
Abstract
Younger sisters of teenage parents have elevated rates of engaging in unprotected sex. This may result from changes in parenting behavior after a sibling becomes pregnant or impregnates a partner, and be particularly pronounced for girls seeking mental health treatment. The current study examines condom use over time in 211 African-American girls recruited from outpatient psychiatric clinics. Findings indicate that having a sibling with a teenage pregnancy history predicts less consistent condom use 2 years later. After accounting for earlier condom use and mental health problems, maternal monitoring moderates condom use such that for girls with a sibling with a pregnancy history, more vigilant maternal monitoring is associated with increased condom use, while for girls with no sibling pregnancy history, maternal monitoring is unrelated to adolescents’ condom use 2 years later. Findings suggest that targeted interventions to increase maternal monitoring of high-risk teens may be beneficial for girls with a sibling history of teenage pregnancy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sisters of childbearing teenagers have significantly elevated rates of teenage pregnancy and risky sexual behavior (Cox et al. 1993; East and Felice 1992; East and Jacobson 2001; East and Kiernan 2001; Friede et al. 1986; Hardy et al. 1998; Hogan and Kitagawa 1985). There are high concordance rates between sibling sexual activity, especially for younger female siblings (Haurin and Mott 1990; McHale et al. 2006; Kornreich et al. 2003; Rodgers and Rowe 1988; Widmer 1997). Further, women with a sister who bore a child during adolescence are almost five times more likely to experience a teenage pregnancy themselves than those without a childbearing sister (East et al. 2007). This risk may be heightened for African American girls and for girls struggling with psychiatric difficulties, as studies indicate that rates of teenage pregnancy and sexual risk are elevated in these groups (Donenberg and Pao 2005; Hogan and Kitagawa 1985; Moore and Chase-Lansdale 2001).
African American girls are at disproportionate risk for contracting HIV and other STIs (Donenberg et al. 2011; Miller et al. 2004), and rates of teenage pregnancy are higher in low-income African American individuals than in other socioeconomic and ethnic groups (Hogan and Kitagawa 1985; Moore and Chase-Lansdale 2001). African American females initiate sex at earlier ages and report higher rates of sexual activity during adolescence than females from other ethnic groups (Centers for Disease Control and Prevention 2000; Dancy et al. 2010). Explanations for these risky sexual behaviors generally fall into two camps: those that emphasize socioeconomic disadvantage and accompanying decreased concern about the adverse health, economic and educational attainment consequences associated with risky sexual behavior; and those that emphasize differences in cultural norms and attitudes (or so-called “cultural deviance”) (Spence and Brewster 2010). These explanations are not mutually exclusive and interactions exist between socioeconomic factors and cultural norms. Regardless of explanatory theories, studies have found that these sexual risk behaviors may be affected by protective parenting behaviors, including monitoring, in African American families (Kogan et al. 2011). Yet, sexual risk behaviors in African-American girls have not yet been explored in conjunction with the specific known risk conferred by having a teenage sibling with a history of pregnancy. A crucial next step for intervention is to identify the ways in which the relationship between sibling pregnancy and sexual risk-taking may be moderated by the context of the parent-adolescent relationship, including the presence of high parental monitoring.
Moreover, research indicates that youth with pre-existing mental health problems are more likely to engage in sexual risk behaviors (Brown et al. 2006). Adolescent depression and emotional problems are associated with inconsistent condom and contraceptive use and negative beliefs about negotiating condom use (Brown et al. 2006; DiClemente et al. 2001a, b). Mental health problems are implicated in adolescents’ risky sexual behavior (Brown et al. 1997; Donenberg et al. 2001, 2011; Donenberg and Pao 2005) via poor risk assessment and decision making, cognitive deficits, low self-esteem, impulsivity, and low self-efficacy and strained interpersonal relationships. For some youth, parental behaviors including monitoring of youths’ activities, may protect against these risks (Donenberg et al. 2002). However, research suggests that these effects are not universal or strong, indicating that some young people may be more protected by parental monitoring than others (Markham et al. 2010). Indeed, girls may be more responsive to an environment of high parental monitoring than boys, as girls spend more time at home and in contact with parents and siblings than do boys (Hofferth and Sandberg 2001).
Two theoretical approaches inform the familial roots of the known link between sibling pregnancy and girls’ sexual behavior. The first is a family socialization model, in which attitudes and behaviors towards sexual behavior are transmitted through the family, including parents and siblings (East 1996; Jaccard et al. 1996). The second is a parental control model, where direct supervision and control may be impacted by the existence of a siblings’ pregnancy (Spence and Brewster 2010). Both mechanisms may be at play, i.e., parental control, in the form of monitoring, moderates risk that may be conferred through direct and indirect mechanisms of family socialization that ensue from a siblings’ teenage pregnancy.
Concordance in sibling sexual activity is partly accounted for by direct mechanisms, such as social learning by a younger sibling modeling an older sibling’s behavior, or by exposure to an older siblings’ deviant peers or risk behavior, as has been found for drug use and delinquency outcomes (Ary et al. 1993; Rowe and Gulley 1992). In support of this hypothesis, aspects of sibling relationship quality, such as conflict and warmth, have been related to younger sibling early sexual activity, risky sex, and condom use (East and Khoo 2005; East and Shi 1997; McHale et al. 2009). Thus, direct effects between teenagers’ positive expectations and their perceptions of their siblings’ pregnancy and sexual behavior likely account for some of the association between siblings’ sexual behavior via family socialization.
Decreased parental control via changes in family structure following a teenage pregnancy may also explain increased risk for younger siblings. While less research has focused on parental effects, studies show that mothers of pregnant teens monitor and communicate less with their other children, and also become more permissive over time (East 1999). Not surprisingly, having an older sibling with a child is associated with increased family stress, which in turn may affect parenting behaviors such as monitoring (East 1998; East and Jacobson 2003). Indeed, mothers report being less strict with their other children in families where an older daughter recently had a baby, perhaps due to the “role strain” and task demands associated with the need to help care for grandchildren (East 1999). These changes in parenting behavior may differ by ethnic group. For example, African-American mothers report that they increase their expectations of their younger children after a sibling has become a teenage parent, while Hispanic mothers treat their child-bearing daughter more harshly than other siblings after the birth of a grandchild (East and Jacobson 2003). Thus, older siblings’ pregnancies may indirectly affect younger sibling sexual behavior via instrumental changes in parenting behaviors, including decreased parental monitoring.
There is a well-documented relationship linking parental monitoring with adolescent risky sexual activity (Donenberg et al. 2002). Higher parental monitoring is linked to less sexual risk taking, such as more frequent use of condoms and other contraception (Baker et al. 1999; DiClemente et al. 2001a, b; Stanton et al. 2002). Yet some longitudinal studies have not found that this link lasts over time (Markham et al. 2010; Stanton et al. 2002). Mixed findings suggest that the impact of parental monitoring may be complex. Parental monitoring may be protective for some girls’ condom use but not others. Indeed, parental monitoring may play an especially important role for girls with a teenage sibling with a history of pregnancy, who are at risk themselves for pregnancy and sexually transmitted infections (including HIV) because they are engaging in more frequent or unprotected vaginal sex than teenagers without childbearing siblings. Despite considerable evidence that high parental monitoring is protective for sexual risk outcomes, and also that monitoring decreases after an older sibling has a child, it is not clear whether high parental monitoring tempers the risk conferred by having a sibling with a history of teenage pregnancy. It is especially important to examine the role of parental monitoring with populations who have been under-represented in the extant literature, including low-income African-American families, adolescents with psychiatric difficulties, and adolescent girls in general. The demands of urban poverty and of coping with a child with mental illness and associated behavioral difficulties may further increase the importance of parental monitoring for these highly stressed families. Early studies of ethnic differences in parenting approaches found that authoritarian parenting styles, which include more rigidity and parental power assertion, may be beneficial for African-American children, especially those growing up in low-income neighborhoods where authoritarian approaches may protect children from increased threat and danger (Baldwin et al. 1990; Baumrind 1972). Likewise, evidence suggests that parental monitoring is linked to sexual behavior in children in psychiatric care, especially for girls, whose parents may engage in more monitoring than those of their male peers (Donenberg et al. 2002). Few studies have examined these relationships in psychiatric samples or the impact of sibling pregnancy and the protective role of parenting on troubled girls.
In the current study we examine whether an environment of high maternal monitoring tempers the impact of a sibling’s teenage pregnancy on sexual risk behavior in African-American female teens seeking mental health treatment. We define sibling pregnancy as having a sister or brother who became pregnant or impregnated someone. Maternal monitoring is defined by a range of activities that include direct supervision, knowing a child’s whereabouts, and setting clear limits and rules for behavior (Parke and Buriel 1998). The examined sexual risk outcome is change in condom use, which serves a dual function in both preventing pregnancy (contraception) and reducing contraction rates for HIV and other STIs. This study seeks to extend the existing literature by examining the moderating role of parental monitoring, over time, on the sexual behavior of African American girls seeking mental health care, a group traditionally underrepresented in research. We explore family factors that may influence sexual behavior among young women at heightened risk for unprotected sex, predicting that girls whose teenage sibling had a history of pregnancy at study baseline would be more likely to engage in decreased condom use 2 years later. We hypothesize that this relationship will be moderated by maternal monitoring even after accounting for baseline condom use; that is, high monitoring will be protective for girls with a sibling teen pregnancy history, but it will not affect outcomes for girls without a sibling pregnancy. In exploring these questions we seek to expand our knowledge of indirect family factors that may contribute to heightened risk, over time, for a very high risk population of African-American teenage girls seeking mental health services.
Method
Participants
Participants were 211 12–16 year-old (M = 14.41; SD = 1.17) daughters and their biological mothers (74 %), grandmothers (15 %), and other female caregivers (11 %). Approximately 83 % of families scored in the first three levels of the Hollingshead index (Hollingshead 1975), indicating low to middle incomes. Mothers’ education levels varied: 23.8 % reported partial high school, 22.4 % were high school graduates, 40.5 % attended partial college and received special training, and 13.3 % were college graduates and/or had graduate or professional training. Symptom ratings (Achenbach 1991a, b) revealed significant rates of adolescent distress at baseline; according to either caretaker or adolescent reports (counting the reporter who endorsed a higher score), about 39 % of adolescents were characterized by some type of clinically significant distress (T ≥ 63; indexed by the Total Problems Scale), with 44 and 61 % of youth in the clinical range of internalizing and externalizing disorders, respectively. Patterns did vary by rater, such that 20 % of youth-self-reported clinically significant internalizing problems and 33 % endorsed clinically significant externalizing problems. Mothers reported that 34 and 51 % of girls reached clinically significant levels of internalizing and externalizing problems respectively. According to youth and parents, between 20 and 23 % of girls in this study, respectively, would meet full criteria for DSM-IV-TR diagnoses of posttraumatic stress disorder, major depressive disorder, or conduct disorder, suggesting significant mental health need. The current study focuses on girls’ siblings’ sexual risk behavior, girls’ reports of maternal permissiveness, mothers’ reports of parental monitoring, and girls’ sexual behavior.
Procedure
All study procedures were approved by the University of Illinois at Chicago’s Institutional Review Board. This study is part of a larger longitudinal study of HIV-risk behavior among 266 African American girls seeking outpatient mental health services. Eligible mother-daughter (“mothers” refers to all female caregivers) dyads were recruited from eight mental health clinics in urban Chicago. Clinic staff obtained the family’s permission to forward their contact information to research staff. Eighty-two percent of the families who were invited to participate enrolled in the study. Girls identified by clinic staff as mentally retarded, with significant cognitive impairment, or wards of the Illinois Department of Child and Family Services (DCFS) were excluded. Interviews were conducted at a university research site, not in the clinics where participants were recruited. Girls and their mothers were interviewed separately in private rooms. Consent and assent to participate were obtained separately for mothers and daughters by trained interviewers, who reviewed study procedures and risks and benefits separately with mothers and daughters. Adolescent refusal to participate superseded maternal consent. Participants were interviewed five times over 2 years and completed Audio Computer Assisted Self Interview (ACASI) administered self-report surveys. Mothers and daughters each received $45 at Time 1 (T1) and $60 at Time 5 (T5) 2 year follow-up as well as travel expenses at each time point. Outcomes in the current study are from 211 families at T5 follow-up (79.32 % retention). This latest time point was chosen in order to maximize the number of study participants who were sexually active at follow-up. Families with available T5 data did not differ significantly from those with missing T5 data on any of the study’s independent variables (child age, presence of siblings, mental health problems, mother-reported monitoring) or socioeconomic status as measured by Hollingshead index.
Measures
Demographics
At baseline, mothers reported on girls’ age and ethnic background, family structure and income, and siblings. Mothers reported on the pregnancy or parenting status of participants’ male and female siblings and the outcomes of each pregnancy (abortion, miscarriage, adoption, stillbirth, baby kept) and age at time of pregnancy. 52 (24.6 %) girls with available T5 data had one or more siblings who became pregnant or impregnated a partner as a teenager (under 19 years of age) at baseline. Of these 52 pregnancies, 43 were pregnant sisters and nine were brothers who had impregnated a sexual partner.
Parental Monitoring
Using the Parenting Style Questionnaire (PSQ) (Oregon Social Learning Center 1990), parents reported on their monitoring practices at baseline from 1 (Not at all True/Never) to 5 (Very True/Almost Every Day) (e.g., “How often would you know if your teen came home an hour late.”). Internal consistency for the full baseline sample was moderate (α = .76). Higher scores indicate greater parent-perceived monitoring of their teen’s activities. The reliability and validity of the PSQ is well-established, and the measure has been used extensively with psychiatric youth samples (Oregon Social Learning Center 1990). As in previous research (e.g., Donenberg et al. 2002), a composite variable, Parental Monitoring, was employed using ten face-valid items (range 22–50; M = 41.07; SD = 6.18).
Mental Health
Parents completed the Child Behavior Checklist (Achenbach 1991a, b) rating of their adolescents’ symptoms at baseline. This ubiquitous measure of psychiatric symptoms has excellent sociometric properties. The Total Problems Scale was derived in order to assess a global index of girls’ problems at the onset of the study.
Risky Sexual Behavior
The AIDS Risk Behavior Assessment (ARBA) (Donenberg et al. 2001) is a computerized self-administered interview designed for use with adolescents to assess their self-reported sexual behavior, drug/alcohol use, and needle use associated with HIV infection. The ARBA uses a skip structure so that more detailed items do not follow initial screening questions answered negatively. We examined safe vaginal sex defined by a single face-valid item, “In the last 6 months, how often did you and your partner use condoms/latex protection during vaginal sex?” with scores ranging from 1 (Never) to 5 (Always Used Condoms) or 6 (Has Not Had Vaginal Sex in the Past 6 Months). We focus on vaginal sex specifically because of our focus on safe sex practices related to pregnancy and HIV/STIs. This method of assessing condom use has been utilized in previous research (e.g., Udell et al. 2011) as a continuous indicator of safe sex practices, with lower scores indicating greater sexual risk. Two forms of condom use were analyzed. A continuous variable was tested in multiple regression analyses, and a dichotomous variable (i.e., not sexually active plus always used a condom vs. did not always use condoms during vaginal sex) was tested in Chi square analyses for teens with and without sibling pregnancy, described below. Study participants reported on their condom use at baseline (T1) as well as at T5 2-year follow-up.
Data Analysis
Multiple regressions were used to examine the impact of sibling pregnancy status at baseline on condom use at T5, moderated by baseline level of maternal monitoring. All continuous variables were centered to reduce multicollinearity. Examination of skewness and kurtosis suggested that the dependent variable, condom use, violated some assumptions of normality. Specifically, condom use was not kurtotic (kurtosis = .54), but slightly skewed (skew = −1.43), indicating that teens were more likely to report safer sexual activity (mean = 4.90, SD = 1.69). Using generally accepted guidelines (e.g., Tabachnick and Fidell 2013), the rank-based BLOM transformation was used to normalize this variable. All substantive analyses were initially performed on the transformed dependent variable, but findings revealed the same patterns for the non-transformed data. In light of recent evidence that rank-transformed data may inflate Type I error, we retained the non-transformed dependent variable in all subsequent analyses (Beasley et al. 2009; Solomon and Sawilowsky 2009). In addition, other potential covariates (e.g., socioeconomic status, maternal age at first pregnancy) were examined and not retained because they did not demonstrate significant associations with the dependent variable in this sample.
For multiple regression analysis, age, total problems at baseline, and condom use at baseline were entered as covariates in Block 1. This allowed for the examination of substantive relationships after accounting for variance associated with age, mental health and history of condom use. Explanatory variables, sibling pregnancy status (yes/no) at baseline and maternal monitoring at baseline, were entered in Block 2. Residualized interaction terms between baseline maternal monitoring and sibling pregnancy status were entered in Block 3 to examine whether monitoring moderated the relationship between sibling pregnancy history and condom use 2 years later.
Results
Table 1 reports descriptive statistics for all key study variables. Girls with a sibling with a history of teenage pregnancy did not differ from those without a pregnant sibling on age at baseline (t = .34, p = .56), mother-reported monitoring (t = 1.27, p = .26), or T1 condom use (t = −.59, p = .55). Groups differed significantly on baseline CBCL total problems (t = 4.41, p = .037) with girls with a sibling pregnancy history showing higher levels of problems (M = 64.87, SD = 10.52) than those with no such history (M = 61.05, SD = 11.63). Groups also differed on follow-up condom use at T5 (t = 7.62, p = .006) with girls with a sibling pregnancy history endorsing decreased condom use (M = 4.35, SD = 2.0) compared with those with no sibling pregnancy history (M = 5.08, SD = 1.55). Table 2 reports bivariate correlations between variables used in hierarchical regression analyses, for descriptive purposes.
Chi square analyses showed that teens with a sibling who had become pregnant or impregnated someone as a teenager were significantly less likely to always use condoms during vaginal sex than those with no prior sibling pregnancy (χ2 = 6.86, p = .009). Indeed, among 211 reporting teens, 36.5 % of those with a sibling pregnancy reported that they did not always use condoms, while only 18.9 % of teens with no sibling pregnancy reported irregular condom use.
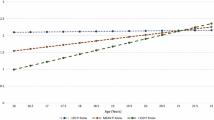
Table 3 displays results for the multiple regression analysis. Results suggest that T5 condom use was significantly predicted by T1 condom use (β = .37, p < .001), maternal monitoring (β = −.29, p < .05), and sibling pregnancy status (β = .18, p < .01), suggesting that baseline condom use, maternal monitoring, and having a sibling with pregnancy history were associated with decreased condom use 2 years later. However, these relationships were qualified by a maternal monitoring × sibling pregnancy status interaction (β = .35, p < .01), such that maternal monitoring was not associated with condom use for girls with no sibling pregnancy history (r = .01, ns), while maternal monitoring was associated with condom use for girls with a sibling with a teenage pregnancy history (r = .32, p < .05). This difference in correlations is significant (Fisher’s Z = 1.96, p < .05) and depicted in Fig. 1.

Interaction between condom use and maternal monitoring for girls with (n = 52) and without (n = 159) a sibling with history of pregnancy
Discussion
This is the first study to prospectively examine the relationship between sibling pregnancy history, a known risk factor for youth sexual behavior, and later condom use among African-American girls receiving psychiatric care. We also tested whether maternal monitoring moderated this relationship. Results indicated that for these at-risk girls, condom use during vaginal sex was predicted by a history of sibling teenage pregnancy. Twice as many girls with a history of sibling teenage pregnancy reported decreased condom use compared to girls with no history of sibling pregnancy. Moreover, maternal monitoring predicted changes in condom use. In particular, higher monitoring was significantly associated with higher levels of condom use for girls with a history of sibling teenage pregnancy, even after accounting for baseline condom use.
As in any study, a number of limitations are worthy of note. These include the presence of only baseline assessments of sibling pregnancy status, mental health, and parental monitoring, which means that findings cannot account for changes over time in these variables. However, the study’s prospective design sheds important light on parenting and sibling behaviors that accord risk for condom use 2 years after initial assessment. Additionally, the measure of maternal monitoring is limited to a single reporter (mother), and some have questioned the validity of this measure of monitoring, asserting that willing youth disclosure is more accurate than unwelcome parental attempt to control of monitor their children’s activities (Kerr et al. 2010; Stattin and Kerr 2000). Yet, a robust literature on the importance of parental monitoring across outcomes attests to the value of mother-reported monitoring, even if flaws may exist in the standardly-applied measurement approaches (Pettit et al. 2007; Racz and McMahon 2011). Indeed, a more general limitation of this research approach is that the data are by nature correlational and nested. Both measures of maternal monitoring, adolescent mental health, and sibling pregnancy history are derived from mothers. Correlational data such as these do not elucidate causal mechanisms. Generalizability to ethnic groups outside of African-American families and to girls without mental health problems is also limited. However, these groups are known to be at particular risk for engaging in unprotected sexual activity. The current study only examines condom use, while sexually active girls may have employed other forms of contraception, including hormonal birth control. However, condom use is an important health outcome regardless of contraception status because of its’ role in protecting against HIV and STIs. Lastly, a variety of factors may contribute to girls’ reports of condom use during vaginal sex, including girls’ feelings of self-efficacy in requesting condom use, her relationship with her sexual partner, and her partner’s attitudes towards contraceptive use. These explanatory factors are not examined in the current study.
However, the current study also makes several notable contributions to the existing literature, including the examination of a novel, high risk sample of African-American girls seeking mental health treatment, a longitudinal design that allows us to examine change in condom use over time, and findings that expand upon previous research implicating parental monitoring in adolescent sexual risk taking. Moreover, we examine converging family influences on adolescent sexual behavior. Specifically, these findings on maternal monitoring extend previous research which suggested that monitoring may be protective in African-American girls, but did not find long-term effects nor examine moderators of those effects (Stanton et al. 2002). The current study indicates that an environment of higher parental monitoring is related to more consistent condom use later in adolescence for youth who have had a sibling with a teenage pregnancy. These findings inform research on family risk and protective factors for girls’ contraceptive use. In particular, mixed findings have been found for the effects of parental monitoring on girls’ condom use (Markham et al. 2010). This study explores a possible risk factor—sibling teenage pregnancy—that may help identify girls for whom maternal monitoring is especially important. In addition, this study identifies an intervening variable—high maternal monitoring—which may protect against the risk conferred by sibling pregnancy on girls’ later sexual risk behavior.
Indeed, after accounting for girls’ mental health and baseline condom use, maternal monitoring predicted condom use for all girls in the study, regardless of sibling pregnancy history. This association between monitoring and decreased condom use was significant, however, only for girls with a sibling pregnancy history. The particular nature of the sample, African-American girls seeking psychiatric care, may inform the interaction between sibling pregnancy history and maternal monitoring. This sample is at increased risk for both inconsistent condom use and parenting disruptions (DiClemente et al. 2001a, b; Miller et al. 1999). Mothers of a mentally-ill teen who are able to increase monitoring of their younger teens even after another child has become pregnant or impregnated someone may be accessing additional resources or exhibiting resilience in the wake of a great deal of cumulative family stress. In fact, these mothers may be actively and purposefully changing their behavior and adapting their parenting strategies to prevent another child from becoming a teenage parent. Indeed, it is worthy of note that parenting is always a bi-directional process between parent and child, and parenting a child with psychopathology can be particularly challenging. Youth with mental health difficulties, including behavioral problems, may influence their parents’ behavior towards them (Dodge and Pettit 2003) and pre-existing youth problems may heighten the effects of poor parenting on later youth problems (Pettit et al. 1999). Thus, the reasons why some mothers can increase their monitoring of troubled younger siblings while others cannot are complex. Indeed, parents’ ability to monitor their children can be complicated by a variety of factors including parent’s own mental health, financial resources, and other caregiving responsibilities. Especially in families where the parent is also helping to raise grandchildren, parents’ ability to monitor their adolescents may be more strained (East 1999). Future research might examine individual, family or community characteristics that permit some mothers to increase their monitoring efforts of younger teens while others cannot.
In the current study, both sisters and brothers with a history of teen pregnancy were included. Most research on risks conferred by sibling teen pregnancy has included only sisters with a teen pregnancy, or only childbearing sisters. While sister’s pregnancies are easier to track and mothers are more likely to be aware of them, there is reason to believe that brother’s sexual activity may still impact teens’ sexual choices. Watching a brother become a parent, or navigating the decision-making involved in impregnating a partner as an adolescent, might indeed make a strong impact on a girls’ own behavior choices. The current study’s finding that a sister or a brother with irregular contraception use can confer risk for decreased condom use for girls suggests that it is not just changes in family structure following the birth of a grandchild that account for this risk. Our results imply that teen girls who have a sibling—a brother or a sister—who have engaged in unprotected sexual activity in adolescence are at a greater risk for doing so themselves. The mechanism for this should be examined more thoroughly through both qualitative and empirical studies exploring the processes of family socialization of adolescent sexual behavior.
A strength and a weakness of the current study is that the sample is extremely high-risk: urban African-American girls seeking psychiatric care. While this group is an important cohort for examining sexual behavior because of elevated rates of pregnancy, HIV and STIs, the sheer accumulation of risk in this sample is high. It is worthy of note that baseline mental health scores were significantly negatively associated with later condom use in the sample as a whole. Thus, girls who were more troubled in early adolescence were less likely to regularly use condoms 2 years later. In addition, girls with a sibling with a history of teenage pregnancy had significantly higher rates of mental health problems than those with no sibling history. Clearly these variables are not operating in isolation, and girls with mental health difficulties may be more likely to have siblings who share risk factors for sexual risk-taking. This suggests that a cumulative risk model may apply here: the girls with greater mental health problems (individual factor) also are more likely to have siblings with a pregnancy history (family factor) and other, untested proximal and distal factors such as community norms, neighborhood safety and peer relationships may also be present (Gerard and Buehler 2004).
Findings of this study do have implications for intervention approaches. Given high rates of pregnancy and STI in African-American girls, condom use may be a particularly important behavioral intervention target. While individual and group interventions for low-income youth have been shown to be effective in promoting consistent contraceptive use for at-risk youth (Boekeloo et al. 1999; DiClemente et al. 2004, 2009; East et al. 2007; Jemmott et al. 1998, 2005), parenting-based interventions may be especially important for certain at-risk groups (Guilamo-Ramos et al. 2011; Prado et al. 2007; Jaccard et al. 2002; Kirby and Miller 2002). In particular, the current study suggests that African-American mothers of child-bearing teens and/or adolescents with mental health difficulties may benefit from education and support around the importance of monitoring their children’s whereabouts and activities. In particular, study results suggest that mothers of teens who have become parents should be educated about the additional risks to their other children and about the benefits of being diligent and attentive in order to promote lower risk sexual behavior. This may be especially important (and challenging) for mothers who are simultaneously helping to raise grandchildren. When it comes to contraceptive use and sexual risk behavior, sibling pregnancy history, parenting behavior and child mental health appear to come together to form a family affair. Therefore, interventions targeted at the family-level, which intervene with both high-risk adolescents with mental health difficulties and with their caregivers, should continue to be developed and employed for preventing adolescent pregnancy, STIs and HIV.
References
Achenbach, T. M. (1991a). Integrative guide for the 1991 CBCL/4-18, YSR, and TRF profiles. Burlington: Department of Psychiatry, University of Vermont.
Achenbach, T. M. (1991b). Child behavior checklist/4–18. Burlington: University of Vermont.
Ary, D. V., Tildesley, E., Hops, H., & Andrews, J. (1993). The influence of parent, sibling, and peer modeling and attitudes on adolescent use of alcohol. Substance Use and Misuse, 28(9), 853–880.
Baker, J. G., Rosenthal, S. L., Leonhardt, D., Kollar, L. M., Succop, P. A., Burklow, K. A., et al. (1999). Relationship between perceived parental monitoring and young adolescent girls’ sexual and substance use behaviors. Journal of Pediatric and Adolescent Gynecology, 12(1), 17–22.
Baldwin, A., Baldwin, C., & Cole, R. E. (1990). Stress-resistant families and stress-resistant children. In J. E. Rolf, A. S. Masten, D. Cichetti, K. N. Wechterlein, & S. Weintraub (Eds.), Risk and protective factors in the development of psychopathology (pp. 257–280). New York: Cambridge University Press.
Baumrind, D. (1972). An exploratory study of socialization effects on Black children: Some Black–White comparisons. Child Development, 43, 261–267.
Beasley, T. M., Erickson, S., & Allison, D. B. (2009). Rank-based inverse normal transformations are increasingly used, but are they merited? Behavior Genetics, 39(5), 580–595.
Boekeloo, B. O., Schamus, L. A., Simmens, S. J., Cheng, T. L., O’Connor, K., & D’Angelo, L. J. (1999). A STD/HIV prevention trial among adolescents in managed care. Pediatrics, 103(1), 107–115.
Brown, L. K., Danovsky, M. B., Lourie, K. J., DiClemente, R. J., & Ponton, L. E. (1997). Adolescents with psychiatric disorders and the risk of HIV. Journal of the American Academy of Child and Adolescent Psychiatry, 36(11), 1609–1617.
Brown, L. K., Tolou-Shams, M., Lescano, C., Houck, C., Zeidman, J., Pugatch, D., & Lourie, K. J. (2006). Depressive symptoms as a predictor of sexual risk among African American adolescents and young adults. Journal of Adolescent Health, 39(3), 444-e1.
Centers for Disease Control and Prevention. (2000). Morbidity and Mortality Weekly Report, Surveillance Summaries. Youth Risk Behavior Surveillance–United States, 1999. Retrieved from http://www.cdc.gov/mmwr/preview/mmwrhtml/ss4905a1.htm.
Cox, J., Emans, S., & Bithoney, W. (1993). Sisters of teen mothers: Increased risk for adolescent parenthood. Adolescent and Pediatric Gynecology, 6(3), 138–142.
Dancy, B. L., Crittenden, K. S., & Ning, H. (2010). African-American adolescent girls’ initiation of sexual activity: Survival analysis. Women’s Health Issues, 20(2), 146–155.
DiClemente, R. J., Wingood, G. M., Crosby, R. A., Sionean, C., Brown, L. K., Rothbaum, B., et al. (2001a). A prospective study of psychological distress and sexual risk behavior among black adolescent females. Pediatrics, 108(5), e85.
DiClemente, R. J., Wingood, G. M., Crosby, R., Sionean, C., Cobb, B. K., Harrington, K., et al. (2001b). Parental monitoring: Association with adolescents’ risk behaviors. Pediatrics, 107, 1363–1368.
DiClemente, R. J., Wingood, G. M., Harrington, K. F., et al. (2004). Efficacy of an HIV prevention intervention for African American adolescent girls: A randomized controlled trial. Journal of the American Medical Association, 292, 171–179.
DiClemente, R. J., Wingood, G. M., Rose, E. S., Sales, J. M., Lang, D. L., Caliendo, A. M., et al. (2009). Efficacy of sexually transmitted disease/human immunodeficiency virus sexual risk-reduction intervention for African American adolescent females seeking sexual health services: A randomized controlled trial. Archives of Pediatrics and Adolescent Medicine, 163(12), 1112.
Dodge, K. A., & Pettit, G. S. (2003). A biopsychosocial model of the development of chronic conduct problems in adolescence. Developmental Psychology, 39(2), 349.
Donenberg, G. R., Emerson, E., Bryant, F. B., Wilson, H., & Weber-Shifrin, E. (2001). Understanding AIDS-risk behavior among adolescents in psychiatric care: Links to psychopathology and peer relationships. Journal of the American Academy of Child and Adolescent Psychiatry, 40(6), 642–653.
Donenberg, G., Emerson, E., & Mackesy-Amiti, M. E. (2011). Sexual risk among African American girls: Psychopathology and mother–daughter relationships. Journal of Consulting and Clinical Psychology, 79(2), 153–158.
Donenberg, G. R., & Pao, M. (2005). Youths and HIV/AIDS: Psychiatry’s role in a changing epidemic. Journal of the American Academy of Child and Adolescent Psychiatry, 44(8), 728–747.
Donenberg, G. R., Wilson, H. W., Emerson, E., & Bryant, F. B. (2002). Holding the line with a watchful eye: The impact of perceived parental permissiveness and parental monitoring on risky sexual behavior among adolescents in psychiatric care. AIDS Education and Prevention, 14(2), 138.
East, P. L. (1996). Do adolescent pregnancy and childbearing affect younger siblings? Family Planning Perspectives, 28, 148–153.
East, P. L. (1998). Racial and ethnic differences in girls’ sexual, marital, and birth expectations. Journal of Marriage and the Family, 60(1), 150.
East, P. L. (1999). The first teenage pregnancy in the family: Does it affect mothers’ parenting, attitudes, or mother–adolescent communication? Journal of Marriage and the Family, 61(2), 306.
East, P. L., & Felice, M. E. (1992). Pregnancy risk among the younger sisters of pregnant and childbearing adolescents. Journal of Developmental and Behavioral Pediatrics, 13(2), 128–136.
East, P. L., & Jacobson, L. J. (2001). The younger siblings of teenage mothers: A follow-up of their pregnancy risk. Developmental Psychology, 37(2), 254.
East, P. L., & Jacobson, L. J. (2003). Mothers’ differential treatment of their adolescent childbearing and nonchildbearing children: Contrasts between and within families. Journal of Family Psychology, 17(3), 384.
East, P. L., & Khoo, S. T. (2005). Longitudinal pathways linking family factors and sibling relationship qualities to adolescent substance use and sexual risk behaviors. Journal of Family Psychology, 19(4), 571.
East, P. L., & Kiernan, E. A. (2001). Risks among youths who have multiple sisters who were adolescent parents. Family Planning Perspectives, 33(2), 75–80.
East, P. L., Reyes, B. T., & Horn, E. J. (2007). Association between adolescent pregnancy and a family history of teenage births. Perspectives on Sexual and Reproductive Health, 39(2), 108–115.
East, P. L., & Shi, C. R. (1997). Pregnant and parenting adolescents and their younger sisters: The influence of relationship qualities for younger sister outcomes. Journal of Developmental and Behavioral Pediatrics, 18(2), 84–90.
Friede, A., Hogue, C. J., Doyle, L. L., Hammerslough, C. R., Sniezek, J. E., & Arrighi, H. (1986). Do the sisters of childbearing teenagers have increased rates of childbearing? American Journal of Public Health, 76(10), 1221–1224.
Gerard, J. M., & Buehler, C. (2004). Cumulative environmental risk and youth maladjustment: The role of youth attributes. Child Development, 75(6), 1832–1849.
Guilamo-Ramos, V., Bouris, A., Jaccard, J., Gonzalez, B., McCoy, W., & Aranda, D. (2011). A parent-based intervention to reduce sexual risk behavior in early adolescence: Building alliances between physicians, social workers, and parents. Journal of Adolescent Health, 48(2), 159–163.
Hardy, J. B., Astone, N. M., Brooks-Gunn, J., Shapiro, S., & Miller, T. L. (1998). Like mother, like child: Intergenerational patterns of age at first birth and associations with childhood and adolescent characteristics and adult outcomes in the second generation. Developmental Psychology, 34(6), 1220.
Haurin, R. J., & Mott, F. L. (1990). Adolescent sexual activity in the family context: The impact of older siblings. Demography, 27(4), 537–557.
Hofferth, S. L., & Sandberg, J. F. (2001). How American children spend their time. Journal of Marriage and Family, 63(2), 295–308.
Hogan, D. P., & Kitagawa, E. M. (1985). The impact of social status, family structure, and neighborhood on the fertility of black adolescents. American Journal of Sociology, 90(4), 825–855.
Hollingshead, A. B. (1975). Four factor index of social status (Unpublished manuscript). Yale University, New Haven, CT.
Jaccard, J., Dittus, P. J., & Gordon, V. V. (1996). Maternal correlates of adolescent sexual and contraceptive behavior. Family Planning Perspectives, 28, 159–165.
Jaccard, J., Dodge, T., & Dittus, P. (2002). Parent–adolescent communication about sex and birth control: A conceptual framework. New Directions for Child and Adolescent Development, 2002(97), 9–42.
Jemmott, J. B., Jemmott, L. S., Braverman, P. K., & Fong, G. T. (2005). HIV/STD risk reduction interventions for African American and Latino adolescent girls at an adolescent medicine clinic: A randomized controlled trial. Archives of Pediatrics & Adolescent Medicine, 159(5), 440–449.
Jemmott, J. B., I. I. I., Jemmott, L. S., & Fong, G. T. (1998). Abstinence and safer sex HIV risk-reduction interventions for African American adolescents. JAMA, the Journal of the American Medical Association, 279(19), 1529–1536.
Kerr, M., Stattin, H., & Burk, W. J. (2010). A reinterpretation of parental monitoring in longitudinal perspective. Journal of Research on Adolescence, 20(1), 39–64.
Kirby, D., & Miller, B. C. (2002). Interventions designed to promote parent-teen communication about sexuality. New Directions for Child and Adolescent Development, 97, 93–110.
Kogan, S. M., Brody, G. H., Gibbons, F. X., Chen, Y. F., Grange, C. M., Simons, R. L., et al. (2011). Mechanisms of family impact on African American adolescents’ HIV-related behavior. Journal of Research on Adolescence, 21(2), 361–375.
Kornreich, J. L., Hearn, K. D., Rodriguez, G., & O’Sullivan, L. F. (2003). Sibling influence, gender roles, and the sexual socialization of urban early adolescent girls. Journal of Sex Research, 40(1), 101–110.
Markham, C. M., Lormand, D., Gloppen, K. M., Peskin, M. F., Flores, B., Low, B., & House, L. D. (2010). Connectedness as a predictor of sexual and reproductive health outcomes for youth. Journal of Adolescent Health, 46(3), S23–S41.
McHale, S. M., Bissell, J., & Kim, J. Y. (2009). Sibling relationship, family, and genetic factors in sibling similarity in sexual risk. Journal of Family Psychology, 23(4), 562.
McHale, S. M., Kim, J. Y., & Whiteman, S. D. (2006). Sibling relationships in childhood and adolescence. In P. Noller & J. Feeney (Eds.), Close relationships (pp. 127–150). Hove, England: Psychology Press, Taylor & Francis (UK).
Miller, K. S., Boyer, C. B., & Cotton, G. (2004). The STD and HIV epidemics in African American youth: Reconceptualizing approaches to risk reduction. Journal of Black Psychology, 30(1), 124–137.
Miller, K. S., Forehand, R., & Kotchick, B. A. (1999). Adolescent sexual behavior in two ethnic minority samples: The role of family variables. Journal of Marriage and the Family, 61(1), 85–98.
Moore, M. R., & Chase-Lansdale, P. L. (2001). Sexual intercourse and pregnancy among African American girls in high-poverty neighborhoods: The role of family and perceived community environment. Journal of Marriage and Family, 63(4), 1146–1157.
Oregon Social Learning Center. (1990). Parental monitoring and supervision constructs (Technical reports) Oregon Social Learning Center.
Parke, R. D., & Buriel, R. (1998). Socialization in the family: Ethnic and ecological perspectives. In W. Damon (Ed.), Handbook of child psychology (5th ed.). New York: Wiley.
Pettit, G. S., Bates, J. E., Dodge, K. A., & Meece, D. W. (1999). The impact of after-school peer contact on early adolescent externalizing problems is moderated by parental monitoring, perceived neighborhood safety, and prior adjustment. Child Development, 70(3), 768–778.
Pettit, G. S., Keiley, M. K., Laird, R. D., Bates, J. E., & Dodge, K. A. (2007). Predicting the developmental course of mother-reported monitoring across childhood and adolescence from early proactive parenting, child temperament, and parents’ worries. Journal of Family Psychology, 21(2), 206.
Prado, G., Pantin, H., Briones, E., Schwartz, S. J., Feaster, D., Huang, S., et al. (2007). A randomized controlled trial of a parent-centered intervention in preventing substance use and HIV risk behaviors in Hispanic adolescents. Journal of Consulting and Clinical Psychology, 75(6), 914.
Racz, S. J., & McMahon, R. J. (2011). The relationship between parental knowledge and monitoring and child and adolescent conduct problems: A 10-year update. Clinical Child and Family Psychology Review, 14(4), 377–398.
Rodgers, J. L., & Rowe, D. C. (1988). Influence of siblings on adolescent sexual behavior. Developmental Psychology, 24(5), 722.
Rowe, D. C., & Gulley, B. L. (1992). Sibling effects on substance use and delinquency. Criminology, 30(2), 217–234.
Solomon, S. R., & Sawilowsky, S. S. (2009). Impact of rank-based normalizing transformations on the accuracy of test scores. Journal of Modern Applied Statistical Methods, 8, 448–462.
Spence, N., & Brewster, K. L. (2010). Adolescents’ sexual initiation: The interaction of race/ethnicity and immigration status. Population Research Policy Review, 29, 339–362.
Stanton, B., Li, X., Pack, R., Cottrell, L., Harris, C., & Burns, J. M. (2002). Longitudinal influence of perceptions of peer and parental factors on African American adolescent risk involvement. Journal of Urban Health, 79(4), 536–548.
Stattin, H., & Kerr, M. (2000). Parental monitoring: A reinterpretation. Child Development, 71(4), 1072–1085.
Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed.). Boston: Pearson Education.
Udell, W., Donenberg, G., & Emerson, E. (2011). The impact of mental health problems and religiousity on African-american girls’ HIV-risk. Cultural Diversity and Ethnic Minority Psychology, 17, 217–224.
Widmer, E. D. (1997). Influence of older siblings on initiation of sexual intercourse. Journal of Marriage and the Family, 59(4), 928–938.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Nichols, S., Javdani, S., Rodriguez, E. et al. Sibling Teenage Pregnancy and Clinic-Referred Girls’ Condom Use: The Protective Role of Maternal Monitoring. J Child Fam Stud 25, 1178–1187 (2016). https://doi.org/10.1007/s10826-015-0306-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-015-0306-4