
Abstract
Objectives
Worldwide, depression is one of the most common medical disorders in adolescence. Adolescent depressive symptoms generally increase over time, but many experience decreases after an initial peak. The purpose of this paper was to examine ecological predictors of baseline and change in adolescent depressive symptoms using Maslow’s Hierarchy of Needs as a framework.
Methods
Adolescents (n = 500; 52% female; baseline age 10–13 years) and their parents living in the northwestern United States completed annual questionnaires over six years. A structural equation model growth curve analysis was conducted to examine how family stressors, neighborhood safety, parent-child connectedness, and youth locus of control predicted adolescent depressive symptoms (baseline and growth).
Results
Results demonstrated that adolescent locus of control was associated with lower baseline depressive symptoms (β = −0.27, p < 0.001). Parent-child connectedness (youth-report) was indirectly predictive of baseline depressive symptoms through locus of control (β = −0.06, p < 0.05). Family economic stress was predictive of less growth in depressive symptoms over time (β = −0.20, p < 0.05). General family stressors, neighborhood safety, and parent report of parent-child connectedness were not predictive of adolescent depressive symptoms. In a sensitivity analysis using an autoregressive model, adolescent-report of parent-child connectedness was the most consistently predictive measure of adolescent depressive symptoms.
Conclusions
Overall, the results suggest that feelings of family connectedness and control are more important to understanding baseline depressive symptoms than physical, contextual factors. However, some adversity may be healthy and provide adolescents with experiences that slow the growth of depression.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
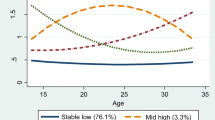
Worldwide, depression is among the top four medical disorders that cause disability in 10–19 year olds (Saluja et al. 2004). In 2016, about 3 million US adolescents experienced one or more major depressive episodes (National Institute of Mental Health 2017). Moreover, suicide rates, which are often associated with depression, have increased over 70% from 2006 to 2016 among adolescents 10–17 years (O’Donnell and Saker 2018). Adolescent depression is associated with academic issues, behavior problems, difficulty sleeping, weight fluctuations, inability to care for one’s self, self-harm, and suicide in adolescence and adulthood (Auerback 2015). Depressive symptoms during adolescence generally increase linearly over time (Kouros and Garber 2014). However, multiple studies have noted that trajectories for adolescent depression typically can be categorized into three to four classes, and many adolescents who initially display moderately high depressive symptoms find that their depressive symptoms decrease over time (Ellis et al. 2017; Mezulis et al. 2014). Approximately half of adults diagnosed with a mental illness begin to experience symptoms by age 14 (Kessler et al. 2005). Consequently, there is considerable value in understanding the predictors of depression and changes in depressive symptoms during adolescence so as to be able to better address depression over the lifecycle.
Ecological frameworks are valuable for understanding the development and growth of depressive symptoms because they model the intersection between individuals, families, and communities. Maslow’s Hierarchy of Needs (Maslow et al. 1970) uses an ecological approach to examining the needs of individuals, by highlighting multiple individual (i.e. esteem and locus of control), family (i.e. family SES, family stressors, and connection between family members), and community (i.e. safe environments) characteristics and how they build on and overlap with each other. This theory postulates that basic needs (food, shelter, clothing etc.), physical and emotional safety, love and belonging, and esteem must be met first in order for individuals to reach self-actualization and transcendence. Failure to meet each need may place an individual at higher risk for depression or increase the rate of growth of depressive symptoms. Alternatively, it may be said that depression hinders the growth of self-actualization, which includes self-regard and self-acceptance; using these concepts, prior research has found a negative relationship between self-actualization and depression in adolescents (Berndt et al. 1982).
Although Maslow’s Hierarchy of Needs is visualized as a pyramid, there is substantial overlap between need levels. Recent models demonstrate that basic needs, safety needs, and love and belonging needs overlap with one another and form lower order needs; these lower order needs must be at least minimally met in order to satisfy the higher order self-esteem needs (Decker and Cangemi 2018). Basic needs include the elements necessary to keep a person alive such as food, shelter and clothing. Safety needs involve protection, living without fear, and having a sense of boundaries and limits. Love and belongingness allow an individual to feel connected to others through offering love and receiving love from others. Meeting esteem needs leads to feelings of capability and internal control (Maslow et al. 1970).
The challenges associated with not meeting lower and higher level needs may lead to increased rates of adolescent depression or increased symptoms of depression over time. Conversely, depression and mental health may be less of a concern for individuals if their lower order needs are not yet met because their energy and resources may first be focused on meeting these more urgent needs. Furthermore, it would be important to examine both direct and indirect relationships as lower order needs (e.g., basic needs, safety, and love/belonging) might work through higher order needs to affect depression. For example, if safety needs of an adolescent are not met, it may make it more challenging to achieve feelings of self-esteem and confidence. Unmet safety needs could independently affect depressive symptoms, or these unmet needs could indirectly lead to increased depressive symptoms through other lower order unmet needs such as lack of belonging or through higher order esteem needs.
Previous research has demonstrated a connection between Maslow’s constructs and adolescent depression. Generally, research has observed that a met need is associated with less adolescent depression and unmet needs are associated with increased depression through both direct and indirect pathways.
Basic needs have a direct and indirect impact on adolescent depression. For example, higher perceived socioeconomic status, a measure of basic needs, has been associated with lower rates of depression (McLaughlin et al. 2012). Conversely, longitudinal studies have observed that ongoing family financial stress, in the absence of mediating parenting techniques, is associated with higher rates of depression (Lee et al. 2013). Family financial stress has also been shown to impair parent-child interactions (i.e. love and belonging needs), leading to increased adolescent depression (Wadsworth et al. 2013).
A lack of emotional and physical safety have both been linked with adolescent depression. For example, increased family conflict (i.e. less emotional safety) is associated with increased depression both directly (Lambert et al. 2014) and indirectly through parent-child attachment (i.e. love and belonging needs) (Constantine 2006). Poor neighborhood physical safety has been associated with greater adolescent depression (Butler et al. 2012), and when parents perceive more neighborhood social isolation and physical disorder this also increases adolescent depression (Ford and Rechel 2012). In a longitudinal study, higher negative safety was predictive of lower adolescent depression via self-efficacy (i.e. esteem needs) (Dupéré et al. 2012).
A large volume of literature has examined love and belonging needs, particularly as it relates to belonging within the family, with adolescent health needs (Carr and Springer 2010). For example, parent and family connection (i.e., love and belonging), which includes parental monitoring, family communication, family meal times, and stronger familial relationships, has generally been associated with lower rates of depression (Utter et al. 2017; Utter et al. 2013). Conversely, adolescents who do not live with their parents experience higher rates of stress and lower self-esteem (Corcoran and Franklin 2002). Although childhood trauma such as sexual abuse has been associated with greater depression, this can be mitigated by adolescents receiving support from their family (Guerra et al. 2018). In Guatemala, a study found that peer connectedness was associated with fewer emotional challenges, but there was no association found between parent-child connection and emotional challenges (Oldfield et al. 2018). In one of few studies to examine adolescent depression trajectories, Kouros and Garber (2014) found that worse family relationship quality, as measured by cohesion, expression, and conflict, predicted steeper linear increases in depressive symptoms from the sixth to twelfth grade.
Internal locus of control (LoC), one measure of esteem needs, is correlated with lower rates of depression in adolescents (Gordon et al. 2012; Powell et al. 1995), improved coping in the event of depression (Guerra et al. 2018), and functions to mediate the effect of early childhood adversity on later depression (Culpin et al. 2015). Conversely, an external locus of control has been associated with adolescent depression (Sullivan et al. 2017).
The extant research demonstrates that individual components of Maslow’s Hierarchy of Needs are associated with adolescent depression. However, the majority of research has been cross-sectional and includes only one or two components from the Maslow Hierarchy of Needs. Having a single model with all Maslow need levels included is important to understanding how each need level relates to other need levels in the context of depressive symptoms. Such a model would provide information on direct and indirect pathways to adolescent depression baseline rates and growth over time and also aid in identifying some of the root factors that increase risk for depression or exacerbate depressive symptoms over time.
Building off of the extant literature, the aim of this study was to explore how Maslow’s Hierarchy of Needs as a whole may be useful for predicting the development and growth of adolescent depressive symptoms from middle-to-late adolescence. We hypothesized that (1) lower-level needs including basic needs, family stress, and neighborhood safety would affect baseline levels and changes in depressive symptoms indirectly through higher order needs; (2) family connection would have an inverse relationship with adolescent depressive symptoms both directly and indirectly through adolescent LoC; and (3) LoC would be inversely associated with baselined depressive symptoms and growth in depressive symptoms.
Methods
Participants
Data came from the Flourishing Families Project, a 10-year longitudinal study with annual follow-ups that was initiated in 2007. The study took place in a large northwestern city in the United States. The sample for the current study included 500 adolescents and their parents who participated in the first six waves of Flourishing Families. Retention was greater than 90% in all waves of the study, and those who did not participate in one wave often returned in a subsequent wave.
Procedures
Census tracts that were representative of local school districts based on socioeconomics and race were carefully chosen, and families living in those census tracts were randomly selected using Polk Directories/InfoUSA, a national survey database with household information. The initial sample (n = 423) underrepresented lower SES and minority families; consequently, in order to increase the socioeconomic and racial diversity of the sample, an additional 77 families were recruited through referrals and fliers. In the first five waves of the project, surveys were conducted in the home. As adolescents began to transition out of their parent’s home in wave 6, the survey was then administered online. The survey responses of the adolescent and the primary responding parent, usually the mother, were included in this study. The procedures of the Flourishing Families Project have been described in more detail previously (Crandall et al. 2017). The study was approved by the university’s Institutional Review Board.
Measures
Adolescent self-report of depressive symptoms was measured in waves 3–6 using The Center for Epidemiological Studies Depression Scale for Children (CES-DC) (Weissman et al. 1980). The CES-DC is a 20-item scale in which items are ranked on a 4-point Likert scale ranging from not at all to a lot. Higher scores indicate greater depressive symptoms. Cronbach’s alpha in wave 3 was 0.91, which is similar to other samples (α = 0.91 for females and 0.87 for males) (Olsson and Von Knotting 1997).
Maslow’s hierarchy of needs constructs
To conceptualize Maslow’s Hierarchy of Needs, we included family stress, neighborhood safety, family connection, and locus of control (LoC). Given the overlap of lower-order needs, we modeled basic needs, safety, and love and belonging (measured by family connection) all at time one. However, given the preponderance of data on the salience of love and belonging to depression and that stress and safety may affect feelings of connection (Carr and Springer 2010; Guerra et al. 2018), we also modeled family connection at wave 2. As LoC, a measure of esteem needs, is a higher order need, we modeled it in wave 3.
Family stress (wave 1) was measured using 9 items from the chronic stress scale that assessed role-, health-, and economic-related stressors (Umberson et al. 2005). Parents responded to questions using a 6-point Likert scale, with higher scores indicating greater stress. Factor analysis revealed two constructs: four items measuring family chronic stress included stressors relating to health of self or others, parenting, and work concerns (e.g., “feeling stressed by work” or “health problems or concerns”; α = 0.67); five items measuring family economic stress included items relating to difficulty making ends meet or paying bills (e.g., “not enough money for housing” or “not enough money for healthcare”; α = 0.85). Prior studies demonstrated strong reliability: family stress scale α = 0.66–0.68 and family economic stress α = 0.73 to 0.80 (Umberson et al. 2005).
Neighborhood safety (wave 1) was assessed using 6-items regarding parent’s perception of children’s physical and social safety in their neighborhood or community from the National Survey of Children’s Health (Centers for Disease Control and Prevention 2003). Responses were on 4-point Likert scale, with higher scores indicating greater agreement. Sample items included “We watch out for each other’s children in this neighborhood” and “My child is safe in this community or neighborhood.” Higher scores indicated greater feelings of safety. Cronbach’s alpha in the current sample was 0.80.
To assess family connection (wave 1), adolescents reported on how connected they felt to their parents using 6 items that were adapted from a general social connectedness measure (Lee et al. 2001). Agreement was measured on a five-point Likert scale. Sample items included “Even though I am very close to my parent, I feel I can be myself” and “I feel so comfortable with my parent that I can tell him/her anything.” Reliability for this scale in the current sample was adequate (α = 0.70). In wave 2, the primary responding parent reported how connected they felt to their child using 9 items (6-point Likert scale) that were also adapted from a general social connectedness measure (Lee et al. 2001). Sample items included “I feel close to my child” and “I see my child as friendly and approachable.” Cronbach’s alpha for the current sample was 0.78. For both parent and adolescent-report, higher scores indicated higher family connection. Correlation between youth-report in wave 1 and parent report in wave 2 was 0.25.
Adolescent locus of control (wave 3) was measured using adolescent self-report of four items from the internal subscale of the Levenson Locus-of-Control Scale (Furnham and Steele 1993). Sample items, measured on a 5-point Likert scale (ranging from strongly disagree to strongly agree), included “What happens to me is my own doing” and “When I get what I want, it’s usually because I worked hard for it.” Higher scores indicated greater internal locus of control. Cronbach’s alpha on the subscale was 0.61. Similarly, other studies have demonstrated an alpha of 0.67 (Blau 1984).
Covariates
Since the majority of the sample was randomly selected but a minority of participants were recruited using convenience sampling techniques, we included sampling as a control in our models (0 = referrals/flyers, 1 = Polk Directories). We also included a variety of sociodemographic controls thought to influence adolescent depression including adolescent age, gender (0 = male, 1 = female), parent marital status (0 = not married, 1 = married), parent education (0 = less than a Bachelor’s degree, 1 = Bachelor’s degree or higher), and parent depressive symptoms (average score using 11 items from The Center for Epidemiological Studies Depression Scale) (Radloff 1977).
Data Analysis
Descriptive statistics were calculated using Stata 14 (StataCorporation 2015). The measurement model was set up by conducting separate confirmatory factor analysis (CFA) on all constructs using a structural equation modeling framework in Mplus Version 7 (Muthén and Muthén 1998–2017). Since data were categorical, the robust weighted least squares maximum likelihood estimator was used. Model fit was assessed using the following fit indices: Comparative Fit Index (CFI) > 0.90 indicated adequate fit and above 0.95 indicated strong fit; Root Mean Square Error of Approximation (RMSEA) < 0.10 indicated adequate fit and below 0.05 indicated strong fit (Little 2013). Items with factor loadings less than 0.40 were dropped.
Change in adolescent depression was examined over time by fitting a longitudinal growth curve model with the four waves of adolescent depression and no covariates (Duncan et al. 2006). After confirming that there was a significant change in depression over time and determining the type of growth (e.g., linear growth, quadratic growth), we regressed the adolescent depression intercept and slope on all of the Maslow constructs. We regressed adolescent internal LoC (wave 3) on all wave 1 and 2 Maslow constructs, and we regressed parent-report of feeling connected to their child (wave 2) on all wave 1 Maslow constructs. Finally, we added the control variables to the model by regressing adolescent depression intercept, slope, and all Maslow constructs on the controls. We tested for mediation by examining the significance of indirect effects using 5000 bootstraps (Preacher and Hayes 2008). The same model fit indices and cut-offs used for conducting the CFA were applied in the growth curve models. Full information maximum likelihood (FIML) was used to account for missing data.
Results
Of the 500 adolescents, 51.6% were female, 67.2% of their parents were married in wave 1, 59.6% of their parents had a bachelor’s degree or higher, and 65.4% of families were of European-American ethnicity. Adolescents were 10–13 years old during wave 1 (15–18 years in wave 6).
In the CFA, model fit was above the minimum cutoffs for all covariates, and latent variables were created for each covariate. Factor loadings ranged from 0.46 to 0.92 for adolescent depressive symptoms in waves 3–6, from 0.47 to 0.66 for internal locus of control, from 0.68 to 0.95 for parent report of connectedness with their adolescent child, from 0.48 to 0.67 for child report of feeling connected to their parents, from 0.55 to 0.93 for neighborhood safety, from 0.52 to 0.68 for family chronic stressors, and from 0.74 to 0.93 for family economic stress. Table 1 includes a correlation matrix for all study variables.
To examine change in adolescent depressive symptoms, we first verified that the construct was invariant over time. We tested for configural, weak, and strict invariance to assess whether the factor loadings and error variances were equivalent across all four waves of data. Cheung and Rensvold recommended examining changes in the CFI between models as a way to test for measurement invariance (Cheung and Rensvold 2002). If the CFI changes by more than 0.01 between models, it would be an indication of measurement non-equivalence. We found that the CFI changed by less than 0.01 between configural, strong, and strict models of adolescent depressive symptoms. Thus, it was appropriate to examine mean differences in the construct over time and a growth curve could be fit to adolescent depression.
We fit a growth curve model with no covariates to assess changes in depressive symptoms. Adolescents experienced an increase in depressive symptoms between waves 3–6, with a mean slope of 0.10 (p < 0.001). A linear slope was found to be the best fit. There was also evidence that adolescents varied in their rate of growth in depressive symptoms (p < 0.001).
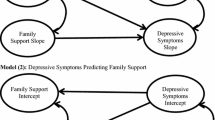
In the final model (Table 2) with all covariates and controls, only adolescent internal LoC was predictive of the adolescent depression intercept, with higher LoC associated with a lower intercept. Family economic stress was predictive of a lower rate of growth in adolescent depressive symptoms; no other covariates were predictive of the slope.
Family stress was associated with lower rates of parent-report of connectedness with their child. Neighborhood safety and child-report of connectedness with their parents were both associated with higher parent-report of connectedness with their child. Neighborhood safety was predictive of lower adolescent internal LoC while child and parent report of connectedness were both predictive of higher adolescent internal LoC. Family economic and chronic stressors did not predict LoC.
In mediation models (Table 3), adolescent LoC mediated the relationship between child-report of their connectedness with their parents and the adolescent depression intercept (β = −0.06, z = 2.05, p = 0.04). There were no other significant indirect pathways.
Based on the results of the final growth curve model, we considered that the results may have been affected by regression toward the mean for adolescent depressive symptoms. We conducted a sensitivity analysis by fitting adolescent depressive symptoms in an autoregressive model (Table 4). Consistent with the results of the growth curve model, adolescent LoC was associated with wave 3 adolescent depressive symptoms, and family economic stress was associated with lower rates of adolescent depression in waves 4 and 5. Unlike the growth curve model, we also found some evidence of a relationship between family chronic stressors and child-report of connectedness with their parents with later adolescent depressive symptoms. Family stress was predictive of more depressive symptoms in wave 4 and marginally associated with more depressive symptoms in wave 5. Adolescent connectedness with their parents was predictive of adolescent depressive symptoms in wave 3, 4, and 5.
Discussion
The purpose of the study was to explore whether Maslow’s Hierarchy of Needs was a useful framework for predicting adolescent depression and growth in depression from middle-to-late adolescence using six years of longitudinal data. Results indicated that Maslow’s Hierarchy of Needs partially predicts and explains baseline and changes in adolescent depressive symptoms. Supporting the hypotheses, higher internal LoC and higher child reported parent-child connection were associated with lower levels of depressive symptoms. Contrary to what was expected, higher family economic stress predicted less growth in adolescent depressive symptoms.
Consistent with our hypothesis, a direct association between internal locus of control and lower baseline depressive symptoms was observed. Further, internal locus of control mediated the relationship between children’s report of their connectedness to their parents and levels of depression. However, neighborhood safety, family stress and economic stress were not directly nor indirectly predictive of the depression intercept. These findings suggest that family factors relating to an adolescent’s feelings of belonging and capability may be more important than structural aspects of the family life such as SES and neighborhood safety. Contrary to previous results (Dupéré et al. 2012), neighborhood safety was negatively associated with internal LoC. One possible explanation is that unsafe neighborhoods may be associated with higher internal LoC as adolescents fulfill more responsibilities and problem solve on their own, thus having more opportunities earlier in life to develop LoC compared to their peers from more affluent neighborhoods (Starnes and Zinser 1983). This finding is also consistent with the challenge model of resiliency theory that posit that modest risks, e.g., less safe neighborhood environments, may actually help adolescents overcome later risks that could have contributed to negative outcomes such as depression because prior challenges enabled them to learn positive coping and problem solving skills and also provided confidence that they have previously successfully coped with a challenge and can do so again (Rutter 1987; Zimmerman 2013).
Child-parent connection was positively associated with internal LoC and indirectly related to baseline depressive symptoms. Positive family relationships may allow adolescents to feel more comfortable seeking advice from their parents which can help the adolescent overcome his/her challenges and feel that the solution is in his/her control. Additionally, when adolescents have high levels of connection with their family members and when those family members have a high internal LoC, then those adolescents may model their behavior/beliefs after those family members and increase their own internal LoC (Powell et al. 1995).
Contrary to the results of Kouros and Garber (2014), the current study revealed no relationship between child-parent connection and the adolescent depression slope. When analyzing the results as an autoregressive model, however, child reported connection to their parents was the most salient construct in predicting change in depressive symptoms. The results are complex, but parent-child connection seemed to be protective against adolescent depression in most of the waves of data. These results suggest that despite a family’s environmental circumstances, such as neighborhood safety or SES, the connection existing between family members can protect adolescents from growth in depressive symptoms.
In the main model, family economic stress was the only predictor of the adolescent depression slope. Contrary to our hypothesis, adolescents in families with higher levels of economic stress experienced less growth in their depressive symptoms over time. One possible explanation for this result is that adolescents whose basic needs are not being met may not be in tune with their own emotional well-being, including depressive symptoms. According to Maslow’s Hierarchy of Needs, each time a set of needs is gratified, a new need emerges (Maslow 1954). Therefore, if basic needs are not being met, emotional needs which are represented further up in the hierarchy are not a priority to consider. For adolescents living in low SES families, basic needs such as money, shelter, and food are likely the most dominant set of needs. Therefore, emotional needs related to depression may be less often considered as these families and adolescents work to meet their basic needs. This may help explain why adolescents in families with higher economic stress experienced less growth in their depressive symptoms over time.
Another possible explanation for this relationship may be that adolescents living in more stressful economic circumstances may be more likely to have employment than their more financially-secure peers. Adolescents’ employment may give them a greater sense of purpose and experience, which could be protective against growth in depressive symptoms (Rutter 1987). Among African American youth, employment was a protective factor against depression in the presence of poor neighborhood conditions, possibly because of the sense of belonging and purpose it provided in their lives (Scott et al. 2015).
A final possible explanation for this inverse relationship may be explained by statistical regression toward the mean. Adolescents who reported higher baseline depressive symptoms had less room for an increase in depressive symptoms based on the scale used compared to their peers reporting lower levels of depressive symptoms at baseline. The inverse correlation between the depression intercept and slope is evidence of this. However, even when controlling for baseline depressive symptoms, there was still an inverse relationship between family financial stress and depressive symptoms in waves 4 and 5 (marginally non-significant), suggesting that regression toward the mean is not likely the only explanation for the inverse relationship between family financial stress and the depression slope. However, regression toward the mean may explain why other study variables, such as child-parent connection, were not predictive of the depression slope.
Limitations and Future Research
A limitation of the study was that not all independent variables were measured at each wave of the study. As a result, we were limited to examining independent variables in the wave that they were available. For example, basic needs, safety, and child-report of connection needs were all measured in wave 1, parent-report of connection was available in wave 2, and locus of control was available in wave 3. Generally this fit with Maslow’s Hierarchy of Needs that posits that basic needs, safety, and love and belonging are intersecting, lower-order needs that contribute to higher order self-efficacy. A second limitation was that data regarding depressive symptoms was collected via self-reported data. Because information was self-reported, some participants may have reported high depression scores in wave 3 but even if depression worsened in later waves, they could not indicate worse depressive symptoms if they had already reported the highest score in a prior wave. It is also important to note that not all aspects of each level of need (based on Maslow’s Hierarchy of Needs) were measured in this study. For example, the love and belonging need was measured by parent-child connection because families are so salient to individual health throughout the life course (Carr and Springer 2010), but other measures of belonging were not included such as peer attachment although this may also be important to adolescent depressive symptoms (Oldfield et al. 2018). We selected variables based on Maslow’s Hierarchy of Needs that were available in the Flourishing Families Project data set and that had research support indicating a relationship with depression.
A primary strength of this study was the collection of depressive symptoms at multiple time points, allowing for the study of baseline adolescent depression as well as growth in depression. Furthermore, the Maslow constructs included both adolescent and parent reporters. Finally, structural equation model (SEM) methodology was also a strength of this study. SEM addresses measurement error, allows for the testing of multiple relationships simultaneously and tests for mediation. This allowed us to test direct and indirect pathways between independent and outcome variables.
References
Auerback, R. (2015). Depression in adolescents: causes, correlates and consequences. Psychological Science Agenda. Retrieved from https://www.apa.org/science/about/psa/2015/11/depression-adolescents.
Berndt, D. J., Kaiser, C. F., & Van Aalst, F. (1982). Depression and self‐actualization in gifted adolescents. Journal of Clinical Psychology, 38, 142–150.
Blau, G. J. (1984). Brief note comparing the Rotter and Levenson measures of locus of control. Perceptual and Motor Skills, 58, 173–174.
Butler, A. M., Kowalkowski, M., Jones, H. A., & Raphael, J. L. (2012). The relationship of reported neighborhood conditions with child mental health. Academic Pediatrics, 12, 523–531.
Carr, D., & Springer, K. W. (2010). Advances in families and health research in the 21st century. Journal of Marriage and Family, 72, 743–761.
Centers for Disease Control and Prevention. (2003). National survey of children’s health (OMB Control No. 0920–0406). Atlanta, GA: Author.
Cheung, G. W., & Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9, 233–255.
Constantine, M. G. (2006). Perceived family conflict, parental attachment, and depression in African American female adolescents. Cultural Diversity and Ethnic Minority Psychology, 12, 697–709.
Corcoran, J., & Franklin, C. (2002). Multi-systemic risk factors predicting depression, self-esteem, and stress in low SES and culturally diverse adolescents. Journal of Human Behavior in the Social Environment, 5, 61–76.
Crandall, A., Magnusson, B. M., Novilla, M. L. B., Novilla, L. K. B., & Dyer, W. J. (2017). Family financial stress and adolescent sexual risk-taking: the role of self-regulation. Journal of Youth and Adolescence, 46, 45–62.
Culpin, I., Stapinski, L., Miles, Ö. B., Araya, R., & Joinson, C. (2015). Exposure to socioeconomic adversity in early life and risk of depression at 18 years: the mediating role of locus of control. Journal of Affective Disorders, 183, 269–278.
Decker, P. J., & Cangemi, J. P. (2018). Emotionally intelligent leaders and self-actualizing behaviors: any relationship? IFE PsychologIA: an International Journal, 26, 27–30.
Duncan, T. E., Duncan, S. C., & Strycker, L. A. (2006). An introduction to latent variable growth curve modeling: concepts, issues, and application. New York, NY: Psychology Press.
Dupéré, V., Leventhal, T., & Vitaro, F. (2012). Neighborhood processes, self-efficacy, and adolescent mental health. Journal of Health and Social Behavior, 53, 183–198.
Ellis, R. E., Seal, M. L., Simmons, J. G., Whittle, S., Schwartz, O. S., Byrne, M. L., & Allen, N. B. (2017). Longitudinal trajectories of depression symptoms in adolescence: psychosocial risk factors and outcomes. Child Psychiatry & Human Development, 48, 554–571.
Ford, J. L., & Rechel, M. (2012). Parental perceptions of the neighborhood context and adolescent depression. Public Health Nursing, 29, 390–402.
Furnham, A., & Steele, H. (1993). Measuring locus of control: A critique of general, children’s health- and work-related locus of control questionnaires. British Journal of Psychology, 84, 443–479.
Gordon, M. S., Tonge, B., & Melvin, G. A. (2012). The self-efficacy questionnaire for depressed adolescents: a measure to predict the course of depression in depressed youth. Australian & New Zealand Journal of Psychiatry, 46, 47–54.
Guerra, C., Farkas, C., & Moncada, L. (2018). Depression, anxiety and PTSD in sexually abused adolescents: association with self-efficacy, coping and family support. Child Abuse & Neglect, 76, 310–320.
Kessler, R. C., Chiu, W. T., Demler, O., & Walters, E. E. (2005). Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62, 617–627.
Kouros, C. D., & Garber, J. (2014). Trajectories of individual depressive symptoms in adolescents: gender and family relationships as predictors. Developmental Psychology, 50, 2633.
Lambert, M., Fleming, T., Ameratunga, S., Robinson, E., Crengle, S., Sheridan, J., & Merry, S. (2014). Looking on the bright side: an assessment of factors associated with adolescents’ happiness. Advances in Mental Health, 12, 101–109.
Lee, R. M., Draper, M., & Lee, S. (2001). Social connectedness, dysfunctional interpersonal behaviors, and psychological distress: testing a mediator model. Journal of Counseling Psychology, 48, 310–318.
Lee, T. K., Wickrama, K. A. S., & Simons, L. G. (2013). Chronic family economic hardship, family processes and progression of mental and physical health symptoms in adolescence. Journal of Youth and Adolescence, 42, 821–836.
Little, T. D. (2013). Longitudinal structural equation modeling. New York, NY: Guilford press.
Maslow, A. H. (1954). The instinctoid nature of basic needs. Journal of Personality, 22, 326–347.
Maslow, A. H., Frager, R., Fadiman, J., McReynolds, C., & Cox, R. (1970). Motivation and personality (Vol. 2). https://doi.org/10.1037/h0038815.
McLaughlin, K. A., Costello, E. J., Leblanc, W., Sampson, N. A., & Kessler, R. C. (2012). Socioeconomic status and adolescent mental disorders. American Journal of Public Health, 102, 1742–1750.
Mezulis, A., Salk, R. H., Hyde, J. S., Priess-Groben, H. A., & Simonson, J. L. (2014). Affective, biological, and cognitive predictors of depressive symptom trajectories in adolescence. Journal of Abnormal Child Psychology, 42, 539–550.
Muthén, L. K., & Muthén, B. O. (1998–2017). Mplus User’s Guide (8th Ed.). Los Angeles, CA: Muthén & Muthén.
National Institute of Mental Health. (2017). Major depression: Statistics. Retrieved from https://www.nimh.nih.gov/health/statistics/major-depression.shtml.
O’Donnell, J., & Saker, A. (2018, March 19). Teen suicide is soaring. Do spotty mental health and addiction treatment share blame? USA Today. Retrieved from https://www.usatoday.com/story/news/politics/2018/03/19/teen-suicide-soaring-do-spotty-mental-health-and-addiction-treatment-share-blame/428148002/.
Oldfield, J., Stevenson, A., Ortiz, E., & Haley, B. (2018). Promoting or suppressing resilience to mental health outcomes in at risk young people: the role of parental and peer attachment and school connectedness. Journal of Adolescence, 64, 13–22.
Olsson, G., & Von Knotting, A. L. (1997). Depression among Swedish adolescents measured by the self rating scale Center for Epidemiology Studies-Depression Child (CES-DC). European Child & Adolescent Psychiatry, 6, 81–87.
Powell, J. W., Denton, R., & Mattsson, Å. (1995). Adolescent depression: Effects of mutuality in the mother-adolescent dyad and locus of control. American Journal of Orthopsychiatry, 65, 263.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40, 879–891.
Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied psychological Measurement, 1(3), 385–401.
Rutter, M. (1987). Psychosocial resilience and protective mechanisms. American Journal of Orthopsychiatry, 57, 316–331.
Saluja, G., Iachan, R., Scheidt, P. C., Overpeck, M. D., Sun, W., & Giedd, J. N. (2004). Prevalence of and risk factors for depressive symptoms among young adolescents. Archives of Pediatrics & Adolescent Medicine, 158, 760–765.
Scott, S., Wallander, J., Cameron, L., Scott, S. M., & Wallander, J. L. (2015). Protective mechanisms for depression among racial/ethnic minority youth: empirical findings, issues, and recommendations. Clinical Child & Family Psychology Review, 18, 346–369.
Starnes, D. M., & Zinser, O. (1983). The effect of problem difficulty, locus of control, and sex on task persistence. The Journal of general psychology, 108, 249–255.
StataCorporation. (2015). Stata statistical software. Release 14. College Station, TX: StataCorp LP.
Sullivan, S. A., Thompson, A., Kounali, D., Lewis, G., & Zammit, S. (2017). The longitudinal association between external locus of control, social cognition and adolescent psychopathology. Social Psychiatry and Psychiatric Epidemiology, 52, 643–655.
Umberson, D., Williams, K., Powers, D. A., Liu, H., & Needham, B. (2005). Stress in childhood and adulthood: effects on marital quality over time. Journal of Marriage and Family, 67, 1332–1347.
Utter, J., Denny, S., Peiris-John, R., Moselen, E., Dyson, B., & Clark, T. (2017). Family meals and adolescent emotional well-being: findings from a national study. Journal of Nutrition Education and Behavior, 49, 67–72.e61.
Utter, J., Denny, S., Robinson, E., Fleming, T., Ameratunga, S., & Grant, S. (2013). Family meals and the well‐being of adolescents. Journal of Paediatrics and Child Health, 49, 906–911.
Wadsworth, M. E., Rindlaub, L., Hurwich-Reiss, E., Rienks, S., Bianco, H., & Markman, H. J. (2013). A longitudinal examination of the adaptation to poverty-related stress model: predicting child and adolescent adjustment over time. Journal of Clinical Child & Adolescent Psychology, 42, 713–725.
Weissman, M. M., Orvaschel, H., & Padian, N. (1980). Children’s symptom and social functioning self-report scales: Comparison of mothers’ and children’s reports. Journal of Nervous Mental Disorders, 168, 736–740.
Zimmerman, M. A. (2013). Resiliency theory: a strengths-based approach to research and practice for adolescent health. Thousand Oaks, CA: Sage.
Author Contributions
AC conceived of the study and the analytical design, performed statistical analyses and interpretation, drafted the methods and results sections, and edited the manuscript. EAP and GCB wrote sections of the introduction and discussion. BMM drafted sections of the introduction and helped edit the entire manuscript. CLG, MDB, and MLBN reviewed and edited the manuscript. RAB was a principal investigator for the Flourishing Families Project and helped edit the manuscript. All authors helped with the interpretation of results and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Crandall, A., Powell, E.A., Bradford, G.C. et al. Maslow’s Hierarchy of Needs as a Framework for Understanding Adolescent Depressive Symptoms Over Time. J Child Fam Stud 29, 273–281 (2020). https://doi.org/10.1007/s10826-019-01577-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-019-01577-4