
Abstract
Although a growing body of literature has examined wraparound implementation and fidelity, child and family team (CFT) members’ levels of participation and the consistency of their attendance have not been systematically examined. This study explored the relationship between CFT member attendance consistency and the fidelity of wraparound team level implementation processes in a System of Care (SOC). Specifically, utilizing Participant Rating Form (PRF) data collected from caregivers, facilitators, youth, supportive persons, and service providers, as well as meeting attendance records, the relationship between team attendance consistency and fidelity of wraparound implementation was explored. Records for 88 teams, with a total of 2,643 members’ ratings of CFT meetings between 2004 and 2009, were examined. Analyses indicate that the structural team factors of attendance consistency and mean team members present relate to CFT members’ ratings of team functioning and the degree to which meeting processes are consistent with the tenets of wraparound. Team attendance variables related to the views of meeting functioning by facilitators, service providers, and caregivers, the individuals most often responsible for implementation of the plan of care, but not ratings by youth or supportive persons. These findings have implications for policy and the successful implementation of wraparound, underscoring the relevance of attending to and tracking the composition of the CFT and more actively encouraging consistent meeting attendance. Results also highlight the need to measure structural variables that may have salience in fidelity and implementation assessments and, more globally, the effectiveness of SOCs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Wraparound, the process by which families and professionals work in collaboration to help plan and implement services, has become the dominant practice model for providing services for children with severe emotional disturbances and their families (Faw 1999), particularly within Systems of Care (SOCs; Hernandez 2003; Stroul and Friedman 1986). The wraparound model consists of ten principles, including a team-based model for planning and implementation of services (Suter and Bruns 2009). These child and family teams (CFTs) are a central component of wraparound implementation. However, growing evidence suggests that the complex set of processes that define wraparound (Burns and Goldman 1999; VanDenBerg and Grealish 1996) are not implemented consistently, even in SOCs where the model is most supported. In fact, research suggests that many CFTs do not engage in many of the practices and processes considered central to wraparound implementation (Bruns et al. 2007; Cook et al. 2008; Walker and Schutte 2005). Although a growing body of literature has examined fidelity of wraparound implementation, factors that contribute to fidelity, and the relationship between fidelity and child and family outcomes, the importance of such factors as the level and stability of team members’ participation over time have not been systematically examined.
In a monograph produced by The National Implementation Research Network (NIRN; Fixsen et al. 2005), the authors synthesize the implementation literature across disciplines and describe core intervention components, stages of implementation, and outcomes for implementation or intervention. They also detail the multiple levels of influences on successful implementation, i.e., implementation components, organizational and contextual influences, and macro-level factors such as political and social influences (Fixsen et al. 2005). Research on SOCs and on wraparound have addressed these various elements with some variability, though evaluation of wraparound fidelity as a way of improving implementation has been the focus of much attention (Bertram et al. 2010). The examination of factors relevant to wraparound implementation (both structural and process variables) can identify areas for improvement, as well as areas in need of further research. Indeed, ongoing fidelity evaluation can serve as a critical feedback mechanism to highlight training and coaching needs and, over time, can help ensure continued implementation of core components of a model or approach (see Fixsen et al. 2005). Although “outcomes” of interventions, programs, or system-change efforts typically garner a greater level of interest, such findings are not adequately grounded if the fidelity of implementation has not been established. Thus, in the stages of early implementation of a program, intervention, or systems-level effort, process evaluation serves the necessary function of aiding administrators and providers in honing in on areas in need of attention and, subsequently, informing recommendations for changes. Identifying key indicators in the early implementation stage is particularly necessary, because such work can help determine if the program or larger-scale initiative has been implemented successfully (Wiseman et al. 2007), and there is typically more flexibility and opportunity for modifications to service provision or system function (Fixsen et al. 2005).
Of particular relevance to the factors investigated in the present study, Walker and Schutte (2003) suggested that effective teamwork is a key process variable in achieving wraparound implementation. In order for a team to work together to address the diverse and dynamic needs of a child and family effectively, rapport and trust with family members are essential, as are knowledge of the family’s dynamics, understanding of the nature and impact of the prior interventions, and a careful monitoring of the family’s changing needs. Teams whose members change frequently, or who participate only sporadically, might have difficulty working together as a team to develop and monitor well-targeted, individualized service plans with families. Better understanding of ways that team participation and involvement relate to team functioning has important implications for policy surrounding the development of SOCs and the ways that wraparound planning processes are supported. This paper examines the relationship between the consistency of team member participation over time and the degree to which those teams implement processes that reflect high fidelity wraparound.
Wraparound Implementation and Fidelity
The implementation process for a program, treatment model, or system change effort typically requires modifications, adjustments and/or changes in operations (Fixsen et al. 2005). Evaluating practices and processes can identify potential areas for improvement and system level issues which may be hindering successful implementation (Centers for Disease Control 2009). The growing emphasis on the wraparound approach as a prescribed practice model within federally-funded SOCs has led to efforts to increase the specificity of the approach (e.g. see National Wraparound Initiative), and research has increasingly focused on the degree to which implementation is consistent with the tenets of wraparound (Bruns et al. 2007; Bruns et al. 2004; Bruns et al. 2005). Examining wraparound fidelity is particularly salient for efforts to advance wraparound practice, because regular feedback about practice is essential for quality improvement efforts. Furthermore, systematic assessment of fidelity enables more rigorous research regarding the degree to which wraparound, and variations in wraparound fidelity, can help meet the needs of children and families. The wraparound practice model operationalizes core characteristics and values of service provision such as strengths-based planning, individualized services and supports, and collaboration. Because CFT meetings represent a periodic (i.e., monthly or more frequent) and critical component of the wraparound process, examining these meetings and participants’ experiences of them constitutes a prime means of assessing fidelity to the model. In defining implementation, Fixsen et al. (2005, p. 5) underscore the weight of “the ‘specific set of activities’ related to implementation,” and the CFT meeting is an accessible and potentially fruitful context for investigating those activities.
To that end, multiple mechanisms, including surveys of team participants (Bruns et al. 2008; Cook et al. 2007), observations of team meetings (Davis and Dollard 2004; Epstein et al. 2003), and expert observations of videotaped meetings (Walker and Schutte 2005) have been used to assess wraparound fidelity. Studies using different means of assessing fidelity have reported consistent findings regarding the aspects of wraparound that are challenging to teams, and there is increasing evidence that higher levels of fidelity relate to better child and family outcomes (Bruns et al. 2005; Haber et al. 2010; Hemphill et al. 2010).
Efforts to increase fidelity have largely focused on changing the knowledge, attitudes, and skills of team members (e.g., Rast and Bruns 2003), focusing on one key component of implementation (staff training). As Rast and Burns (2003) note, administrators, professionals and families alike find the wraparound approach difficult to implement. This may be due, at least in part, to the lack of consensus “regarding the types, techniques, processes, or procedures that translate the value base into practice at the team level” (Walker and Bruns 2003; Walker and Schutte 2004, p. 182). In addition, the potential influence of key structural elements of CFTs, such as the size, composition, and levels of participation, has only begun to be explored and may provide indicators of successful program installation. For example, a recent effort (Wright et al. 2006) examined the relationship between team structure and achievement of treatment goals. Using social network analysis, the researchers concluded that teams with between 4 and 7 members had the greatest impact on positive youth outcomes, and having multiple family members and the presence of fathers and educators on CFTs related positively to the team’s ability to meet treatment goals (Wright et al. 2006). Consideration of these types of structural elements, and ensuring that necessary resources are in place, could have important implications for improving the implementation of wraparound.
Team Attendance Consistency
For the purposes of this study, team attendance consistency is defined as having the same set of individuals present at each team meeting from meeting to meeting. Although research on the effects of team attendance consistency is scarce, work across multiple contexts suggests that team member turnover and consistency of participation relate to the ability of teams to accomplish their goals (Delva et al. 2008). For instance, among dual diagnosis treatment teams in hospitals, inconsistency in team member involvement due to frequent staff changes was associated with discontinuities of care (Woltmann and Whitley 2007). Similarly, an exploration of retention and turnover among child welfare and human service workers found that high turnover impeded effective delivery of services, disrupted continuity of care, and contributed to the deterioration of rapport with those served (Barak et al. 2001). Moreover, in a study of team factors that contribute to collaboration in parent and service provider teams working to treat children with special needs, collaboration was enhanced when service coordinators had regular and consistent contact with families (Dinnebeil et al. 1999). Notably, caregivers specifically identified turnover among service providers as a key factor that detracted from collaboration and care (Dinnebeil et al. 1999).
CFTs, which can include a diverse array of professionals, family members, and supportive community members, may be especially vulnerable to variability in participation, since turnover has been found to occur more frequently in teams with heterogeneous team members (Jackson et al. 1991). Furthermore, inconsistency of member participation can have particularly negative consequences in wraparound, since implementation of team goals may depend on the actions of individual team members, and teams often meet only once a month or less frequently. In addition, inconsistent participation would likely have a negative impact on team cohesion, the set of feelings and relationships that induce group members to continue to work as part of a group (Mullen and Cooper 1994). Although training has been found to buffer the effects of changes related to turnover on teams, it would appear that team consistency could have a meaningful influence on the fidelity of wraparound and, in turn, the degree to which wraparound teams are able to address the needs of children and families.
The Present Study
This study examines the relationship between CFT attendance consistency and the fidelity of wraparound team processes in a federally-funded SOC. Archival records of attendance by team members at CFT meetings were examined to assess the degree to which teams evidenced consistency in member attendance. Team attendance consistency was then examined in relation to team member ratings of the fidelity of implementation of wraparound in two domains, reflecting team functioning and team cohesion. Given the many findings that link fluctuations in team attendance to poor outcomes, such as the failure of teams to meet treatment goals (Barak et al. 2001; Delva et al. 2008; Goodman and Patrick-Leyden 1991; Woltmann and Whitley 2007), we expected that inconsistent team attendance would have a negative effect on team members’ perceptions of wraparound fidelity.
Method
Procedures
Data were gathered between July 2004 and April 2009 as part of the ongoing evaluation of MeckCARES, the SOC serving children and families in Mecklenburg County, NC. This evaluation includes regular assessment of CFT functioning as an indicator of wraparound fidelity, using the Participant Rating Form (PRF; described below in Measures), administered at the end of CFTs, as the main measure of team members’ perceptions of the meeting (Cook et al. 2007, 2008). Additionally, team attendance consistency data were gathered from sign-in sheets that team facilitators handed out during the team meeting to record attendance. Participants’ roles and agency affiliation were included in the sign-in sheet, but no demographic information was obtained, nor was information provided regarding the degree to which members participated on other CFTs.
Measures
Child and Family Team Functioning
The Participant Rating Form (PRF) assesses team functioning and wraparound fidelity (Cook et al. 2007) and constitutes the study’s primary measure of interest. This brief measure was designed through collaboration among parents, youth, service providers and academics and has been found to be a reliable and valid method of assessing team functioning and the fidelity of wraparound team meetings (Cook et al. 2007, 2008). The PRF is administered at the conclusion of each CFT meeting. There are five separate versions for parent/caregivers, youth, team facilitators, service providers, and informal supportive persons. The PRF forms consist of 21–28 items, depending upon form, and assesses multiple elements of team process, such as the team’s focus on strengths of the child and family, meeting organization, and team cohesion. Items were designed to focus on participants’ perceptions of what took place at the meeting (e.g., the parent felt heard; participants know what to do) as opposed to observable characteristics of the meeting (e.g., the presence of a written agenda) that can better be captured through records and/or observations (Cook et al. 2007). Each item is rated on a four-point scale (1 = not at all true; 4 = very true). The PRF has been found to be consistent with the ratings of outside observers at the same meetings (Cook et al. 2007, 2008), and with findings from other studies that have assessed wraparound fidelity (e.g., Bruns et al. 2005; Epstein et al. 2003).
Previous principal components analysis of PRF items (e.g., Hemphill 2009) identified a 3-factor solution, with 2 primary factors of relevance to the present study: Team Functioning (TF) and Team Cohesion (TC). TF includes the degree to which the team focused on the child’s strengths, created a plan that addressed the needs of the child and the family, implemented the plan, and considered potential barriers to the plan (Cronbach’s alphas range from .78 to .88 for different types of raters). TC refers to the degree to which the team members perceived they were heard, believed the team functioned collaboratively, and experienced their fellow team members as sensitive to their culture (Cronbach’s alphas range from .76 to .85 for different types of raters). Overall team ratings of TC and TF have been found to be moderately correlated (r = .67). Recent work has demonstrated that PRF scores are associated with improvements in youth functioning (Haber et al. 2010; Hemphill et al. 2010).
Team Attendance Consistency
Team attendance consistency information, gathered from attendance records from each CFT, was used to predict wraparound fidelity scores. Attendance records included names, roles, and affiliation for team members present at each CFT. These data were coded by date, team, team member, and team member role. Each team was assigned a unique identifying number as was each team member. Team member numbers were coded such that they could be linked to specific teams and meeting dates.
Preliminary Analysis: Team Meeting Data and Criteria for Inclusion
First, data for each team meeting were included for this study only for teams for which both team attendance data and PRF data were available. Team facilitators are responsible for ensuring that data are collected at the end of each meeting, but many team facilitators did not do this consistently. Furthermore, the presence of these data are the only record of whether or not a CFT occurred. Consequently, there is no way to know how many meetings occurred for which no data were available, and no way to determine differences between teams providing data at any given point in time versus teams that did not provide data.
Utilizing the data available regarding CFT attendance, a series of tables was developed, for each team, which listed each team member by row, team meeting dates by column, and a count of the number of team meetings each team member attended for the time period. The data from these tables allowed for the calculation of multiple team member attendance factors for each CFT. For example, these data allowed us to track changes in team member attendance from meeting to meeting as well as calculate aggregate data such as mean number of meeting attendees over a given time period.
CFTs ideally meet every month; however, it is not unusual for scheduling conflicts, holidays, and other family business to interfere with these efforts. In order to reduce potential confounds such as gross changes in team membership and substantial differences in team goals inherent in long gaps between team meetings, a decision rule was established such that teams were only included when data were available for at least 4 meetings, and there was no more than a calendar month without a meeting between any two meetings. For example, if a team met in January, February, March and May in a given year, data for that team were included since only 1 month without a meeting occurred between meetings. If a team held meetings in January, February, March and June in a given year, data for that team were not included in this study, since there was a two-month meeting gap between the March and June meetings. Since the first meeting served as a baseline meeting from which the following meetings are then compared, this process insured that each team had a minimum of 3 subsequent meetings from which to draw data.
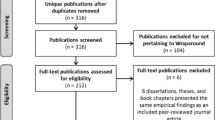
Of 292 CFTs from which attendance data were available, 272 had 4 or more meetings, 131 teams had 4 or more meetings that met criteria for regularity outlined above. Of these, 88 teams met all the above criteria and had matching PRF data available. For those 88 teams, a total of 2,643 PRF forms were collected and used here, including 541 caregiver respondents, 629 facilitators, 350 youth, 164 supportive persons, and 959 service providers. Team meetings occurred between July 2004 and April 2009. For those CFTs that met criteria, teams had between 4 and 23 meetings that met criteria for regularity (M = 7.09, SD = 3.47) and between 4 and 41 total team members (M = 11.66, SD = 6.28) who had attended any meeting during the time period. A separate analysis of team meetings from the same system found that teams, on average, had 4.4 people attending each meeting (Hemphill et al. 2010).
Preliminary correlations, followed by a series of hierarchical regressions, were run to test the degree to which various indicators of membership attendance and consistency were associated with team members’ ratings of wraparound fidelity. These potential indicators included mean number of team member attendees present over time, mean members in common from one meeting to the next, change in number of attendees from meeting to meeting, mean consistency percentage (the proportion of total team members at a given meeting who were also present at the previous meeting for that team), mean number of meetings attended by team members, total meetings for time period and total team members present for time period. Following these exploratory analyses, two prime criteria were used in evaluating these indicators: (1) the strength of the variable’s relationship with the factors assessing fidelity/team functioning, and (2) the unique contribution of the variable to the factors assessing fidelity/team functioning. Put another way, we sought to identify variables that evidenced the strongest association with wraparound fidelity but that did not have a high degree of intercorrelation with the other selected variable(s). Thus, while mean number of members in common from one meeting to the next is a ‘face valid’ indicator of attendance consistency and may evidence a stronger association with PRF scores, it also correlated highly with mean consistency percentage, raising issues of multicollinearity and reducing the likelihood of detecting active variables in subsequent regression analyses. On the basis of these criteria, two team attendance indicators were identified for use in subsequent analyses: (1) Mean Consistency Percentage, which reflects the proportion of total team members at a given meeting who were also present at the previous meeting for that team, and (2) Mean Number of Team Members Present, reflecting the average number of participants at a team’s meetings over time.
Results
Core Analyses
As illustrated in Table 1, correlations indicated that both team attendance indicators related significantly to ratings of wraparound fidelity. Mean Consistency Percentage was associated positively with the total PRF ratings (i.e., across all form types). Mean Number of Team Members Present was associated negatively with total PRF ratings, indicating that the more members a team had, the lower their overall team scores on meeting fidelity. To better explore the association between team attendance and fidelity ratings, hierarchical multiple regression analyses were conducted with Mean Consistency Percentage and Mean Number of Team Members Present entered together as the potential predictors of the PRF total scores. These analyses revealed that, when entered together, team attendance variables contributed significantly to the variance in PRF ratings averaged across all form types (Adjusted R 2 = .11, F(85) = 6.35, p < .01). In the model including both team attendance indicators, Mean Consistency Percentage (β = .34, p < .01) significantly contributed to total PRF ratings, but Mean Number of Team Members Present (β = −.01, p = .30) did not.
Mean Consistency Percentage and Mean Number of Team Members Present were then entered together as potential predictors of the PRF subscales Team Functioning (TF) (Adjusted R 2 = .10, F(85) = 5.59, p < .01) and mean Team Cohesion (TC) (Adjusted R 2 = .04, F(85) = 2.60, p = .08). The model predicting TF was significant, and Mean Consistency Percentage (β = .35, p < .01) significantly contributed to total TF ratings, but Mean Number of Team Members Present (β = −.01, p = .32) did not. Neither Mean Consistency Percentage (β = .11, p = .43) nor Mean Number of Team Members Present (β = −.03, p = .09) were significant predictors of mean TC ratings across team member types.
As an additional step, correlations were run for total PRF rating scores and the different types of team members (see Table 2). Although there were some significant correlations among raters, most notably of the adult respondents, scores were sufficiently different to warrant using the five rater types separately. As a next step, Mean Consistency Percentage and Mean Number of Team Members Present were entered at the same step in a series of regression analyses to assess the association between team member attendance factors and the TF and TC subscales for each of the PRF form types. Given findings from previous investigations that suggest that there might be an ideal number of team members that would most significantly relate to fidelity (Wright et al. 2006), for those analyses in which Mean Team Members Present were significantly associated with TC and TF additional analyses (not detailed here) explored the possibility of curvilinear effects. However, no significant effects were identified.
Team Facilitators
For ratings of the meeting by team facilitators, Mean Consistency Percentage significantly contributed to the model predicting Team Functioning (TF) (β = .36, p < .01) and Team Cohesion (TC) (β = .31, p < .01); however, Mean Team Members Present did not significantly contribute to the models predicting TF (β = −.05, p = .67) or TC (β = −.08, p = .49). Together Mean Consistency Percentage and Mean Team Members Present accounted for 12% of the variance in team facilitator TF ratings (F(85) = 7.05, p < .01) and 10% of the variance in team facilitator TC ratings (F(85) = 5.74, p < .01).
Service Providers
Both Mean Consistency Percentage (β = .29, p < .01) and Mean Team Members Present (β = −.24, p < .05) related significantly to service providers’ ratings of TF, together accounting for 17% of the variance in TF scores for service provider respondents (F(85) = 9.95, p < .01). With both attendance variables included in the model, Mean Team Members Present related significantly to TC (β = −.29, p < .05), but Mean Consistency Percentage did not (β = .07, p = .56). The model including both team attendance variables accounted for 8% of the variance in service provider TC ratings (F(85) = 4.58, p < .05).
Caregivers
For caregivers, neither Mean Consistency Percentage (β = .12, p = .32) nor Mean Number of Team Members Present (β = −.13, p = .29) significantly related to TF (F(85) = 1.77, p = .18). Mean Team Members Present was significantly related to TC (β = −.29, p < .05), but Mean Consistency Percentage was not (β = .03, p = .77). Together, the team attendance variables accounted for a total of 7% of the variance in caregiver TC ratings (F(85) = 4.23, p < .05).
Supportive Persons
Regression analyses revealed that the two attendance variables failed to significantly predict TF or TC ratings by supportive persons. That is, when entered together, neither Mean Consistency Percentage (β = .14, p = .39) nor Mean Team Members Present (β = .14, p = .37) were significantly related to supportive person TF ratings (F(85) = .63, p = .54). Furthermore, Mean Consistency Percentage (β = .13, p = .40) and Mean Team Members Present (β = −.06, p = .69) were not significantly related to supportive person TC ratings. Together the two team attendance variables did not account for meaningful variance in supportive person TC ratings (F(85) = .56, p = .57).
Youth
Neither attendance variable contributed meaningfully to models predicting youth ratings of team fidelity. When entered together, Mean Consistency Percentage (β = .05, p = .88) and Mean Team Members Present (β = −.03, p = .48) were not significantly related to youth TF score. Likewise, the model including both Mean Consistency Percentage (β = −.28, p = .51) and Mean Team Members Present (β = −.05, p = .31) did not relate to youth TC scores. When entered in the same model, the two team attendance variables did not account for meaningful variance in youth TF ratings (F(85) = .35, p = .70) or youth TC scores (F(85) = .56, p = .57).
Overall, as reflected in Table 3, results indicate that team attendance factors relate most strongly to professionals’ ratings of CFT wraparound fidelity. More specifically, team attendance factors appear to have a significant impact on both team facilitator and service provider PRF scores. Mean Consistency Percentage, or having the same team members present from meeting to meeting, was found to have significant impact on team facilitator ratings of wraparound fidelity. For service providers, team attendance consistency and mean number of team members present were significantly associated with their perceptions of how well the team functions or operates in a manner consistent with high fidelity wraparound. Mean Team Members Present was also significantly associated with service provider’s ratings of team cohesion. Caregivers’ ratings of team cohesion were also negatively associated with mean number of team members present. However, results failed to reveal an association between team attendance variables and youth or supportive persons’ ratings of wraparound fidelity.
Discussion
This study sought to examine the influence of team attendance consistency on CFT member perceptions of team functioning and wraparound fidelity. In essence, the study sought to examine a structural aspect of wraparound implementation (e.g., team member attendance and the continuity of members’ participation) to gain a better understanding of the effects of process level variables on model implementation. To our knowledge, it is the first study to examine the degree to which consistent meeting attendance of CFT members relates to CFT functioning over time. Drawing from over 2,600 separate ratings by members of 88 CFTs, its most basic finding is that these structural variables (i.e., Mean Consistency Percentage and Mean Team Members Present) appear relevant to CFT members’ views of (a) how well the team functions as a cohesive team, and (b) the degree to which the practices and processes of the team are consistent with the values and tenets of wraparound. Of the diverse respondents, it appears that the views of the meeting by the professional members of the team, including the facilitators of the meetings, were most closely related to the size of the team and the consistency of team member participation. This is not surprising, given that these individuals are most often responsible for implementation of critical components of the plan of care. These findings suggest that having a core set of team members who regularly attend team meetings may facilitate team functioning and cohesion and aid in accomplishing team goals. Furthermore, consistent with the findings of Wright et al. (2006), keeping teams relatively small may relate to higher attendance rates and greater fidelity.
Several explanations for the differential relationships between team participation and fidelity across team members seem plausible. For facilitators, having frequent changes in team member attendance may negatively affect perceptions of both team functioning and team cohesion variables of wraparound fidelity. Other than youth and family, team facilitators such as case managers and SOC coaches are the team members most likely to have the longest tenure on CFTs and, therefore, they may be the professionals most familiar with the history and needs of the family. The responsibility for following up and ensuring that the plan of care is being implemented as agreed upon by the team often rests on the team facilitator. Indeed, because the facilitator is the person most responsible for managing the meeting processes, a lack of consistency among team members and having more members to keep informed over time would likely lead to a greater sensitivity by facilitators to these factors. Moreover, frequent team member turnover may result in larger workloads for team facilitators, the team members who may be most likely to assume responsibility for taking over identified strategies in the plan of care. Consistent with other explorations (Barak et al. 2001; Woltmann and Whitley 2007), these findings indicate that frequent absences or changes in membership may disrupt implementation of the plan of care and may interfere with establishing rapport among team members.
Service providers’ impressions of wraparound are also affected by team attendance factors. Given the difficulties many teams have in including informal supports (Cook et al. 2007; Epstein et al. 2003; Walker and Schutte 2005), considerable weight for implementation of components of the plan of care likely falls on service providers, a factor that may relate to the degree to which team attendance variables influence their perceptions of the team. Beyond that possibility, it is notable that service providers rated fidelity lower as teams became larger. It is, of course, important that those individuals who are involved in decision-making about or providing care for the system-identified youth need to be at the meeting; nevertheless, this finding is consistent with Wright et al. (2006) suggestion that having smaller teams may not only make practical sense, it may contribute to greater fidelity to wraparound. That is, if a team consists of 4 or 5 members, consistent attendance and follow up will be easier to achieve. Steps to ensure that team members are all “on the same page” will also likely be more straightforward on a smaller team.
Caregivers’ ratings of team cohesion are also influenced by team size. Caregivers reported less team cohesion as teams became larger. This finding may indicate that caregivers have a more difficult time feeling connected and heard within larger CFTs. In many cases, as teams increase in number of participants, their growth does not relate to an inclusion of informal or natural supports; rather, they will more typically involve a higher number of professionals, a factor that may leave caregivers feeling outnumbered by representatives of “the system”. These notions are consistent with prior studies suggesting that establishing rapport with families may be more difficult in large teams (Wright et al. 2006).
Our study failed to find an association between team attendance factors and youth and supportive persons’ ratings of fidelity. The fact that we did not detect these associations may relate to the present study’s foci on two prime aspects of team structure: attendance consistency and team size. It is possible that these are not the characteristics of team structure most salient to youth and supports. Alternatively, it may be that wraparound factors other than team structure are more important to youth and supportive persons. The PRF is designed to address aspects of wraparound specific to team interaction and plan implementation. Youth may benefit from adherence to the wraparound model while finding one on one interaction with therapists and case managers to be more comfortable and beneficial than the dynamics of the CFT. Unfortunately, supportive persons are the types of team members least likely to participate in CFT meetings (e.g., Cook et al. 2007; Epstein et al. 2003). They may not attend enough meetings to fully engage in CFTs, or we may simply not have enough data on these participants to detect an association. Given that the youth is the primary focus of the SOC approach and that supportive persons are integral members of CFTs (VanDenBerg and Grealish 1996), more research is needed to better understand youth and supportive persons’ impressions of wraparound fidelity.
Study Limitations and Directions for Future Research
The current study begins to illuminate the relationship between team attendance consistency and wraparound fidelity; however, this study is limited in several ways. Although we utilized data from a large number of team meetings and team members, we used only one measure of wraparound fidelity that focuses on implementation of wraparound in the team meeting. This measure, like many self-report measures of group processes, has a fairly restricted range of scores. Nonetheless, the measure, despite this limitation, has been found to be related to child outcomes (Hemphill et al. 2010). In addition, even though the overall variance explained by these measures of team structure may be considered relatively low, accounting for 7–17% of the variance in some areas suggests that these factors may be of practical significance in efforts to improve wraparound fidelity. Future studies may address other aspects of wraparound fidelity or expand to assess not only team functioning and fidelity, but the impact of team structure on child and family outcomes. Moreover, because our data were all collected from one site, it is unknown if findings can be generalized to other SOC sites. Expanding the study of team attendance to other SOC sites would be beneficial to understanding the impact of team structure on fidelity to the wraparound model. Finally, although we have begun to establish a connection between team structure and wraparound fidelity, there is still much to be learned.
The present study investigated consistency of attendance only, and our fidelity instrument is designed to measure only certain kinds of fidelity that can be identified in the context of a CFT meeting. Attendance is most certainly not the only consistency measure that might be important or related to fidelity. One can easily conceive that consistency of tone or consistency in delivering on services or promises to the family might be of relevance. Given that different team members’ ratings of fidelity appear to be affected by attendance variables, our hope is that this study will serve as a starting point from which to investigate the relationship between attendance and consistency further.
Another limitation of this study is that the data were coded such that an individual team member was associated by number with a particular team. If there were team members such as facilitators associated with multiple teams there is no way to track that with the current data. Future studies might include data collection that identifies individuals across teams to address possible confounds associated with nesting.
Future efforts could also include examinations of different types of attendance. For instance, future studies could investigate the impact of the presence or absence of particular team members on other team members, CFTs, and fidelity. Reasons for team member turnover or absence might also be studied to better understand how organizational or more macro-level (e.g., system) policies and procedures could best address these gaps in attendance.
Implications for Policy and Practice
This is the first study that investigates longitudinal CFT attendance and its impact on wraparound fidelity and implementation. These results highlight the need to measure structural variables that may have salience in fidelity assessments and, more globally, the effectiveness and impact of wraparound. They also underscore the relevance of attending to and tracking the composition of the CFT and more actively encouraging meeting attendance. Furthermore, given recent findings that the fidelity of wraparound implementation at child and family team meetings (i.e., rated at the team meeting level) relates to child outcomes (Haber et al. 2010; Hemphill et al. 2010), meeting size and consistency become particularly salient. Indeed, in addition to the need for ongoing fidelity evaluation, the present findings highlight the importance of several organizational factors related to implementation (see Fixsen et al. 2005). It is particularly critical that facilitators receive support and well-targeted supervision to facilitate model “buy in”, check in about meeting processes, and problem solve regarding the complexities of team or planning functions (Fixsen et al. 2005). Moreover, the results presented here also suggest that system administrators, supervisors, trainers, and team facilitators should take steps to attend to factors that will enable and encourage team members to be stable, active participants. Although the mechanisms of the detected effects are not yet known, it may be that consistent attendance by members facilitates greater team cohesion, collaboration, and commitment, which likely contribute to continuity of care for those served.
Although it is still unknown what factors contribute to the failure of team members to attend team meetings regularly, meeting times which are convenient to all team members may be a place to start. CFTs might explore less traditional hours and meeting locations that may better fit families’ complex lives. Furthermore, system-wide incentives for professionals to attend meetings after hours or on weekends may be a way to motivate professional team members’ attendance. Some sites are pursuing a reimbursement code for CFT attendance, a change that could increase the likelihood that professionals will attend reliably. In that context, it is important to examine the relationship between size of the team and team participation. Consistent with VanDenBerg and Grealish’s (1996) views, it may be that teams should strive to increase the number of informal supports while simultaneously decreasing the number of professionals over time, to keep the size and consistency manageable, rather than simply trying to add to the number of team members. In that vein, future research could assess the degree to which these findings hold for teams on which informal supportive persons comprise a higher proportion of the teams.
Given the goal of early implementation analyses is to identify opportunities for change, this study identifies areas of relevance for CFT fidelity to the SOC philosophy and the wraparound model. To increase the likelihood of successful outcomes for children and families, changes may need to be made to the structural characteristics of CFT operation. Although more research is needed to determine the reasons for inconsistent CFT attendance, prior work indicates that turnover prevalent in the mental health and social services fields (Barak et al. 2001; Blankertz and Robinson 1997), may be a contributing factor to fluctuations in team attendance. Many of the determinants of high turnover, such as job dissatisfaction, low job commitment, and lack of social support (Barak et al. 2001; Blankertz and Robinson 1997) may be difficult to address via policy or procedure, though several elements of the organizational context could be used to provide support (Fixsen et al. 2005) and reduce turnover which, in the longer-term, can help maintain continuity of care. For instance, previous studies have found that both training and positive rewards can help reduce turnover (Blankertz and Robinson 1997) among mental health professionals. Stressing the importance of CFT attendance and its impact on those served in training newly hired professionals within SOCs may be one way of addressing team attendance. It is also critical to ensure that meetings are at times and places accessible to the members. In addition, creating recognition and other forms of rewards may increase consistent participation and reduce turnover. Similarly, it may be that better functioning meetings could result in more team members attending on a consistent basis. Members may then feel that the team, and their participation in it, is more likely to result in positive outcomes for the family. As such, it is critical that communities utilize data from ongoing process-oriented evaluations to provide feedback to their systems and their teams, as they work to optimally address the needs of the children and families served.
References
Barak, M. E. M., Nissly, J. A., & Levin, A. (2001). Antecedents to retention and turnover among child welfare, social work, and other human service employees: What can we learn from past research? A review and metaanalysis. Social Science Review, 75, 625–661.
Bertram, R. M., Suter, J. C., Bruns, E. J., & O’Rourke, K. E. (2010). Implementation literature: Building a research agenda. Journal of Child and Family Studies. http://www.springerlink.com/content/ww5631471k6nu087/fulltext.pdf.
Blankertz, L. E., & Robinson, S. E. (1997). Turnover intentions of community mental health workers in psychological rehabilitation services. Community Mental Health Journal, 33, 517–529.
Bruns, E. J., Burchard, J. D., Suter, J. C., Leverentz-Brady, K., & Force, M. M. (2004). Assessing fidelity to community-based treatment for youth: The Wraparound Fidelity Index. Journal of Emotional and Behavioral Disorders, 12, 79–89.
Bruns, E. J., Suter, J. C., Force, M. M., & Burchard, J. D. (2005). Adherence to wraparound principles and association with outcomes. Journal of Child and Family Studies, 14, 521–534.
Bruns, E. J., Leverentz-Brady, K. M., & Walker, S. (2007). Wraparound fidelity in systems of care and association with outcomes. Paper presented at the 20th Annual Research Conference, A System of Care for Children’s Mental Health: Expanding the Research Base, Tampa, FL.
Bruns, E. J., Suter, J. C., & Leverentz-Brady, K. (2008). Is it wraparound yet? Setting quality standards for implementation of the wraparound process. The Journal of Behavioral Health Services and Research, 35, 240–252.
Burns, B. J., & Goldman, S. K. (Eds.). (1999). Promising practices in wraparound for children with serious emotional disturbance and their families. Systems of Care: Promising Practices in Children’s Mental Health, 1998 Series, Volume IV. Washington, DC: Center for Effective Collaboration and Practice, American Institutes for Research.
Centers for Disease Control. (2009). Developing process evaluation questions. Department of Health and Human Services. Evaluation Brief, 4, 1–2. Retrieved April 14, 2010, from http://www.cdc.gov/healthyYouth/evaluation/pdf/brief4.pdf.
Cook, J. R., Kilmer, R. P., DeRusso, A., Vishnevsky, T., & Meyers, D. C. (2007). Assessment of child and family team functioning using the Participant Rating Form. In C. Newman, C. Liberton, K. Kutash, & R. Friedman (Eds.), 19th Annual Research Conference Proceedings: A System of Care for Children’s Mental Health: Expanding the Research Base (pp. 317–322). Tampa, FL: University of South Florida, The Louis de la Parte Florida Mental Health Institute, Research and Training Center for Children’s Mental Health.
Cook, J. R., Kilmer, R. P., Cable, E., Campbell, K., DeRusso, A., & Vishnevsky, T. (2008). Utilizing the Participant Rating Form to assess child and family team functioning and enhance wraparound fidelity. In C. Newman, C. Liberton, K. Kutash, & R. Friedman (Eds.), 20th Annual Research Conference Proceedings: A System of Care for Children’s Mental Health: Expanding the Research Base (pp. 165–170). Tampa, FL: University of South Florida, The Louis de la Parte Florida Mental Health Institute, Research and Training Center for Children’s Mental Health.
Davis, C. S., & Dollard, N. (2004). Team process and adherence to wraparound principles in a children’s community mental health care system of care. Unpublished Manuscript. Child and Family Studies, Louis de la Parte Florida Mental Health Institute, University of South Florida.
Delva, D., Jamieson, M., & Lemieux, M. (2008). Team effectiveness in academic primary health care teams. Journal of Interprofessional Care, 22, 598–611.
Dinnebeil, L. A., Hale, L., & Rule, S. (1999). Early intervention program practices that support collaboration. Topics in Early Childhood Special Education, 19, 225–235.
Epstein, M. H., Nordness, P. D., Kutash, K., Duchnowski, A., Schrepf, S., Benner, G., et al. (2003). Assessing the wraparound process during family planning meetings. Journal of Behavioral Health Services and Research, 30, 352–362.
Faw, L. (1999). The state wraparound survey. In B. J. Burns & S. K. Goldman (Eds.), Systems of care: Promising practices in children’s mental health, 1998 series: Volume IV. Promising practices in wraparound for children with severe emotional disorders and their families (pp. 79–83). Washington, DC: Center for Effective Collaboration and Practice, American Institutes for Research.
Fixsen, D. L., Naoom, S. F., Blasé, K. A., Friedman, R. M., & Wallace, F. (2005). Implementation research: A synthesis of literature. Tampa, FL: The University of South Florida, Louis de la Parte Florida Mental Health Institute, The National Implementation Research Network (FMHI Publication #231).
Goodman, P.S. & Leyden, D.P. (1991). Familiarity and group productivity. Journal of Applied Psychology, 76, 578-586.
Haber, M. G., Cook, J. R., Kilmer, R. P., & Hemphill, B. T. (2010). Relationships of child and family team meeting processes to initial and long-term changes in youth functioning. Paper presented at the 23rd Annual Children’s Mental Health Research and Policy Conference, Tampa, FL.
Hemphill, B.T. (2009). Evaluating the effectiveness of systems of care in Mecklenburg County: Assessing the relationship between child and family team practices and youth functioning. Unpublished master’s thesis, University of North Carolina at Charlotte.
Hemphill, B. T., Cook, J. R., & Kilmer, R. P. (2010). Child and family team meeting processes as predictors of changes in youth functioning. Paper presented at the 23rd Annual Children’s Mental Health Research and Policy Conference, Tampa, FL.
Hernandez, M. (Ed.). (2003). Special series: Children’s mental health policy. Journal of Emotional and Behavioral Disorders, 11, 1–58.
Jackson, S. E., Brett, J. F., Sessa, V. I., Cooper, D. M., Julin, J. A., & Peyronnin, K. (1991). Some differences make a difference: Individual dissimilarity and group heterogeneity as correlates of recruitment, promotions, and turnover. Journal of Applied Psychology, 76, 675–689.
Mullen, B., & Cooper, C. (1994). The relation between group cohesiveness and performance: An integration. Psychological Bulletin, 115, 210–227.
Rast, J., & Bruns, E. (2003). Ensuring fidelity to the wraparound process. Focal Point: A national bulletin on family support and children’s mental health, 17, 21–24.
Stroul, B. A., & Friedman, R. M. (1986). A system of care for children and youth with severe emotional disturbances (revised edition). Washington, D.C.: Georgetown University Child Development Center, CASSP Technical Assistance Center.
Suter, J. C., & Bruns, E. J. (2009). Effectiveness of the wraparound process for children with emotional and behavioral disorders: A meta-analysis. Clinical Child and Family Psychology Review, 12, 336–351.
VanDenBerg, J. E., & Grealish, E. M. (1996). Individualized services and supports through the wraparound process: Philosophy and procedures. Journal of Child and Family Studies, 5, 7–21.
Walker, J. S., & Bruns, E. (2003). Quality and fidelity in wraparound. Focal Point: A national bulletin on family support and children’s mental health: Quality and fidelity in Wraparound, 17, 3.
Walker, J. S., & Schutte, K. (2003). Practices to promote effective teamwork in ISP/wraparound. Focal Point: A national bulletin on family support and children’s mental health, 17, 12–14.
Walker, J. S., & Schutte, K. M. (2004). Practice and process in wraparound teamwork. Journal of Emotional and Behavioral Disorders, 12, 182–192.
Walker, J. S., & Schutte, K.M. (2005). Quality and individualization in wraparound team planning. Journal of Child and Family Studies, 14, 251–267.
Wiseman, S., Chinman, M., Ebener, P. A., Hunter, S., Imm, P., & Wandersman, A. (2007). Getting to outcomes: 10 steps for achieving results-based accountability. Santa Monica, CA: RAND Corporation.
Woltmann, E. M., & Whitley, R. (2007). The role of staffing stability in the implementation of integrated dual disorders treatment: An exploratory study. Journal of Mental Health, 16, 757–769.
Wright, E. R., Russell, L. A., Anderson, J. A., Kooreman, H. E., & Wright, D. E. (2006). Impact of team structure on achieving treatment goals in a system of care. Journal of Emotional and Behavioral Disorders, 14, 240–250.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Palamaro Munsell, E., Cook, J.R., Kilmer, R.P. et al. The Impact of Child and Family Team Composition on Wraparound Fidelity: Examining Links Between Team Attendance Consistency and Functioning. J Child Fam Stud 20, 771–781 (2011). https://doi.org/10.1007/s10826-011-9444-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-011-9444-5