
Abstract
This mixed method study examined factors associated with parents not attending their child’s mental health treatment after initially seeking help for their 2–5 year old child. It was part of a larger study comparing two evidence-based treatments among low-income racial/ethnic minority families seeking child mental health services. Of 123 parents who initiated mental health treatment (71 % African American or multi-racial; 97.6 % low-income), 36 (29.3 %) never attended their child’s first treatment session. Socio-demographic characteristics, parenting stress, depression, severity of child behavior problems, and length of treatment delay from intake to first scheduled treatment session were compared for families who did and did not attend their first treatment session. Parents who never attended their child’s first treatment session were more likely to live with more than four adults and children (p = .007) and have more depressive symptoms (p = .003). Median length of treatment delay was 80 days (IQR = 55) for those who attended and 85 days (IQR = 67.5) for those who did not attend their child’s first treatment session (p = .142). Three themes emerged from caregiver interviews: (a) expectations about the treatment, (b) delays in getting help, and (c) ambivalence about research participation. Findings suggest the need to develop better strategies for addressing risk factors early in the treatment process and reducing the length of time families with adverse psychosocial circumstances must wait for child mental health treatment.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The U.S. Surgeon General’s report brought national attention to the significant disparities in mental health care for underserved ethnic and racial groups (Satcher 2001). Racial, ethnic, and socioeconomic disparities in children’s mental health service use are well documented. Children from low income and historically disadvantaged racial/ethnic populations are less likely than White and middle income children to initiate mental health treatment (Coker et al. 2009). Even among families who initiate a referral for mental health treatment, families from low income and historically underserved populations, i.e., African American and Latino, are less likely to attend their first appointment (Harrison et al. 2004). Recent advances in the development of evidence based parenting intervention programs for parents of children with behavioral problems have not been matched by specific methods for engaging parents, facilitating adherence to treatment, and increasing treatment attendance. Given the complex needs of low income and underserved families who seek mental health and behavioral intervention services, a more comprehensive examination of mental health systems of care, including studies of risk factors associated with lack of treatment initiation and engagement, intake and scheduling systems, and evaluation of strategies to improve access and engagement in mental health services, is of utmost public health importance.
Engagement is defined in the literature as a dynamic process with distinct phases, beginning with identification of the need for treatment through treatment completion or disengagement (Becker et al. 2015; Staudt 2007). McKay and Bannon (2004) delineate three phases of the initial mental health treatment engagement process: (1) recognition by caregivers or other individuals in the child’s life that the child has a mental health problem, (2) connecting the child and family to a mental health treatment agency, and (3) bringing the child to the mental health agency to receive treatment. Given this definition, treatment engagement begins well before families meet the mental health clinician (Staudt et al. 2012). Failure to effectively negotiate this initial mental health treatment engagement process is a significant problem; rates of non-attendance for the first mental health treatment session range from 28 % (McKay et al. 2005) to 62 % (McKay et al. 1996) despite the fact that parents still need and want treatment for their child (Harrison et al. 2004).
Prior research highlights the importance of identifying psychosocial risk factors that may interfere with initial treatment engagement. In addition to perceived parenting skills and severity of child behaviors, factors such as parent characteristics (e.g., mental health, parental competencies, parental attributions and cognitions), social challenges (e.g., socioeconomic status), family factors, cultural practices and other domains impact health decision making (Mendez et al. 2009; Nock and Ferriter 2005). For low income and underserved families, additional social factors such as homelessness, lack of transportation, unemployment, and family-based stressors including domestic violence, parental depression, substance abuse, and traumatic loss, and chronic illness (e.g., asthma, developmental disability) may influence treatment engagement. A consistent finding is that parental socioeconomic disadvantage, being from an underserved racial or ethnic group, single parenthood, and poor parental mental health are associated with reduced likelihood of initiating or completing mental health treatment (Haine-Schlagel and Walsh 2015; Oslin et al. 2006). Indeed, there is a growing population of impoverished families in the United States living on incomes of $2 per person per day (Edin and Schaefer 2015), making it difficult to find stable housing, afford transportation, or feed their children. These social determinants not only increase the need for support and service utilization to promote engagement and attendance at child and parent mental health services, (Acri et al. 2016; Wilcox et al. 2016) but also make those services more challenging to access despite parents feeling motivated to help their children. Examining factors that influence attendance at the child’s first treatment session is particularly important as it may identify remediable treatment barriers for parents who initiated and completed the mental health referral and diagnostic evaluation, yet decided not to pursue treatment.
Fear of stigmatization regarding mental health, as well as uncertainty about what to expect from mental health services have also been identified as barriers to mental health treatment engagement (Lindsey et al. 2013; Thompson et al. 2013). How these factors specifically affect treatment engagement is not well understood. These factors are likely linked to a range of practical (e.g., schedule conflicts, childcare issues, lack of transportation, difficulties juggling competing demands) and perceptual (e.g., stigma, concern that child will be placed on medication, prior negative experienced with mental health care, feeling judged, parents’ thoughts and beliefs about problems and ambivalence to change) barriers (Breland-Noble et al. 2006; Gordon et al. 2010; Larson et al. 2013, Murphy et al. 2012).
Another important barrier to treatment is the length of time families wait for their first scheduled appointment (Westin et al. 2014). Waiting lists are a common agency strategy for managing treatment loads that exceed provider capacities (Brown et al. 2002; McGurran and Noseworthy 2002). Longer delays between intake and the first scheduled appointment, however, are linked to greater odds of patients not showing up for their psychiatric appointment (Ho et al. 2015). Recent data indicate that the average wait time for appointments to see a child mental health provider is approximately 7.5 weeks (Children’s Hospital Association Survey 2012), which can feel like a very long time for a parent in crisis. In fact, patients’ opinions of acceptable wait times are poorly captured in available scheduling assessment tools (Paterson et al. 2006). According to a recent Institute of Medicine (2015a) report, timely access to mental health services continues to be a challenge for many Americans. Organization-specific factors including organizational culture and management also contribute to access difficulties and long wait times.
In the current study, we used a convergent mixed methods design (Creswell and Plano Clark 2010) to examine barriers to first treatment attendance in a predominantly low-income, African American population of parents who initially sought mental health services for their child but did not attend the first treatment session. We interviewed those parents to understand their perspective and identify remediable factors that could strengthen parent engagement in child mental health treatment. Based on the literature describing barriers to mental health treatment engagement faced by families raising young children under adverse psychosocial conditions (i.e., poverty, unemployment, low educational attainment, homelessness, parenting stress, and depression), we examined the impact of barriers on the likelihood of attending their child’s first mental health treatment session. We also examined whether the perceived severity of their children’s behavior problems and the length of time they waited for their first treatment visit were associated with parents choosing not to attend their child’s first treatment. We hypothesized that adverse social determinants and delays in accessing mental health treatment would negatively influence attendance at first treatment visit. We further hypothesized that parents who perceived their child’s behavior problems to be more severe would be more motivated to persevere despite potential barriers and therefore more likely to attend their child’s first treatment session. As the current study is part of a larger trial imbedded within the mental health clinic (Gross et al. 2014), parents were also interviewed about whether aspects of the research protocol may have contributed to their decision to not attend their child’s first treatment session.
Method
Participants
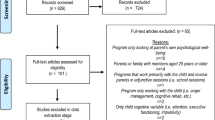
Participants for this study were 123 parents who enrolled between January 2012 and March 2015 in a randomized clinical trial comparing two evidence-based parenting skills training programs at an urban based children’s mental health center (Gross et al. 2014). The center provides mental health services to children who have a history of behavior problems, child maltreatment, neglect, exposure to community violence, homelessness, and caregiver mental health concerns. Parents or legal guardians whose children were between 2 and 5 years of age, who requested treatment for behavior problems were invited to participate in the clinical trial following intake and a diagnostic assessment. The diagnostic assessment interview, which is used to identify the mental health and psychosocial needs of the family, enabled the study team to determine study eligibility. Parents actively involved in a child welfare investigation for maltreatment or who did not speak English were excluded from the study. Parents of children who met eligibility criteria and expressed interest in the study were contacted by a research team member to describe the study and answer questions. Parents were informed that they would be randomly assigned to one of two parenting programs already demonstrated to be effective for reducing behavior problems in young children (see Gross et al. 2014 for more details on the larger study). If parents were interested in participating, a time was scheduled to obtain informed consent and complete baseline parent–child study assessments. None of the parents who expressed interest refused participation. The baseline assessment battery took about 90 min to complete and parents received $30 and a children’s book as compensation for their time. Following consent and completion of the baseline study assessments, parents were scheduled for their child’s first treatment session. If the family was placed on the wait list to start treatment, clinicians at the center phoned parents weekly to assess risk and help parents stay connected. All families living within a 20-mile radius of the mental health center received free cab services, if needed, to attend treatment sessions.
Typical of the mental health center’s patient population, most of the parents enrolled were African American or multi-racial (n = 87; 70.7 %), unemployed (n = 89; 72.9 %), and economically disadvantaged (n = 116; 94.5 % received Medicaid or reported annual incomes less than $20,000). Most families (n = 96; 78.0 %) were self-referred to the child mental health center. Primary diagnoses were Adjustment Disorder (n = 63; 51.2 %), Disruptive Behavior Disorder (n = 18; 14.6 %), Attention Deficit/Hyperactivity Disorder (n = 17; 13.8 %), Oppositional Defiant/Conduct Disorders (n = 12; 9.8 %), Post-traumatic Stress Disorder (n = 10, 8.13 %), and Separation Anxiety (n = 3, 2.4 %).
Of the 123 parents who enrolled in the clinical trial and completed the baseline assessment battery, 29.3 % (n = 36) never attended their child’s first mental health treatment session. In 2015, we attempted to contact all 36 parents to determine their interest in being interviewed by phone about their reasons for not continuing to pursue treatment for their child at the clinic. The current study was approved by the Johns Hopkins Medical Institutions-Institutional Review Board.
Procedure
A convergent mixed method research design (Creswell and Plano Clark 2010) was employed to address objective and subjective barriers to parents attending their child’s first mental health treatment session. For the quantitative strand, we examined the associations among socio-demographic and psychosocial risk, parent stress, severity of child’s behavior problems, length of treatment delay, and likelihood of the parent attending the child’s first mental health treatment session. For the qualitative strand, we interviewed only those parents who did not attend their child’s first mental health treatment session to understand their perspectives on why they did not bring their child back for treatment. Phone interviews were conducted by one research team member using questions described in Table 1. To increase comfort and disclosure, interviews were not audio recorded and abridged transcripts collected from the phone interviews were used for the data analysis. Qualitative software was not utilized. Each phone interview was about 30-min long. Responses on the Interview guide domains and questions were reviewed on the phone with the participants and quotations were selected from the interview scripts to illustrate the participants lived experiences. The semi-structured interviews sought to understand (a) the parent’s reasons for initially seeking treatment, (b) perceptions of barriers to treatment, (c) experience with the research evaluation, (d) reason(s) for ending treatment, and (e) whether they were still interested in receiving treatment for their child. The purpose of the interview was to identify factors leading to the parent’s decision not to pursue treatment. The long term goal was to use these data to develop more effective strategies to engage parents in their child’s treatment and in research. Qualitative data analysis strategy is described in detail below.
Measures
We examined several indicators of child, parent, and psychosocial risk previously found to predict non-attendance as well the length of treatment delay. These include severity of child behavior problems, parenting stress, parent depression, and history of social adversity. All parent and child data used in this study were collected from the parent at baseline. Below is a brief description of the variables and measures used in this study.
Parental Reports of Child Internalizing and Externalizing Symptoms
Child behavior problems were measured using the Child Behavior Checklist 1½-5 (CBCL). The CBCL is a well-validated 99-item measure of parent’s report of their young child’s externalizing and internalizing behavior problems (Achenbach and Rescorla 2000). Reliabilities for the externalizing scale range from .88 to .91 and from .77 to .81 for the internalizing scale (Gross et al. 2006). For the current sample, alpha reliabilities were .91 for the externalizing and .85 for the internalizing scales.
Parenting Stress
Parenting stress was measured using the Parenting Stress Index Short Form (PSI-SF) (Abidin 1995). Previous research supported the validity of this shorter 36-item version of the PSI among parents from lower socioeconomic backgrounds (Reitman et al. 2002). In the current study, alpha reliability for the PSI total scale was .86.
Parental Depressive Symptoms
The 20-item Center for Epidemiologic Studies Depression Scale-Revised (CESDR) was used to measure symptoms of parental depression. The validity of the CESDR was determined by confirmatory factor analyses and significant associations with other measures of depression (Van Dam and Earleywine 2011). CESDR scores were analyzed as a continuous score (i.e., severity of depressive symptoms) and as a dichotomous score (i.e., depressive symptoms exceeding the clinical cut point of 16 or higher). Alpha reliability for the total CESDR scale in the current sample was .92.
Socio-demographic Dackground and Psychosocial Adversity
Demographic information was collected on the Family Demographic Sheet and included questions about the parent’s race, ethnicity, age, gender, education level, employment status, income level, and marital status. Based on the work by Popp et al. (2008), we created a social risk index to collect information on 11 indicators of family social adversity. These 11 indicators (coded yes/no) included whether parent had less than a high school education, was currently unemployed, reported an annual family income less than $20,000 or was receiving Medicaid, was living with more than four adults and children, had more than three children living in the home, had a history of homelessness, was less than 20 years old, was less than 20 years old at the birth of their first child, had a history of substance use, had a history of domestic violence, and had a baseline CESDR score of 16 or higher. These social risk indicators were analyzed separately to better understand which risks in this vulnerable population were associated with initial treatment engagement.
Length of Treatment Delay
Length of treatment delay was calculated as number of days between the intake appointment date and the date of their first scheduled treatment session, regardless of whether the family showed for that first scheduled treatment session.
Data Analyses
Participants’ demographic and psychosocial characteristics were summarized using means (SD) and medians (IQR) for continuous variables and frequencies and percent for categorical variables. The study sample was divided into two groups. Group 1 consisted of participants who attended their child’s first treatment visit (n = 87), and Group 2 included participants who did not attend the first treatment visit (n = 36). We compared the two groups to assess whether parents who never attended their child’s first treatment session differed from those who did attend on socio-demographic background, psychosocial adversity, length of treatment delay, parenting stress, and severity of child behavior problems. χ 2 test was used for categorical data, and if expected frequency per cell was <5 a Fisher’s exact test was used. For continuous variables, the groups were compared using a Wilcoxon rank-sum test as distribution was skewed for all of the variables.
Qualitative Analyses
Husserl asserted that everyone’s experiences of things are different and should be studied as they happen in the person’s real world—going “back to the things themselves” (Husserl 1900/1970, p. 252). Thus, qualitative phenomenological approach was used to understand the lived experience of parents who sought mental health treatment for their children but did not attend their child first treatment session. The qualitative data analysis was guided by Giorgi and Giorgi’s (2003) four basic steps of descriptive phenomenological method. The first analysis step involves initial read and re-read of all interview transcripts to gain a holistic view of the experiences of the parents. The second step involves identification of the meaning units and themes and assignment of codes to the identified meaning units. The third step involves the re-read of the identified meaning units to uncover the hidden meanings and transform them into psychological relevant concepts to arrive at each parent’s essence of the experience. In the final step, the insights contained in each parent’s essence were synthesized and integrated into a consistent statement or structure to capture the meaning of the lived experience described by the parents. Two research team members independently coded the transcripts for themes and then compared them for consistency of interpretation. Disagreements were managed through consensus.
Results
Socio-Demographic and Psychosocial Adversity by Attendance at First Treatment Session
Of the 123 parents who initiated mental health treatment for their children, 36 (29.3 %) never attended their child’s first mental health treatment session. Tables 2 and 3 present socio-demographic data for the parents and children in the sample, respectively. As shown in Table 2, parents who did not attend were younger (Mdn = 28.5, IQR = 11.5) than those who did attend (Mdn = 34, IQR = 15; p = 0.005) their child’s first treatment session. No differences were found between those who did and did not attend their child’s first treatment session on parent or child race/ethnicity; marital status, child sex, child age, child’s primary diagnosis, or referral source.
We hypothesized that adverse social determinants would negatively influence attendance at first treatment session. As shown in Table 4, parents who did not attend their child’s first treatment session were more likely to live with more than four people in the home (n = 21; 58.3 %) compared to those who did attend (n = 28; 32.2 %) (p = 0.007). No differences were found between those who did and did not attend their child’s first treatment session on parent education; having more than three children in the home; a history of substance use, homelessness, domestic violence; or annual household income less than $20,000 or receiving Medicaid.
Nearly 46 % (n = 56) of the sample had depression scores exceeding the clinical cutoff score of 15. Parents who did not attend their child’s first treatment session were more likely to exceed this score at baseline (n = 22; 61.1 %) compared to those who did attend (n = 34; 39.1 %) (p = .026). Median depression scores were also higher among parents who did not attend treatment (Mdn = 21.5, IQR = 25) relative to those who did attend (Mdn = 13, IQR = 18; p = 0.003). Contrary to hypotheses, parenting stress and severity of the child’s internalizing or externalizing behavior problems did not differentiate those who did and did not attend their child’s first treatment session (see Table 5).
Length of Treatment Delay
As shown in Table 5, median number of days between the parents’ initial intake appointment and their child’s first scheduled mental health treatment visit was 80 days (IQR = 55, range 20–442 days) for those who attended their first treatment session and 85 days (IQR = 67.5, range 31–386 days) for those who never attended. The distribution of treatment delay between the two groups was not significantly different (p = 0.142). We compared the treatment delay non-parametrically using a Wilcoxon rank-sum test, because the variable showed skewness as some parents waited for a long time to start the treatment. For example, approximately 8 % in the “never attended group” and 3 % in the “attended group” waited six months or longer for their first scheduled treatment session; however, the difference was not statistically significant (p = 0.357).
Qualitative Analyses
Of the 36 parents who did not attend their child’s first treatment session, 19 (53 %) were reached by phone and agreed to be interviewed for this study. None refused to be interviewed. Parents not reached for interview were more likely to have a history of homelessness (n = 9; 52.9 %) compared to those interviewed (n = 1; 5.3 %) (p = 0.002). There were no other socio-demographic differences between those who were and were not reached for interview. Moreover, no differences in baseline depression, parenting stress, or child behavior problem scores were found between those who were and were not reached for interview. These results suggest that those parents interviewed were comparable to those who were not.
Three super-ordinate themes emerged from the study’s qualitative analysis and include (a) immediate treatment needs, (b) perceived barriers to treatment, and (c) mixed feelings about research participation. Each of these themes are described below and listed in Table 6.
Immediate Treatment Needs: Aspects of Behavior that Motivated Parents to Seek Treatment for their Children
The theme of “immediate treatment needs” describes aspects of behavior that motivated parents to seek treatment for their children. There were six sub-themes within this theme and include: “problem awareness”, “seeking treatment out of desperation”, “having no other option”, “feeling overwhelmed”, “looking for an answer”, and “needing help now”. These sub-themes reflected some of the intrinsic motivators towards parents’ mental health help-seeking for their children. All of the parents in the study reported that they sought help because they knew something was not right—“problem awareness” and they needed to know what was wrong with their child. “Seeking treatment out of desperation” was exemplified by one parent reflection, “I don’t want him to be kicked out of daycare”. Twenty-one percent of the parents reported seeking help to look for an answer to their child’s behavior problem after they had “tried everything but nothing worked”. There was an expectation of quick results when parents felt overwhelmed with their children’s behavior problems; 89 % of the parents reported wanting to be helped right away, “needing help now”. One parent, who had waited about 5 months for their first scheduled appointment shared, “When people seek help, they want it now”.
Perceived barriers to treatment: parents perspectives about why they did not continue with treatment
This theme described parents’ perspectives about why they did not continue with treatment and included those circumstances that are considered to be outside the control of parents. Within the theme of “perception of barriers to treatment”, there were seven sub-themes: “long wait time”, “scheduling conflict/appointment availability”, “competing demands and level of adversity”, “loss of contact/unable to reach”, “service location”, “concern that diagnosis will follow child”, and “unmet service needs”.
Treatment delay was a common experience described in the interviews; 95 % of the parents cited long wait time as one barrier to their treatment engagement. One parent, who waited for 49 days, described her experience as “He is acting out and I can’t get the help I needed right then”. Another parent, who waited for 63 days, shared, “I called because I need help with my child’s behavior and it took so long that I actually forgot that I called”. Sixteen percent of the parents reported that they lost contact with the center. As one parent, who waited for 103 days, reflected, “I was hoping to get help for my child but no one called me”. Parents reported waiting to be contacted and gave up when no one called them back. One parent reflected, “I got sick and then I went through my own depression and then one thing after another and I couldn’t commit to come”. Some of the parents in this study shared that they could not reach the center or be reached by the center staff to reschedule their first treatment appointment because their phone was off or their phone number had changed. One parent reported that “I was in the process of moving and looking for a new job”. Another parent shared that “I had a lot going on” and another, “I started a work program”.
“Scheduling conflict and availability of appointments” were also reported as barriers affecting parents’ decision to participate in treatment. Scheduling conflicts and dissatisfaction with the appointment times offered were reported by 68 % of the parents. Dissatisfaction of the appointment times were characterized by lack of evening and weekend appointments as well as parents and clinicians not having flexible work hours. Competing work and domestic demands as well as the ability to make the time commitment were identified as barriers to help seeking by 32 % of the parents. One parent shared “the timing was a problem. I can’t take off work once a week to come to therapy” and “they did not have weekends or late evening hours”. Another parent shared that “the time of the appointment was not good for me. If you all have evening hours, it would have been good”.
“Unmet service needs” were reflected in one parents’ story of how her child’s problems ultimately resolved on their own following about 5 months delay in getting treatment: “I called because he was acting out. I think it is the age thing, he is older now and is doing fine”. This unmet need and resolution of the problem without intervention may reflect that parents often seek help in time of crisis and may discontinue treatment once the crisis subsides. The theme of “service location” reflected the difficulties caused by geographical distance and the burden of travel time on parents who are seeking mental health treatment for their children. Eleven percent of the parents shared that they had “moved out of the area” and with limited economic resources, they were unable to get to the clinic.
The theme of “concern that diagnosis will follow child” reflected some parents’ concerns about the stigma of their child receiving a psychiatric diagnosis. As one parents stated, “I’m worried that the diagnosis will follow him and I don’t want that”. It is possible that the length of time between the intake appointment and initiating treatment allowed more time for parents to reflect on this problem before having the opportunity to engage in a trusting relationship with a mental health provider who might have alleviated the concern. Eleven percent of the parents interviewed reported that they received the services they needed elsewhere. None of the parents interviewed expressed that they were still trying to find help for their child.
Mixed Feelings on Research Participation: Willingness to Participate in Research yet Uncomfortable with the Evaluation
This theme reflected parents’ reactions to participating in a research study that focused on early parenting. This study is part of a larger trial that required participants to complete surveys about their parenting skills, their own mental health, and their child’s behavior and to be video recorded interacting with their child during a free-play and clean-up session. This assessment battery took approximately 90 min to complete. We therefore asked parents about their experiences with the research evaluation to determine whether aspects of the research assessments may have contributed to their decision to not attend their child’s first treatment session.
There were five sub-themes within the theme of “mixed feelings on research participation” including those reflecting positive (“desire to learn and help others”, “increase personal insight”) and negative (“feeling judged”, “feeling uncomfortable”, “too much personal questions”, and “concern that study will follow child”) experiences. Over half (53 %) of the parents interviewed reported mixed feelings about their research participation. Eleven percent of the parents wanted to participate in the study and “had no problem with being in the study”. One of the parents reflected that understanding what works comes from exploring—“I’m okay with it because it is research and people learn from doing research”. The theme of “increased personal insight” reflected personal benefits associated with participating in research evaluation. Twenty-one percent of the parents ascribed their participation in the research evaluation with positive and meaningful benefits and their reports include “the questions made me think about my own behaviors”, “I still remember the questions, they make you think”, “I like the questions, it made me think about things I don’t really think about”.
However, participation in the research evaluations was not a universally positive experience. The following themes, “feeling judged”, “feeling uncomfortable”, and “too much personal questions”, reflect that rating ones behavior can cause feelings of discomfort and sharing personal information and being observed can be difficult. These feelings of discomfort may be particularly heightened when parents worry that they are being blamed for their children’s problems. One parent described her experience as “I felt the study was for me and not my child. The questions were in-depth for me. The video was not natural because others kids and people were not around. It would be nice if you video him in the waiting room and watch how he interacts with other kids”. Twenty-six percent of the parents reflected on their discomfort with the evaluation: “It was a little awkward for me. It was a little uncomfortable. I feel like am being graded or judged. It made me nervous”. “I was fine with it. The video part was a little uncomfortable. It was weird for me to be there and pretend not to be there”.
Discussion
This study is one of the few to use a mixed methods approach to identify barriers to initial treatment engagement in a highly vulnerable population of parents seeking mental health treatment for their young children. Although prior research has consistently shown that high levels of social adversity are associated with decreased odds of engaging in mental health treatment (Haine-Schlagel and Walsh 2015; Oslin et al. 2006), those results do not advance our understanding of what parents endure in trying to access mental health services for their child. Indeed, most of the parents in this study were single and unemployed, many had histories of homelessness and substance use, and nearly 46 % had high levels of depressive symptoms. Yet all had recognized the need for help and initiated mental health services for their child. The results of this study sought to deepen our understanding of how social and psychological adversities may contribute to barriers they experienced obtaining mental health services for their young children with behavior problems.
Younger parent age, higher levels of depressive symptoms, and living with more than four adults and children in the home were found to differentiate those who did and not did attend their child’s first treatment session. The finding of more depressive symptoms among parents who did not continue pursuing mental health treatment for their child is consistent with previous findings (Davis et al. 2015; Harrison et al. 2004; Pawlby et al. 2011). Depression can make it more difficult to maintain a schedule and manage multiple competing demands. Depression can also contribute to a sense of helplessness and hopelessness managing difficult child behavior. Many of the parents interviewed described feeling overwhelmed and desperate by the time they sought treatment for their child’s problems. It is interesting to note that higher parenting stress scores did not significantly differentiate parents who did and did not attend their child’s first treatment session, suggesting that parents’ feelings of hopeless and helplessness that typically accompany depression may have been important barriers for these parents.
Younger parents were less likely to attend the first treatment session. Younger parents may have fewer resources to manage multiple demands and follow through on treatment attendance for their child. Other studies have also found significant associations between treatment engagement and younger parent age (Haine-Schlagel and Walsh 2015).
Although having more children in the home did not discriminate those who did and did not attend treatment, living with more than four people did affect attendance at the first treatment appointment. Nearly 95 % of the sample was living in poverty. In order to make ends meet, many urban poor families merge households with other family members to share the costs of rent and utilities (Edin and Schaefer 2015). This can lead to overcrowding and complex family lives that can make life and parenting more challenging. As one parent reflected, “I had a lot going on”. Multi-family living may also be more common among younger parents, another variable found to differentiate those who did and did not attend treatment. As this is the first study to find that living with more than four people in the home affected initial treatment engagement in child mental health services, more research is needed. Future studies should include more detail on size of the living space, number of people per bedroom, household composition, housing stability, and mental health problems evident among others living in the home to better understand the impact of housing conditions on parent engagement in child mental health services.
It is not clear why attendance at the first treatment session did not vary by parent education, histories of homelessness, substance abuse, or domestic violence; or having an annual include less than $20,000 or receiving Medicaid. It is possible that the finding was related to limited variability in the sample (i.e., most of the families had low incomes and limited education) or the measures (i.e., the binary scales used to assess histories of homelessness, substance abuse, and domestic violence failed to capture important qualities of these experiences that affect parent well-being).
All parents had lengthy waits between their intake appointment and their child’s first scheduled treatment session, averaging nearly 3 months. Although the delay was longer for those who never attended their child’s first treatment session, the difference was not statistically significant. Nonetheless, long waiting time was a consistent theme that emerged from the qualitative analysis and was cited as a reason for dropping out of treatment. As one parent who waited 147 days to begin treatment commented, “It took forever to get in. When people seek help, they want it now”. These parents showed a high levels of readiness to engage in treatment for their children. However, the longer that the parent waits to receive help, the greater the potential that their level of readiness will dissipate, especially if they are struggling with depression. One parent, who waited 49 days, advised “Don’t let parents wait for too long. I made the decision to stop coming”.
Many factors contribute to long treatment wait times, including competing demands, parents and clinicians not having flexible work hours, clinic hours that are primarily available during parents’ regular work hours, shortages in mental health providers, parents’ disconnected phone numbers, changes in parents’ job schedules, chaotic living situations, and health insurance status. Clinic hours may be a particularly significant barrier to attendance for working poor parents who have limited control over their work schedules.
Delays in getting treatment from mental health care providers may lead to increased use of primary care providers’ care. According to Anderson et al. (2015), a greater proportion of US children and youth receive mental health treatment from their primary care providers compared to psychiatrists, psychologists, or social workers. This trend may reflect the shortage of mental health providers and parents’ need to get help quickly for their children’s needs. Parents may be more motivated to invest time, energy, and resources into treatment when they are provided with an action plan early in treatment. Therefore, clinicians involved in the initial evaluation of the child’s mental health needs should consider providing parents with feedback that encourages an understanding of the child’s treatment needs.
Findings from the current study are consistent with previous studies that point to several barriers to engaging underserved families and children in mental health treatment including level of social adversity, fear of stigma, and needing help but not knowing what to expect (Becker et al. 2015; Lindsey et al. 2013). Parent depression, which is associated with less optimal parenting skills and child outcomes (Davis et al. 2015; Pawlby et al. 2011; Hay et al. 2008), has also been linked to histories of violence and maltreatment during the parent’s childhood (Ammerman et al. 2016; Hodgkinson et al. 2014). Findings from this study underscore the role of social adversity and parental depression as risk factors that may make it more difficult for parents to successfully engage in their child’s mental health treatment without first getting their own mental health needs met. Parents who face social adversity frequently have limited resources and social supports to cope with their children’s behavior problems (Harrison et al. 2004).
A number of effective strategies for engaging underserved families and children in mental health treatment have been identified in the literature (Becker et al. 2015; Gopalan et al. 2010; Lindsey et al. 2013; Nock and Kazdin 2005). Assessment, accessibility promotion, psychoeducation about services, homework assignment, and appointment reminders have been cited as the most frequently identified engagement practice elements associated with effective engagement outcomes with assessment and accessibility as the two most prevalent engagement practice elements used among engagement randomized controlled trials (Lindsey et al. 2014; Nock and Kazdin 2005). Moreover, Becker et al. (2015) found that certain engagement practices are differentially associated with attendance, participation, and attitude, suggesting that engagement procedures can be strategically applied to enhance engagement. Practices such as increasing timely access to mental health services by addressing long wait time, exploring and discussing possible barriers to treatment with families early in treatment have been shown to promote treatment attendance and participation (Ingoldsby 2010). A parents’ comment of “having no other option” may reflect the limited social support networks that parents who did not engage in mental health services for their children could rely on. The decision to seek outside help comes only after one “tried everything but nothing worked”. Collaborative care, clinicians and parents working together to address the child’s mental health needs, may be efficacious for improving engagement among underserved families (Ell et al. 2010). Mental health clinics and clinicians should consider collaborative treatment services approaches that support interpersonal openness and disclosure among parents.
Parents “feeling overwhelmed” may also reflect the challenge of balancing the many responsibilities associated with depression, complex home environments, and other social factors faced by parents living in urban low-income communities. Competing demands, parent strain, and depleted resources may impact parent engagement when parents have to wait for help (Haine-Schlagel and Walsh 2015). Negative life events such as loss and other traumatic events in the context of the home, school, and community may further complicate family situations and increase child behavior and mental health problems (Ofonedu et al. 2013) leading to parents feelings overwhelmed. Feeling overwhelmed and failing to successfully manage their child’s behavior may lower parental confidence. The parent feels alone and unsupported in the quest to find help to address the child’s behavior problems. Guilt about the problems reported and fear of diagnosis following their children for the rest of their lives may also serve as reasons for lack of willingness to continue with research and treatment (Dempster et al. 2013).
A “desire to learn and help others” expressed by parents suggests that underserved low-income parents are willing to participate in parenting intervention clinical trials. The parents’ responses to questions related to their research experience suggest that overall researchers are making progress in ensuring that evaluation measures are appropriate for the population and that research participants living in urban areas feel well informed about the research study following the consent process.
Some of the interviewed parents, however, expressed themes of “feeling judged”, “feeling uncomfortable”, and “too much personal questions”, reflecting a concern about the research evaluation measures, many of which focused on the parent. Child mental health researchers should consider the impact of adding multiple assessments that focus on the parent and qualities of the parent–child relationship as they may contribute to parents feeling judged and blamed. Adding an explanation to parents about the relevance of these assessments for guiding treatment may reduce parents’ discomfort with their use.
Findings from the quantitative data and qualitative interviews provide insight into the central predictors of treatment engagement and attendance. Parental depression and social adversity are prevalent factors identified with failure to attend their child’s initial treatment session. Previous studies reported high rates of depression among mothers bringing their children to a mental health clinic for evaluation and treatment and maternal depression is associated with poor treatment outcomes in children (Swartz et al. 2005, 2006). Children’s mental health services should consider a two-generation approach, supporting children, parents, and families (Institute of Medicine 2015a, b) because successful treatment of maternal depression has been associated with improved mental health outcomes of their mother’s offspring (Weissman et al. 2006). Characteristics of the parents seeking mental health treatment for their children should be assessed and addressed, as necessary, early in treatment. Exploring and addressing parental depression early in treatment may facilitate treatment engagement, participation, and adherence. Child focused mental health may benefit from taking a family-centered approach, providing mental health services addressing parents’ and child’s mental health and well-being. Parents’ increased awareness of their child’s behavior problems together with the mental health clinics ability to address the presenting problems in a timely fashion may lead to increased engagement in child mental health treatment. Given the impact of wait times on treatment attendance and engagement, strategies to increase the number of mental health providers, including those from culturally diverse backgrounds, and expand the hours of clinic operation may result in reduced wait times. Implementing flexible appointment hours to improve treatment access and attendance in child mental health treatment is essential. Pre-waitlist strategies (e.g., centralized intake process, triage incorporated into the intake process for prioritization of cases by clinical severity) are among the strategies used by agencies and found to demonstrate significant reductions in wait times and missed appointments (Clemente et al. 2006; Williams et al. 2008). Other strategies may include providing immediate intervention services during assessment and prior to treatment, weekly monitoring of children and families on the waitlist, collaboration with other providers and agencies, and utilization of clinical pathways (Ingoldsby 2010). Initial intensive phone session that addressed practical and psychological barriers to treatment was associated with higher rates of attendance at a first treatment appointment among underserved inner-city families and children (McKay et al. 1996). Culturally relevant care and communication can increase parents motivation and engagement in treatment, improve quality of care and positive treatment outcomes. Given that parents may feel that diagnostic labels such as attention deficit hyperactivity disorder and post-traumatic stress syndrome are stigmatizing (Dempster et al. 2015, 2013), providing parent education about the benefits of early diagnosis and answering parent’s questions may help with treatment engagement and reduce attrition. Treatment screening questionnaires that are not culturally relevant may be inadequate for assessing cultural factors that influence the mental health of underserved ethnic families and children. Also, care should be taken when selecting research questionnaires to ensure questions are culturally relevant and thoughtfully administered to elicit valid responses that will inform study conclusion.
Limitations
This study has some limitations. First, some of the parents interviewed had initially sought treatment for their child as part of the larger study initiated over 2 years earlier. Given the length of time between the last parent contact and the interview, recall bias may have affected their responses. In addition, almost half of the parents who failed to attend their child’s first treatment could not be contacted for interview. The use of abridged transcript collected from the phone interviews for the data analysis may have resulted to important qualitative information lost. Although few differences were found between those reached and not reached for interview, qualitative results may have been different if those parents’ perspectives had been included in the study. Finally, generalizability is limited given the small sample size and the focus on families from a single urban mental health clinic.
Eliciting parents’ opinions about barriers to treatment is an important step in addressing treatment engagement in underserved populations. Comprehensive family-based mental health services, in clinics that have flexible hours and limited wait times, may be necessary to improve engagement and attendance in children’s mental health treatment. Findings suggest the need to develop strategies aimed at targeting engagement early and throughout the treatment process for younger parents and families with a history of parental depression, poverty, and increased household occupancy. Studies examining mental health treatment engagement for young children, parental risk factors, and research acceptability for urban underserved populations are of critical importance to reduce health disparities.
References
Abidin, R. (1995). Parenting stress index: Professional manual. 3rd edn. Odessa, FL: Psychological Assessment Resources.
Achenbach, T. M., & Rescorla, L. A. (2000). Manual for the ASEBA preschool forms & profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, and Families.
Acri, M. C., Bornheimer, L. A., O’Brien, K., Sezer, S., Little, V., Cleek, A. F., & McKay, M. M. (2016). A model of integrated health care in a poverty-impacted community in New York City: Importance of early detection and addressing potential barriers to intervention implementation. Social Work in Health Care, 55(4), 314–327. doi:10.1080/00981389.2015.1137256.
Ammerman, R. T., Peugh, J. L., Teeters, A. R., Putnam, F. W., & Van Ginkel, J. B. (2016). Child maltreatment history and response to CBT treatment in depressed mothers participating in home visiting. Journal of Interpersonal Violence, 31(5), 774–791. doi:10.1177/0886260514556769.
Anderson, L. E., Chen, M. L., Perrin, J. M., & Cleave, J. V. (2015). Outpatient visit and medication prescribing for US children with mental health conditions. Journal of the American Academy of Pediatrics. doi:10.1542/peds.2015-0807.
Becker, K. D., Lee, B. R., Daleiden, E. L., Lindsey, M., Brandt, N. E., & Chorpita, B. F. (2015). The common elements of engagement in children’s mental health services: Which elements for which outcomes? Journal of Clinical Child and Adolescent Psychology, 44(1), 30–43. doi:10.1080/15374416.2013.814543.
Breland-Noble, A. M., Bell, C., & Nicolas, G. (2006). Family first: The development of an evidence-based family intervention for increasing participation in psychiatric clinical care research in depressed African American adolescents. Family Process, 45, 153–169.
Brown, S., Parker, J., & Godding, P. (2002). Administrative, clinical and ethical issues surrounding the use of waiting lists in the delivery of mental health services. Journal of Behavioral Health Services & Research, 29, 217–228.
Children’s Hospital Association Survey (2012). Pediatric specialist physician shortages affect access to care. https://www.childrenshospitals.org/issues-andadvocacy/graduate-medical-education/fact-sheets/2012/pediatric-specialistphysicianshortages-affect-access-to-care.
Clemente, C., McGrath, R., Stevenson, C., & Barnes, J. (2006). Evaluation of a waiting list initiative in a child and adolescent mental health service. Child and Adolescent Mental Health, 11(2), 98–103.
Coker, A. D., Huang, H., & Kashubeck-West, S. (2009). Research with African Americans: Lessons learned about recruiting African American women. Journal of Multicultural Counseling and Development, 37(3), 153–165. doi:10.1002/j.2161-1912.2009.tb00099.x.
Creswell, J. W., & Plano Clark, V. L. (2010). Designing and conducting mixed methods research. 2nd edn. Thousand Oaks, CA: Sage Publications.
Davis, D. W., Myers, J., Logsdon, M. C., & Bauer, N. S. (2015). The relationship among caregiver depressive symptoms, parenting behavior, and family-centered care. Journal of Pediatric Health Care. doi:10.1016/j.pedhc.2015.06.004.
Dempster, R., Davis, D. W., Faye Jones, V., Keating, A., & Wildman, B. (2015). The role of stigma in parental help-seeking for perceived child behavior problems in urban, low-income African American parents. Journal of Clinical Psychology in Medical Settings. doi:10.1007/s10880-015-9433-8.
Dempster, R., Wildman, B., & Keating, A. (2013). The role of stigma in parental help-seeking for child behavior problems. Journal of Clinical Child and Adolescent Psychology, 42, 56–67.
Edin, K. J., & Schaefer, H. L. (2015). $2.00 a day: Living on almost nothing in America. New York: Houghton Mifflin Harcourt Publishing Company.
Ell, K., Katon, W., Xie, B., Lee, P. J., Kapetanovic, S., Guterman, J., & Chou, C. P. (2010). Collaborative care management of major depression among low-income, predominantly Hispanic subjects with diabetes: A randomized controlled trial. Diabetes Care, 33, 706–713.
Giorgi, A., & Giorgi, B. (2003). The descriptive phenomenological psychological method. In P. M. Camic, J. E. Rhodes, & L. Yardley (Eds.), Qualitative research in psychology: Expanding perspectives in methodology and design (pp. 243–273). Washington, DC: American Psychological Association.
Gopalan, G., Goldstein, L., Klingenstein, K., Sicher, C., Blake, C., & McKay, M. M. (2010). Engaging families in child mental health treatment: Updates and special considerations. Journal of the Canadian Academy of Child & Adolescent Psychiatry, 19(3), 182–196.
Gordon, M., Antshel, K. M., Lewandowski, L., & Seigers, D. (2010). Predictors of missed appointments over the course of child mental health treatment. Psychiatric Services, 61(7), 657–659.
Gross, D. A., Belcher, H. M. E., Ofonedu, M. E., Breitenstein, S., Frick, K. D., & Budhathoki, C. (2014). Study protocol for a comparative effectiveness trial of two parent training programs in a fee-for-service mental health clinic: Can we improve mental health services to low-income families? Trials, 15, 70 doi:10.1186/1745-6215-15-70.
Gross, D., Fogg, L., Young, M., Ridge, A., Cowell, J. M., Richardson, R., & Sivan, A. (2006). The equivalence of the child behavior checklist/1½ across parent race/ethnicity, income level, and language. Psychological Assessment, 18(3), 313–323.
Haine-Schlagel, R., & Walsh, N. E. (2015). A review of parent participate engagement in child and family mental health treatment. Clinical Child and Family Psychological Review, 18, 133–150.
Harrison, M. E., McKay, M. M., & Bannon, W. J. (2004). Inner-city child mental health service use: The real question is why youth and families do not use services. Community Mental Health Journal, 40(2), 119–131. doi:10.1023/B:COMH.0000022732.80714.8b.
Hay, D. F., Pawlby, S., Waters, C. S., & Sharp, D. (2008). Antepartum and postpartum exposure to maternal depression: Different effects on different adolescent outcomes. Journal of Child Psychology and Psychiatry, 49(10), 1079–1088.
Ho, C. P., Zinski, A., Fogger, S. A., Peters, J. D., Westfall, A. O., Mugavero, M. J., Lawrence, S. T., et al. (2015). Factors associated with missed psychiatry visits in an urban HIV clinic. AIDS and Behavior, 19(8), 1423–1429.
Hodgkinson, S., Beers, L., Southammakosane, C., & Lewin, A. (2014). Addressing the mental health needs of pregnant and parenting adolescents. Pediatrics, 133(1), 114–122. doi:10.1542/peds.2013-0927.
Husserl, E. (1900/1970). Logical Investigation (trans: Findlay, J. N.). New York: Humanities Press.
Ingoldsby, E. M. (2010). Review of interventions to improve family engagement and retention in parent and child mental health programs. Journal of Child and Family Studies, 19, 629–645.
Institute of Medicine. (2015a). Transforming health care scheduling and access: getting to now. Washington, DC: National Academy Press.
Institute of Medicine. (2015b). Opportunities to promote children’s behavioral health: Health care reform and beyond. Washington, DC: National Academy Press.
Larson, J., dosReis, S., Stewart, M., Kushner, R., Frosch, E., & Solomon, B. (2013). Barriers to mental health care for urban, lower income families referred from pediatric primary care. Administration and Policy in Mental Health and Mental Health Services Research, 40, 159–167.
Lindsey, M. A., Brandt, N. E., Becker, K. D., Lee, B. R., Barth, R. P., Daleiden, E. L., & Chorpita, B. F. (2014). Identifying the common elements of treatment engagement interventions in children’s mental health services. Clinical Child and Family Psychology Review, 17(3), 283–298. doi:10.1007/s10567-013-0163-x.
Lindsey, M. A., Chambers, K., Pohle, C., Beall, P., & Lucksted, A. (2013). Understanding the behavioral determinants of mental health service use by urban, under-resourced Black youth: Adolescent and caregiver perspectives. Journal of Child and Family Studies, 22(1), 107–121. doi:10.1007/s10826-012-9668-z.
McGurran, J., & Noseworthy, T. (2002). Improving the management of waiting lists for elective health care service: public perspectives on proposed solutions. Hospital Quarterly, 5(3), 28–32.
McKay, M. M., & Bannon, W. J. (2004). Engaging families in child mental health services. Child and Adolescent Psychiatric Clinics of North America, 13(4), 905–921. doi:10.1016/j.chc.2004.04.001.
McKay, M. M., Lynn, C. J., & Bannon, W. M. (2005). Understanding inner city child mental health need and trauma exposure: Implications for preparing urban service providers. American Journal of Orthopsychiatry, 75(2), 201–210. doi:10.1037/0002-9432.75.2.201.
McKay, M. M., McCadam, K., & Gonzales, J. J. (1996). Addressing the barriers to mental health services for inner city children and their caretakers. Community Mental Health Journal, 32(4), 353–361.
Mendez, J. L., Carpenter, J. L., LaForett, D. R., & Cohen, J. S. (2009). Parental engagement and barriers to participation in a community-based preventive intervention. American Journal of Community Psychology, 44, 1–14.
Murphy, S. M., Zweifach, J., & Hoffman, L. (2012). The everyday concerns of mothers of young children and the motivation to seek ongoing parenting support from experts. Early Child Development and Care, 182(9), 1125–1137. doi:10.1080/03004430.2011.597505.
Nock, M. K., & Ferriter, C. (2005). Parent management of attendance and adherence in child and adolescent therapy: A conceptual and empirical review. Clinical Child and Family Psychology Review, 8(2), 149–166. doi:10.1007/s10567-005-4753-0.
Nock, M. K., & Kazdin, A. E. (2005). Randomized controlled trial of a brief intervention for increasing participation in parent management training. Journal of Consulting and Clinical Psychology, 73, 872–879.
Ofonedu, M. E., Percy, W. H., Harris-Britt, A., & Belcher, H. M. (2013). Depression in inner city African American youth: a phenomenological study. Journal of Child and Family Studies, 22(1), 96–106. doi:10.1007/s10826-012-9583-3.
Oslin, D. W., Ross, J., Sayers, S., Murphy, J., Kane, V., & Katz, I. R. (2006). Screening, assessment, and management of depression in VA primary care clinics: the behavioral health laboratory. Journal of General Internal Medicine, 21, 46–50.
Paterson, W. G., Depew, W. T., Pare, P., Petrunia, D., Switzer, C., Veldhuyzen van Zanten, S. J., & Daniels, S. (2006). Canadian consensus on medically acceptable wait times for digestive health care. Canadian Journal of Gastroenterology, 20(6), 411–423.
Pawlby, S., Hay, D., Sharp, D., Waters, C. S., & Pariante, C. M. (2011). Antenatal depression and offspring psychopathology: The influence of childhood maltreatment. British Journal of Psychiatry, 199(2), 106–112. doi:10.1192/bjp.bp.110.087734.
Popp, T. K., Spinrad, T. L., & Smith, C. L. (2008). The relation of cumulative demographic risk to mothers’ responsivity and control: Examining the role of toddler temperament. Infancy, 13(5), 496–518. doi:10.1080/15250000802329446.
Reitman, D., Currier, R. O., & Stickle, T. R. (2002). A critical evaluation of the parenting stress index-short form (PSI-SF) in a head start population. Journal of Clinical Child and Adolescent Psychology, 31(3), 384–392.
Satcher, D. (2001). Mental health: culture, race, and ethnicity—a supplement to mental health: a report of the surgeon general. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services.
Staudt, M. (2007). Treatment engagement with caregivers of at-risk children: Gaps in research and conceptualization. Journal of Child and Family Studies, 16(2), 183–196. doi:10.1007/s10826-006-9077-2.
Staudt, M., Lodato, G., & Hickman, C. R. (2012). Therapists talk about the engagement process. Community Mental Health Journal, 48(2), 212–218. doi:10.1007/s10597-011-9377-x.
Swartz, H. A., Shear, M. K., Greeno, C., Wren, F. J., Sales, E., Sullivan, B. K., & Ludewig, D. P. (2005). Depression and anxiety among mothers bringing their children to a pediatric mental health clinic. Psychiatric Services, 56, 1077–1083.
Swartz, H. A., Zuckoff, A., Frank, E., Spielvogle, H. N., Shear, M. K., Fleming, M. D., & Scott, J. (2006). An open-label trial of enhanced brief interpersonal psychotherapy in depressed mothers whose children are receiving psychiatric treatment. Depression and Anxiety, 23(7), 398–404. doi:10.1002/da.20212.
Thompson, R., Dancy, B. L., Wiley, T. A., Najdowski, C. J., Perry, S. P., Wallis, J., & Knafl, K. A. (2013). African American families’ expectations and intentions for mental health services. Administration and Policy in Mental Health and Mental Health Services Research, 40(5), 371–383. doi:10.1007/s10488-012-0429-5.
Van Dam, N. T., & Earleywine, M. (2011). Validation of the center for epidemiologic studies depression scale-revised (CESD-R): Pragmatic depression assessment in the general population. Psychiatry Research, 186(1), 128–132. doi:10.1016/j.psychres.2010.08.018.
Weissman, M. M., Pilowsky, D. J., Wickramaratne, P. J., Talati, A., Wisniewski, S. R., Fava, M., & Hughes, C. W. (2006). Remissions in maternal depression and child psychopathology: A STAR*D-child report. Journal of the American Medical Association, 295, 1389–1398.
Westin, A. M. L., Barksdale, C. L., & Stephan, S. H. (2014). The effect of waiting time on youth engagement to evidence based treatments. Community Mental Health Journal, 50, 221–228.
Wilcox, H. C., Rains, M., Belcher, H., Kassam-Adams, N., Kazak, A., Lee, R., et al. (2016). Behavioral problems and service utilization in children with chronic illnesses referred for trauma-related mental health services. Journal of Developmental and Behavioral Pediatrics, 37(1), 62–70. doi:10.1097/DBP.0000000000000236.
Williams, M., Latta, J., & Conversano, P. (2008). Eliminating the wait for mental health services. The Journal of Behavioral Health Services and Research, 35(1), 107–114.
Acknowledgments
Research reported in this publication was supported by the National Institute of Nursing Research of the National Institutes of Health under award #R01 NR012444. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors give special thanks to the families and children who participated in this study, Jasmine Gilmore for her assistance with the qualitative data analysis, and Melissa Kurtz and Kellie Miller for their assistance with data collection.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Ofonedu, M.E., Belcher, H.M.E., Budhathoki, C. et al. Understanding Barriers to Initial Treatment Engagement among Underserved Families Seeking Mental Health Services. J Child Fam Stud 26, 863–876 (2017). https://doi.org/10.1007/s10826-016-0603-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-016-0603-6