
Abstract
There is an increasing number of young adults living at home with their parents, and this can lead to tension and conflict in the family home. One way to help increase the pro-social interactions and connectedness between young adults and their parents is with using Loving-Kindness Meditations (LKM). There is considerable evidence suggesting that LKM, which is a cultivation of good-will for self and others, can have many direct benefits on psychological distress and interpersonal interactions, and can indirectly increase self-compassion. This study examined the effects of using a 15-min Loving-Kindness Meditation for young adults living. A total of 97 participants (79 female, mean age = 18.64 years), were randomly allocated to LKM or a Focused Imagery control. Participants completed measures examining self-compassion, compassion motivation, and emotional, cognitive and interpersonal responses to vignettes describing conflict between young adults and their parents. As predicted, compared to controls, young adults who received LKM were higher in motivation to be self-compassionate, however, there was no difference in levels of self-compassion. Initial fear of self-compassion influenced emotional responses on the vignettes. The findings suggest that self-compassion could assist young adults in managing their own internal distress when interacting with their parents.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Loving-kindness meditations (LKM) stem from Buddhist traditions and is a practice that forms part of the four immeasurables, which include: compassion, equanimity, appreciative joy and loving-kindness (Wallace 1999). Specifically, LKM is an intention and wish that others, as well as self, flourishes and has a positive life well-being (Bodhi 1994). This differs to compassion, which focuses on suffering and alleviation and prevention of that suffering and its causes (Bodhi 1994). Therefore, the focus of LKM compared to compassion meditations differs slightly, where LKM does not require suffering in others and self, which compassion does. Despite this distinction, empirical research examining LKM has found that through specifically cultivating loving-kindness for self and others it can reduce psychological distress, increase well-being, and also indirectly increase individuals’ own levels of self-compassion (Galante et al. 2014; Jazaieri et al. 2013; Neff and Germer 2013). LKM as a practice typically uses a progressive sequence of contemplations that start with wishing safety, good health, happiness and peace to self, then a good friend, a neutral person, a “difficult” person, and finally to all of humanity without distinction (Buddharakkhita 1995; The Dalai Lama 2001).
The effectiveness of LKM has been examined in numerous randomized controlled trials (RCTs; Carson et al. 2005; Fredrickson et al. 2008), and has also been evaluated in a number of systematic reviews and meta-analyses (Galante et al. 2014; Hofmann et al. 2011; Shonin et al. 2015). Specifically, LKM has been found to be helpful for individuals with chronic lower back pain (Carson et al. 2005), individuals wanting to reduce stress (Fredrickson et al. 2008), individuals with schizophrenia (Johnson et al. 2011), and individuals with high levels of self-criticism (Shahar et al. 2015). LKM has since emerged as an integral component in several compassion-based interventions (Kirby 2016), including the Mindful-Self Compassion program (Neff and Germer 2013), the Compassion Cultivation Training program (Jazaieri et al. 2013), Cognitively-Based Compassion Training (Pace et al. 2009), and also in Compassion-Focused Therapy (Gilbert 2014).
A recent systematic review and meta-analysis conducted on LKM and Compassion Meditations (CM; Shonin et al. 2015) concluded that both Buddhist-derived interventions have applications towards a range of mental health issues, such as depression, anxiety, stress, emotional suppression, interpersonal skills, and fears of self-compassion. Shonin et al. (2015) reviewed in total 20 studies and indicated that LKM and CM may be acceptable for adolescents, students, and adults, in both clinical settings and for the general population. Moreover, Shonin et al. (2015) highlighted that LKM can be taught in a short time period, such as in a single session of 20 min (May et al. 2012). As a single session, LKM has also been examined by Templeton (2007) who found that participants who listened to a 20-min LKM recording reported more compassion, though only measured by a single item, and more positive emotion than a progressive relaxation control group. Feldman et al. (2010) found that a 15-min LKM was not as effective at de-centering as a mindful breathing exercise, nor in reducing negative reactions to repetitive thoughts. Crane et al. (2010) measured conditional goal setting, a trait positively correlated with depressive symptoms, before and after a 15-min LKM, and found that it was significantly increased by the meditation. In another study Hutcherson et al. (2008) found that compared to an equivalent focused imagery task, participants who engaged in a 7-min LKM reported improved mood, and increased explicit and implicit feelings of social connection to novel individuals. Finally, Law (2012) randomly assigned 113 undergraduate students (mean age 18.97) to either a 10-min LKM or an imagery control condition and found that the LKM group had greater implicit positivity towards themselves than the control group, and protected against some negative effects of social stress. Collectively, although these results are somewhat mixed, overall these results indicate how a single session of LKM can have an immediate impact on outcomes of interest.
Two other reviews of LKM, one a systematic review (Hofmann et al. 2011) and the other a meta-analysis (Galante et al. 2014) have also explored the positive impacts of LKM. In the review by Hofmann et al. (2011) they found LKM to have moderate to large significant effects on alleviating depression, social anxiety, marital conflict, and anger. Galante et al.’s (2014) meta-analysis included 22 RCTs, and found significant moderate effect sizes for depression (Hedges’s g = 0.60), self-compassion (Hedges’s g = 0.45) and positive affect (Hedge’s g = 0.42). Thus, as an intervention LKM offers itself as a potential trans-treatment approach for clinicians in attempting to address a range of presenting problems, including reducing interpersonal difficulties and for a range of populations.
An important consideration when using LKM is whether the individual has a fear of self-compassion. Gilbert (2014) has also postulated that an individual’s initial fears of self-compassion is an important moderator when considering LKM exercises. That is, individuals you believe that there are not deserving of support or kindness from others will respond negatively to the concept of giving kindness to themselves (Gilbert et al. 2011). Importantly, the relationship of fear of self-compassion to LKM in isolation has not been previously studied (Galante et al. 2014), but in combination with therapist-based treatment programs it has been found that people with high levels of fear towards self-compassion do not respond favourably to LKM or self-compassion based exercises (Kelly and Cater 2014), Therefore, examination of initial fears of self-compassion will be of interest when examining LKM in isolation.
A context where LKM could be helpful is with young adults living at home, yet there is a paucity of research assessing its potential in this population. When defining young adults there are many different definitions, for example the Australian Bureau of Statistics (ABS 2007) typically considers youth aged between 16 to 24 years, whereas others indicate to be considered a young adult you must be over 18 years (Aquilino 1997), and others again suggest young person is anyone over 12 years of age (McGorry 1996). For our study we were interested in those individuals between 18–25 years, which is often used when describing mental health prevalence rates (Kessler et al. 2005). Young adulthood is characterized by transitions: transitions from school, family relationships, romantic relationships, working environments, and living arrangements (Aquilino 1997; Dubas and Petersen 1996; Weston et al. 2001; White 2002). Typically a time of uncertainty and instability, it is not surprising that young adulthood has been described as a stressful period with high levels of interpersonal stress between family members and friends (Neff and Pommier 2012; White 2002). Despite young adults indicating an increased desire to be independent (White 2002), this is tempered with the realization that there are many times where young adults still require the support, both emotionally and financially, of their parents. This struggle can lead to family conflict and tension, which can negatively impact the relationship between the young adult and parent (Weston et al. 2001; White 2002). Loving-Kindness Meditations, which have been found to help with interpersonal difficulties, emotions such as anger, and for increasing self-compassion could be one way to help support young adults during this period of uncertainty and stress, particularly with the relationship with their parents, yet this has not been investigated.
Despite LKM not being specifically investigated to examine the relationship between young adults and parents, there has been some research examining self-compassion, with results indicating that it is helpful in moderating the effect of negative family functioning on young adults. In a cross sectional survey of 235 adolescents and 287 young adults Neff and McGehee (2010) found that for both groups, self-compassion partially mediated the effect of maternal support, family functioning and attachment style on depression, anxiety and social connectedness. The authors concluded that self-compassion has the potential to help soothe pain and conflict between family members, such as between young adults and parents (Neff and McGehee 2010), but this has not yet been tested empirically. In another study, Yarnell and Neff (2013) examined the association between self-compassion and conflict resolution style in young adults when interacting with their mothers, fathers, best friends, and romantic friends. The study asked 506 young adults whether they resolved their conflicts by (a) subordinating, (b) self-prioritizing or, (c) compromising. It was found that across all relationships, higher levels of self-compassion were linked to greater compromising. The authors suggested that self-compassionate individuals are more likely to resolve relationship conflict in a way that balances the needs of self and others, which keeps the interpersonal relationship positive. These results suggest that Buddhist approaches such as self-compassion and loving-kindness can play an important role in the experience of family relationships, and may be a viable option of protecting against harmful family interactions.
One way to examine the utility of LKM and whether it improves the young adult-parent relationship is to experimentally evaluate its usefulness in a micro-trial design (Kirby 2016). Micro-trials can be operationally defined as a way to test the effects of relatively brief and focused environmental manipulations (typically in experimental conditions) designed to suppress risk mechanisms or enhance protective mechanisms, but not to bring about full treatment or prevention effects on distal outcomes (Howe et al. 2010). If such experimental evidence is found that LKM can positively influence the young adult-parent relationship, and improve the level of self-compassion for young adults, this provides greater evidence for its use as an intervention, which can then be tested in larger more costly randomized controlled trials (Kirby 2016).
There are two key benefits to using a micro-trial design in this experiment. The first is their cost-effective and low-burden nature, as it makes them a feasible starting-point for research regarding novel applications of existing interventions (Kirby 2016). The second is that they allow testing of an individual component, in this case LKM, through an isolated experiment, allowing evidence of its preliminary impact to be gathered at its smallest unit (Embry and Biglan 2008).
The aim of this study was to examine the impact of using LKM with young adults living at home to determine whether it could positively influence the relationship between young adult and parents. The current study developed a between-groups experimental micro-trial design. Participants were randomly assigned to receive either LKM or a Focused Imagery task, which was used as a control condition against LKM (Hutcherson et al. 2008; Law 2012). Based on previous research, it was hypothesized that relative to the FI group, young adults in the LKM group would experience higher levels of self-compassion and motivation to be compassionate. Second, it was hypothesised that in response to a series of hypothetical conflict scenarios between young adults and parents, the LKM group, compared to the control, would report less of an emotional reaction (e.g., stress, anxiety, frustration and anger); more self-compassionate cognitions; and show a greater chance of engaging in compromise than other less socially useful reactions. Third, it was hypothesised that initial fear of compassion would moderate these outcomes. Thus, it was predicted that individuals with low levels of fear of self-compassion would have larger effects on the compassion outcomes and conflict vignettes when compared individuals with high fear of self-compassion.
Method
Participants
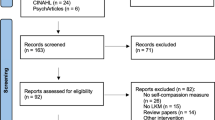
The sample was 97 undergraduate University students living at home, consisting of 79 females and 18 males, ranging in age from 18 to 25 years (M = 18.64, SD = 1.41). The sociodemographic characteristics of the sample are presented in Table 1. Participants were recruited through psychology undergraduate courses, and received one course credit for their participation. The description of the study stated that the young adults needed to be living at home with their parents, and that the study would include listening to audio guided instructions. The ethical approval for the study was obtained from the University of Queensland, and all participants gave their informed voluntary consent. Participants were randomly assigned to LKM or FI (control condition) through Qualtrics randomization software. The experimenters were blind to assigned condition. Two participants did not complete the experiment due to technological failures and were removed prior to data analysis. The study was granted ethical approval through the University of Queensland. See Table 1 for demographics.
Procedure
This experiment was conducted using a between-groups design, where participants were randomly allocated into an experimental group and a control group. Participants were given an information sheet and invited to sit at a computer in a group-based lab with eight computers, where the online survey was set up. After reading the information sheet and giving their informed consent participants were then instructed to put on the headphones provided and listen to the audio recording embedded in the online questionnaire software (Qualtrics). For the experimental group this was the LKM, and for the control group, a Focused Imagery (FI) exercise was used. A timer was added to the experiment so that participants could not move forward from the audio recording until 15 min had passed. The study was completed in the University of Queensland’s Psychology laboratories, and was structured in four parts. Participants first received a set of preliminary questionnaires including: demographic questions, as well as questions related to mental health and fears of compassion. Second, participants were randomly assigned to listen to the LKM (experimental condition) or FI (control condition) audio-guided recording. Third, participants completed the dependent measures, which included responding to a series of Conflict Vignettes, the Self-Compassion Scale, and the Compassion Motivation Scale. Lastly, participants completed the Manipulation checks and Social Desirability Scale. All participants were given a debriefing sheet by the experimenter once the experiment was completed.
Two audio-guided recordings (each approximately 15 min) were created for use in this study. Both recordings were developed and voiced by the first author. In both conditions the first author provided instructions to the participants. LKM follows a structured script with six steps: (a) a mindful focus on the breath; then directing phrases to, (b) oneself; (c) a person that makes them smile; (d) a stranger; (e) someone they dislike; and (f) finally to a group, such as a family, community or all of humanity. The LKM exercise was based on the structure provided by Hofmann et al. (2011) and Germer (2009). The whole guided meditation can be accessed from here https://soundcloud.com/jamesn-kirby/loving-kindness-meditation, and the initial instructions for the exercise included:
Hi, I’m James, and today I will take you through an exercise called a Loving-Kindness Meditation. The meditation aims to bring warmth and good will into your life. All up it will take 15 min to complete. And all you need to do is follow my instructions as we go along. So to begin with get yourself comfortable. Sit reasonably upright, but not overly rigid. Rest your hands by your side or on your legs. And when you are ready you might like to gently close your eyes.
The Focused Imagery (FI) exercise was used as the control condition. It has been used previously when evaluating the impact of LKM (e.g., Hutcherson et al. 2008; Law 2012), as it aims to control for the effects of both audio-guided instructions and visual imagery. FI encourages participants to visualise different aspects of the face and body focusing on specific regions (i.e. shape of face, eyebrows), first starting with themselves, then moving towards visualizing others. The whole guided imagery exercise can be accessed from https://soundcloud.com/jamesn-kirby/focused-imagery, and the initial instructions for the exercise included:
Hi, I’m James, and today I will take you through an exercise called a Focused Imagery Technique. The aim of the technique will be to visualize different parts of your body such as your aims, legs and face. All up it will take 15 min to compete. And all you need to do is follow my instructions as we go along. So to begin with get yourself comfortable. Sit reasonably upright, but not overly rigid. Rest your hands by your side or on your legs. And when you are ready you might like to gently close your eyes.
Measures
Demographic information
Questions on demographics included: age, gender, ethnicity, employment, relationship status, previous mindfulness experience, previous time spent living away from home, nights spent at home per week, and whether they had concerns with the relationship with their mother or father.
Mental health
The Depression Anxiety Stress Scale with 21 items (DASS-21, Lovibond and Lovibond 1995) was used. The measure has three subscales: depression, anxiety and stress, which are calculated by summing the relevant seven items. A sample item is ‘I found it difficult to relax’. Items are scored on a scale from zero ‘Did not apply to me at all’ to three ‘Applied to me very much, or most of the time’. In this study it had excellent internal consistency overall (α = .92), and good internal consistency for each subscale (depression α = .90, anxiety α = .73, and stress α = .83). The DASS has also been found to have previous good internal consistency (α = .95) and good discriminant and convergent validity (Lovibond and Lovibond 1995).
Psychological flexibility
The Acceptance and Action Questionnaire—II (AAQ-II; Bond et al. 2011) was used to assess psychological flexibility and it is a seven-item scale, which has been shown to have good reliability (α = .84) and convergent validity with other scales of psychological distress. A sample item is: ‘I’m afraid of my feelings’. The items are scored on a five-point Likert scale form one ‘Never true’ to seven ‘Always true’. The items are summed with higher scores indicating higher levels of psychological flexibility. In this study it had good internal consistency (α = .88).
Fears of compassion
The Fear of Compassion Scale (FCS; Gilbert et al. 2011), specifically the fear of expressing compassion to oneself was used. The FCS is a 15-item scale measuring participants’ fear of giving compassion to themselves. A sample item is: ‘I feel I don’t deserve to be kind and forgiving to myself’. Items were scored on a five-point Likert scale from zero ‘Don’t agree at all’ to four ‘Completely agree’. The items are summed with higher scores indicating higher fears of self-compassion. In this study it had excellent internal consistency (α = .91). The FCS has previously shown good reliability (α = .92) and convergent validity with self-criticism and the SCS (negative association; Gilbert et al. 2011).
Compassion motivation scale (CMS)
An 11-item questionnaire was developed to measure the individual’s motivation to direct compassion towards oneself. This measure assessed participants’ desire, ability, and readiness to engage in self-compassion. An example item included, “I would like to be kind and caring towards myself”. The scale is scored on a five-point Likert scale, from one ‘Strongly Disagree’ to five ‘Strongly Agree’. Items are averaged to find a mean score. The CMS was found to have good internal consistency (α = .93), good convergent validity with the SCS (r = .20, p = .048), and negatively with the Fear of self-compassion scale (FCS; r = −.25, p = .012).
Self-compassion scale
The Self-Compassion Scale (SCS; Neff 2003) was used to measure self-compassion. It is a 26-item scale designed to assess an individuals’ tendency towards self-compassion. It has a total score, and six subscales scores: self-kindness, self-judgement, common humanity, isolation, mindfulness and over-identification. An example item is: ‘I’m kind to myself when I’m experiencing suffering.’ Items were measured on a five-point Likert scale from one ‘Almost never’ to five ‘Almost always’. Cronbach’s alpha (α) was .89 indicating the scale had good internal consistency. Internal consistencies for each subscale were: self-kindness: α = .81, self-judgement: α = .69, common humanity: α = .54, isolation: α = .76, mindfulness: α = .74, and over-identification: α = .63. Previously it has also been shown to have excellent internal consistency overall (α = .92), and for each sub-scale (α’s > .75) The SCS has previously demonstrated both convergent and discriminant validity (Neff 2003).
Conflict vignettes
There were six hypothetical scenarios developed, each detailing a conflict situation between a young adult and a parent (e.g., “Your parents state that you have no life plans, and don’t inform them enough about what you do. You reply by saying at the moment your focus is just to complete your degree, but they say that is not good enough”). The theme of each vignette was concerning an interpersonal conflict between the young adult and parent, and included: (1) coming home late, (2) wanting boy/girlfriend to stay the night, (3) attend a party of a friends over being at a family event, (4) not contributing enough financially to the running of the house, (5) not helping enough around the house, and (6) parents ask you when you plan to move out. Participants’ were asked to imagine that they were the young adult. Each vignette assessed multiple items across three scales, (a) emotional, (b) cognitive, and (c) interpersonal.
The Emotional Scale consisted of items measuring seven different emotions. Participants were asked to rate the intensity of emotions on a scale from 0 (Low Intensity), to 10 (High Intensity). The seven emotions were adopted from Goetz et al. (2010) appraisal framework of distress: anxiety, stress, sadness, anger, frustration, calmness and sympathy. Participants’ scores for each emotion were averaged across the six vignettes, giving seven separate emotion scores. All emotion scores demonstrated good internal consistency (ranging from α = .80 to α = .85).
The Cognitive Appraisal Scale consisted of six items assessing the cognitions of self-compassion according to Neff (2003): kindness, mindfulness, common humanity, over-identifying, judgement, and isolation. For example, the item assessing mindfulness asked ‘How likely is it that you would notice that this is a moment when you are struggling?’ Items were assessed on a five-point Likert scale from 1 (Strongly Disagree) to 5 (Strongly Agree). Each cognition score was averaged across the six vignettes, giving six separate cognition scores. Each cognition score had good internal consistency (ranging from α = .79 to α = .86).
The Interpersonal Response Scale consisted of four items assessing responses to the situation. Options were informed by Rahim’s (1983) model of handling interpersonal conflict. The options included: anger, avoidance, submission, and compromise. For example, the compromise item was: ‘In this scenario, what is the likelihood of you reacting in the following way: try to understand your parents point of view, and attempt to compromise’. Items were answered on a five-point Likert scale from one (Not at all likely) to five (Very likely). Scores for each interpersonal response was averaged across the six vignettes, giving four different scores. Each interpersonal response score had good internal consistency (ranging from α = .77–α = .83).
Social desirability
The Social Desirability Response Set-5 (SDRS-5; Hays et al. 1989) was used, and has good internal consistency (α = .72) and test-retest reliability (α = .75). The Social Desirability scale is a five-item measure assessing individuals’ bias to answering questions in a socially desirable manner. An example item is: ‘I am always courteous even to people that are disagreeable.’ Items were scored on a five-point Likert scale, from one ‘Definitely True’ to Five ‘Definitely False’, and were dichotomized into socially desirable responses, extreme scores in the appropriate direction, and all other responses. The dichotomized scores were translated to a 100-point mean with higher scores indicating higher social desirability. This scale had good internal consistency (α = .71), and in previous studies it has shown sound internal consistency (α = .68; Hays et al. 1989).
Manipulation checks
Two questions were included to assess participants’ engagement with the audio-guided recordings. The first question: “How closely did you listen to the initial audio instructions? ” was measured on a seven-point Likert scale from one (Very True) to seven (Very Untrue). The second question: “Did you find the initial recording made you feel compassionate? ” was measured on a five-point Likert scale from one (Strongly Disagree) to five (Strongly Agree).
Data Analyses
Preliminary analyses compared participants’ scores on all pre-measures between the two groups (LKM v. FI) using chi-square tests (for categorical variables) and t-tests (for continuous variables). Bivariate correlations were also conducted on pre-measures: DASS, AAQ-II and FCS across conditions. Fear of self-compassion scores were converted into two groups, low and high, using a median-split approach (Maxwell and Delaney 1993). A series of Multivariate Analyses of Variance (MANOVAs) and ANOVAs assessed the impact of condition and level of fear of self-compassion on the outcomes at post.
Two participants were deleted, as they did not fill out all the questionnaires due to technological failures, leaving a total sample of 95 participants. Missing data was found to be missing completely at random (Little’s MCAR test: χ 2 (856) = 402.22, p > .99) and so was estimated using the Expectation Maximisation (EM) approach (Dempster et al. 1977).
Results
A series of chi-square tests and independent samples t-tests found no significant differences in demographics between the two groups, suggesting that the randomization process was successful in producing two equally comparable groups (see Table 1).
A MANOVA was conducted to assess differences in scores on pre-measures (AAQ-II, DASS-21 and FSC) between the two conditions (LKM vs. FI). A non-significant multivariate effect revealed that there was no difference between mean scores between the groups F(4,51) = 0.36, p = .818. Further univariate analyses revealed that there were no significant differences on each of the pre-measures between groups (see Table 2). There was no significant difference between participants’ scores on social desirability t(54) = −1.62, p = .106.
Significant bivariate correlations were found between participant’s scores on DASS-21, AAQ-II, and FCS across conditions (see Table 3).
No significant difference between conditions was found in terms of participants’ reported attention to instructions, t(92) = −1.31, p = .185). A significant t-test, t (92) = 2.61, p = .005, indicated that participants in the LKM condition found the audio recording to make them feel more compassionate than the FI condition.
All MANOVAs and ANOVAs used condition (LKM or FI) and fear of self-compassion (FCS; high or low) as independent variables.
A two-way MANOVA with condition and fear of self-compassion as IVs and the SCS mean and subscale scores as the dependent variables (DVs) found a non-significant effect of condition (Pillai’s Trace = .056, F (6, 91) = .90, p = .500, η2 p = .06), a significant effect of fear of self-compassion (Pillai’s Trace = .21, F (6, 91) = 3.96, p = .001, η2 p = .21), and a non-significant interaction effect (Pillai’s Trace = .06, F (6, 91) = 1.05, p = .397, η2 p = .07). Results from ANOVAs on the main effect of fear of self-compassion are reported in Table 4, with the low fear of self-compassion group scoring significantly lower on the self-judgement, isolation, and over-identification subscales of the SCS compared to the high fear of self-compassion group.
A two-way ANOVA with the CMS as the DV found that the LKM group (M = 4.05, SD = .40) scored significantly than the FI group (M = 3.81, SD = .35; F (1, 96) = 12.22, p = .001, η2 p = .11), that low fear of self-compassion (M = 4.03, SD = .44) scored significantly higher than high fear of self-compassion (M = 3.82, SD = .30; F (1, 96) = 10.99, p = .001, η2 p = .10), and that there was a significant interaction effect (F (1, 96) = 4.89, p = .029, η2 p = .05). Follow-up simple effects found that in the low FCS group, the LKM group scored significantly higher on the CMS than the FI group (F (1, 96) = 2.12, p > .001), while in the high FCS group, there was no significant difference (F (1, 96) = .10, p = .376). The results of the main effects are summarized in Tables 4 and 5.
A series of two-way ANOVAs with condition (LKM vs. FI) and fear of self-compassion as IVs were used to compare the two groups on all the measures used in the conflict vignettes, as reported in Table 4. The LKM group was significantly less anxious than the FI group (p = .030), and the low fear of self-compassion group was less anxious (p = .009), less stressed (p = .004), less angry (p = .021) and less frustrated (p = .027) than the high fear of self-compassion group. No other main effects were significant (see Tables 4 and 5) and no interaction effects were significant.
Discussion
This micro-trial designed experiment examined the impact of self-compassion on young adults and how they interact with their parents through a single 15-min LKM. There were three specific hypotheses, of which two were partially supported. The first hypothesis predicted that subjects in the LKM condition, compared to the FI condition, would report higher levels of self-compassion and motivation to be self-compassionate. This was partially supported. No difference was found in self-compassion scores, while motivation for self-compassion was higher in the LKM group but not the FI group, as expected. The lack of findings could be the result of the SCS being a reflection of a more stable trait measure, as opposed to a state based measurement. However, investigations of the moderating effects of fear of compassion (as tested in hypothesis 3), showed that higher levels of self-compassion were found for participants with initial low levels of fear of self-compassion, but not with participants with initial high levels of fear of self-compassion. This result has important clinical implications and supports Gilbert’s (2014) view that individuals with high fears in compassion will have difficulty being self-compassionate or bringing loving-kindness to themselves. These results indicate that clinicians should exercise caution when considering the utility of LKM for individuals with high fears of compassion, as much like our study found, the intervention is unlikely to work for these individuals.
The second hypothesis predicted that participants in the LKM condition, compared to the FI condition, would respond to hypothetical conflict situations with less negative emotion, more self-compassionate cognitions, and more likelihood to respond with an attempt to compromise than other socially undesirable reactions. There was no difference between groups on cognitions and interpersonal responses, and the only significant finding from the emotional subscale was anxiety. However, it should be noted that this vignette measure was developed for the current study and has not been validated. A potential reason for the lack of findings on cognitions and interpersonal responses is that we only used a brief LKM, and this may have been ineffective in modifying the views of young adults. Indeed, previous research has found mixed results when using LKM as a single standalone session (Feldman et al. 2010). In addition, the intention of LKM is to wish that self and others flourish and have positive life well-being. This intention of goodwill may not reflect what is required in situations of conflict, rather a compassion-based meditation, one focused on suffering, maybe more appropriate as it recognises the distress and aims to alleviate it, which LKM does not.
Our final hypothesis predicted that initial levels of fear of self-compassion would moderate results, and this was partially supported. This micro-trial found that fear of self-compassion was an important factor when considering using LKM. Young adults with initial low levels of fear of self-compassion scored significantly higher on the SCS after listening to LKM compared to the control condition, whereas there was no difference on the SCS in individuals with high levels of fear of self-compassion. The relation of fear of self-compassion to LKM in isolation has not been previously studied (Galante et al. 2014), but in combination with therapist-based treatment programs it has been shown that people with high levels did not experience increases in self-compassion (Kelly and Cater 2014), and that the intervention lessened that fear of self-compassion (Jazaieri et al. 2013). This suggests that over a longer intervention LKM might be successful at lowering fear of self-compassion, but over a short period, high levels of that fear may preclude participants’ benefitting from it. For small dosage uses of LKM it may be useful to screen out people with high fear of self-compassion, and engage them in an alternative exercise.
The major implication from this experiment is that LKM may have the ability to engage young adults and motivate them to develop self-compassion, thus providing support to trial LKM on a larger scale in a more costly randomized controlled trial design, with a greater dosage (e.g., be able to practice the meditation multiple times over a longer period of time). The relevance of fear of self-compassion to young adult mental health and family conflict suggest that decreasing this fear may be a worthwhile target for future interventions. Although the single standalone LKM intervention tested did not lead to higher levels of self-compassion, this is not surprising, given LKM in a single dosage delivery has mixed outcomes (Boellinghaus et al. 2014). In ideal testing conditions the LKM intervention would be offered to participants to complete multiple times over a period of time, similar to other self-compassion-based interventions (Neff and Germer 2013). However, this study adopted a micro-trial design where the aim is to not bring about full treatment or prevention effects, rather demonstrate initial impact in a cost-effective experiment.
There were several methodological strengths to this study. The first of which was the experimental design that allowed us to compare the effects of the LKM to an active control, rather than waitlist control, or correlation-based studies as most other self-compassion research has done (Yarnell and Neff 2013). The micro-trial design also allowed us to isolate LKM, and also have control over potential confounding factors, such as length of the meditation, the instructors voice, the room and administrator, and the instructions given throughout the experiment. The use of manipulation checks was another methodological strength.
There were several limitations that should be taken into account, and improved upon in future research. First, the majority of participants were females aged 18–19 years, and all were studying undergraduate degrees. This may be problematic when generalizing the results to the entire population of young adults living at home. Second, was the use of a median split to dichotomise fear of self-compassion scores into low and high groups. Such an approach may have sacrificed some of the complexity in the data, which can reduce statistical power (Maxwell and Delaney 1993). Third, the CMS and the Conflict Vignettes were developed for this experiment and have not been psychometrically validated. Finally, the study relied on self-report measures, which are open to possible biases such as demand characteristics and may not reflect actual observed behavior.
Young adulthood is a period of high transition and uncertainty, which can impact on the relationship between young adults with their parents. Self-compassion is a growing field that has been linked to an array of positive mental health outcomes (Barnard and Curry 2011), and may be a strong basis for improving this period of uncertainty for young adults (Neff and Pommier 2012; Yarnell and Neff 2013). This study showed that LKM, a method of increasing self-compassion, may be a potentially useful intervention to help reduce negative emotional reactions in interpersonal interactions with their parents. Future research is needed to target this population and see if increasing self-compassion results in better family and mental health outcomes.
References
Aquilino, W. S. (1997). From adolescent to young adult: A prospective study of parent-child relations during the transition to adulthood. Journal of Marriage and the Family, 59, 670–686. doi:10.2307/353953.
Australian Bureau of Statistics. (2007). National survey of mental health and wellbeing: User’s guide, 2007. Canberra: Australian Bureau of Statistics.
Barnard, L. K., & Curry, J. F. (2011). Self-compassion: Conceptualizations, correlates, & interventions. Review of General Psychology, 15, 289–303. doi:10.1037/a0025754.
Bodhi, B. (1994). The noble eightfold path: Way to the end of suffering. Kandy: Buddhist Publication Society.
Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., et al. (2011). Preliminary psychometric properties of the acceptance and action questionnaire–II: A revised measure of psychological inflexibility and experiential avoidance. Behavior Therapy, 42, 676–688. doi:10.1016/j.beth.2011.03.007.
Boellinghaus, I., Jones, F. W., & Hutton, J. (2014). The role of mindfulness and loving-kindness meditation in cultivating self-compassion and other-focused concern in health care professionals. Mindfulness, 5, 129–138. doi:10.1007/s12671-012-0158-6.
Buddharakkhita, A. (1995). Metta: The philosophy and practice of universal love. Kandy: Buddhist Publication Society.
Carson, J. W., Keefe, F. J., Lynch, T. R., Carson, K. M., Goli, V., Fras, A. M., & Thorp, S. R. (2005). Loving-kindness meditation for chronic low back pain: Results from a pilot trial. Journal of Holistic Nursing, 23, 287–304. doi:10.1177/0898010105277651.
Crane, C., Jandric, D., Barnhofer, T., & Williams, J. M. (2010). Dispositional mindfulness, meditation, and conditional goal setting. Mindfulness, 1, 204–214. doi:10.1007/s12671-010-0029-y.
Dempster, A. P., Laird, N. M., & Rubin, D. B. (1977). Maximum likelihood from incomplete data via the EM algorithm. Journal of the Royal Statistical Society, 39, 1–38. doi:10.1.1.133.4884.
Dubas, J. S., & Petersen, A. C. (1996). Geographical distance from parents and adjustment during adolescence and young adulthood. New Directions for Child and Adolescent Development, 1996, 3–19. doi:10.1002/cd.23219967103.
Embry, D. D., & Biglan, A. (2008). Evidence-based kernels: Fundamental units of behavioural influence. Clinical Child and Family Psychology Review, 11, 75–113. doi:10.1007/s10567-008-0036-x.
Feldman, G., Greeson, J., & Senville, J. (2010). Differential effects of mindful breathing, progressive muscle relaxation, and loving-kindness meditation on decentering and negative reactions to repetitive thoughts. Behaviour Research and Therapy, 48, 1002–1011. doi:10.1016/j.brat.2010.06.006.
Fredrickson, B. L., Cohn, M. A., Coffey, K. A., Pek, J., & Finkel, S. M. (2008). Open hearts build lives: Positive emotions, induced through loving-kindness meditation, build consequential personal resources. Journal of Personality and Social Psychology, 95, 1045–1061. doi:10.1037/a0013262.
Galante, J., Galante, I., Bekkers, M.-J., & Gallacher, J. (2014). Effect of kindness-based meditation on health and well-being: A systematic review and meta-analysis. Journal of Consulting and Clinical Psychology, 82, 1101–1114. doi:10.1037/a0037249.
Germer, C. K. (2009). The mindful path to self-compassion: Freeing yourself from destructive thoughts and emotions. New York, NY: Guilford Press.
Gilbert, P. (2014). The origins and nature of compassion focused therapy. British Journal of Clinical Psychology, 53, 6–41. doi:10.1111/bjc.12043.
Gilbert, P., McEwan, K., Matos, M., & Rivis, A. (2011). Fears of compassion: development of three self-report measures. Psychology and Psychotherapy, 84, 239–255. doi:10.1348/147608310X526511.
Goetz, J. L., Keltner, D., & Simon-Thomas, E. (2010). Compassion: An evolutionary analysis and empirical review. Psychological Bulletin, 136, 351–374. doi:10.1037/a0018807.
Hays, R. D., Hayashi, T., & Stewart, A. L. (1989). A five-item measure of socially desirable response set. Educational and Psychological Measurement, 49, 629–636. doi:10.1177/001316448904900315.
Hofmann, S. G., Grossman, P., & Hinton, D. E. (2011). Loving-kindness and compassion meditation: Potential for psychological interventions. Clinical Psychology Review, 31, 1126–1132. doi:10.1016/j.cpr.2011.07.003.
Howe, G. W., Beach, S. R., & Brody, G. H. (2010). Microtrial methods for translating gene environment dynamics into preventive interventions. Prevention Science, 11, 343–354. doi:10.1007/s11121-010-0177-2.
Hutcherson, C. A., Seppala, E. M., & Gross, J. J. (2008). Loving-kindness meditation increases social connectedness. Emotion, 8, 720–724. doi:10.1037/a0013237.
Jazaieri, H., Jinpa, G. T., McGonigal, K., Rosenberg, E. L., Finkelstein, J., Simon-Thomas, E., et al. (2013). Enhancing compassion: a randomized controlled trial of a compassion cultivation training program. Journal of Happiness Studies, 14, 1113–1126. doi:10.1007/s10902-012-9373-z.
Johnson, D. P., Penn, D. L., Fredrickson, B. L., Kring, A. M., Meyer, P. S., Catalino, L. I., & Brantley, M. (2011). A pilot study of loving-kindness meditation for the negative symptoms of schizophrenia. Schizophrenia Research, 129, 137–140. doi:10.1016/j.schres.2011.02.015.
Kelly, A. C., & Cater, J. C. (2014). Self-compassion training for binge eating disorder: A pilot randomized controlled trial. Psychology & Psychotherapy: Theory, Research and Practice, 88, 285–303. doi:10.1111/papt.12044.
Kessler, R., Bergland, P., Demler, O., Jin, R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62, 593–602. doi:10.1001/archpsyc.62.6.593.
Kirby, J. N. (2016). The role of mindfulness and compassion in enhancing nurturing family environments. Clinical Psychology: Science & Practice, 23, 142–157. doi:10.1111/cpsp.12149.
Law, R. W. (2012). An analogue study of loving-kindness meditation as a buffer against social stress. Dissertation Abstracts International: Section B. Sciences and Engineering, 72(7), 4365.
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behaviour Research and Therapy, 33, 335–343. doi:10.1016/0005-7967(94)00075-U.
Maxwell, S. E., & Delaney, H. D. (1993). Bivariate median splits and spurious statistical significance. Psychological Bulletin, 113, 181–190. doi:10.1037/0033-2909.113.1.181.
May, C. J., Weyker, J., Spengel, S. K., Finkler, L. J., & Hendrix, S. E. (2012). Tracking longitudinal changes in affect and mindfulness caused by concentration and loving-kindness meditation with hierarchical and linear modelling. Mindfulness, 5, 249–258. doi:10.1007/s12671-012-0172-8.
McGorry, P. D. (1996). The centre for young people’s mental health: Blending epidemiology and developmental psychiatry. Australasian Psychiatry, 4, 243–247. doi:10.3109/10398569609080496.
Neff, K. D. (2003). The development and validation of a scale to measure self-compassion. Self and Identity, 2, 223–250. doi:10.1080/15298860309027.
Neff, K. D., & Germer, C. K. (2013). A pilot study and randomized controlled trial of the mindful self‐compassion program. Journal of Clinical Psychology, 69, 28–44. doi:10.1002/jclp.21923.
Neff, K. D., & McGehee, P. (2010). Self-compassion and psychological resilience among adolescents and young adults. Self & Identity, 9, 225–240. doi:10.1080/15298860902979307.
Neff, K. D., & Pommier, E. (2012). The relationship between self-compassion and other-focused concern among college undergraduates, community adults, and practicing meditators. Self and Identity, 12, 160–176. doi:10.1080/15298868.2011.649546.
Pace, T. W., Negi, L. T., Adame, D. D., Cole, S. P., Sivilli, T. I., Brown, T. D., et al. (2009). Effect of compassion meditation on neuroendocrine, innate immune and behavioral responses to psychosocial stress. Psychoneuroendocrinology, 34, 87–98. doi:10.1016/j.psyneuen.2008.08.011.
Rahim, M. A. (1983). A measure of styles of handling interpersonal conflict. Academy of Management Journal, 26, 368–376. doi:10.2307/255985.
Shahar, B., Szsepsenwol, O., Zilcha‐Mano, S., Haim, N., Zamir, O., Levi‐Yeshuvi, S., & Levit‐Binnun, N. (2015). A wait‐list randomized controlled trial of loving‐kindness meditation programme for self‐criticism. Clinical Psychology & Psychotherapy, 22, 346–356. doi:10.1002/cpp.1893.
Shonin, E., Van Gordon, W., Compare, A., Zangeneh, M., & Griffiths, M. D. (2015). Buddhist-derived loving-kindness and compassion meditation for the treatment of psychopathology: A systematic review. Mindfulness, 6, 1161–1180. doi:10.1007/s12671-014-0368-1.
Templeton, J. L. (2007). Expanding circle morality: Believing that all life matters. Dissertation Abstracts International: Section B. Sciences and Engineering, 68(2), 1342.
The Dalai Lama. (2001). An open heart: Practicing compassion in everyday life. Boston, MA: Little Brown and Company.
Wallace, B. A. (1999). The four immeasurables. Cultivating the boundless heart. New York, NY: Snow Lion Publications.
Weston, R., Stanton, D., Qu, L., & Soriano, G. (2001). Australian families in transition: Some socio-demographic trends 1901-2001. Family Matters, 60, 12–23.
White, N. R. (2002). “Not Under My Roof!”: Young people’s experience of home. Youth & Society, 34, 214–231. doi:10.1177/004411802237864.
Yarnell, L. M., & Neff, K. D. (2013). Self-compassion, interpersonal conflict resolutions, and well-being. Self and Identity, 12, 146–159. doi:10.1080/15298868.2011.649545.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
We do not believe we have anything to disclose in relation to this manuscript. However, for full transparency we submit the following disclosure statement. James Kirby is a co-author of the Grandparent Triple P program. The Triple P—Positive Parenting Program is owned by The University of Queensland. The University, through its technology transfer company Uniquest Pty Ltd, has licensed Triple P International Pty Ltd to disseminate the program worldwide. Royalties stemming from this dissemination work are paid to UniQuest, which distributes payments to the University of Queensland Faculty of Social and Behavioural Sciences, School of Psychology, Parenting and Family Support Centre, and contributory authors in accordance with the University’s intellectual property policy. No author has any share or ownership in Triple P International. David Laczko has nothing to declare.
Research Involving Human Participants
The ethical approval for the study was obtained from the University of Queensland
Informed Consent
All participants gave their informed voluntary consent.
Rights and permissions
About this article

Cite this article
Kirby, J.N., Laczko, D. A Randomized Micro-Trial of a Loving-Kindness Meditation for Young Adults Living at Home with their Parents. J Child Fam Stud 26, 1888–1899 (2017). https://doi.org/10.1007/s10826-017-0692-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-017-0692-x