
Abstract
Behavioural parenting programs are an effective intervention for behavioural and emotional problems in children, however these programs have low utilisation rates by culturally diverse parents. We examined the cultural acceptability of program materials, preferences for delivery methods, and barriers to use of the Triple P-Positive Parenting Program. One hundred and thirty seven parents watched a video outlining the 17 strategies in Triple P and read through a tip sheet before completing a series of questionnaires. Results revealed that parents found the strategies highly acceptable, highly useful, were very likely to use the strategies and reported currently using the strategies often. They also rated the program materials as very culturally appropriate and identified group, seminar, television, and individual as the most preferred delivery methods. Parents identified location and timing of services, financial cost, and competing work commitments as the most frequently cited barriers to accessing a parenting intervention. The findings of this study suggest that elements of parenting programs may not be contributing to the low rates of access among culturally diverse parents. These findings highlight the need for more research addressing variables that may contribute to increasing culturally diverse parents’ access of behavioural parenting programs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The quality of parenting children receive impacts on every aspect of children’s development and adult outcomes (e.g., Vimpani et al. 2002). Many interventions have been developed to assist parents in their role and to help prevent the development of conduct and emotional problems in children. Of the available parenting interventions, behavioural family interventions based on social learning models have the strongest empirical support (Lundahl et al. 2006). These aim to effect change in children’s behaviour and adjustment by modifying aspects of the family environment which maintain and reinforce a child’s problem behaviours (Sanders 1992). However, epidemiological surveys show that relatively few parents (approximately 14%) participate in any form of parent education and exposure to evidence based intervention is lower (Sanders et al. 1999). Parents from culturally diverse backgrounds are even less likely than other families to access parenting programs (Cunningham et al. 2000; Katz et al. 2007; Sawrikar and Katz 2008) and this is despite the fact that culturally diverse children can be at a greater risk for developing behaviour problems (McCabe et al. 2005; McKay et al. 1996; Willgerodt and Thompson 2006).
Considering the serious consequences associated with childhood behaviour problems and given the information related to the efficacy of behavioural parenting programs, it is important to understand why fewer culturally diverse parents are accessing parenting programs. Potentially, there are many barriers that parents face when accessing parenting programs, including parental characteristics, child factors, the therapeutic relationship, intervention characteristics and contextual variables (Morawska and Sanders 2006).
The general parenting literature suggests that the low access of services by parents is the result of a number of different barriers, including practical barriers such as time constraints and scheduling conflicts (Heinrichs et al. 2005; Owens et al. 2002), problems with child care, transport, the cost involved in attending sessions, and a lack of information on what services are offered (Sawrikar and Katz 2008; Spoth et al. 1996). Individual parent factors may also prevent parents from accessing services, such as a belief that a child does not need help or that they can manage problems on their own (Spoth et al. 1996). Socio-demographic barriers have also been reported in the literature, with socially isolated, low income, single, or depressed parents being less likely to participate in behavioural parenting programs (Snell-Jones et al. 2004; Spoth et al. 1996). The literature also suggests that cultural barriers such as language, family opinions about seeking help, distrust of mental health services, and a lack of mental health providers with a matched cultural background can prevent individuals accessing mental health services (Griner and Smith 2006; McKay et al. 1996; Sawrikar and Katz 2008). However, few studies have focused specifically on behavioural parenting programs and whether culturally diverse parents identify any cultural barriers to accessing these programs.
There is currently debate in the literature as to whether existing parenting programs are effective in addressing the needs of culturally diverse parents, or whether programs need to be tailored or adapted to be more effective for these parents (Lau 2006). Most adapted programs have shown an increase in the recruitment of culturally diverse parents, which is important considering the lower rates of access of services (Harachi et al. 1997; Kumpfer and Alvarado 1995; Martinez and Eddy 2005; McCabe et al. 2005). Despite the positive results in terms of recruitment, few studies have shown any increases in the outcomes for parents or children of culturally diverse backgrounds, and some studies have found negative outcomes for parents where practitioners have eliminated important content or reduced the number of behavioural strategies in order to adapt the program (Castro et al. 2004; Kumpfer et al. 2002).
Researchers have also suggested that the adaptations made to these programs are based more on practitioners’ perceptions of what culturally diverse parents want, and a need to be politically correct as opposed to empirical evidence (Elliot and Mihalic 2004; Kumpfer et al. 2002). These limitations raise the questions of whether adapting behavioural parenting programs is really necessary and suggest that more research is needed to address this issue. Furthermore, the difficulty in tailoring a program to every possible cultural group, and the logistic and financial cost associated with adapting a program for each individual group is enormous and needs consideration (Kumpfer et al. 2002). More importantly, once a program has been adapted for one cultural group it may become inappropriate for other cultural groups, meaning fewer people are able to benefit from the program.
Gauging parents’ perception of program acceptability is very important because there is a lack of research addressing this issue and it plays a vital role in individuals accessing treatment. Individuals are more likely to access treatments that they view as acceptable (Borrego and Pemberton 2007), while treatments that are perceived as unacceptable may not be accessed regardless of their effectiveness (Eckert and Hintze 2000). Assessing acceptability is also important in determining if a program needs to be adapted to suit a given community (Lau 2006).
There is substantial research regarding consumer satisfaction and acceptability of parent-training programs, however the majority of this research was conducted in the 1980s (e.g., McMahon and Forehand 1983). Whilst research has found that parent’s satisfaction ratings are generally high, the majority of studies in this area have measured satisfaction ratings post-intervention. This does not address the issue of whether perception of program content prior to participation is likely to contribute to participation, and there is even less literature assessing culturally diverse parents’ perceptions of acceptability.
The Triple P-Positive Parenting Program is a multilevel parenting and family support system, which aims to prevent childhood behavioural and emotional problems by targeting parents’ behaviour. The program focuses on increasing the skills and knowledge of parents as well as enhancing their self-sufficiency and resourcefulness in dealing with their child’s behaviour. The program also focuses on promoting positive interactions between parents and children and ensuring that parents provide a safe, engaging, and loving environment for their children (Sanders 2008). Triple P has been widely disseminated in Australia and internationally (Prinz and Sanders 2007; Sanders 2008). Despite the widespread use of the program, there is some concern in the literature about the program being appropriate for culturally diverse families (Thomas and Zimmer-Gembeck 2007).
This study examined parents’ opinions in terms of barriers, acceptability, and preferences for Triple P, to determine if the program needed to be adapted for culturally diverse parents and to guide adaptation if necessary. Addressing each of these areas is important because it enables researchers to examine if elements of the intervention are contributing to underutilisation of parenting programs. It also provides researchers with information regarding what culturally diverse parents want from a parenting program and helps determine whether programs need to be modified to better suit the needs of culturally diverse parents.
Methods
Participants
There were 137 participants in this study, of which 109 (79.6%) were women. The average age of participants was 35.78 (SD = 8.27), and most (78.5%) participants were married. Participants were born in many different countries with the two most common including Australia (33.6%) and Vietnam (18.7%), representing a diversity of ethnic backgrounds as shown in Table 1. Many participants had a university education (42.2%), or had less than 12 years of school education (26.7%), while smaller proportions had completed high school only (14.8%) or had some college or trade qualifications (16.3%). Twenty two percent participants were employed full-time, 24.4% were employed part-time, 24.4% were homemakers, 13.7% were unemployed, and 15.3% were students. Twenty two percent of families had an annual income of AUD$25,000 or less, 13.8% were between AUD$25,000 and $40,000, 20.1% were between AUD$40,000 and $75,000, 20.2% were between AUD$75,000 and $100,000, while 23.9% had an annual income of more than AUD$100,000. The majority of participants lived in an original intact family (79.4%) with a minority in a single parent (14.5%) or step (5.3%) family. Most household had one (29.7%), two (40.7%) or three (15.3%) children living in the house, with a minority (14.2%) reporting four or more children. The target child for completion of questionnaires had an average age of 4.33 (SD = 2.81) and was more likely to be male (58.7%).
Nearly 30% of parents had participated in a parenting program in the past. Most (70.2%) had previously heard about Triple P largely from friends or relatives (44.1%), school (35.0%), medical professionals (19.3%) or the media (18.4%). Almost 16% of participants had previously sought help for their child’s behaviour, with help being sought from counsellors (29.7%), teachers (25.0%), primary care physicians (23.1%), psychologists (16.2%), paediatricians (15.2%) or others (21.1%). Most parents indicated that they found parenting very or extremely rewarding (90.7%), very or extremely demanding (66.1%), moderately to very stressful (62.7%), very or extremely fulfilling (84.3%) and not at all to slightly depressing (81.2%). The vast majority of parents were moderately to extremely confident in their parenting over the past 6 weeks (99.2%), moderately to extremely supported in their parenting in general (89.1%), and by their partner (92.1%), and reported a high level of satisfaction in their marital relationship (M = 7.40, SD = 2.48).
Materials
The Every Parent’s Survival Guide (Sanders et al. 2005) is a DVD that provides parents with an explanation of the 17 strategies utilised by Triple P. The strategies are divided into two sections: promoting children’s development and managing misbehaviour. Each of the strategies is presented individually and the DVD provides a description of how to implement the strategy. The DVD uses adult and child actors who reflect a number of different cultural backgrounds to act out the appropriate way to use each strategy. The DVD had an approximate running time of 20 min.
The Triple P tip sheets offer parents practical information and advice on positive approaches to parenting in dealing with a range of situations and behaviours they may encounter with their children. This study used three tip sheets aimed at toddlers, preschoolers, and primary schoolers and parents received one tip sheet that was relevant to the age of the child they were completing the questionnaire for. The tip sheet for toddlers focused on sharing, for preschools it dealt with having visitors and for primary schoolers it looked at doing chores. Each tip sheet focused on teaching children new behaviours, preventing problems from occurring, and managing problems if they arose, and included an overview of the key steps. The tip sheets were written in plain and easy to understand English and were one page front and back.
Measures
The Family Background Questionnaire gathered information on the demographic background of the sample, specifically the age, gender, marital status, and ethnicity of the participant. Level of education, employment status, yearly income, and household composition were also reported. Participants were also asked if they had ever participated in any parenting programs, if and where they had heard of Triple P and if they had ever sought professional help for any problems their child might have experienced. Finally, the participants were asked a number of questions dealing with their parenting over the last 6 weeks. These questions related to the experience of being a parent, confidence in being a parent, how supported they felt in their role as parent, how supportive their partner was in parenting, and their degree of happiness in their relationship with their partner.
Child behaviour was assessed using the Eyberg Child Behavior Inventory (ECBI; Eyberg and Pincus 1999), a 36-item measure of parental perceptions of disruptive behaviour in children between the ages of 2 and 16. It consists of a measure of the frequency of disruptive behaviours (Intensity) rated on a 7-point scale, ranging from never (1) to always (7) and a measure of the number of behaviours that are a problem for parents (Problem), using a yes–no format. In this sample there was good internal consistency (α = .91 and .90, respectively), and the ECBI has good test–retest reliability (r = .86 and .88, respectively). Scores greater than 131 on the Intensity scale and greater than 15 on the Problem scale are indicative of difficulties in the clinical range, and were used as clinical cutoffs in this study.
The Parenting Scale (PS; Arnold et al. 1993) is a 30-item questionnaire measuring three dysfunctional discipline styles: laxness (permissive discipline), over-reactivity (authoritarian discipline, displays of anger), and verbosity (overly long reprimands or reliance on talking). Each item has a more effective and a less effective anchor, and parents indicate on a 7-point scale, which end better represents their behaviour. The scales had good internal consistency in this sample (α = .83, .81, .36, and .80 respectively) and the scale has good test–retest reliability (r = .83, .82, and .79, respectively).
A questionnaire was devised based on Whittingham et al. (2006) to examine the acceptability and usefulness of each Triple P strategy. The 17 strategies are divided into four categories: promoting relationships, encouraging appropriate behaviour, teaching new skills and behaviours, and managing misbehaviour. Parents rated the acceptability, usefulness, likelihood of usage and current use for each strategy by circling a number on a 10-point scale with higher scores indicating that a strategy is more acceptable, useful, likely to be used, and is currently used. Following this, parents indicated whether or not there were barriers to using each strategy, and if yes, they were asked to indicate what these potential barriers were by ticking the appropriate box or writing on the line provided.
The second part of the questionnaire examined the appropriateness of the program materials and delivery modalities utilised by Triple P, as well as any potential barriers to accessing the program. The first section looked at the program materials; specifically the DVD, and an age appropriate tip sheet. Participants were asked to rate how helpful the DVD was and whether they found the examples and the way the actors spoke on the video culturally appropriate. They were asked to rate their responses from 1 (not at all helpful) to 10 (extremely helpful) or 1 (not at all appropriate) to 10 (extremely appropriate). Participants were also asked a number of questions dealing with the relevance and usefulness of the tip sheet (e.g., “how relevant did you find the tip sheet?”) and asked to rate their responses on a 10-point scale ranging from 1 (not at all relevant) to 10 (extremely relevant) or 1 (not at all useful) to 10 (extremely useful). Participants were also asked about the extent to which they would use the ideas in the tip sheet at home with their child, again on a 10-point scale ranging from 1 (never) to 10 (always). Participants were then asked to rate the cultural appropriateness of the tip sheet using the same scale that had been used for the video and listing their concerns with the tip sheet if they gave a rating of five or below. Finally, this section looked at whether participants would be interested in receiving additional tip sheets on other issues. Parents rated their response on a 10-point scale ranging from 1 (not at all interested) to 10 (extremely interested).
Participants were asked to rate the extent to which they would find different delivery modalities useful, on a scale of 1 (not at all useful) to 10 (extremely useful). Participants were also asked about the likelihood of participating in Triple P in the future or if their child developed emotional or behavioural problems, on a scale of 1 (not at all likely) to 10 (extremely likely). They were also asked how interested they were in the possibility of participating in Triple P in the future, on a 10-point scale ranging from 1 (not at all interested) to 10 (extremely interested). Finally, the participants were given a list of potential barriers to accessing Triple P and asked to indicate any of those which applied to them. If parents checked cultural or other barriers they were asked to provide a written example of a potential barrier to accessing the program.
Procedure
Community organisations, local councils and cultural group leaders were contacted and links were developed through meetings and discussions. Once these links were established, the researchers organised suitable times to conduct the study. Parents were asked to complete all questions in regards to their child aged 2–10 years. If they had more than one child in that age range, they were asked to complete the questionnaires in regards to their youngest child in that age range. The parents completed the family background questionnaire, the ECBI and the Parenting Scale; then watched the DVD and completed part one of the questionnaire. Participants were then given an age appropriate tip sheet to read through and answer additional questions on. Finally, participants were asked to complete the section of the questionnaire which dealt with the delivery modalities and any potential barriers to accessing Triple P.
Results
Child Behaviour and Parenting
Parents reported generally low levels of child behaviour difficulties, with a mean ECBI Intensity score of 110.53 (SD = 26.38) and a mean Problem score of 9.02 (SD = 7.56), with about 13% of children reported as in the clinical range for either scale. In contrast, many parents scored in the clinical range for laxness (36.8%), over-reactivity (37.2%), verbosity (39.0%) and total ineffective parenting (48.1%) on the Parenting Scale.
Acceptability of Strategies
As shown in Table 2, parents found all of the Triple P parenting strategies highly acceptable, useful, and most parents reported either currently using the strategy or being likely to use the strategy in the future. Given the relatively higher number of White Australian parents in the sample compared to any other ethnic group, between groups ANOVAs were used to check for differences between White Australian and all others parents for all strategies. Across the 17 strategies there were no differences in acceptability, except for directed discussion F(1,131) = 4.13 p = .044 with White Australian parents rating the strategy as less acceptable (M = 8.11, SD = 2.11) than all other parents (M = 8.75, SD = 1.48). Similarly, for strategy usefulness, there were no differences except for directed discussion F(1,132) = 4.21 p = .042 and engaging activities F(1,134) = 4.25 p = .041. White Australian parents rated directed discussion as less useful (M = 7.86, SD = 2.14) than all other parents (M = 8.62, SD = 1.79), but rated engaging activities as more useful (M = 9.31, SD = 1.28) than all other parents (M = 8.66, SD = 1.72).
Across the 17 strategies there were no differences between White Australian parents in the likelihood of use of any of the strategies. However, compared to all other parents, White Australian were less likely to report current use of ask-say-do, F(1,132) = 10.81 p = .001 (M = 7.74, SD = 1.99 vs. M = 6.50, SD = 1.58), behaviour charts F(1,127) = 5.86 p = .017 (M = 7.45, SD = 2.36 vs. M = 6.97, SD = 2.65), rules F(1,130) = 9.90 p = .002 (M = 7.62, SD = 2.17 vs. M = 6.28, SD = 2.20), and directed discussion F(1,131) = 6.31 p = .013 (M = 7.12, SD = 2.60 vs. M = 5.92, SD = 1.93). As there were only minor differences in means between groups, and the small number of significant differences between White Australian and other parents, all subsequent analyses were conducted on the sample as a whole.
In general, as shown in Table 3, paired samples t tests revealed different types of strategies more acceptable than others. In particular, acceptability ratings were highest for strategies for promoting relationships, and lowest for strategies for managing misbehaviour. However, means across all of the four types of strategies were very high.
Barriers to Strategy Use
Parents were asked to indicate whether they perceived any barriers to using each of the strategies. Table 4 shows the percentage of parents indicating barriers to use of the strategies. Interestingly, parents were most likely to encounter barriers to using quality time, behaviour charts and engaging activities, followed by quiet time and time out. Table 5 lists the type of barriers experienced by parents in relation to each of the strategies. As can be seen from the table the most commonly experienced barriers related to the time required to implement the strategy, and the belief that the strategy would not work, while the least likely barriers were cultural barriers and lack of support. Parents were also asked to describe the cultural barriers they encountered, and while most parents did not provide information, comments related to general barriers rather than cultural barriers.
Acceptability of Resources
Participants reported that they found the video very helpful (M = 7.78, SD = 1.72), and the examples and language very culturally appropriate (M = 7.87, SD = 1.84 and M = 7.93, SD = 1.73, respectively). Similarly, parents found the tip sheet useful (M = 7.83, SD = 1.69) and culturally appropriate (M = 7.80, SD = 1.93), and were interested in receiving other Triple P tip sheets (M = 8.25, SD = 1.85).
Preferences for Intervention Delivery and Barriers to Access
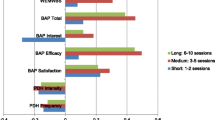
While all delivery modalities were seen as useful, Table 6 indicates that television or group based delivery were parents’ preferred methods of accessing parenting information, while radio and self-directed programs were the least preferred methods. Parents also indicated that they would be very interested in participating in Triple P (M = 8.10, SD = 1.86), especially if they experienced problems with their child (M = 8.22, SD = 2.06). Table 7 shows the potential barriers to accessing Triple P reported by parents. The most commonly endorsed barriers included practical barriers such as costs, location of service and competing work demands, while barriers related to culture were identified by a very small minority of parents. Of the five parents who indicated cultural barriers to program access two were Vietnamese, one was Indian, one Samoan, and one Fijian.
Discussion
The results indicated overall parents perceived the strategies in Triple P to be highly acceptable, highly useful, were very likely to use the strategies and reported currently using the strategies often. Although no previous research has been conducted examining the acceptability, usefulness, likelihood of use, and current use of the strategies in parenting programs for culturally diverse parents, or parents in general, these findings do support previous studies examining the overall acceptability and satisfaction with the program content in parenting programs (McMahon et al. 1984; Webster-Stratton 1998). Furthermore, the findings are consistent with previous research examining the acceptability and usability of the Triple P strategies for parents of children with Autism Spectrum Disorder (Whittingham et al. 2006). Parents also found the video very helpful and rated the examples used in the video and the way the actors spoke on the video as very culturally appropriate.
In general parents did not report many barriers to strategy use and cultural barriers did not pose a significant problem. Overall, parents reported that the strategies of quality time, behaviour charts and engaging activities had the most barriers to use. In regards to the barriers identified by parents, the main barriers were related to issues surrounding time, and the ineffectiveness of a strategy for a certain child. Therefore, based on these findings it appears that the strategies in parenting programs do not pose significant cultural barriers. Previous research has found that issues surrounding time demands consistently arise as barriers to participation in parenting programs for all parents, including culturally diverse parents (Heinrichs et al. 2005; Owens et al. 2007; Spoth et al. 1996; Wood and Baker 1999).
In examining the general barriers to accessing Triple P, the most frequently cited barriers were timing of services, location of services, financial cost, and competing work commitments. These findings are in line with the existing literature that has found practical barriers such as time constraints, scheduling conflicts and the cost involved in attending sessions, are often the most frequently cited barriers to accessing behavioural parenting programs (Heinrichs et al. 2005; Owens et al. 2007; Spoth et al. 1996).
These findings provides a valuable insight into the strategies in parenting programs that may potentially pose barriers for culturally diverse parents. Considering the results of this study within the context of prior research, it appears that Triple P is appropriate for culturally diverse families. These findings have theoretical implications for the ongoing debate regarding the cultural tailoring of parenting programs. It appears that, based on the current findings, cultural adaptation of parenting programs may not be necessary. The results can be used to help inform practitioners working with culturally diverse parents. Clearly the issues of time, whether it will work for a certain child, parental thoughts/beliefs and attributions of the child are pertinent barriers that culturally diverse parents face in using certain strategies and may prevent them from participating in parenting programs. Practitioners may be able to anticipate such barriers and assist parents in overcoming them. Moreover, the information gained from this study can inform efforts aimed at increasing participation in parenting programs through addressing potential barriers. The results suggest that efforts to increase engagement by focusing on these areas could be beneficial to parents regardless of their cultural background. Finally, the findings of this study can directly inform the development of parenting programs. In particular, programs can include psycho-education segments that assist parents in identifying the barriers they face and encouraging successful management of these barriers.
Parents most preferred television and group based delivery methods, however, all of the delivery methods were rated as useful, which suggests that parents prefer a wide range of ways of accessing parenting information. Further research examining these findings is important because delivering a parenting program through the medium of television has the potential to reach a wide variety of parents and children (Sanders et al. 2008). It also has the potential to help parents overcome a number of barriers identified for attending parenting programs.
The present study had a number of limitations that need to be considered when interpreting the results. Although the study was fairly diverse in terms of ethnicity, overall there was a fairly small sample of culturally diverse parents. This raises some concerns as to whether the results can be generalised to a wider range of culturally diverse parents. Due to the constraints of the study, gaining access to a large number of linguistically diverse parents was also an issue. In order to participate in this study parents needed to understand English, which may have limited the diversity of the sample. Future research should endeavour to get a larger culturally and linguistically diverse sample, to replicate the findings and ensure that the results can be generalised. Finally, parents provided high ratings of all of the strategies, implying a possible impact of social desirability on ratings. However, there were significant differences in ratings between different categories of strategies, indicating that parents did discriminate between strategies, and were not simply rating everything highly.
Considering the lack of empirical research investigating culturally diverse parents’ acceptability of the content of parenting programs and the barriers they experience, it would be hasty to assume that these findings are conclusive. It is critical that future research continues to investigate this population so that a greater understanding can be gained of the barriers they face in accessing and participating in parenting programs. Once there is sufficient research, this information can be used to address efforts to increase access and participation in parenting programs for culturally diverse parents.
References
Arnold, D. S., O’Leary, S. G., Wolff, L. S., & Acker, M. M. (1993). The Parenting Scale: A measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5, 137–144.
Borrego, J., & Pemberton, J. R. (2007). Increasing acceptance of behavioural child management techniques: What do parents say? Child & Family Behaviour Therapy, 29, 27–43.
Castro, F. G., Barrera, M., Jr., & Martinez, C. R., Jr. (2004). The cultural adaptation of prevention interventions: Resolving tensions between fidelity and fit. Prevention Science, 5(1), 41–45.
Cunningham, C. E., Boyle, M. H., Offord, D. R., Racine, Y., Hundert, J., Secord, M., et al. (2000). Tri-Ministry study: Correlates of school-based parenting course utilization. Journal of Consulting and Clinical Psychology, 68, 928–933.
Eckert, T. L., & Hintze, J. M. (2000). Behavioural conceptions and applications of acceptability: Issues related to service delivery and research methodology. School Psychology Quarterly, 15(123–148).
Elliot, D. S., & Mihalic, S. (2004). Issues in disseminating and replicating effective prevention programs. Prevention Science, 5, 47–53.
Eyberg, S. M., & Pincus, D. (1999). Eyberg child behavior inventory and sutter-eyberg student behavior inventory—revised: Professional manual. Odessa, FL: Psychological Assessment Resources.
Griner, D., & Smith, T. B. (2006). Culturally adapted mental health interventions: A meta-analytic review. Psychotherapy: Theory, Research, Practice, Training, 43, 531–548.
Harachi, T. W., Catalano, R. F., & Hawkins, D. J. (1997). Effective recruitment for parenting programs within ethnic minority communities. Child and Adolescent Social Work Journal, 14, 23–39.
Heinrichs, N., Bertram, H., Kuschel, A., & Hahlweg, K. (2005). Parent recruitment and retention in a universal prevention program for child behavior and emotional problems: Barriers to research and program participation. Prevention Science, 6, 275–286.
Katz, I., La Placa, V., & Hunter, S. (2007). Barriers to inclusion and successful engagement of parents in mainstream services. Retrieved May 5, 2008, from http://www.jrf.org.uk/bookshop/ebooks/barriers-inclusion-parents.pdf .
Kumpfer, K. L., & Alvarado, R. (1995). Strengthening families to prevent drug use in multi-ethnic youth. In G. Botvin, S. Schinke, & M. Orlandi (Eds.), Drug abuse prevention with multi-ethnic youth (pp. 253–292). Newbury Park, CA: Sage.
Kumpfer, K. L., Alvarado, R., Smith, P., & Bellamy, N. (2002). Cultural sensitivity and adaptation in family-based prevention interventions. Prevention Science, 3(3), 241–246.
Lau, A. S. (2006). Making the case for selective and directed cultural adaptations of evidence-based treatments: Examples from parent training. Clinical Psychology: Science and Practice, 13(4), 295–310.
Lundahl, B., Risser, H. J., & Lovejoy, M. C. (2006). A meta-analysis of parent training: Moderators and follow-up effects. Clinical Psychology Review, 26, 86–104.
Martinez, C. R., & Eddy, J. M. (2005). Effects of culturally adapted parent management training on Latino youth behavioural health outcomes. Journal of Consulting and Clinical Psychology, 73, 841–851.
McCabe, K. M., Yeh, M., Garland, A. F., Lau, A. S., & Chavez, G. (2005). The GANA program: A tailoring approach to adapting parent child interaction therapy for Mexican Americans. Education and Treatment of Children, 28, 111–129.
McKay, M. M., McCadam, K., & Gonzales, J. J. (1996). Addressing the barriers to mental health services for inner city children and their caretakers. Community Mental Health Journal, 32, 353–361.
McMahon, R. J., & Forehand, R. L. (1983). Consumer satisfaction in behavioral treatment of children: Types, issues and recommendations. Behavior Therapy, 14, 209–225.
McMahon, R. J., Tiedemann, G. L., Forehand, R., & Griest, D. L. (1984). Parental satisfaction with parent training to modify child noncompliance. Behavior Therapy, 15(3), 295–303.
Morawska, A., & Sanders, M. R. (2006). A review of engagement and strategies to promote engagement with parenting interventions. Journal of Children’s Services, 1, 29–40.
Owens, P. L., Hoagwood, K., Horwitz, S. M., Leaf, P. J., Poduska, J. M., Kellam, S. G., et al. (2002). Barriers to children’s mental health services. Journal of the American Academy of Child and Adolescent Psychiatry, 41, 731–738.
Owens, J. S., Richerson, L., Murphy, C. E., Jageleweski, A., & Rossi, L. (2007). The parent perspective: Informing the cultural sensitivity of parenting programs in rural communities. Child & Youth Care Forum, 36, 179–194.
Prinz, R. J., & Sanders, M. R. (2007). Adopting a population-level approach to parenting and family support interventions. Clinical Psychology Review, 27, 739–749.
Sanders, M. R. (1992). Enhancing the impact of behavioural family intervention with children: Emerging perspectives. Behaviour Change, 9, 115–119.
Sanders, M. R. (2008). Triple P-Positive parenting program as a public health approach to strengthening parenting. Journal of Family Psychology, 22(3), 506–517.
Sanders, M., Calam, R., Durand, M., Liversidge, T., & Carmont, S. A. (2008). Does self-directed and web-based support for parents enhance the effects of viewing a reality television series based on the Triple P—Positive Parenting Programme? Journal of Child Psychology and Psychiatry, 49, 924–932.
Sanders, M., Markie-Dadds, C., & Turner, K. M. T. (2005). Every Parents Survival Guide [DVD]. Brisbane, Australia: Triple P International.
Sanders, M. R., Tully, L. A., Baade, P. D., Lynch, M. E., Heywood, A. H., Pollard, G. E., et al. (1999). A survey of parenting practices in Queensland: Implications for mental health promotion. Health Promotion Journal of Australia, 9, 112–121.
Sawrikar, P., & Katz, I. (2008). Enhancing family and relationship service accessibility and delivery to culturally and linguistically diverse families in Australia. Family Relationships Clearinghouse, 3, 1–20.
Snell-Jones, J., Smith, B. H., & Mendez, J. L. (2004). Evidence-based solutions for overcoming access barriers, decreasing attrition and promoting change with undeserved families. Journal of Family Psychology, 18, 19–35.
Spoth, R., Redmond, C., Hockaday, C., & Shin, C. Y. (1996). Barriers to participation in family skills preventive interventions and their evaluations: A replication and extension. Family Relations, 45, 247–254.
Vimpani, G., Patton, G., & Hayes, A. (2002). The relevance of child and adolescent development for outcomes in education, health and life success. In A. Sanson (Ed.), Children’s health and development: New research directions for Australia (pp. 14–37). Melbourne: Australian Institute of Family Studies.
Webster-Stratton, C. (1998). Preventing conduct problems in head start children: Strengthening parenting competencies. Journal of Consulting and Clinical Psychology, 66, 715–730.
Whittingham, K., Sofronoff, K., & Sheffield, J. K. (2006). Stepping Stones Triple P: A pilot study to evaluate acceptability of the program by parents of a child diagnosed with Autism Spectrum Disorder. Research in Developmental Disabilities, 27(4), 364–380.
Willgerodt, M., & Thompson, E. (2006). Ethnic and generational influences on emotional distress and risk behaviors among Chinese and Filipino American Adolescents. Research in Nursing & Health, 29(311–324).
Wood, W. D., & Baker, J. A. (1999). Preferences for parent education programs among low socioeconomic status, culturally diverse parents. Psychology in the Schools, 36, 239–247.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/s10826-015-0161-3.
Rights and permissions
About this article
Cite this article
Morawska, A., Sanders, M., Goadby, E. et al. Is the Triple P-Positive Parenting Program Acceptable to Parents from Culturally Diverse Backgrounds?. J Child Fam Stud 20, 614–622 (2011). https://doi.org/10.1007/s10826-010-9436-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-010-9436-x