
Abstract
Parents of children with developmental delays (DD) report higher levels of parenting stress compared to parents of typically developing children. High levels of parenting stress have been associated with negative outcomes for their children, including higher levels of emotion dysregulation. However, this relationship between parenting stress and child emotion dysregulation has rarely been examined in families of children with DD. Additionally, the mechanisms through which parenting stress influences child emotion dysregulation remain unclear; it may be that parenting stress impacts parenting behaviors (i.e., sensitive and intrusive parenting), which in turn influence the development of the child’s emotion regulatory abilities. In the current study, we employed a waitlist-control design to examine whether changes in parenting stress through Mindfulness-Based Stress Reduction (MBSR) predict changes in emotion dysregulation among children with DD, as well as examine parenting behaviors that may mediate the impact of parenting stress on child emotion dysregulation. Eighty parents of children with DD between the ages of 2½ and 5 (M = 4.18, SD = 1.01) were randomly assigned to an immediate treatment or waitlist-control group. Results indicated that reductions in parenting stress through MBSR significantly predicted reductions in child emotion dysregulation. Regarding mechanisms, only intrusive parenting was found to significantly mediate the relationship between parenting stress and child emotion dysregulation. These findings suggest that by intervening with parents of children with DD early on, there may be a spillover effect on their children, reducing the rates of emotion dysregulation that are common in this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Parents of children with developmental delays (DD) experience significantly higher levels of stress compared to parents of typically developing (TD) children (Baker et al. 2002). This is concerning, because parents of children with both DD and TD who are highly stressed tend to exhibit more intrusive parenting and less sensitivity to their children’s needs, which can negatively impact their children’s development (Anthony et al. 2005; Crnic et al. 2005). In particular, parenting behaviors that are more intrusive and less sensitive are highly predictive of greater child emotion dysregulation, which places these children at a higher risk for developing behavioral and social problems (Morris et al. 2007; NICHD Early Child Care Research Network 2004). Despite the findings that parents of children with DD consistently report higher levels of parenting stress, few studies have explored the relationship between parenting stress and child emotion dysregulation in this population.
High levels of parenting stress in parents of children with DD is concerning given the associated negative outcomes for both parents and their children. Research has indicated that highly stressed parents are particularly prone not only to compromised physical health (Eisenhower et al. 2009), but also to significantly poorer mental health and subsequent risk for psychopathology, including depression (Hastings et al. 2006) and anxiety (Firth and Dryer 2013). Moreover, parents who experience higher levels of stress typically report family problems, including marital conflict (Kersh et al. 2006), lower parental satisfaction and well-being, less parental competence and social support (Pisula 2007), as well as less effective parenting (Crnic et al. 2005). Their children are also at increased risk for elevated behavior problems (Baker et al. 2002; Hastings et al. 2006; Neece et al. 2012), later psychopathology (Baker et al. 2010), depression (Anthony et al. 2011), poor overall quality of life (Moreira et al. 2014), and increased child emotion dysregulation (Chazan-Cohen et al. 2009; Mathis and Bierman 2015).
Emotion regulation is commonly defined as the “extrinsic and intrinsic processes responsible for monitoring, evaluating, and modifying emotional reactions, to accomplish one’s goals” (Thompson 1994, pp. 27-28), with dysfunction in regulatory abilities commonly referred to as emotion dysregulation (Cole et al. 1994). Although researchers have shown that children with DD present significantly higher levels of emotion dysregulation compared to their typically developing peers (Baker et al. 2007), there is a shortage of studies examining the emergence and function of emotion regulatory abilities in children with DD (Crnic and Neece 2015; Mazefsky et al. 2012). This lack of attention is concerning, given the host of negative outcomes associated with poor regulatory abilities documented among typically developing children, including an increased risk of psychopathology (Cole et al. 1994), elevated behavior problems (Cole et al. 2004), social skills problems, worse physical health, and lower academic and work performance (Aldao et al. 2010). Considering that the development of emotion regulatory abilities depends heavily on a child’s cognitive executive functioning (Posne and Rothbart 2000), which is impaired in children with DD (Japundža-Milisavljevic and Macešic-Petrovic 2008), children with DD may be placed at an increased risk for these negative outcomes.
It is only in the past decade that researchers have begun to study emotion regulatory abilities in children with DD. For instance, Morris et al. (2007) reported that children with DD had more difficulties adapting to the demands of emotionally challenging events because of their limited cognitive capabilities, thus increasing their risk for behavior problems. Moreover, Gerstein et al. (2011) conducted a longitudinal study examining the extent to which children with DD employ emotion regulatory strategies across the preschool period, and found that children with DD used more maladaptive regulatory strategies over time when engaged in a mildly frustrating task. Emotion regulation is a key construct of interest among children with DD because research indicates that emotion regulation abilities may mediate the relationship between developmental status and child social skills and behavior problems (Baker et al. 2007; Gerstein et al. 2011). In study by Baker et al. (2007), global dysregulation at age four not only significantly predicted children’s social skills at age six, but it also partially mediated the relationship between children’s developmental risk and later social skills. These studies suggest that the elevated rates of behavior and social skills problems observed in children with DD may not simply be a byproduct of the developmental delay itself, but may instead reflect indirect effects that are at work through emergent emotion regulatory capabilities (Crnic and Neece 2015), highlighting the need to study the development of emotion regulation in children with DD.
Parenting stress has long been implicated as a salient player in the development of regulatory abilities among typically developing children (Anthony et al. 2005; Crnic et al. 2004). In a longitudinal study, Chazan-Cohen et al. (2009) reported that higher levels of parenting stress when children were 14 months old predicted higher levels of emotional dysregulation in children when they were five years old. These effects may also be bidirectional, such that elevated parenting stress may increase levels of child emotion dysregulation, which may subsequently exacerbate further the stress that parents experience. Williford et al. (2007), for example, found that parents who had children who were more dysregulated at age two also reported subsequent increases in parenting stress. However, to the authors’ knowledge, none of the studies in the literature examining the relationship between parenting stress and child emotion dysregulation have employed an experimental design. As a result, while causality has been assumed between parenting stress and child emotion dysregulation, the causal relationship has not yet been empirically tested.
Although associations between parenting stress and child emotion dysregulation have been found, the mechanisms through which parenting stress may impact child emotion dysregulation remain unclear. Indeed, researchers have proposed theoretical models in which parenting behaviors mediate the relationship between parenting stress and child outcomes; however, a dearth of empirical studies exist in the literature examining the full mediational model (Deater-Deckard 1998; Hastings 2002). Researchers have found that elevated levels of parenting stress can interfere with the parenting practices that help regulate children’s emotions. Crnic et al. (2005) reported that higher levels of parenting stress were predictive not only of lower levels of positive parenting (i.e., warmth, spontaneous smiles and laughter), but also of lower levels of dyadic pleasure in the parent-child interaction. Further, Pianta and Egeland (1990) demonstrated that parents who reported higher levels of stress were also more intrusive in their parenting. Similarly, Anthony et al. (2005) found that parents who were more stressed tended to have lower expectations of their children and demonstrated less nurturing parenting.
Regarding the relationship between parenting behavior and emerging emotion regulatory abilities, researchers have consistently found that warm and sensitive parenting promotes better emotion regulatory abilities in children (von Suchodoletz et al. 2011). Sensitive parents are nurturing and child-centered, and are thus more likely to respond to their child’s emotional cues in a way that promotes their child’s use of regulatory abilities (Morris et al. 2007). Besides sensitive parenting, researchers have also noted the association between intrusive parenting and greater levels of subsequent child emotion dysregulation (Egeland et al. 1993; NICHD Early Child Care Research Network 2004). Intrusive parents impose their agenda on the child despite signals from the child that a different pace is needed in the interaction, which may make them less likely to model and teach their children appropriate means of regulating their emotions during challenging situations (Morris et al. 2007). These findings suggest a promising mechanism by which parenting behavior mediates the relationship between parenting stress and child emotion dysregulation.
As noted, the relationship between parenting stress and emotion dysregulation among children with DD remains an understudied area. Thus, in the current study, we sought to contribute to the literature by employing an experimental design in order to determine whether a causal relationship exists between parenting stress and emotion dysregulation among children with DD. The current study took place in the context of a larger study in which parents of children with DD received Mindfulness-Based Stress Reduction (MBSR) training, allowing us to experimentally manipulate parenting stress and observe subsequent changes in child outcomes. We also examined sensitive and intrusive parenting behaviors as potential mediators of the relationship between parenting stress and emotion dysregulation. We hypothesized that reductions in parenting stress through MBSR would lead to reductions in emotion dysregulation among children with DD. Additionally, we hypothesized that sensitive and intrusive parenting behavior would mediate the relationship between parenting stress and emotion dysregulation among children with DD.
Method
Participants
In the current study, we used data from two cohorts of Mindful Awareness for Parenting Stress (MAPS) Project, the first one from 2012-2013, and the second one from 2014–2015. Eligibility criteria for the study included: (a) having a child ages 2.5 to 5 years, (b) child had been determined by the Inland Regional Center (or by an independent assessment) to have a developmental delay, (c) parent reported more than ten child behavior problems on the Eyberg Child Behavior Inventory (Robinson et al. 1980), (d) parent was not receiving any form of psychological or behavioral treatment at the time of the referral, and (e) parent spoke and understood English (for the first cohort only). In the second cohort, we also enrolled parents who were monolingual Spanish speakers.
Our sample included a total of 80 parent-child dyads; 41 were part of an immediate treatment group, and 39 were in a waitlist-control group. The majority of the children were boys (71.3%), and the mean age of the children was 4.18 years (SD = 1.01 years). We had a diverse sample, with parents reporting 47.5% of the children to be Latino, 25.0% Caucasian, 21.3% Other, 3.8% Asian, and 2.5% African American. Among the parents sampled, the majority were mothers (96.3%) and married (75.0%), and the mean age of the parents was 37.21 years (SD = 7.22 years). Parents’ family income ranged from $0 to $95,000, with 53.8% of parents reporting annual family income to be less than $50,000 and 46.3% reporting annual family income to be above $50,000. In terms of language, 17.5% of the parents were monolingual Spanish speakers. Demographic data are summarized in Table 1.
Regarding the child’s diagnosis, the majority of the children (63.6%) were reported to have a diagnosis on the autism spectrum. At baseline, 47.5% of the children were receiving in-home behavioral services, 88.2% of the children were reported to receive special education services in school, and 79.4% of the children were enrolled in a special education classroom. Although not formally assessed, the majority of children were estimated to have intellectual functioning in the mild to moderate range given the demands of the laboratory assessment. Children had to understand and follow directions in a structured play task in order to be eligible for the study.
Procedure
The current study took place in the context of a larger randomized control trial in which parents of children with DD received Mindfulness-Based Stress Reduction (Chan and Neece 2018; Neece 2014). MBSR is an empirically-supported stress-reduction intervention that has undergone over three decades of extensive research showing its effectiveness in reducing stress and anxiety, as well as promoting overall well-being in a variety of populations (Grossman et al. 2004). Data from a recent randomized controlled trial demonstrated that MBSR was effective in reducing parenting stress within the same sample of parents used in the current study (Chan and Neece 2018).
We recruited most of the participants through the Inland Regional Center, which is a government agency that provides services for individuals with developmental delays; additional recruitment was done through the local newspaper, local elementary schools, and community disability groups. Research staff first did a phone screening with all parents who had contacted the laboratory and expressed interest in participating in the study, in order to ensure that these families met the specified eligibility criteria. Eligible families were then scheduled for a baseline assessment, and received a packet of questionnaires in the mail prior to the baseline assessment.
At the baseline assessment, parents turned in the completed packet of questionnaires and participated in a 15-minute play assessment in the lab with their child, which was videotaped for later coding. The play assessment included three parts: (1) a five-minute child-led play, in which the parent was instructed to allow the child to choose any activity and to play along with the child; (2) a five-minute parent-led play, in which the parent was instructed to select an activity and to keep the child playing according to the parent’s rules; and (3) a five-minute clean-up activity, in which the parent was instructed to give the child a command to clean up. The play assessment was used as an observational measure of child emotion dysregulation and parenting behavior. After the observation task, parents were interviewed by research staff to gather demographic data, and were then randomly assigned to an immediate treatment or waitlist-control group.
The mindfulness-based stress reduction (MBSR) intervention followed the manual from the University of Massachusetts Medical Center (Kabat-Zinn 1990). Parents assigned to the immediate treatment group received the eight-week long intervention following the baseline assessment. The procedures for the MBSR intervention used in this study are detailed in a pilot study for the MAPS Project (Neece 2014). As part of the waitlist-control design, parents from both the immediate treatment and waitlist group returned for a second assessment, during which only the immediate treatment group had received MBSR, and completed the same questionnaire and observational measures collected at the baseline assessment. After the second assessment, parents in the waitlist group received MBSR and returned to the MAPS laboratory for a post-treatment assessment.
Video coding
Video recordings of each play assessment from baseline and post-treatment were randomized in order to ensure coder blindness to the assessment time points and parent group assignment. For each coding system, coding was done paper-and-pencil in the laboratory. Coders watched each video recording all the way through, and assigned a global code for the variables of interest (see Measures section for more details). During the training phase for each coding system, a senior graduate student who was an expert on the coding system served as the “master coder” for reliability monitoring. Two graduate students were trained using a consensus rating procedure in which their ratings were discussed in a group format with the master coder, until their independent ratings agreed with the master coder’s above the specified reliability criterion level. To establish and maintain the reliability of the observational coding systems, we used a minimum reliability criterion of an intra-class correlation (ICC) = 0.60, which has been widely recommended as a minimum level of inter-rater reliability for ordinal level data (Cicchetti 1994). Once the specified training reliability was achieved, the two coders coded in pairs, first coding independently and then coming to a consensus. Twenty percent of the pair’s consensus codes were compared against the codes of a master coder to monitor inter-rater reliability. Thirty-one videos from the second cohort included Spanish-speaking parent-child dyads. For these videos, a linguistically and culturally competent translator provided in-vivo translation for the coders.
Measures
Demographic data
Demographic information was collected during an interview with the parent during the baseline assessment.
Parenting stress
The Parenting Stress Index—Short Form (PSI-SF; Abidin 1990) is a standardized self-report questionnaire designed to measure the extent to which parents are experiencing stress. Parents rate 36 items on a five-point Likert scale that ranges from 1 (strongly agree) to 5 (strongly disagree). In this study, we used only the Parental Distress subscale, which measures the extent to which the parent is experiencing stress in his or her role as a parent. This subscale was chosen because it assesses parenting stress independent of child variables, including child emotion dysregulation, which was a key outcome variable of the current study. Some example items include: “I often have the feeling that I cannot handle things very well,” “Since having this child, I have been unable to do new and different things,” and “I feel trapped by my responsibility as a parent.” In the current study, internal consistency for the Parental Distress subscale was good, with Cronbach’s alphas of .84 and .87 for the baseline and second assessments, respectively. The PSI-SF also has a validity index that measures the extent to which the parents are answering in a way that they think will make them look best. A score of 10 or less on this index suggests responding in a defensive manner and indicates that caution should be used in interpreting any of the scores. Three participants had a defensive responding score of 10 or less at the post-treatment assessment; accordingly, these scores were removed from the analysis.
Emotion dysregulation
The Dysregulation Coding System (DCS; Hoffman et al. 2006) is an observational coding system that measures child emotion dysregulation by determining the appropriateness of the type, duration, and intensity of emotional expressions, as well as the lability and the extent to which the child can be soothed. Emotion dysregulation is coded on a five-point Likert scale from 0 (no evidence of dysregulation) to 4 (very high degree of dysregulation). A score of 1 represents a low degree of emotion dysregulation and describes a child who exhibits some combination of the following: (a) displayed only one or two brief emotional expressions that were inappropriate to the situation and who were able to regroup on his/her own, or (b) displayed one or two brief instances of emotional lability and/or variability in intensity of emotional expression and usually recovered quickly from inappropriate emotional experience. On the other hand, a score of 4 represents a very high degree of dysregulation and describes a child who exhibits some combination of the following: (a) displayed several intense, frequent emotional expressions and is virtually unable to regroup, or (b) very labile, extreme variability in intensity of emotion, and/or very slow to recover from emotional experiences. We used this coding system to measure child dysregulation only during the clean-up task in the parent-child interaction, which was intended to facilitate the need for the child to regulate his or her emotions in the face of an undesirable situation (i.e., being told to clean up). Data from this coding system were collected from all assessment time points. There was excellent inter-rater reliability on this coding system, with ICC = .96. Inter-rater reliability for Spanish videos from the second cohort (n = 7) was excellent (ICC = 1.00).
Parenting behavior
The Parent-Child Interaction Rating System (PCIRS; Belsky et al. 1995) is an observational coding system that measures parent and child behavior within a parent-child dyadic activity. Although the PCIRS includes different categories of parent qualities, the parent ratings of interest include indices of Sensitive Parenting and Intrusive Parenting, which are rated on a five-point Likert scale from 1 (not at all present) to 5 (highly characteristic). The sensitive parent is attuned to the child and manifests awareness of the child’s needs, moods, interests, and capabilities, and allows this awareness to guide his or her interaction with the child. A score of 1 on the Sensitive Parenting code indicates that there are almost no signs of parent sensitivity, and that the parent rarely responds appropriately to the child’s cues; whereas, a score of 5 indicates that the parent displays consistent sensitivity to the child throughout the rating period. Intrusive parents impose their agenda on the child despite signals from the child that a different activity, level, or pace of interaction is needed. A score of 1 on the Intrusive Parenting code indicates that there are almost no signs of parent intrusive behavior; whereas a score of 5 indicates that the parent is consistently intrusive, and that most of the observation period is marked by the parent completely controlling the interaction, allowing the child little lee-way in his/her play.
This coding system has been found to be a reliable and valid measure of naturalistic parent-child interaction (Fenning et al. 2007), and has been extensively used elsewhere (Crnic et al. 2005; Fenning et al. 2014). These data were rated by two sets of coders, one for each cohort of participants. The first set of coders rated 97 video clips from the first cohort; the second set of coders rated 158 video clips from the second cohort. For the first cohort, inter-rater reliability was variable across the three parent-child interaction activities. Inter-rater reliability was good for on the child-led and clean-up tasks for both sensitive parenting (ICC = .60 and .76, respectively) and intrusive parenting (ICC = .64 and .80, respectively); however, there was poor inter-rater reliability on the parent-led task (ICC = .39 and .40 for sensitive and intrusive parenting, respectively). For the second cohort, inter-rater reliability was high across child-led, parent-led, and clean-up tasks for both sensitive (ICC = .87, .88, and .89, respectively) and intrusive parenting (ICC = .97, .93, and .96, respectively). Inter-rater reliability for Spanish videos from the second cohort (n = 7) was high across child-led, parent-led, and clean-up tasks for both sensitive (ICC = .82, .86, and .88, respectively) and intrusive parenting (ICC = .92, .86, and .96, respectively). Due to the poor inter-rater reliability on the parent-led task for the first cohort of participants, we excluded data from the parent-led task, and used an average of the codes from the child-led and clean-up tasks for analysis.
Data Analyses
Examining relationship between parenting stress and emotion dysregulation
Due to the longitudinal nature of our study, missing data was an issue, such that 37.5% (n = 30) of cases had missing data at post-treatment. The majority of these missing cases were due to attrition from treatment (n = 17, 21.25% of the entire sample). Besides attrition, four cases had missing PSI-SF data, six cases had missing emotion dysregulation data due to missing or faulty video (e.g., no audio for coding), and three cases were excluded due to a violation of the PSI-SF validity index criterion. Independent sample t-tests indicated that there were no significant differences in outcome and demographic variables at baseline between those with and without data at post-treatment (p > .05). Because missing data was an issue, we used an Intent-to-Treat analysis (ITT; Chakraborty and Gu 2009) by using the Last Observation Carried Forward (LOCF, Shao and Zhong 2003) strategy to impute missing data, such that scores from baseline were used at post-treatment for cases with missing data. This strategy produces a more conservative estimate of treatment effects.
Using ITT with LOCF, we conducted a hierarchical linear regression analysis to examine whether changes in parenting stress through MBSR would predict changes in emotion dysregulation among children with DD. Baseline scores for child emotion dysregulation were entered in the first step of the regression, followed by baseline scores for parenting stress entered in the second step of the regression. Post-treatment scores for parenting stress were entered in the final step of the regression. By controlling for baseline levels of each variable, we were able to examine how changes in parenting stress were related to child emotion dysregulation.
Parenting behaviors as mediators
In the current study, we tested both sensitive parenting and intrusive parenting as possible mediators in the relationship between parenting stress and child emotion dysregulation at baseline. While researchers have used the causal steps strategy to analyze mediation models (Baron and Kenny 1986), this strategy is prone to Type 1 error and relies on null hypothesis significance testing, which does not actually test the significance of the mediation effect. More recent literature suggests that a multiple mediation analysis using bootstrapping is the most effective method of evaluating the significance of multiple mediators simultaneously (Preacher and Hayes 2008), and was therefore the analysis of choice in our study.
In the bootstrapping procedure, a sample of size n is taken with replacement from our sample, from which regression coefficients a and b are estimated and used to calculate the indirect effect ab. This process is repeated k times, producing an empirically-derived sampling distribution of ab, with the mean of this sampling distribution serving as our point estimate of the indirect effect. The bootstrapping procedure provides the total indirect effect, the specific indirect effect for each mediating variable, as well as all pairwise comparisons among the mediating variables. Additionally, standard errors and 95% confidence intervals are provided for each statistic. The confidence intervals (CIs) can be used to assess significance for the indirect effects of interest.
In our study, we used the statistical software SPSS 22 to conduct our analysis with the “INDIRECT” macro for bootstrapping in multiple mediation (Preacher and Hayes 2008). Using this macro, we included parenting stress as the x-variable, child emotion dysregulation as the y-variable, and sensitive parenting as well as intrusive parenting as the mediating variables. Estimates of the total indirect effect, specific indirect effects for each mediating variable, pairwise contrast among mediators, standard errors, and 95% CIs were calculated from 5000 randomly sampled bootstraps. We set the macro to calculate bias-corrected (BC) 95% CIs, because they are considered to be the most accurate (Preacher and Hayes 2008). Indirect effects for each mediator were considered to be significant at α = .05 if the BC 95% CI does not contain zero.
Results
Preliminary Data Analyses
Distributions for each variable were screened for univariate outliers with z scores greater than 3 and multivariate outliers with Mahalanobis distances exceeding the critical value for α = .001 (Tabachnick and Fidell 2013). One univariate outlier was found in the PCIRS Intrusive Parenting code at baseline (z = 4.05). Following the recommendations by Cohen et al. (2002), all univariate outliers were set equal to plus or minus three standard deviations from the mean in order to reduce the influence of extreme data points on the results. No multivariate outliers were detected. Further, demographic variables and child characteristics (i.e., child behavior problems and whether the child was receiving behavioral services) that had a significant relationship with one or more of the independent variables and one or more of the dependent variables would have been tested as covariates in the analyses. No covariates were identified for the subsequent analyses. Finally, our data did not violate the assumptions of linear regression.
Regarding descriptive statistics of the outcome variable, children were observed to exhibit a low degree of emotion dysregulation at baseline, characterized by a few brief emotional expressions that are inappropriate to the situation, and/or a few brief instances of emotional lability or variability in intensity of emotional expressions (M = 1.00, SD = 1.12). Descriptive statistics of key study variables are presented in Table 2.
Examining the Relationship between Parenting Stress and Emotion Dysregulation
Using Intent-to-Treat Analysis with the Last Observation Carried Forward strategy, we conducted a hierarchical linear regression to determine whether post-treatment levels of parenting stress predicted post-treatment child emotion dysregulation, after controlling for the effects of baseline levels of child emotion dysregulation and parenting stress. Results indicated that after controlling for baseline child emotion dysregulation and parenting stress, post-treatment parenting stress significantly predicted post-treatment child emotion dysregulation, such that a one standard deviation increase in post-treatment parenting stress was associated with a 0.27 standard deviation increase in post-treatment child emotion dysregulation (β = 0.27, sr2 = .06, p < .05). Adding post-treatment levels of parenting stress to our model explained approximately 6% of the variance in post-treatment child emotion dysregulation above and beyond the contributions of baseline child emotion dysregulation and parenting stress (p < .05). Results are summarized in Table 3.
Parenting Behaviors as Mediators
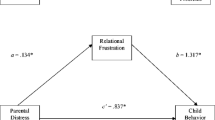
We conducted a multiple mediation analysis using bootstrapping to determine whether sensitive and intrusive parenting mediated the relationship between parenting stress and child emotion dysregulation at baseline (See Table 4 and Fig. 1). Results indicated that only intrusive parenting significantly mediated the relationship between parenting stress and child emotion dysregulation. Specifically, as parenting stress increased by one-point, child emotion dysregulation increased by 0.01 points via the effect of intrusive parenting, BC 95% CI [0.0004, 0.0328]. Sensitive parenting did not significantly mediate the relationship between parenting stress and child emotion dysregulation, BC 95% CI [−0.0040, 0.0056]. A pairwise comparison of the specific indirect effects showed that the relative strengths of the two mediators were not significantly different from each other, BC 95% CI [−0.0356, 0.00043].

Results of analysis testing sensitive and intrusive parenting as mediators of the relationship between parenting stress and child emotion dysregulation at baseline. Asterisks denote significance at p < .05
Discussion
A growing body of research suggests that family processes and parental well-being play key roles in a child’s emotional and behavioral development (Crnic and Neece 2015; Woodman et al. 2015). In particular, researchers have recognized parenting stress as a salient risk factor in the development of children with developmental delay (DD). However, few studies have examined the relationship between parenting stress and emotion dysregulation among children with DD. In the current study, we investigated the extent to which parenting stress influences emotion dysregulation in a sample of young children with DD. Accordingly, using MBSR in the current study allowed us to experimentally manipulate parenting stress and examine its subsequent effects on child emotion dysregulation. Recent studies have shown that MBSR is not only a feasible intervention to implement among families with children with DD (Roberts and Neece 2015), but it is also effective in reducing parenting stress in this population (Bazzano et al. 2015; Dykens et al. 2014; Minor et al. 2006; Neece 2014). In particular, data from a recent randomized controlled trial demonstrated that MBSR was effective in reducing parenting stress within the same sample of parents used in the current study (Chan and Neece 2018).
Results from the current study suggest that a significant relationship exists between parenting stress and child emotion dysregulation, such that reductions in parenting stress through an empirically-based stress reduction intervention, Mindfulness-Based Stress Reduction (MBSR), predicted reductions in emotion dysregulation among children with DD. It should be noted that our results demonstrate that baseline levels of parenting stress did not significantly predict post-treatment child emotion dysregulation (Model 2 in Table 3), suggesting that changes in child emotion dysregulation did not depend on parents’ initial stress levels prior to intervention; instead, it was changes in parenting stress through MBSR that significantly predicted changes in child emotion dysregulation. Results from our study are consistent with those in the extant literature, which suggest that higher levels of parenting stress are associated with higher levels of child emotion dysregulation among typically-developing children (Mathis and Bierman 2015; Samuelson et al. 2017). Moreover, our study extends these findings by employing a more rigorous methodological approach in examining the relationship between parenting stress and child emotion dysregulation. Previous studies relied on cross-sectional data, limiting the extent to which we can make conclusions regarding causal mechanisms and directionality of effects. In our study, we experimentally manipulated parenting stress using MBSR, and observed subsequent changes in the child emotion dysregulation over time.
In addition to examining the effect of parenting stress on child emotion dysregulation, we also examined parenting behaviors (i.e., sensitive and intrusive parenting) as potential mediators in this relationship. Results from our study suggest that intrusive parenting, but not sensitive parenting, significantly mediated the relationship between parenting stress and child emotion dysregulation at baseline. It should be noted that the effect size for intrusive parenting as a mediator was relatively small (ab = 0.01). This may be explained by the floor effect seen in our observational measure for intrusive parenting, in which intrusive parenting was a relatively low frequency behavior (M = 1.37, SD = 0.51). Yet, despite the small effect size and low frequency of intrusive parenting behaviors observed, it was still a significant mediator, suggesting that intrusive parenting, even at low frequencies, may have a significant impact on children’s regulation abilities. Furthermore, intrusive parenting was measured in relatively short laboratory-based parent-child interaction tasks where parents knew they were being observed. Thus, it is notable that we observed a significant effect of intrusive parenting given the context of the parent-child interaction used for the observations. We also used different measurement methods to assess the variables of interest (i.e., parent-report questionnaire, observational), which reduces shared method variance and increases objectivity, specifically with regard to the observational measures of parenting behavior which reduce the risk of biases inherent in self-report measures of parenting behaviors (Burbach and Borduin 1986; Krain and Kendall 2000); however, multi-method analyses are more conservative (McLeod et al. 2007).
In our study, we conceptualized intrusive parents as those who impose their will on their child during interactions, overwhelming their child with excessive stimulation, and leaving little to no room for their child to dictate the pace of the play or interaction. Indeed, when parents are highly stressed, they may have less cognitive resources to attend to their child’s pace and interests, and may be more likely to impose their own agenda over their child’s during play. This is consistent with previous research conducted among parents of children with typical development, which showed that both physiological (i.e., cortisol; Mills‐Koonce et al. 2009; Tarullo et al. 2017) and parent-report (Pianta and Egeland 1990) measures of stress were associated with intrusive parenting. Furthermore, it is possible that when parents engage in more intrusive parenting, they may overwhelm their child with constant stimulation, making it difficult for the child to have an opportunity to regulate his or her own emotions during challenging situations, resulting in increased emotional dysregulation. A previous longitudinal study demonstrated that intrusive parenting during infancy led to higher levels of child emotion dysregulation in the first grade (Egeland et al. 1993). While the associations between these variables have been explored in the typically-developing children literature, our study contributes to the literature by testing the full mediational model among families of children with DD.
Inconsistent with our hypothesis, however, our results suggested that sensitive parenting did not significantly mediate the relationship between parenting stress and emotion dysregulation among children with DD at baseline. In our study, we conceptualized the sensitive parent as one who is attuned to the child and manifests awareness of the child’s needs, moods, interests, and capabilities, and allows this awareness to guide his or her interaction with the child. It is possible that the role of sensitive parenting in child development may differ depending on the age of the child. It may be that sensitive parenting is necessary for providing support to the child while the child is still dependent on the parent to help with emotion regulation, but becomes less important as the child becomes more autonomous. For instance, in a study conducted among parents of infants, parents who experienced higher levels of daily parenting stresses exhibited less sensitivity in their parenting, which was subsequently associated with higher levels of oppositional and emotionally dysregulated child behavior (Patterson and Fisher 2002). On the other hand, in a study conducted among parents of children transitioning from preschool to kindergarten, warm-sensitive parenting was not found to significantly mediate the relationship between parenting stress and child emotion regulation (Mathis and Bierman 2015). This is consistent with results from our study, in which sensitive parenting did not mediate the relationship between parenting stress and emotion dysregulation among children between the ages of 2½ and 5 years old. Future studies would benefit from using longitudinal data to examine the extent to which the relationship between sensitive parenting and child emotion dysregulation changes across the trajectory of a child’s development.
Besides the age of the child, it is possible that negative parenting behaviors (e.g., intrusive parenting) may have a greater influence on child emotion dysregulation than positive parenting behaviors (e.g., sensitive parenting) among families of children with DD. In our sample, parents displayed relatively high levels of sensitivity (M = 3.76, SD = 0.78), suggesting that, on average, parents were characterized as between “moderately sensitive” and “mostly sensitive.” As noted, there was no significant association between sensitive parenting and child emotion dysregulation or parenting stress in our sample. The role of sensitive parenting in relation to parenting stress and child outcomes may be more pertinent in populations in which sensitive parenting is a bigger concern and has been shown to have more variability (e.g., in the foster system; Gabler et al. 2014). On the other hand, although parents in our sample exhibited relatively lower levels of intrusive parenting (M = 1.37, SD = 0.51), our results showed significant associations between intrusive parenting and parenting stress as well as child emotion dysregulation. Whereas sensitive parenting has been found to promote more positive child outcomes among children with DD (i.e., cognitive development, social skills, attachment security; see Guralnick 2017 for a review), it is possible that the presence of negative parenting behaviors (e.g., intrusive parenting)—even when occurring infrequently or at low levels—may play a bigger role in the development of problematic child outcomes than positive parenting behaviors (e.g., sensitive parenting). This is consistent with recent studies, which have highlighted the role of negative parenting behaviors (such as criticism and harsh discipline) as mediators in the relationship between parenting stress and child behavior problems among children with autism spectrum disorders (Shawler and Sullivan 2017).
The study of the mechanisms through which parenting stress influences child emotion dysregulation may also have clinical implications. With over 40% of parents of children with DD reporting clinically significant levels of parenting stress (Davis and Carter 2008), there is a great need for stress-reduction interventions for this population. Researchers have argued that the best short-term and long-term investment for improving clinical practice and patient care is the study of mechanisms of treatment, because understanding why a given treatment works serves as a basis for maximizing its effects and ensuring that the critical features of treatment are generalized to clinical practice (Kazdin and Nock 2003). Our findings that parenting behaviors (i.e., intrusive parenting) may mediate the relationship between parenting stress and emotion dysregulation among young children with DD may be particularly relevant for interventions that target child emotion dysregulation via parent-training in this highly stressed population (e.g., The Incredible Years Preschool Basic Parent Program, Secret Agent Society: Operation Regulation; Dababnah and Parish 2016; Weiss et al. 2018). Because our findings suggest that parenting stress may influence child emotion dysregulation through the effects of parenting behaviors, it may be important to monitor and intervene with parents’ stress levels as they go through these parent-training interventions in order to optimize child outcomes. This is consistent with previous research which suggests that high levels of parenting stress decrease the efficacy of parent-training interventions, resulting in poorer child outcomes (Osborne et al. 2008). Future studies should investigate whether augmenting existing behavioral parent training programs (e.g., The Incredible Years; Webster-Stratton 2007) with a stress-reduction component would improve the efficacy of these interventions by reducing the parents’ intrusive parenting behaviors, and subsequently their child’s emotion dysregulation.
Limitations and Future Research
Although our findings were promising, these results must be considered within the context of several study limitations. First, because missing data was an issue in our longitudinal analysis, we imputed data using the Last Observation Carried Forward strategy (Shao and Zhong 2003). However, the LOCF strategy may have the potential to bias estimates of treatment effects and associated standard errors (Mallinckrodt et al. 2003). Thus, we also conducted the analysis using multiple imputation (Enders 2010) to address missing data, and found the same results, increasing our confidence in our findings. Second, in order to optimize our sample size, the mediation analysis relied on cross-sectional data at baseline; as a result, we cannot draw firm conclusions regarding directionality of effects. It may also be possible that child emotion dysregulation predicts parenting stress through the effects of parenting behaviors. Future studies may benefit from employing longitudinal data to examine the mechanisms through which parenting stress influence child emotion dysregulation. Third, our sample was heterogeneous in terms of child diagnoses. While the majority of children in our study were reported to have a diagnosis of Autism Spectrum Disorder (ASD), other child diagnoses reported in our sample include Down’s Syndrome, Intellectual Disability, Learning Disability, Prader-Willi Syndrome, Speech Delay, Cerebral Palsy, Fragile X, and Microcephaly. Considering that families of children with ASD tend to exhibit higher levels of parenting stress as well as more difficulties with emotion dysregulation compared to both typically developing and developmentally delayed children (Davis and Carter 2008; Mazefsky et al. 2012), future studies should consider examining an ASD diagnosis as a moderator in the relationship between parenting stress and child emotion dysregulation.
Despite these limitations, the implications of these results are significant. This study explored not only the impact of parenting stress on emotion dysregulation among children with DD using an experimental design, but also the mechanisms through which these processes occur. Our results suggest that parenting behaviors (i.e., intrusive parenting) may mediate the relationship between parenting stress and emotion dysregulation among children with DD. With a growing body of research suggesting that the family context plays an integral role in a child’s development (Crnic and Neece 2015; Woodman et al. 2015), this study reiterates the finding that parenting stress remains a salient risk factor in the development of emotional and behavioral difficulties in children with DD. As a highly vulnerable population in great need of intervention, it is important that future research further explore how early intervention with parents of children with DD may have a spillover effect for the child.
References
Abidin, R. R. (1990). Parenting Stress Index Manual. 3rd edn Charlottesville, VA: Pediatric Psychology Press.
Aldao, A., Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion-regulation strategies across psychopathology: a meta-analytic review. Clinical Psychology Review, 30, 217–37.
Anthony, K., Bromberg, M., Gil, K., & Schanberg, L. (2011). Parental perceptions of child vulnerability and parent stress as predictors of pain and adjustment in children with chronic arthritis. Children’s Health Care, 40, 53–69.
Anthony, L., Anthony, B., Glanville, D., Naiman, D., Waanders, C., & Shaffer, S. (2005). The relationships between parenting stress, parenting behavior and preschoolers’ social competence and behavior problems in the classroom. Infant and Child Development, 14, 133–154.
Baker, B. L., Blacher, J., Crnic, K. A., & Edelbrock, C. (2002). Behavior problems and parenting stress in families of three-year-old children with and without developmental delays. American Journal of Mental Retardation, 107, 433–444.
Baker, B. L., Neece, C. L., Fenning, R. M., Crnic, K. A., & Blacher, J. (2010). Mental disorders in five-year-old children with or without developmental delay: focus on ADHD. Journal of Clinical Child and Adolescent Psychology, 39, 492–505.
Baker, J. K., Fenning, R. M., Crnic, K. A., Baker, B. L., & Blacher, J. (2007). Prediction of social skills in 6-year-old children with and without developmental delays: contributions of early regulation and maternal scaffolding. American Journal on Mental Retardation, 112, 375–391.
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. Journal of personality and Social Psychology, 51, 1173.
Bazzano, A., Wolfe, C., Zylowska, L., Wang, S., Schuster, E., Barrett, C., & Lehrer, D. (2015). Mindfulness based stress reduction (MBSR) for parents and caregivers of individuals with developmental disabilities: a community-based approach. Journal of Child and Family Studies, 24, 298–308.
Belsky, J., Crnic, K., & Woodworth, S. (1995). Personality and parenting: Exploring the mediating role of transient mood and daily hassles. Journal of Personality, 63, 905–929.
Burbach, D. J., & Borduin, C. M. (1986). Parent-child relations and the etiology of depression: a review of methods and findings. Clinical Psychology Review, 6, 133–153.
Chakraborty, H., & Gu, H. (2009). A mixed model approach for intent-to-treat Analysis in longitudinal clinical trials with missing values. RTI Press Publication No. MR-0009-0903. Research Triangle Park, NC: RTI International.
Chan, N., & Neece, C. L. (2018). Mindfulness-based stress reduction for parents of children with developmental delays: a follow-up study. Evidence-Based Practice in Child and Adolescent Mental Health, 3(1), 16–29.
Chazan-Cohen, R., Raikes, H., Brooks-Gunn, J., Ayoub, C., Pan, B. A., Kisker, E. E., & Fuligni, A. S. (2009). Low-income children’s school readiness: parent contributions over the first five years. Early Education and Development, 20, 958–977.
Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychological Assessment, 6, 284–290.
Cohen, P., Cohen, J., West, S. G., & Aiken, L. A. (2002). Applied Multiple Regression/Correlational Analysis for Behavioral Sceinces. Hillsdale, NJ: Lawrence Erlbaum Associates.
Cole, P. M., Marin, S. E., & Dennis, T. A. (2004). Emotion regulation as a scientific construct: methodological challenges for child development research. Child Development, 75, 317–333.
Cole, P. M., Michel, M. K., & Teti, L. O. (1994). The development of emotion regulation and dysregulation: a clinical perspective. Monographs of the Society for Research in Child Development, 59, 73–100.
Crnic, K. A., Gaze, C., & Hoffman, C. (2005). Cumulative parenting stress across the preschool period: relations to maternal parenting and child behaviours at age 5. Infant and Child Development, 11, 201–209.
Crnic, K. A., Hoffman, C., Gaze, C., & Edelbrock, C. (2004). Understanding the emergence of behavior problems in young children with developmental delays. Infants & Young Children, 17, 223–235.
Crnic, K., & Neece, C. (2015). Socioemotional Consequences of Illness and Disability. Handbook of Child Psychology and Developmental Science 3, (1–37.
Dababnah, S., & Parish, S. L. (2016). Feasibility of an empirically based program for parents of preschoolers with autism spectrum disorder. Autism, 20, 85–95.
Davis, N. O., & Carter, A. S. (2008). Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: associations with child characteristics. Journal of Autism and Developmental Disorders, 38, 1278–1291.
Deater-Deckard, K. (1998). Parenting stress and child adjustment: Some old hypotheses and new questions. Clinical Psychology: Science and Practice, 5, 314–332.
Dykens, E., Fisher, M., & Taylor, J. (2014). Reducing distress in mothers of children with autism and other disabilities: a randomized trial. Pediatrics, 134, 454–463.
Egeland, B., Pianta, R., & O’Brien, M. A. (1993). Maternal intrusiveness in infancy and child maladaptation in early school years. Development and Psychopathology, 5, 359–370.
Eisenhower, A. S., Baker, B. L., & Blacher, J. (2009). Children’s delayed development and behavior problems: impact on mothers’ perceived physical health across early childhood. Social Science and Medicine, 68, 89–99.
Enders, C. K. (2010). Applied missing data analysis. New York, NY: Guilford Press.
Fenning, R. M., Baker, J. K., Baker, B. L., & Crnic, K. A. (2007). Parenting children with borderline intellectual functioning: a unique risk population. American Journal on Mental Retardation, 112(2), 107–121.
Fenning, R. M., Baker, J. K., Baker, B. L., & Crnic, K. A. (2014). Parent-child interaction over time in families of young children with borderline intellectual functioning. Journal of Family Psychology, 28(3), 326.
Firth, I., & Dryer, R. (2013). The predictors of distress in parents of children with autism spectrum disorder. Journal of Intellectual and Developmental Disability, 38, 163–171.
Gabler, S., Bovenschen, I., Lang, K., Zimmermann, J., Nowacki, K., Kliewer, J., & Spangler, G. (2014). Foster children’s attachment security and behavior problems in the first six months of placement: associations with foster parents’ stress and sensitivity. Attachment & Human Development, 16, 479–498.
Gerstein, E. D., y Arbona, A. P., Crnic, K. A., Ryu, E., Baker, B. L., & Blacher, J. (2011). Developmental risk and young children’s regulatory strategies: predicting behavior problems at age five. Journal of Abnormal Child Psychology, 39, 351–364.
Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness-based stress reduction and health benefits: a meta-analysis. Journal of Psychosomatic Research, 57, 35–43.
Guralnick, M. J. (2017). Early intervention for children with intellectual disabilities: an update. Journal of Applied Research in Intellectual Disabilities, 30, 211–229.
Hastings, R. P. (2002). Parental stress and behaviour problems of children with developmental disability. Journal of Intellectual and Developmental Disability, 27(3), 149–160.
Hastings, R. P., Daley, D., Burns, C., & Beck, A. (2006). Maternal distress and expressed emotion: cross-sectional and longitudinal relationships with behavior problems of children with intellectual disabilities. American Journal of Mental Retardation, 111, 48–61.
Hoffman, C., Crnic, K., & Baker, J. (2006). Maternal depression and parenting: implications for children’s emergent emotion regulation and behavioral functioning. Parenting: Science and Practice, 6, 271–295.
Japundža-Milisavljevic, M., & Macešic-Petrovic, D. (2008). Executive functions in children with intellectual disabilities. The British Journal of Developmental Disabilities, 54, 113–121.
Kabat-Zinn, J. (1990). Full catastrophe living: The program of the stress reduction clinic at the University of Massachusetts Medical Center. New York, NY: Delta.
Kazdin, A. E., & Nock, M. K. (2003). Delineating mechanisms of change in child and adolescent therapy: methodological issues and research recommendations. Journal of Child Psychology and Psychiatry and Allied Disciplines, 44, 1116–1129.
Kersh, J., Hedvat, T. T., Warfield, M. E., Hauser-Cram, P., & Warfield, M. E. (2006). The contribution of marital quality to the well-being of parents of children with developmental disabilities. Journal of Intellectual Disability Research, 50, 883–93.
Krain, A. L., & Kendall, P. C. (2000). The role of parental emotional distress in parent report of child anxiety. Journal of Clinical Child Psychology, 29, 328–335.
Mallinckrodt, C. H., Sanger, T. M., Dubé, S., DeBrota, D. J., Molenberghs, G., Carroll, R. J., & Tollefson, G. D. (2003). Assessing and interpreting treatment effects in longitudinal clinical trials with missing data. Biological Psychiatry, 53, 754–760.
Mathis, E. T., & Bierman, K. L. (2015). Dimensions of parenting associated with child prekindergarten emotion regulation and attention control in low-income families. Social Development, 24, 601–620.
Mazefsky, C. A., Pelphrey, K. A., & Dahl, R. E. (2012). The need for a broader approach to emotion regulation research in autism. Child Development Perspectives, 6, 92–97.
McLeod, B. D., Wood, J. J., & Weisz, J. R. (2007). Examining the association between parenting and childhood anxiety: a meta-analysis. Clinical Psychology Review, 27(2), 155–172.
Mills‐Koonce, W. R., Propper, C., Gariepy, J. L., Barnett, M., Moore, G. A., Calkins, S., & Cox, M. J. (2009). Psychophysiological correlates of parenting behavior in mothers of young children. Developmental Psychobiology, 51, 650–661.
Minor, H., Carlson, L., Mackenzie, M., Zernicke, K., & Jones, L. (2006). Evaluation of a mindfulness-based stress reduction (MBSR) program for caregivers of children with chronic conditions. Social Work in Health Care, 43, 91–109.
Moreira, H., Gouveia, M. J., Carona, C., Silva, N., & Canavarro, M. C. (2014). Maternal attachment and children’s quality of life: The mediating role of self-compassion and parenting stress. Journal of Child and Family Studies, 24(8), 2332–2344.
Morris, A. S., Silk, J. S., Steinberg, L., Myers, S. S., & Robinson, L. R. (2007). The role of the family context in the development of emotion regulation. Social Development, 16, 361–388.
Neece, C. L. (2014). Mindfulness‐based stress reduction for parents of young children with developmental delays: Implications for parental mental health and child behavior problems. Journal of Applied Research in Intellectual Disabilities, 27, 174–186.
Neece, C. L., Green, S. A., & Baker, B. L. (2012). Parenting stress and child behavior problems: A transactional relationship across time. American Journal on Intellectual and Developmental Disabilities, 117, 48–66.
NICHD Early Child Care Research Network. (2004). Affect dysregulation in the mother-child relationship in the toddler years: Antecedents and consequences. Development and Psychopathology, 16, 43–68.
Osborne, L. A., McHugh, L., Saunders, J., & Reed, P. (2008). Parenting stress reduces the effectiveness of early teaching interventions for autistic spectrum disorders. Journal of Autism and developmental Disorders, 38, 1092.
Patterson, G. R., & Fisher, P. A. (2002). Recent developments in our understanding of parenting: Bidirectional effects, causal models, and the search for parsimony. Handbook of parenting, 5, 59–88.
Pianta, R. C., & Egeland, B. (1990). Life stress and parenting outcomes in a disadvantaged sample: Results of the mother-child interaction project. Journal of Clinical Child Psychology, 19, 329–336.
Pisula, E. (2007). A comparative study of stress profiles in mothers of children with autism and those of children with Down’s syndrome. Journal of Applied Research in Intellectual Disabilities, 20, 274–278.
Posne, M. I., & Rothbart, M. K. (2000). Developing mechanisms of self-regulation. Development and Psychopathology, 12, 427–441.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40, 879–891.
Roberts, L. R., & Neece, C. L. (2015). Feasibility of mindfulness-based stress reduction intervention for parents of children with developmental delays. Issues in Mental Health Nursing, 36, 592–602.
Robinson, E. A., Eyberg, S. M., & Ross, A. W. (1980). The standardization of an inventory of child conduct problem behaviors. Journal of Clinical Child & Adolescent Psychology, 9, 22–28.
Samuelson, K. W., Wilson, C. K., Padrón, E., Lee, S., & Gavron, L. (2017). Maternal PTSD and children’s adjustment: Parenting stress and emotional availability as proposed mediators. Journal of Clinical Psychology, 73(6), 693–706.
Shao, J., & Zhong, B. (2003). Last observation carry‐forward and last observation analysis. Statistics in Medicine, 22, 2429–2441.
Shawler, P. M., & Sullivan, M. A. (2017). Parental stress, discipline strategies, and child behavior problems in families with young children with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 32, 142–151.
Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics. 6th edition Boston: Allyn & Bacon.
Tarullo, A. R., John, A. M. S., & Meyer, J. S. (2017). Chronic stress in the mother-infant dyad: Maternal hair cortisol, infant salivary cortisol and interactional synchrony. Infant Behavior and Development, 47, 92–102.
Thompson, R. A. (1994). Emotion regulation: A theme in search of definition. Monographs of the Society for Research in Child Development, 59, 25–52.
von Suchodoletz, A., Trommsdorff, G., & Heikamp, T. (2011). Linking maternal warmth and responsiveness to children’s self-regulation. Social Development, 20, 486–503.
Webster-Stratton, C (2007). Tailoring the Incredible Years Parent Programs according to children's developmental needs and family risk factors. In J. M. Briesmeister & C. E. Schaefer, (eds.) Handbook of parent training: Helping parents prevent and solve problem behaviors. (pp. 305–344). Hoboken, NJ, US: John Wiley & Sons Inc.
Weiss, J. A., Thomson, K., Burnham Riosa, P., Albaum, C., Chan, V., Maughan, A.,… & Black, K. (2018). A randomized waitlist‐controlled trial of cognitive behavior therapy to improve emotion regulation in children with autism. Journal of Child Psychology and Psychiatry. 10.1111/jcpp.12915.
Williford, A. P., Calkins, S. D., & Keane, S. P. (2007). Predicting change in parenting stress across early childhood: child and maternal factors. Journal of Abnormal Child Psychology, 35, 251–263.
Woodman, A. C., Mawdsley, H. P., & Hauser-Cram, P. (2015). Parenting stress and child behavior problems within families of children with developmental disabilities: Transactional relations across 15 years. Research in Developmental Disabilities, 36, 246–276.
Author Contributions
N.C. designed and conceptualized the current study, coded and analyzed the data, and drafted the manuscript. C.N. was the P.I. for the larger study; obtained funding and oversaw all elements of the larger study; provided feedback on the design, writing, and interpretation of the data; and contributed edits and revisions of the manuscript.
Funding
This study was funded by the GRASP (Grants for Research and School Partnership Program) awarded to the second author.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study. Procedures were approved by the Institutional Review Board at Loma Linda University.
Rights and permissions
About this article

Cite this article
Chan, N., Neece, C.L. Parenting Stress and Emotion Dysregulation among Children with Developmental Delays: The Role of Parenting Behaviors. J Child Fam Stud 27, 4071–4082 (2018). https://doi.org/10.1007/s10826-018-1219-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-018-1219-9