
Abstract
The current study examined whether social problems accounted for the relation between reactive aggression and withdrawn/depressed symptoms in a sample of 147 children (54.4% male) ranging from 5 to 13 years of age (M = 8.22 years) who attended a community based after-school program. Findings suggested that indeed social problems mediated the link between reactive aggression and withdrawn/depressed symptoms, such that high levels of reactive aggression are associated with high levels of social problems, which in turn are associated with high levels of withdrawn/depressed symptoms. Findings suggest the need to target peer relationships in the prevention of subsequent negative emotions for children who exhibit high levels of reactive aggression.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Aggression is a risk factor for a host of problem behaviors in childhood, adolescence and adulthood, including negative emotions. In fact, there is literature supporting a link between child aggression and a multitude of negative emotions, such as depression, anxiety, and suicidal behavior (e.g., Grube 2004; Lochman and Wayland 1994; Zahn-Waxler et al. 2005). However, aggression is not a unidimensional construct (Coie and Dodge 1998), and not all types of aggressive behavior are linked to negative emotions (e.g., Card and Little 2006). Furthermore, the mechanisms that account for the link between aggression and negative emotions are not known. Identifying the types of aggressive behavior that are risk factors for negative emotions, as well as understanding the mechanisms that link subtypes of aggression to negative emotions, can aid in developing targeted prevention and intervention strategies for depressive symptoms and other negative emotions. Accordingly, the current study examined the link between reactive (impulsive) and proactive (goal-oriented) subtypes of aggression and withdrawn/depressed symptoms. Furthermore, the study examined social problems as a potential mediator of these associations in a sample of school age children.
Proactive and Reactive Aggression
A common way in which child aggression researchers subdivide aggressive behavior is by the function or motivation that drives the behavior, namely reactive and proactive aggression. Reactive aggression represents aggressive behavior that occurs in response to behavior that is perceived as hostile or intentional. An example of reactive aggression would be a child hitting another child after that child tripped him/her. Reactive aggression appears to be most consistent with the frustration aggression hypothesis, which postulates that aggressive behavior results from a hostile and angry reaction to frustration (e.g., Berkowitz 1978, 1989).
Proactive aggression, on the other hand, represents aggressive behavior that is goal oriented and calculated in nature. An example of proactive aggression is a child kicking a peer in order to acquire a desired object. Proactive aggression appears to be most consistent with social learning theory, which posits that one learns to use aggression in order to obtain a desired goal or object (Bandura 1973; Card and Little 2007).
In addition to being best described by different theories, reactive and proactive aggression have also been found to be differentially related to a host of social and behavioral outcomes (e.g., Card and Little 2006). More specific to the current study, research has linked reactive, not proactive, aggression to negative emotions across a multitude of studies (e.g., Card and Little 2006; Conner et al. 2003; Fite et al. 2009; Fite et al. 2010; Raine et al. 2006). For example, Dodge et al. (1997) found that reactive aggression was associated with more sadness in social situations than proactive aggression. Reactive aggression has also been found to be associated with less happiness than proactive aggression (Day et al. 1992). Moreover, Vitaro et al. (2002) found that reactive, not proactive, aggression is associated with depressive feelings. However, potential mechanisms that account for the relation between reactive aggression and negative emotions have not been examined. Understanding the factors that account for this relation is important, as identifying these factors can aid in the refinement of prevention and intervention strategies aimed at reducing the development of subsequent problem behavior.
One factor that may account for the relation between reactive aggression and negative emotions is social problems. Reactive, not proactive, aggression is linked to peer rejection and social isolation at all ages (e.g., Day et al. 1992; Dodge and Coie 1987; Dodge et al. 1997; Fite et al. 2007, 2008; Prinstien and Cillessen 2003). For example, reactive aggression has been found to be negatively associated with peer social status in kindergarten and first grade (Price and Dodge 1989). Furthermore, reactive, not proactive, aggression was found to be positively associated with sociometric ratings of peer rejection at 5th grade (e.g., Fite et al. 2007).
Social isolation is conceptualized as a stressful life event that can lead to distress and negative emotions (e.g., Bierman 2004; Dodge et al. 2003; Prinstein and Aikins 2004; Prinstein et al. 2000). Thus, reactive aggression may be associated with negative emotions, such as withdrawn/depressed symptoms, through social problems. That is, reactive aggression may lead to social problems, which results in experiencing withdrawn/depressed symptoms.
Current Study
In sum, the goal of the current was to examine the link between reactive (and proactive) aggression and withdrawn/depressed symptoms and determine whether social problems accounted for the link between reactive aggression and withdrawn/depressed symptoms in a sample of 147 children that attended an after school care program at a community based organization that services primarily low income families. The current study focused on a socioeconomically disadvantaged sample, as low socioeconomic status is a risk factor for aggression and other externalizing behavior (e.g., Dodge et al. 1994) as well as depressive symptomology (e.g., Gilman et al. 2003). Data was collected at baseline and 2-months later, allowing us to examine whether social problems mediated the link between reactive aggression and withdrawn/depressed symptoms above and beyond prior levels of withdrawn/depressed symptoms.
Methods
Participants and Procedures
Participants were recruited from a local community based organization that provides low-cost after school and summer care for approximately 250 school-age children. Data regarding 147 children was collected. Children ranged from 5 to 13 years of age (M = 8.22, SD = 1.99). Just over half of the children were male (54.4%). The majority of the sample was identified as African American (67%; 20.5% Caucasian, 5 % Hispanic/Latino, and 7.5% biracial or identified with another racial/ethnic group). The sample is representative of the population of children for which the organization provides services. The majority of study participants received a fee reduction (96%) for their children to attend the program, and 87% of the children received government assistance in paying fees. All of the children had been attending the program for at least 1 month, with over half of the children (58%) attending the program for more than a year. Most children (86%) attended the program daily, with only 7% attending the program on average 3 or fewer days per week.
Parental consent and staff consent were obtained prior to data collection, in accordance with institutional review board approval of the study. Caregivers provided consent for organization staff to answer questions regarding their children. Of importance to the current study, the education director reported on child behavior and peer relationships at baseline and 2 months later using Medialab interview software. The education director was provided a laptop for 2 weeks to respond to questions for children whose parents signed consent forms. Interviews were completed in less than 10 min per child and the education director was compensated $3.00 per child at each timepoint. Data from the education director was collected, because he had daily contact with study participants. He oversees all of their educational needs, which is a major component to the after school program. Additionally, the educational director also oversees many group activities and field trips that the children engage in. Finally, this individual also aids in providing bus transportation for the children (from schools to the afterschool program). As such, the education director had frequent direct interactions with the children within a multitude of social situations, providing ideal reports of behavior.
Measures
Proactive and Reactive Aggression
Proactive and reactive aggression were assessed using education director reports of the Dodge and Coie’s (1987) proactive and reactive aggression questionnaire. The questionnaire consists of 6 items, 3 items assessing proactive aggression and 3 items assessing reactive aggression. The education director responded to items using a 5-point likert scale (1 = never to 5 = almost always) at baseline. Subscales were averaged and used for analyses. This measure has been found to be reliable and valid (Dodge et al. 1997; Waschbusch et al. 1998). Internal consistencies of the scales were good (reactive aggression α = .99 and proactive aggression α = .98).
Social Problems
Social problems were assessed using education director reports of 4 items (Doesn’t get along with other kids, feels others are out to get him/her, gets teased a lot, and not liked by other kids) from the Teacher Report Form (Achenbach and Rescorla 2001). The education director responding using a 3-point likert scale (1 = Not True, 2 = Somewhat or Sometimes True, 3 = Very or Often True) at baseline. This subscale has been used in previous research and has been found to be related to other peer and social constructs (e.g., Fite et al. 2010), providing some evidence of construct validity. Items were averaged and used for analyses. Internal consistency of the scale was good (α = .91).
Withdrawn/Depressed Symptoms
Withdrawn/depressed symptoms were assessed using education director reports of the 8-items from the withdrawn/depressed syndrome scale of the Teacher Report Form (Achenbach and Rescorla 2001). The education director responded using a 3-point likert scale (1 = Not True, 2 = Somewhat or Sometimes True, 3 = Very or Often True) at baseline and 2-months later. This measure has been found to be valid and reliable (Achenbach and Rescorla 2001). Items were averaged and used for analyses. Internal consistencies of the scale at both timepoints were good (Time 1 α = .88; Time 2 α = .88).
Results
A structural equation model was estimated using Mplus 5.2 (Muthen and Muthen 2008) statistical software in order to evaluate whether social problems accounted for the relation between reactive aggression and withdrawn depressed symptoms. Skewness of all variables was less than 3 (−.17 to 2.09), suggesting that non-normality of the data was not a concern (Kline 2005). Furthermore, there was no missing data at either timepoint. Accordingly, maximum likelihood estimation was used (Muthen and Muthen 2008). The estimated model included all direct and indirect paths, which provides the most stringent test of mediation. This resulted in a fully saturated model (i.e., a model that has zero degrees of freedom). A fully saturated model always results in a perfect fit to the data. Accordingly, model fit indices are not reported.
The biased corrected bootstrap method was used to evaluate mediated paths. This method has been found to provide a more accurate balance between Type 1 and Type 2 errors than other methods used to test mediation, such as Sobel’s method (MacKinnon et al. 2004). Five hundred bootstrap samples and the 95% bias-corrected confidence intervals (CIs) were used to test the significance of indirect effects.
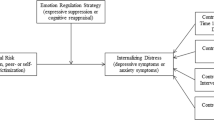
Age and gender were included as covariates in the model, as prior research has found age and gender differences in levels of aggression as well as levels of negative emotions (e.g., Achenbach and Rescorla 2001; Coie and Dodge 1998). Furthermore, due to the positive association between reactive and proactive aggression, proactive aggression was included in the model in order to evaluate unique relations with reactive aggression. Finally, the stability of withdrawn/depressed symptoms was also considered in the model. As seen in Fig. 1, age was positively associated with social problems, such that older children were more likely to experience social problems. Withdrawn/depressed symptoms were moderately stable over the 2-months. Reactive aggression was positively associated with social problems, which in turn predicted withdrawn/depressed symptoms at Time 2. Indeed, social problems mediated the relation between reactive aggression and withdrawn/depressed symptoms (B = .31, 95% CI = .08–.53). Proactive aggression, on the other hand, was unrelated to social problems or withdrawn/depressed symptoms.

Mediational model. Standardized parameter estimates are reported outside parentheses and unstandardized parameter estimates are reported inside parentheses. * p < .05. Covariances between exogenous variables were estimated but are not depicted for clarity purposes. Estimates for the disturbances (D1 and D2) are proportions of unexplained variance
Note that correlations between the exogenous variables in the model were also estimated, and findings were consistent with expectation. Noteworthy, withdrawn/depressed symptoms at Time 1 were positively associated with reactive aggression (r = .31; p = .01) but unrelated to proactive aggression (r = .20; p > .05). Additionally, proactive and reactive aggression were strongly positively related (r = .89; p = .00).
Discussion
The current study examined the role of social problems in the link between reactive aggression and withdrawn/depressed symptoms. As expected, findings suggested that reactive, not proactive, aggression was positively associated with social problems, which in turn predicted withdrawn/depressed symptoms while also controlling for prior levels of withdrawn/depressed symptoms, and the test of this indirect effects was statistical significant. That is, social problems mediated the link between reactive aggression and subsequent withdrawn/depressed symptoms. Findings are consistent with previous research linking reactive aggression to rejection and social isolation (e.g., Day et al. 1992; Dodge and Coie 1987; Dodge et al. 1997; Fite et al. 2007, 2008; Prinstien and Cillessen 2003) as well as literature linking both reactive aggression and social problems to negative emotions (e.g., Bierman 2004; Card and Little 2006; Conner et al. 2003; Dodge et al. 2003; Fite et al. 2009; Fite et al. 2010; Prinstein and Aikins 2004; Prinstein et al. 2000; Raine et al. 2006). However, to our knowledge, this is the first study to empirically evaluate whether social problems account for the relation between reactive aggression and withdrawn/depressed symptoms. Formally examining this relation is important, as it has many intervention implications for the prevention/treatment of child problem behavior. Findings suggest which aggressive individuals (i.e., reactively aggressive individuals) need to be targeted for the prevention of internalizing symptoms as well as social problems. Furthermore, findings indicate that targeting social relationships for reactively aggressive individuals can potentially prevent subsequent negative emotions.
It is important that the current finding be interpreted in light of the limitations associated with the current study. First, all data was paper and pencil assessments collected from a single informant, which may have inflated associations between study constructs. Note, however, that current findings are consistent with previous research. Nonetheless, future research should examine associations using multiple informants (e.g., parents, children, peers) and multiple types of assessments (e.g., observations). Furthermore, although the current study was longitudinal in nature, the timing in between assessments was brief (i.e., 2 months). Current findings suggest that reactive aggression is predictive of subsequent withdrawn/depressed symptoms above and beyond the stability of symptoms, and that social problems are accounting for this relation in the short-term. However, it would be useful for future research to determine if this relation holds true over longer periods of time. Finally, this study examined residual scores of proactive and reactive aggression. That is, the present study examined how proactive and reactive aggression were related to social problems and withdrawn/depressed symptoms once partialling out their shared variance. Due to the high correlation between these aggression subtypes, current findings may be quite different from data analytic strategies that do not partial out the common variance between proactive and reactive aggression (Miller and Lynam 2006).
Despite the aforementioned limitations, the current study has many implications for treatment and intervention as well as implications for future research. Current findings suggest the need for interventions to focus on peer relationships and perhaps social skills training for reactively aggressive youth in order to prevent subsequent negative emotions from developing. Future intervention studies that evaluate the effectiveness of targeting social problems for reactively aggressive individuals need to be conducted.
Additionally, there may be other potential mediators of the relation between reactive aggression and negative emotions that need to be examined. For example, reactive aggression is associated with harsh and abusive parenting (e.g., Dodge et al. 1997; Shields and Cicchetti 1998) and harsh parenting has been linked to negative emotions (e.g., Bender et al. 2007; Gershoff 2002). Thus, it may be useful for future research to examine whether the relation between reactive aggression and negative emotions is also accounted for by harsh discipline, along with other potential mediators.
References
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms and profiles. Burlington, VT: University of Vermont Department of Psychiatry.
Bandura, A. (1973). Aggression: A social learning analysis. Englewood Cliffs, NJ: Pretince-Hall.
Bender, H. L., Allen, J. P., McElhaney, K. B., Antonishak, J., Moore, C. M., Kelly, H. O. B., et al. (2007). Use of harsh physical discipline and developmental outcomes in adolescence. Development and Psychopathology, 19(1), 227–242.
Berkowitz, L. (1978). Whatever happened to the frustration-aggression hypothesis? American Behavioral Scientist, 32, 691–708.
Berkowitz, L. (1989). Frustration-aggression hypothesis: Examination and reformulation. Psychological Bulletin, 106, 59–73.
Bierman, K. L. (2004). Peer rejection: Developmental processes and intervention strategies. New York: Guilford.
Card, N. A., & Little, T. D. (2006). Proactive and reactive aggression in childhood and adolescence: A meta-analysis of differential relations with psychosocial adjustment. International Journal of Behavioral Development, 30, 466–480.
Card, N. A., & Little, T. D. (2007). Differential relations of instrumental and reactive aggression with maladjustment: Does adaptivity depend on function? In P. H. Hawley, T. D. Little, & P. C. Rodkin (Eds.), Aggression and adaptation: The bright side to bad behavior (pp. 107–134). Mahwah, New Jersey: Lawrence Erlbaum.
Coie, J. D., & Dodge, K. A. (1998). Aggression and antisocial behavior. In W. Damon & N. Eisenberg (Eds.), Handbook of child psychology: Vol 3, social, emotional, and personality development (pp. 779–862). New York: Wiley.
Conner, K. R., Duberstein, P. R., Conwell, Y., & Caine, E. D. (2003). Reactive aggression and suicide: Theory and evidence. Aggression and Violent Behavior, 8, 413–432.
Day, D. M., Bream, L. A., & Pal, A. (1992). Proactive and reactive aggression: An analysis of subtypes based on teacher perceptions. Journal of Clinical Child Psychology, 21, 210–217.
Dodge, K. A., & Coie, J. D. (1987). Social-information-processing factors in reactive and proactive aggression in children’s peer groups. Journal of Personality and Social Psychology, 53, 1146–1158.
Dodge, K. A., Pettit, G. S., & Bates, J. E. (1994). Socialization mediators of the relation between socioeconomic status and child conduct problems. Child Development, 65, 649–665.
Dodge, K. A., Lochman, J. E., Harnish, J. D., Bates, J. E., & Pettit, G. S. (1997). Reactive and proactive aggression in school children and psychiatrically impaired chronically assaultive youth. Journal of Abnormal Psychology, 106, 37–51.
Dodge, K. A., Lansford, J. E., Burks, V. S., Bates, J. E., Pettit, G. S., et al. (2003). Peer rejection and social information-processing factors in the development of aggressive behavior problems in children. Child Development, 74(2), 374–393.
Fite, P. J., Colder, C. R., Lochman, J. E., & Wells, K. C. (2007). Pathways from proactive and reactive aggression to substance use. Psychology of Addictive Behaviors, 21, 355–364.
Fite, P. J., Colder, C. R., Lochman, J. E., & Wells, K. C. (2008). The relation between childhood proactive and reactive aggression and substance use initiation. Journal of Abnormal Child Psychology, 36, 261–271.
Fite, P. J., Stoppelbein, L., & Greening, L. (2009). Proactive and reactive aggression in a child psychiatric inpatient population. Journal of Clinical Child and Adolescent Psychology, 38, 199–205.
Fite, P. J., Raine, A., Stouthamer-Loeber, M., Loeber, R., & Pardini, D. A. (2010). Reactive and proactive aggression in adolescent males: Examining differential outcomes 10-years later in early adulthood. Criminal Justice and Behavior, 37, 141–157.
Gershoff, E. T. (2002). Corporal punishment by parents and associated child behaviors and experiences: A meta-analytic and theoretical review. Psychological Bulletin, 128(4), 539–579.
Gilman, S. E., Kawachi, I., Fitzmaurice, G. M., & Buka, S. L. (2003). Family disruption in childhood and risk for adult depression. American Journal of Psychiatry, 160, 939–946.
Grube, M. (2004). Which types of aggressive behavior are associated with suicidal and self-injurious behaviour at the time of admission? Psychopathology, 37, 41–49.
Kline, R. B. (2005). Principles and practice of structural equation modeling, 2nd edition. New York: Guilford Press.
Lochman, J. E., & Wayland, K. K. (1994). Aggression, social acceptance, and race as predictors of negative adolescent outcomes. Journal of the American Academy of Child and Adolescent Psychiatry, 33, 1026–1037.
MacKinnon, D. P., Lockwood, C. M., & Williams, J. (2004). Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research, 39, 99–128.
Miller, J. D., & Lynam, D. R. (2006). Reactive and proactive aggression: Similarities and differences. Personality and Individual Differences, 41, 1469–1480.
Muthen, L. K., & Muthen, B. (2008). Mplus: The comprehensive modeling program for applied researchers. Los Angeles, CA: Muthen & Muthen.
Price, J. M., & Dodge, K. A. (1989). Reactive and proactive aggression in childhood: Relations to peer status and social context dimensions. Journal of Abnormal Child Psychology, 17, 455–471.
Prinstein, M. J., & Aikins, J. W. (2004). Cognitive moderators of the longitudinal association between peer rejection and adolescent depressive symptoms. Journal of Abnormal Psychology, 32(2), 147–158.
Prinstein, M. J., Boergers, J., Spirito, A., Little, T. D., & Grapentine, W. L. (2000). Peer functioning, family dysfunction, and psychological symptoms in a risk factor model for adolescent inpatients’ suicidal ideation severity. Journal of Clinical Psychology, 29(3), 392–405.
Prinstien, M. J., & Cillessen, A. H. N. (2003). Forms and functions of adolescent peer aggression associated with high levels of peer status. Merrill-Palmer Quarterly, 49, 310–342.
Raine, A., Dodge, K. A., Loeber, R., Gatzke-Kopp, L., Lynam, D., Reynolds, C., et al. (2006). The reactive-proactive aggression questionnaire: differential correlates of reactive and proactive aggression in adolescent boys. Aggressive Behavior, 32, 159–171.
Shields, A., & Cicchetti, D. (1998). Reactive aggression among maltreated children: The contributions of attention and emotion dysregulation. Journal of Clinical Child Psychology, 27, 381–395.
Vitaro, F., Brendgen, M., & Tremblay, R. E. (2002). Reactively and proactively aggressive children: antecedent and subsequent characteristics. Journal of Child Psychology and Psychiatry, 43, 495–505.
Waschbusch, D. A., Willoughby, M. T., & Pehlam, W. E. (1998). Criterion validity and the utility of reactive and proactive aggression: Comparisons to attention deficit hyperactivity disorder, oppositional defiant disorder, oppositional defiant disorder, and other measures of functioning. Journal of Clinical Child Psychology, 27, 396–405.
Zahn-Waxler, C., Park, J. H., Essex, M., Slattery, M., & Cole, P. (2005). Relational and overt aggression in disruptive adolescents: prediction from early social representations and links with concurrent problems. Early Education and Development, 16(2), 259–282.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fite, P.J., Rathert, J.L., Stoppelbein, L. et al. Social Problems as a Mediator of the Link Between Reactive Aggression and Withdrawn/Depressed Symptoms. J Child Fam Stud 21, 184–189 (2012). https://doi.org/10.1007/s10826-011-9461-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-011-9461-4