
Abstract
This paper frames how parents’ health problems may affect a child’s subsequent working status. Parental health problems occurring in their prime working years undermine an adult child’s resources and tend to affect the child’s preferences over time-allocations among leisure, market- and non-market-labor. Empirical applications in this paper focus on a situation with pervasive health problems, lack of social safety network, and a substantial gender gap in labor market return. Exploiting Russia Longitudinal Monitoring Survey (RLMS) for the period 1994–2004, empirical results indicate that a father’s poor health status is a significant predictor of lowering a daughter’s educational attainment and working probability during her subsequent, adulthood years.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Intergenerational transfers of time and money are prevalent in both developing countries (Lillard and Willis 1997; Lee et al. 1994; Logan and Bian 2003) and developed countries (Bianchi et al. 2006; Couch et al. 1999; McGarry and Schoeni 1995; Sloan et al. 2002). Parental life-course characteristics such as health have a more noticeable effect on age-patterns in receipt of parental support than do adult child factors (Cooney and Uhlenberg 1992).
As many societies experience the aging-population phenomenon, much of the recent attention to family support has focused on care-giving for elderly parents (Caputo 2002; McGarry 1998; Piette et al. 2010). Some studies show that time spent on informal care increases significantly if parents suffer chronic illness (Langa et al. 2002a, b, c) and that long-term care from adult children can adversely affect those care-givers’ health (Coe and Houtven 2009; Lai and Leonenko 2007) and labor supply (Ettner 1995, 1996; Navaie-Waliser et al. 2002). However, little research exists on exploring parental health problems occurring in parents’ middle age and adult children’s subsequent labor market behaviors.
Limited working conditions or job loss due to health problems can result in substantially lower family income (Smith 1999). If parents’ health deteriorates in their middle age, such care-giving need, in addition to family income decline, not only can affect a child’s short-term time allocation but also can reshape the long-term trajectory of economic behavior due to reduced investment in the child’s education and health.
In this paper, I depict an economic framework to discuss pathways in the relationship between parents’ health problems and their children’s subsequent working status. For empirical application of the economic model, I explore the Russia Longitudinal Monitoring Survey (RLMS), for the period 1994–2004, which provides important and interesting features. First, Russia experienced severe, pervasive health problems during that period; men of prime working age suffered most (Becker and Bloom 1998; Brainerd and Cutler 2005; Shkolnikov et al. 1998). Second, return to schooling increased, especially among the younger generation (Gorodnichenko and Peter 2005). Therefore, interruption of a child’s schooling is likely to reduce his or her future labor market returns. Third, a significant gender gap existed in the labor market, leading to differences between sons’ and daughters’ behavioral responses in the labor market (Brainerd 1998, 2000; Linz 1995, 1996; Ogloblin 1999). Fourth, substantial fluctuations occurred in the social safety network system and other government policies; in such a situation, Russian families were more likely to rely on informal networks (Cox et al. 1997; Kennedy et al. 1998).
This paper is organized thus: section “A Framework: Intergenerational Health Implications in the Labor Market” addresses an economic framework to understand the mechanism of an adult child’s time allocation associated with parental health problems, and discusses implications for the adult child’s resulting labor supply. Section “Empirical Application: Parents’ Health, Children’s Education and Working Probability” provides empirical applications exploring the RLMS. Section “Summary” summarizes and discusses implications arising from the economic model and empirical findings. Section “Limitations and Discussions” addresses the study’s limitations.
A Framework: Intergenerational Health Implications in the Labor Market
Overview
Parents’ resources play a major role in mitigating economic hardship, especially among young adults (Cooney and Uhlenberg 1992; McGarry and Schoeni 1995; Schoeni 1997). Economic transfers from parents to adult children can be reduced significantly if the parents encounter health problems, and even can trigger upstream transfers from children to parents (Lee et al. 1994; Lillard and Willis 1997; Sloan et al. 2002). Exhaustive theoretical works underline intergenerational economic linkage (Bergstrom 1997; Laitner 1993) and explain the motivation behind intergenerational transfers (Arrondel and Masson 2006; Koh and MacDonald 2006). Some studies suggest that women’s market activity is reduced by care-giving duty towards chronically ill parents (Lai and Leonenko 2007; Pagani and Marenzi 2008).
Because this paper explores a long-term association as well as a short-term association, it might be natural to seek a model of intergenerational economic linkage in an inter-temporal or dynamic programming. However, such a model might not effectively explain behaviors of a family with a binding budget constraint in a situation with limited social safety network plus substantial uncertainty in market variables. Moreover, the main explanatory variable of interest in this paper is parents’ health status which might not be perfectly perceived nor well predicted by children.
Figure 1 presents an overview of economic framework which comprises two parts: intergenerational economic linkage and time allocation. With parental health problems, an adult child has greater preference for transferring money or time to unhealthy parents (I-A); this will reshape the child’s utility function. Note that market income per unit of labor is constant but non-market labor productivity increases due to a greater opportunity cost as care-giving for unhealthy parents is needed (I-B). Because of reduced parental resources, a child’s human capital level is lower with unhealthy parents (I-C), as is transfer from parents to child (I-D). Consequently, the indifference curve will be reshaped (II-A). The production curve slope will be changed via the substitution effect (II-B), and the level of production possibility is changed via the income effect (II-C). As a result, an adult child’s optimal time allocation will be changed to maximize his or her utility under the new preference and production possibility frontier.

Overview of the economic framework association between parental health and adult children’s working status
Intergenerational Economic Linkage
In this paper, altruism is assumed as the baseline motivation of intergenerational transfer especially associated with health problems. And I assume that the parent–adult child pair plays a non-cooperative game—in other words, an adult child maximizes utility by taking as given the actions of parents. Let X i be a commodity that contributes to child i’s utility. Note that commodity here not only includes a commodity consumed directly by the individual, but also transfers to others (such as transfers to parents). U i is the utility function which contains two parts: utility from the child’s own consumption (u i ), and the perceived utility of parents (\( u_{i}^{p} \)).
I assume that an adult child does not know the exact amount of parents’ consumption but conjectures it as \( \tilde{X}_{p} \) before he or she transfers. The adult child transfers a part of the commodity to parents by the fraction of t ip which ranges from 0 inclusively to 1 exclusively. Suppose the perceived parents’ utility can be additive with a proportional adjustment by ρ for simplicity. Then the child’s utility function can be specified.
I assume that the more altruistic child is more conscious of parents’ consumption level—in other words, a greater ρ.
Time Allocation and Labor Supply
The baseline framework for time allocation in this paper borrows from Gronau (1977). An adult child’s time allocation among consumption (i.e., leisure), non-market labor and market labor will be determined, so as to maximize utility from the amount of commodity (X).
The production function in this paper focuses on individual production rather than on joint production of parents and children. The commodity (X) is a combination of goods/services and consumption time (or leisure). Goods and services can be obtained by market-labor income and home production. Therefore, an adult child’s available time will be used to earn market-labor income (M), to produce home-goods/services (N) or to consume goods/services (L).
In sum, a child’s production curve is characterized by market labor productivity (W), non-market labor productivity (f′), and external resources (V). Optimal time allocation will be determined to maximize the child’s utility given the production curve. Focusing on labor supply, the amount of time allocated to market labor (M*) of an adult child can be expressed as:
Empirical Application: Parents’ Health, Children’s Education and Working Probability
Background of Russian Families During Health and Economic Crisis
For application of the economic model, I explore families in Russia during its economic reform period—1990s and early 2000s. Health problems in Russia during the early transition period, 1991–1995, have received considerable attention due to a sharp increase in mortality rate, concentrated disproportionately among prime-working-age men (Becker and Bloom 1998; Brainerd and Cutler 2005; Shkolnikov et al. 1998). Since 1994, lack of money has emerged clearly as the primary obstacle to obtaining prescribed medications (Zohoori 2004). To mitigate economic hardship, Russian families were more likely to rely on informal sources (family and friends) to alleviate day-to-day problems (Cox et al. 1997; Kennedy et al. 1998). During the pension crisis in 1996 and financial crisis in 1998, families tended to increase total family labor supply and to sell assets (Jensen and Richter 2003), men tended to seek supplementary jobs to compensate for lowered family income, and women tended to reduce expenditure or to turn to relatives for help (Lokshin and Yemtsov 2001). Some studies also provide evidence of the significantly lower labor return for women in Russia (Brainerd 1998, 2000; Linz 1995; Ogloblin 1999) and those gender differences in earnings are not explained by educational attainment (Linz 1996).
Data and Sample
The Russia Longitudinal Monitoring Survey (RLMS) is a series of nationally representative surveys designed to monitor the effects of Russian reforms on the health and economic welfare of households and individuals in the Russian Federation. The RLMS has been organized and coordinated by fellows of the Carolina Population Center at the University of North Carolina at Chapel Hill. Since 1995, numerous academic papers and reports have been published using the RLMS (for the list of publications: http://www.cpc.unc.edu/projects/rlms/papers.html).
RLMS Phase II is a longitudinal study of populations of dwelling units—some 4,000 households—beginning in 1994 and ongoing. Relating to general health assessment, it asks ‘How would you evaluate health—Very good, good, average, bad or very bad?’ A poor health indicator in this paper is created based on this self-rated health status by assigning value one for the health status, bad or very bad. Regarding employment status, a working indicator is created based on the question, ‘Do you now work?’
A dwelling-unit-based, longitudinal design of RLMS allows us to track individuals if they remain in the same dwelling unit as in the baseline year. To explore the long-term relationship of parental health and adult children’s working status as well as the short-term relationship, the sample is restricted to those (i) whose mothers were aged 35–55 in 1994, (ii) who themselves were aged 13–29 in 1994, i.e., 23–39 in 2004, (iii) who lived with both parents in 1994 and (iv) who remained in the same dwelling unit between 1994 and 2004. Table 1 presents the overall sample summary for empirical estimations: Conditional on living with both parents in 1994, 884 children aged 13–29 are identified. With additional sample restriction of living in the same dwelling unit between 1994 and 2004, I have 385 children in the analyzed sample for estimation. Potential problems associated with sample selection will be discussed more in section “Limitations and Discussions” and in Appendices.
Specification and Estimations
Suppose market labor productivity (W) and non-market labor productivity (f’) are functions of demographic characteristics (D), health (H), and schooling (S). Then Eq. 2 will be reduced thus:
External resources of an adult child (V) comprise private transfers (such as family support) and governmental transfers. For simplicity, I assume that parental transfers are the only source of the private transfer. By denoting parents as p and government as g, external resources can be expressed so:
Transfers from parents (V p ) depend on relative economic status of parents and the adult child. Suppose economic status of parents and the adult child is a function of demographic characteristics (D p , D i ), health (H p , H i ) and schooling (S p , S i ). Then the Eq. 3 can be reduced further as:
For estimation, baseline demographic covariates include the child’s own age and region in 1994. In addition, parents’ education level and poverty level measured in 1994 will be included to control for baseline socio-economic characteristics. Reflecting the limited safety network in Russia during this analysis period, I assume zero transfers from government (V g ). Individual’s utility and preference are not observable and are assumed as the same for all children.
Parents’ Health and Adult Children’s Education
The analyzed sample in this paper includes relatively young adult children (age 13–29) at the base year, 1994. Accordingly, before I examine working status of those adult children, it is necessary to explore the status of schooling of the analysis sample. Figure 2 presents overall patterns of children’s schooling for 1994–2004 by parents’ health conditions in 1994. Overall, the majority of children in the analyzed sample completed schooling by 2000: less than 10% of children in the analyzed sample are still in school in 2000 and less than 1% in 2004.

Ratio of in-school 1994–2004: by parents’ health status in 1994 (age 13–29 in 1994, longitudinal). a Sons’ in-school ratio. b Daughters’ in-school ratio. Note: Sample is restricted to children aged 13–29 in 1994, (i) whose mothers were aged 35–55 in 1994, (ii) who lived with both parents in 1994 and (iii) who remained in the same dwelling unit between 1994 and 2004
This descriptive figure also shows that those with unhealthy parents are less likely to be in school during most sample periods. To explore whether there is a significant relationship between parental health and completed schooling level after controlling for baseline covariates measured in 1994, I specify an estimation equation for the long-term relationship between parental health and schooling as:
\( S_{i,2004} \) denotes an adult child’s years of schooling completed in 2004, \( H_{{{\text{p}},1994}} \) represents parental health measured in 1994, \( B_{ 1994} \) contains baseline characteristics such as the child’s age, health, poverty level, region and parents’ education measured in 1994.
After controlling for baseline characteristics in 1994, estimated coefficients from the probit model and adjusted predicted probabilities are presented in Table 2. With an unhealthy father in 1994, the probability of obtaining higher schooling level is significantly lower for daughters: with a healthy father, the predicted probability of obtaining higher education until 2004 is 70% but with unhealthy father is only 35% for daughters. Regardless of parental health status, the probability of a son obtaining higher education remains between 30 and 35%.
One might conjecture that such gender difference in educational attainment responding to parental health status is a result of family investment behavior based on return to schooling. However, there is no evidence on gender gap in return to schooling in the study cohort (see Appendix Table 5). Rather, the substantial gender gap in labor-market outcome (see Appendix Fig. 5) is attributable to occupational and industrial segregation by gender (Ogloblin 1999).
Parents’ Health and Adult Children’s Subsequent Working Probability
Short-Term Relationship
I first examine a short-term association between parental health problem and adult children’s working status. More specifically, I explore whether parental health in the preceding year (t − 1) is significantly related with working status of an adult child in the current year (t) after controlling for parental health in two-years prior (t − 2). Baseline covariates such as children’s age, health status, poverty level, region and parent’s education level are included as controls. Given that the majority of adult children had completed schooling around 2000, the analysis sample period for this short-term relationship is 2000–2004. Equation 7 shows the estimation specification.
where t = 2000–2004; M it denotes an adult child’s time spent in the labor market in year t; \( H_{p,t - 1} \) represents parental health measured in t – 1; \( H_{p,t - 2} \) represents parental health measured in t – 2; and \( B_{ 1994} \) contains baseline characteristics such as the adult child’s age, health, poverty level, region and parents’ education measured in 1994.
As summarized in Table 3, a father’s poor health in year t − 1 is a significant predictor of lower probability of a daughter’s working status (coefficient: −0.405). The probability of working in year t is 47% if she had an unhealthy father in year t − 1; that probability is 62% if she had an healthy father in year t − 1.
Long-Term Relationship
To estimate the long-term relationship between parental health and adult children’s working status, I specify estimate equation as:
\( M_{\text{i,2004}} \) denotes an adult child’s time spent in the labor market in year 2004; \( H_{p,1994} \) represents parental health measured in 1994; and \( B_{ 1994} \) contains baseline characteristics such as the adult child’s age, health, poverty level, region and parents’ education measured in 1994.
Table 4 summarizes the estimate results on adult children’s working probability in 2004. It shows a father’s poor health status is a significant predictor of lowering a daughter’s working probability in her adulthood: The predicted probability of a daughter working in 2004 is 34% if she had an unhealthy father in 1994, while that probability is 71% if she had a healthy father in 1994.
I also estimate the same working equation after controlling for the adult child’s completed education in 2004 to check whether such a significant long-term relationship has been mediated by the education channel.
\( M_{\text{i,2004}} \) denotes an adult child’s time spent in the labor market in year 2004; \( H_{p,1994} \) represents parental health measured in 1994, \( S_{i,2004} \) represents the adult child’s schooling years completed in 2004; and \( B_{ 1994} \) contains baseline characteristics such as the adult child’s age, health, poverty level, region and parents’ education measured in 1994. After controlling for the child’s education completed by 2004, the magnitude of relationship between parental health and children’s working status decreases but remains significant for daughters (Coefficient: −0.776, Daughter’s predicted probability of working: 72% if a father’s health is good in 1994 and 42% if a father’s health is poor in 1994).
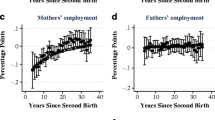
Figure 3 presents the predicted probabilities of working in each year 1994–2004. All baseline covariates (\( B_{ 1994} \)) are evaluated at mean values. Shaded areas in the Fig. 3 indicate significant gaps in working probabilities between good and poor parental health at 5% significant level. In general, mother’s health in 1994 is not a significant predictor of adult children’s working status, except with a marginal significance in 2001 for sons. The working probability of a daughter is significantly lower in most years since 1998 if she had an unhealthy father in 1994.

Adjusted predicted probability of working 1994–2004: by parents’ health in 1994 (age 13–29 in 1994, longitudinal). a Sons’ working probability. b Daughters’ working probability. Notes: Sample is restricted to children aged 13–29 in 1994 (i) whose mothers were aged 35–55 in 1994, (ii) who lived with both parents in 1994 and (iii) who remained in the same dwelling unit between 1994 and 2004. Equation 8a is the estimation specification. Baseline covariates are evaluated at mean values. Shaded areas indicate significant difference at 5% significance level
Empirical Application Within the Economic Framework
In this section, I discuss how empirical results can be driven in the economic framework addressed in this paper. Women in Russia had more housework obligations than do men, which might be the main factor resulting in gender differences in labor earnings (Ofer and Vinokur 1981). In contrast, women’s labor participation in Russia was as high as men’s, but women’s working hours were significantly lower than men’s (Ogloblin 1999).
Reflecting these specific situations, Fig. 4 illustrates how different working outcomes between adult sons and daughters can be driven: initially both an adult son (with choice c) and an adult daughter (with choice d) work in the market, but a son’s working hours are greater than a daughter’s, and a daughter’s choice is closer to the threshold between non-market work and market work (m d ).

Parental poor health impacts on an adult son’s and an adult daughter’s optimal time allocation. Initial assumptions/conditions: same preference between son and daughter (i.e., same indifference curve); same non-market labor productivity between son and daughter (i.e., same shape of non-market production curve); greater market return for son (i.e., steeper slope in market production line for son); and both son and daughter working in the market (although son spends more time in the market than does daughter, due to gender gap in market labor return)
With parents’ health problems, both son and daughter have greater utility from transferring commodity to the unhealthy parent (e.g., greater ρ in Eq. 1). A daughter’s market labor productivity (marginal labor return) decreases due to lower educational attainment, while a son’s market productivity (marginal labor return) is not affected. Non-market labor productivities for both son and daughter increase because of care-giving for unhealthy parents, the substitute (such as medical care) for which is an expensive commodity. This might be even truer for a daughter than a son in a society in which a woman is specialized in non-market labor but a man in market labor. As a result, responding to parental health problems, a daughter is less likely to work (from d to d′ in Fig. 4) in the market than is a son (from c to c′).
Summary
This paper explores the relationship between parents’ health and their adult children’s working status in an economic framework of intergenerational transfers and time allocation. Empirical applications in this paper exploit a situation with significant gender gap in the labor market, pervasive health problems especially among working age men, lack of medical service and social safety network, and high poverty rate, in which informal transfers play significant roles in mitigating families’ and individuals’ economic hardships. Empirical results indicate that a daughter is less likely to obtain higher education and less likely to work in the market during subsequent years if she has an unhealthy father.
Limitations and Discussions
The economic model provides a framework of how individuals adjust their optimal time-allocations responding to parental health problems. However, some important questions are not explored explicitly in this paper due to the limitation of the study.
First, this paper does not explicitly examine roles of government transfers or changes of market conditions, understanding government transfers is necessary to predict directions and magnitude of the effect of parental health problems on adult children’s economic behaviors. Suppose a governmental transfer to ill persons replaces the intergenerational transfer associated with health problems; then we might not observe adult children’s behavioral responses as much as we otherwise might. And, if the market has a lower gender gap in marginal labor return, the difference in working behavior between son and daughter responding to parents’ health problems is likely to decrease.
Second, despite a substantial gender gap in market earning, there is no evidence on return to schooling in the study cohort (see Appendix Table 5 and Appendix Fig. 5). Thus, this paper cannot explain different parental health effects on schooling outcomes between son and daughter on the basis of return to schooling. A plausible answer is that the family believes a daughter has greater productivity in non-market-labor or a daughter’s care-giving is more socially prevalent and acceptable, which results in preference of daughter rather than son for informal care and other related home production.
Third, at least to some degree, family members might pool their resources and might allocate efforts based on relative labor productivity (Becker 1985) among son, daughter, mother and father, which might enhance the different response in working status between son and daughter. For example, based on differences in market labor return by gender and age cohorts of the study (see Appendix Fig. 6) if a father is ill, it should be the case that son or mother works in the market to compensate for lowered family income, and a daughter becomes a care-giver for the ill father. Such a division of labor in the allocation of time might occur in extended relationships such as marriage. Suppose a married woman is mainly responsible for non-market works including caring for parents-in-law. In such a case, a married adult son’s non-market labor productivity might not respond to his ill parents. Consequently, a son tends to spend more time in the market responding only to adverse income effect.
Fourth, how about the roles of competing events such as having children and having an unhealthy mother-in-law or father-in-law? For example, a sandwiched care-giver might have different preference of employment (Rubin and White-Means 2009) and at the same time different time restrictions in market activity (Pagani and Marenzi 2008) compared to the not sandwiched care-giver. The relationship between adult children and their own parents’ health problems might be affected as adult children allocate their time not only for their own unhealthy parents but also for other family members (e.g., their own children, mother-in-law, father-in-law).
Fifth, estimating labor supply at an extensive margin (e.g., labor participation) rather than at an intensive margin (e.g., hours of working), the analysis does not fully capture changes in time spent on labor supply. For example, if a daughter’s optimal choice is near the threshold between market and non-market labor, compared to a son’s, we tend to observe more variations from a daughter’s behavioral responses.
Sixth, to examine a mother’s and a father’s health at the same time in each estimation model, the main empirical analysis in this paper includes adult children only if they lived with both mother and father in the baseline year. In other words, the analyzed sample excludes those children living with one parent and those non-coresident with parent/s. Appendix 1 provides a supplementary analysis which examines all mothers’ and fathers’ health status regardless of parent/s’ marital status and regardless of coresident status with those children. Overall results from this supplementary analysis are consistent with findings in the main analysis.
Seventh, due to the RLMS restriction of dwelling-unit-based longitudinal design rather than individual-based, the subsequent working status of adult children cannot be observed if the adult children moved out from the initial dwelling units. This might limit the implication of empirical results only to children who live in the same dwelling unit for several years. Although this sample selection might not be overcome completely, I provide a couple of auxiliary analyses to deal with such an issue and summarize results in Appendix 2.
This paper suggests the plausibility of significant relationships between parents’ health and children’s subsequent working status. To understand the full mechanism of spill-over health impacts on economic behaviors and potential policy implications, more theoretical work and empirical work are needed.
References
Altonji, J. G., Elder, T. E., & Taber, C. R. (2005). Selection on observed and unobserved variables: Assessing the effectiveness of catholic schools. Journal of Political Economy, 113, 151–184.
Arrondel, L., & Masson, A. (2006). Altruism, exchange or indirect reciprocity: What do the data on family transfers show? In S. Kolm & J. M. Ythier (Eds.), Handbook of the economics of giving, altruism and reciprocity (Vol. 1, pp. 971–1053). Amsterdam: Elsevier.
Becker, G. S. (1985). Human capital, effort, and the sexual division of labor. Journal of Labor Economics, 3(1), S33–S58.
Becker, C., & Bloom, D. (1998). The demographic crisis in the former Soviet Union: Introduction. World Development, 26(11), 1913–1919.
Bergstrom, T. (1997). A survey of theories of the family. In M. R. Rosenzweig & O. Stark (Eds.), Handbook of population and family economics (pp. 21–79). Amsterdam: Elsevier.
Bianchi, S. M., Hotz, J. V., McGarry, K., & Seltzer, J. A. (2006). Intergenerational ties: Alternative theories, empirical findings and trends, and remaining challenges. In A. Booth, A. C. Crouter, S. Bianchi, & A. Seltzer (Eds.), Intergenerational caregiving (pp. 3–43). Washington, DC: Urban Institute.
Brainerd, E. (1998). Winners and losers in Russia’s economic transition. American Economic Review, 88(5), 1094–1116.
Brainerd, E. (2000). Women in transition: Changes in gender wage differentials in Eastern Europe and the former Soviet Union. Industrial and Labor Relations Review, 54(1), 138–162.
Brainerd, E., & Cutler, D. M. (2005). Autopsy on an empire: Understanding mortality in Russia and the former Soviet Union. Journal of Economic Perspectives, 19(1), 107–130.
Caputo, R. K. (2002). Adult daughters as parental caregivers: Rational actors versus rational agents. Journal of Family and Economic Issues, 23(1), 27–50.
Coe, N. B., & Houtven, C. V. (2009). Caring for mom and neglecting yourself? The health effects of caring for an elderly parent. Health Economics, 18(9), 991–1010.
Cooney, T. M., & Uhlenberg, P. (1992). Support from parents over the life course: The adult child’s perspective. Social Forces, 71(1), 63–84.
Couch, K. A., Daly, M. C., & Wolf, D. A. (1999). Time? Money? Both? The allocation of resources to older parents. Demography, 36(2), 216–232.
Cox, D., Eser, Z., & Jimenez, E. (1997). Family safety nets during economic transition. In J. Klugman (Ed.), Poverty in Russia: Public policy and private response (pp. 211–249). Washington, DC: World Bank.
Ettner, S. L. (1995). The impact of “Parent care” on female labor force decisions. Demography, 32, 63–80.
Ettner, S. L. (1996). The opportunity costs of eldercare. Journal of Human Resources, 31, 189–201.
Gorodnichenko, Y., & Peter, K. S. (2005). Returns to schooling in Russia and Ukraine: A semiparametric approach to cross-country comparative analysis. Journal of Comparative Economics, 33, 324–350.
Gronau, R. (1977). Leisure, home production, and work—the theory of the allocation of time revisited. Journal of Political Economy, 85(6), 1099–1123.
Jensen, R. T., & Richter, K. (2003). The health implications of social security failure: Evidence from the Russian pension crisis. Journal of Public Economics, 88, 209–236.
Kennedy, B. P., Kawachi, I., & Brainerd, E. (1998). The role of social capital in the Russian mortality crisis. World Development, 26(11), 2029–2043.
Koh, S.-K., & MacDonald, M. (2006). Financial reciprocity and elder care: Interdependent resource transfers. Journal of Family and Economic Issues, 27, 420–436.
Lai, D. W., & Leonenko, W. (2007). Effects of caregiving on employment and economic costs of Chinese family caregivers in Canada. Journal of Family and Economic Issues, 28, 411–427.
Laitner, J. (1993). Intergenerational and interhousehold economic links. In M. R. Rosenzweig & O. Stark (Eds.), Handbook of population and family economics (pp. 189–238). Amsterdam: Elsevier.
Langa, K., Fendrick, A. M., Flaherty, K. R., Martinez, F. J., Kabeto, M. U., & Saint, S. (2002a). Informal caregiving for chronic lung disease among older Americans. Chest, 122(6), 2197–2203.
Langa, K. M., Fultz, N. H., Saint, S., Kabeto, M. U., & Herzog, A. R. (2002b). Informal caregiving time and costs for urinary incontinence in older individuals in the United States. Journal of American Geriatrics Society, 50(4), 733–737.
Langa, K., Vijan, S., Hayward, R. A., Chernew, M. E., Blaum, C. S., Kabeto, M. U., et al. (2002c). Informal caregiving for diabetes and diabetic complications among elderly Americans. Journal of Gerontology, 57B(3), S177–S186.
Lee, Y.-J., Parish, W. L., & Willis, R. J. (1994). Sons, daughters, and intergenerational support in Taiwan. The American Journal of Sociology, 99(4), 1010–1041.
Lillard, L. A., & Willis, R. J. (1997). Motives for intergenerational transfers: Evidence from Malaysia. Demography, 34(1), 115–134.
Linz, S. J. (1995). Russian labor market in transition. Economic Development and Cultural Change, 43(4), 693–716.
Linz, S. J. (1996). Gender differences in the Russian labor market. Journal of Economic Issues, 30(1), 161–185.
Logan, J. R., & Bian, F. (2003). Parents’ need, family structure, and regular intergenerational financial exchange in Chinese cities. Sociological Forum, 18(1), 85–101.
Lokshin, M. M., & Yemtsov, R. (2001). Household strategies for coping with poverty and social exclusion in post-crisis Russia. World Bank, Policy Research Working Paper 2556.
McGarry, K. (1998). Caring for the elderly: The role of adult children. In D. A. Wise (Ed.), Inquiries in the economics of aging (pp. 133–163). Chicago: University of Chicago Press.
McGarry, K., & Schoeni, R. (1995). Transfer behavior in the health and retirement study: Measurement and redistribution of resources within the family. Journal of Human Resources, 30, S184–S226.
Navaie-Waliser, M., Spriggs, A., & Feldman, P. H. (2002). Informal caregiving: Differential experiences by gender. Medical Care, 40(12), 1249–1259.
Ofer, G., & Vinokur, A. (1981). Earnings differentials by sex in the Soviet Union: A first look. In S. Rosefielde (Ed.), Economics welfare and the economics of Soviet socialism (pp. 127–162). Cambridge: Cambridge University Press.
Ogloblin, C. G. (1999). The gender earnings differential in the Russian transition economy. Industrial and Labor Relations Reviews, 52(4), 602–627.
Pagani, L., & Marenzi, A. (2008). The labor market participation of sandwich generation Italian women. Journal of Family and Economic Issues, 29, 427–444.
Piette, J. D., Rosland, A. M., Silveira, M., Kabeto, M., & Langa, K. M. (2010). The case for involving adult children outside of the household in the self-management support of older adults with chronic illnesses. Chronic Illness, 6, 34–45.
Rubin, R. M., & White-Means, S. I. (2009). Informal caregiving: Dilemmas of sandwiched caregivers. Journal of Family and Economic Issues, 30, 252–267.
Schoeni, R. F. (1997). Private interhousehold transfers of money and time: New empirical evidence. Review of Income and Wealth Series, 43(4), 423–448.
Shkolnikov, V. M., Cornia, G. A., Leon, D. A., & Mesle, F. (1998). Causes of the Russian mortality crisis: Evidence and interpretations. World Development, 26(11), 1995–2011.
Sloan, F. A., Zhang, H. H., & Wang, J. (2002). Upstream intergenerational transfers. Southern Economic Journal, 69(2), 363–380.
Smith, J. P. (1999). Healthy bodies and thick wallets: The dual relation between health and economic status. Journal of Economic Perspectives, 13(2), 145–166.
Zohoori, N. (2004). Monitoring health conditions in the Russian Federation—the Russian longitudinal monitoring survey 1992–2003. Chapel Hill: University of North Carolina at Chapel Hill.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 1: Parents’ Physical Limitations and Adult Children’s Working Probability (Including Both Coresident and Non-Coresident Children)
For non-coresident adult children, we do not have parents’ health information responded by parents themselves. The RLMS, however, surveyed time-use for 1994–1997, and asked respondents whether their parents are older than 50 and need help for daily activities. By utilizing this, I examine parental health and adult children’ working status after controlling for adult children’s own schooling level and health status, as well as other demographic covariates (adult children’s age, marital status, coresident indicator and regions) in the estimation.
Children’s age is restricted to 20–39 to replicate a similar age group of adult children analyzed in the main analysis. About 6% of adult children have a mother needing help for daily activity and about 5% have such a father. Using the probit model, I estimate the relationships specified in the following Eq. 9.
where t = 1995, 1996, 1997; P mother, father; \( H_{\text{p,1994}} \) represents parental health measured in 1994; \( S_{\text{i,1994}} \) denotes an adult child’s years of schooling in 1994; and \( B_{ 1994} \) contains baseline characteristics such as the adult child’s age, health, marital status, region measured and status of coresident with parents in 1994.
Estimate results are presented in Appendix Table 6 and suggest that a daughter with a father needing help for daily activity in 1994 is less likely to work in the labor market during 1995–1997. Among daughters, for example, the predicted probability of working decreases from 73% to 53% in 1997 if they had a father with functional limitations for daily activity in 1994. A mother’s having functional limitation in 1994 is also associated with a daughter’s lower probability of subsequent working status but only significantly in 1996.

Monthly labor income (in rubles) by gender and education. Data: Russia Longitudinal Monitoring Survey. Note: The monthly labor income is divided by 1,000 for 1994. Sample is restricted to children aged 13–29 in 1994 (i) whose mothers were aged 35–55 in 1994, (ii) who lived with both parents in 1994 and (iii) who remained in the same dwelling unit between 1994 and 2004. Higher education is defined as: years of schooling ≥13 for parents and years of schooling ≥15 for children

Monthly labor income (for the earning variable, RLMS questions ‘How much money in the last 30 days did you receive from your primary place of work after taxes?’) by gender and age. Data: Russia Longitudinal Monitoring Survey. Note: The monthly labor income is divided by 1,000 for 1994
Appendix 2: Sensitivity Analysis
Due to the RLMS restriction of dwelling-unit-based longitudinal design rather than individual-based, I cannot explicitly explore working status of adult children who have moved out from the initial dwelling units. Such a restriction of sample design reduces the sample size substantially for analysis of long-term association between parental health and children’s working status.
For example, the significant relationship between father’s health and adult daughter’s working status might have been driven by those who stayed in the same dwelling unit as the baseline year. To discuss this selection issue, I specify selection equation and working equation as follows: Sample Selection:
Y = 1 if staying in the same household in 2004; 0 otherwise. Working Status:
M = 1 if working; 0 otherwise.And
Potential sample selection may be corrected with a valid exclusion restriction. Due to the absence of such an excluded variable, it might not be plausible to achieve a valid correction of selection bias. Instead, I adopt a sensitivity analysis by restricting the correlation between error terms in a selection equation and working equation (Altonji et al. 2005).
Important questions regarding sample selection in this paper are (i) whether/how parents’ health status relates to sample selection and (ii) whether unobserved terms (\( \varepsilon_{Y} ,\varepsilon_{M} \)) in two equations relate significantly to each other. Here I denote the correlation between residuals as ρ Y,M. If children tend to move out for jobs regardless of parents’ health, sample attrition would not harm consistency in the coefficient of a parent’s health in the working equation. However, if children tend to leave the household to find jobs due to parents’ poor health (ρ Y,M < 0), ignoring sample selection can lead to underestimation of the coefficient of parental health in the working equation (i.e., overstate the magnitude of adverse parental health impact).
There are 813 daughters for the selection equation and 180 for the working equation. I estimate coefficients of parents’ health in both selection equation and working equation simultaneously, by varying correlations of residuals from −0.75 to 0.75. As summarized in Appendix Table 7, estimates for father’s health impact on selection are insignificant for all ranges of correlation. Estimate results for the daughter’s working status show significant, negative coefficients in father’s poor health indicator in most correlation ranges (−0.5 and higher). This suggests that the relationship between a father’s poor health and an adult daughter’s working status is significant, unless most daughters who left households are working in the market.
Rights and permissions
About this article
Cite this article
Choi, H. Parents’ Health and Adult Children’s Subsequent Working Status: A Perspective of Intergenerational Transfer and Time Allocation. J Fam Econ Iss 32, 493–507 (2011). https://doi.org/10.1007/s10834-010-9240-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10834-010-9240-1