:
-
Inappropriate shock
- SD:
-
Standard deviation
- SVT:
-
Supraventricular arrhythmia
References
Huikuri HV, Castellanos A, Myerburg RJ. Sudden death due to cardiac arrhythmias. N Engl J Med. 2001;345(20):1473–82. https://doi.org/10.1056/NEJMra000650.
Brachmann J, Hilbel T, Schols W, Beyer T, Schweizer M, Sterns L, et al. The implantable cardioverter/defibrillator (ICD). Developments up to the present time and future perspectives. Herz. 1994;19(5):246–50.
Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N Engl J Med. 1996;335(26):1933–40. https://doi.org/10.1056/NEJM199612263352601.
The Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N Engl J Med. 1997;337(22):1576–83.
Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346(12):877–83. https://doi.org/10.1056/NEJMoa013474.
Kadish A, Dyer A, Daubert JP, Quigg R, Estes NA, Anderson KP, et al. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med. 2004;350(21):2151–8. https://doi.org/10.1056/NEJMoa033088.
Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352(3):225–37. https://doi.org/10.1056/NEJMoa043399.
van Veldhuisen DJ, Maass AH, Priori SG, Stolt P, van Gelder IC, Dickstein K, et al. Implementation of device therapy (cardiac resynchronization therapy and implantable cardioverter defibrillator) for patients with heart failure in Europe: changes from 2004 to 2008. Eur J Heart Fail. 2009;11(12):1143–51. https://doi.org/10.1093/eurjhf/hfp149.
Priori SG, Blomstrom-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al. ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC) endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. 2015;36(41):2793–867.
Thomas SA, Friedmann E, Kao CW, Inguito P, Metcalf M, Kelley FJ, et al. Quality of life and psychological status of patients with implantable cardioverter defibrillators. Am J Crit Care. 2006;15(4):389–98.
van Rees JB, Borleffs CJ, de Bie MK, Stijnen T, van Erven L, Bax JJ, et al. Inappropriate implantable cardioverter-defibrillator shocks: incidence, predictors, and impact on mortality. J Am Coll Cardiol. 2011;57(5):556–62. https://doi.org/10.1016/j.jacc.2010.06.059.
Germano JJ, Reynolds M, Essebag V, Josephson ME. Frequency and causes of implantable cardioverter-defibrillator therapies: is device therapy proarrhythmic? Am J Cardiol. 2006;97(8):1255–61. https://doi.org/10.1016/j.amjcard.2005.11.048.
Sweeney MO, Wathen MS, Volosin K, Abdalla I, DeGroot PJ, Otterness MF, et al. Appropriate and inappropriate ventricular therapies, quality of life, and mortality among primary and secondary prevention implantable cardioverter defibrillator patients: results from the Pacing Fast VT REduces Shock ThErapies (PainFREE Rx II) trial. Circulation. 2005;111(22):2898–905. https://doi.org/10.1161/CIRCULATIONAHA.104.526673.
Gasparini M, Proclemer A, Klersy C, Kloppe A, Lunati M, Ferrer JB, et al. Effect of long-detection interval vs standard-detection interval for implantable cardioverter-defibrillators on antitachycardia pacing and shock delivery: the ADVANCE III randomized clinical trial. JAMA. 2013;309(18):1903–11. https://doi.org/10.1001/jama.2013.4598.
Gasparini M, Menozzi C, Proclemer A, Landolina M, Iacopino S, Carboni A, et al. A simplified biventricular defibrillator with fixed long detection intervals reduces implantable cardioverter defibrillator (ICD) interventions and heart failure hospitalizations in patients with non-ischaemic cardiomyopathy implanted for primary prevention: the RELEVANT [role of long dEtection window programming in patients with LEft VentriculAr dysfunction, non-ischemic eTiology in primary prevention treated with a biventricular ICD] study. Eur Heart J. 2009;30(22):2758–67. https://doi.org/10.1093/eurheartj/ehp247.
Steinberg JS, Martins J, Sadanandan S, Goldner B, Menchavez E, Domanski M, et al. Antiarrhythmic drug use in the implantable defibrillator arm of the Antiarrhythmics Versus Implantable Defibrillators (AVID) Study. Am Heart J. 2001;142(3):520–9. https://doi.org/10.1067/mhj.2001.117129.
Gilliam FR, Hayes DL, Boehmer JP, Day J, Heidenreich PA, Seth M, et al. Real world evaluation of dual-zone ICD and CRT-D programming compared to single-zone programming: the ALTITUDE REDUCES study. J Cardiovasc Electrophysiol. 2011;22(9):1023–9. https://doi.org/10.1111/j.1540-8167.2011.02086.x.
Daubert JP, Zareba W, Cannom DS, McNitt S, Rosero SZ, Wang P, et al. Inappropriate implantable cardioverter-defibrillator shocks in MADIT II: frequency, mechanisms, predictors, and survival impact. J Am Coll Cardiol. 2008;51(14):1357–65. https://doi.org/10.1016/j.jacc.2007.09.073.
Theuns DA, Klootwijk AP, Simoons ML, Jordaens LJ. Clinical variables predicting inappropriate use of implantable cardioverter-defibrillator in patients with coronary heart disease or nonischemic dilated cardiomyopathy. Am J Cardiol. 2005;95(2):271–4. https://doi.org/10.1016/j.amjcard.2004.09.017.
Jodko L, Kornacewicz-Jach Z, Kazmierczak J, Rzeuski R, Zielonka J, Kaliszczak R, et al. Inappropriate cardioverter-defibrillator discharge continues to be a major problem in clinical practice. Cardiol J. 2009;16(5):432–9.
Rauwolf T, Guenther M, Hass N, Schnabel A, Bock M, Braun MU, et al. Ventricular oversensing in 518 patients with implanted cardiac defibrillators: incidence, complications, and solutions. Europace. 2007;9(11):1041–7.
Occhetta E, Bortnik M, Magnani A, Francalacci G, Marino P. Inappropriate implantable cardioverter-defibrillator discharges unrelated to supraventricular tachyarrhythmias. Europace. 2006;8(10):863–9.
Moss AJ, Schuger C, Beck CA, Brown MW, Cannom DS, Daubert JP, et al. Reduction in inappropriate therapy and mortality through ICD programming. N Engl J Med. 2012;367(24):2275–83. https://doi.org/10.1056/NEJMoa1211107.
Guedon-Moreau L, Kouakam C, Klug D, Marquie C, Brigadeau F, Boule S, et al. Decreased delivery of inappropriate shocks achieved by remote monitoring of ICD: a substudy of the ECOST trial. J Cardiovasc Electrophysiol. 2014;25(7):763–70. https://doi.org/10.1111/jce.12405.
Klein GJ, Gillberg JM, Tang A, Inbar S, Sharma A, Unterberg-Buchwald C, et al. Improving SVT discrimination in single-chamber ICDs: a new electrogram morphology-based algorithm. J Cardiovasc Electrophysiol. 2006;17(12):1310–9. https://doi.org/10.1111/j.1540-8167.2006.00643.x.
Duru F, Bauersfeld U, Candinas R. Avoiding inappropriate ventricular tachycardia detection due to T-wave oversensing in an implantable cardioverter defibrillator: a novel application of the electrogram width criterion. Europace. 2001;3(1):80–4.
Kleemann T, Becker T, Doenges K, Vater M, Senges J, Schneider S, et al. Annual rate of transvenous defibrillation lead defects in implantable cardioverter-defibrillators over a period of >10 years. Circulation. 2007;115(19):2474–80. https://doi.org/10.1161/CIRCULATIONAHA.106.663807.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was conducted according to the principles expressed in the Declaration of Helsinki of 1964, as revised in 2013, and was in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national). Patient consent was not required, since data was collected and analyzed retrospectively as well as anonymously, and there were no new procedural studies undertaken due to the retrospective study design. This article does not contain any new studies with human subjects performed by any of the authors. The local ethical committee (Kantonale Ethikkomission Zürich) approved the study in advance.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published.
Disclosures
Dr. Hofer reports educational and travel funds from St. Jude Medical and Biosense Webster. Dr. Krasniqi and Prof. Eriksson report research grants and educational funds from Boston Scientific, St. Jude Medical, Medtronik, and Biotronik. Dr. Hürlimann reports speaker honoraria and consulting fees from Biotronik, Boston Scientific, LivaNova, Medtronic, and St. Jude Medical. Dr. Haegeli reports speaker honoraria and consulting fees from St. Jude Medical. Dr. Steffel has received consultant and/or speaker fees from Amgen, Astra-Zeneca, Atricure, Bayer, Biosense Webster, Biotronik, Boehringer-Ingelheim, Boston Scientific, Bristol-Myers Squibb, Cook Medical, Daiichi Sankyo, Medtronic, Novartis, Pfizer, Sanofi-Aventis, Sorin, St. Jude Medical, and Zoll. Dr. Steffel is co-director of CorXL. He has received grant support through his institution from Bayer Healthcare, Biosense Webster, Biotronik, Boston Scientific, Daiichi Sankyo, Medtronic, and St. Jude Medical. Prof. Duru reports institutional funds from Boston Scientific, Biotronik, St. Jude Medical, Biosense Webster, and Medtronic. All other authors report no relationships to disclose.
Rights and permissions
About this article

Cite this article
Hofer, D., Steffel, J., Hürlimann, D. et al. Long-term incidence of inappropriate shocks in patients with implantable cardioverter defibrillators in clinical practice—an underestimated complication?. J Interv Card Electrophysiol 50, 219–226 (2017). https://doi.org/10.1007/s10840-017-0297-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-017-0297-8