
Abstract
Biederman and colleagues reported that a CBCL profile identified youngsters who were diagnosed with bipolar disorder. Some studies found that this CBCL profile does not reliably identify children who present with bipolar disorder, but nonetheless this CBCL does identify youngsters with severe dysfunction. However, the nature of the impairment of youngsters who fit this profile is unclear. The goal of this study was to describe the clinical characteristics of youngsters who fit this CBCL profile. The sample included 310 youngsters referred to an outpatient psychopharmacology clinic. There were 55 youngsters who fit the CBCL profile. These youngsters were compared to 255 youngsters who did not fit the CBCL profile. Measures included the CBCL, standardized measures of aggression and ADHD symptoms, youngsters’ self-reported depression, DSM-IV diagnoses, and child and adolescent psychiatrists’ ratings of impairment and functioning. Compared to youngsters who did not fit the CBCL bipolar disorder profile, youngsters who fit the profile had significantly higher scores on all but one CBCL scale and significantly higher levels of aggression. Youngsters who fit the CBCL profile also had greater psychosocial impairment and more DSM-IV diagnoses than youngsters who did not fit the profile. Youngsters who fit the CBCL profile exhibit severe dysregulation across multiple domains of functioning including attention, affective, and behavioral dysregulation that are not easily nor efficiently captured by extant DSM-IV diagnoses. These youngsters are not uncommon and comprise slightly less than 1 in 5 referrals to a child psychiatry clinic.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Pediatric bipolar disorder is difficult to diagnose, particularly for prepubertal youngsters. There are significant challenges in diagnosing bipolar disorder in children and adolescents because of high rates of comorbidity with attention deficit hyperactivity disorder, oppositional defiant disorder, and conduct disorder (Biederman et al. 2000; Fields and Fristad 2009; Kim and Miklowitz 2002). These disorders have several features that are very similar to bipolar disorder, including high levels of motor activity, impulsivity, irritability, hostility and aggression, impaired attention, and pressured speech or talkativeness (Fields and Fristad 2009; Kim and Miklowitz 2002).
There has been increasing interest in the utility of behavior checklists as a way to identify bipolar disorder in children and adolescents since Biederman and colleagues reported that a specific Child Behavior Check List (CBCL) profile identified youngsters who were diagnosed with bipolar disorder (Youngstrom 2007). Biederman and colleagues (Biederman et al. 1995, 1996; Faraone et al. 2005) reported that youngsters who were diagnosed with bipolar disorder (using a semi-structured diagnostic interview) had clinically significant elevations (T-scores > 70) on the following CBCL subscales: Aggression, Attention Problems, and Anxious/Depressed. This profile has been replicated by other investigators (e.g., Carlson and Kelly 1998; Carlson et al. 1998; Diler et al. 2007; Giles et al. 2007; Hazell et al. 1999) and meta-analysis showed that this profile differentiated between youngsters diagnosed with bipolar disorder and those with ADHD (Mick et al. 2003).
Based on evidence that youngsters with bipolar disorder exhibit a consistent pattern of elevations on the Aggression, Attention Problems, and Anxious/Depressed subscales, Mick et al. (2003) proposed that this CBCL profile could be used in clinical settings to identify youngsters with bipolar disorder. Findings from studies that used this CBCL profile to identify children and adolescents with bipolar disorder have been mixed, however. Some studies found that this CBCL profile identified youngsters with bipolar disorder with a high degree of accuracy (Biederman et al. 1995; Faraone et al. 2005; Hazell et al. 1999), but other studies reported that the CBCL profile did not reliably distinguish youngsters with bipolar disorder from youngsters with other disorders (Diler et al. 2009; Doerfler et al. 2010; Holtmann et al. 2007; Volk and Todd 2007; Youngstrom et al. 2005).
One finding to emerge from this research is that the CBCL profile is more common among youngsters with bipolar disorder compared to youngsters with other disorders (e.g., ADHD or conduct disorder), but this profile is not specific to pediatric bipolar disorder. That is, many youngsters with elevations on these CBCL subscales are diagnosed with another disorder instead of bipolar disorder. For example, Doerfler et al. (2010) found that 37% of youngsters diagnosed with bipolar disorder fulfilled the criteria for the CBCL bipolar disorder profile, compared to 19.6% of youngsters with ADHD without bipolar disorder. Even though a higher percentage of youngsters diagnosed with bipolar disorder fit the CBCL profile, over 80% of the youngsters with this profile were diagnosed with ADHD without bipolar disorder. Other studies also have reported that youngsters who fit criteria for the CBCL bipolar disorder profile were more likely to be diagnosed with a variety of disruptive behavior disorders, including ADHD, oppositional defiant disorder, and conduct disorder (Diler et al. 2009; Holtmann et al. 2007; McGough et al. 2008; Volk and Todd 2007; Youngstrom et al. 2005).
To date, investigators have focused primarily on whether this CBCL profile is useful in diagnosing bipolar disorder in children and adolescents. Considering the accumulating evidence that this profile is sensitive to bipolar disorder, but not specific to the diagnosis (Youngstrom 2007), the nature of the impairment and the DSM diagnoses of youngsters who fit this profile are unclear. Youngsters who fit this profile often receive multiple diagnoses (Doerfler et al. 2010), and the high degree of comorbidity may be an indication of complex ADHD or other severe disruptive behavior disorders (McGough et al. 2008). Alternatively, this profile may identify another form of severe psychopathology that is not described in DSM-IV (Althoff 2010; Ayer et al. 2009).
In their examination of youngsters who fit the CBCL bipolar disorder profile, Ayer et al. (2009) reported that this combination of CBCL subscales measures a single syndrome involving severe dysregulation across several domains. According to Ayer et al. (2009), youngsters indentified by this CBCL profile experience major difficulties in regulating mood, behavior, and cognition. No single DSM-IV diagnosis for children or adolescents includes such severe dysfunction and impairment in these domains. Ayer et al. (2009) concluded that youngsters identified by the CBCL bipolar disorder profile experience psychopathology across multiple domains of functioning but indicators of dysfunction in this study were limited to the CBCL (Achenbach 1991).
The present study used a wider range of assessment measures to examine the nature and severity of impairment in children and adolescents who fit the CBCL bipolar disorder profile. Measures in the present study included the CBCL, along with standardized measures of aggression and ADHD symptoms, youngsters’ self-reported depression, DSM-IV diagnoses, and child and adolescent psychiatrists’ ratings of impairment and functioning.
The present study compared youngsters who fit the CBCL bipolar disorder profile to youngsters who did not fit this profile in a sample of children and adolescents who were referred to a pediatric psychopharmacology clinic. It was hypothesized that youngsters who fit the CBCL profile would have significantly higher Externalizing and Internalizing CBCL scale scores than youngsters who did not fit this profile. It was also hypothesized that youngsters who fit this profile would exhibit higher levels of aggression and ADHD symptoms. These youngsters were also predicted to report higher levels of depressive symptoms. Finally, it was predicted that psychiatrists would rate youngsters who fit the CBCL profile as exhibiting poorer daily functioning and greater overall psychopathology.
Method
Participants and Procedure
This was a naturalistic study based on a clinical database. The sample was accrued by consecutive case ascertainment unselected for any specific psychiatric disorder. All children and adolescents who were referred to the outpatient Pediatric Psychopharmacology Clinic at the University of Massachusetts Medical School were systematically evaluated for psychopathology. Systematic clinical assessment included information from the child, parent, and teacher. Evaluations included child psychiatrist-administered clinical and structured diagnostic interviews. The Schedule for Affective Disorders and Schizophrenia for School Age Children—Epidemiologic Version (K-SADS; Orvaschel 1995) was used to obtain DSM-IV diagnoses for each child. Diagnoses were assigned based on parental-report data from the K-SADS. Parental report was emphasized because children under the age of 10 years may be unreliable when reporting symptoms (Edelbrock et al. 1986; Grills and Ollendick 2002; Schniering et al. 2000). Because many youngsters referred to this clinic were below 10 years old, parental report was used to maintain consistency in diagnostic procedures.
Psychiatrists also conducted a clinical interview with each child. Children completed several self-report rating scales and parents and teachers completed rating scales assessing the child’s behavior. Parents and legal guardians provided clinical consent for all evaluation procedures. The study was approved by the University of Massachusetts Medical Center’s Institutional Review Board. Children with autism, mental retardation (IQ < 70), or unstable medical or neurological illness were excluded from the study.
The sample included 310 children and adolescents (217 male, 93 female). The mean age of these youngsters was 10.65 years (SD = 3.4). With regard to racial background, 92% of the youngsters were Caucasian, 4% were Hispanic, 2% were African-American, 1% were Asian, and 2% were another ethnic group. In terms of annual family income, 26% earned less than $40,000, 13% earned $40,000–$49,000, 23% earned $50,000–$75,000, and 37% earned more than $75,000. There was a significant difference for mother’s education (M CBCL profile group = 14.7 years, SD = 2.6, M group that did not fit CBCL profile = 13.8 years, SD = 1.9), t (95.5) = 2.70, p < .01.Footnote 1 Fathers did not differ in terms of education (M CBCL profile group = 14.7 years, SD = 3.0, M group that did not fit CBCL profile = 13.9 years, SD = 2.8), t (250) = 1.58.
Of the 310 youngsters evaluated in this clinic, 55 (18%) had a T-score > 70 on the CBCL Aggression, Attention Problems and Anxious/Depressed subscales. These 55 youngsters (42 male, 13 female) fit the CBCL bipolar disorder profile. The remaining 255 youngsters (175 male, 80 female) did not fit the CBCL bipolar disorder profile. The groups did not differ in age, t (308) = 0.76, gender, X2 (1) = 1.29, N = 310, or racial background, X2 (4) = 0.91, N = 310.
Measures
K-SADS
A board certified child psychiatrist administered the K-SADS (Orvaschel 1995) individually to the parent or guardian about the referred child. A total of five child and adolescent psychiatrists conducted the interviews. Interrater reliability for diagnosis was assessed using the Kappa statistic (Cohen 1960) in a subsample of 53 children by two psychiatrists. These psychiatrists listened to audiotapes of the parent interview (N = 23) or observed the interview directly (N = 30). Interrater reliability was high (K = .87) for all diagnoses (current and lifetime). Interrater reliability for individual diagnoses was as follows: ADHD (K = .85), bipolar disorder (K = .79), conduct disorder (K = 1.0), oppositional defiant disorder (K = 1.0), tic disorder (K = 1.0), separation anxiety disorder (K = .92), panic disorder (K = .89), social phobia (K = .85), generalized anxiety disorder (K = .88), obsessive compulsive disorder (K = 1.0), and major depression (K = .84).
In addition to the DSM-IV diagnosis, the child psychiatrist rated impairment using the Children’s Global Assessment Scale (CGAS), which is a reliable measure of daily functioning and impairment (Green et al. 1994; Shaffer et al. 1983). Agreement on this scale was measured with the intraclass correlation coefficient (ICC; Bartko 1966) between child psychiatrists for 50 children. Agreement on this measure was good (ICC = 0.74). Severity of illness was assessed using the psychiatrist-rated Clinical Global Impression (CGI) Severity Scale (Guy 1976). This scale was used to assess severity of psychopathology regardless of diagnosis. The CGI is a 7-point rating scale that ranges from (1) “no signs of illness” to (4) “moderately ill” to (7) “extremely ill.” The scale has been shown to have acceptable concurrent validity in children with severe emotional disturbance (Mattison et al. 1990).
Child Behavior Check List
Parents completed the CBCL (Achenbach 1991), a 118-item parent-report measure of children’s behavioral and emotional problems. The CBCL contains eight narrow-band scales (Anxious/Depressed, Withdrawn, Somatic Complaints, Social Problems, Delinquent Behavior, Thought Problems, Attention Problems, and Aggressive Behavior) and two broad-band scales (Internalizing Problems, Externalizing Problems). A Total Score can also be calculated. For this study, T scores are reported.
Aggression and Hostility
The Modified Overt Aggression Scale (MOAS; Sorgi et al. 1991; Yudofsky et al. 1986) is a 20-item scale that assessed the frequency and severity of overt aggression during the previous month. Parents completed this scale, which is commonly used to rate aggression in clinical settings. The MOAS assesses four categories of aggression, including Verbal Aggression (threats to harm others), Object Aggression, (impulsive property destruction), Self-Aggression (self-injurious behavior), and Other Aggression (physical assault). Proactive and reactive aggression was assessed using the Proactive/Reactive Aggression Rating Scale (Dodge et al. 1997). This scale consists of three questions assessing reactive aggression and three questions assessing proactive aggression. Parents completed the Reactive/Proactive Aggression Rating Scale. The Buss Durkee Hostility Inventory (Buss et al. 1956; Treiber et al. 1989) was used to assess the child’s self-report of hostility. This scale yields an Expressed Hostility subscale and an Perceived Hostility subscale, as well as a Total Hostility score.
Hyperactive/Impulsive Behavior
Classroom teachers assessed the child’s hyperactive and impulsive behaviors using the 10-item Conners Teacher Rating Questionnaire (CTR; Conners, 2001). The CTR is a 10-item measure that is scored on a 0- to- 3 scale. Parents completed the ADHD Rating Scale-IV (DuPaul et al. 1998). This measure uses a 0- to- 3 scale to rate the frequency of 18 ADHD items listed in DSM-IV (American Psychiatric Association 2000). Internal consistency and test–retest reliability is well established for both measures.
Children’s Depression Inventory
The CDI (Kovacs 1992) is a 27-item child self-report measure of depressive symptoms. The CDI has sound psychometric properties, including high internal consistency, test–retest reliability, and discriminant validity.
Children’s School Functioning
Parents provided information about three indicators of their child’s school functioning. Parents reported whether their child (1) was receiving special education services, (2) had repeated a grade, and (3) had been suspended or expelled from school.
Results
CBCL
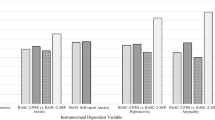
Table 1 presents the results for the CBCL scales. With the exception of the Withdrawn subscale, youngsters who fit the CBCL bipolar disorder profile had significantly higher scores on all CBCL scales than youngsters who did not fit the CBCL profile. The CBCL profile group had T-scores of 70 or greater on the following scales: Aggression, Attention Problems, Anxious/Depressed, Social, Thought Problems, and Delinquent Behavior. The CBCL profile group had a mean T-score of 80.8 on the Aggression subscale.
Aggression and Hostility
Table 2 presents the results for the aggression and hostility measures. Youngsters who fit the CBCL profile had significantly higher levels of aggression than youngsters who did not fit the CBCL profile on the MOAS Verbal Aggression, Physical Aggression, Other Aggression, and Total Aggression scales. There were no significant group differences for the MOAS Self-Aggression scale. Youngsters who fit the CBCL profile also had significantly higher scores on the Proactive Aggression and Reactive Aggression scales. For the Expressed Hostility and Perceived Hostility scales, there were no significant group differences.
ADHD Measures
On the ADHD Rating Scale, youngsters who fit the CBCL profile (M = 37.6, SD = 13.4) had significantly higher scores than youngsters who did not fit the CBCL profile (M = 31.5, SD = 20.1), t (270) = 2.09, p < .05. There were no significant differences on the Conners Teacher Questionnaire between youngsters who fit the CBCL profile (M = 17.8, SD = 10.5) and youngsters who did not fit the CBCL profile (M = 14.6, SD = 11.3), t (244) = 1.77.
Child-Reported Depression and Indicators of Impaired Functioning
There were no significant differences in the severity of child-reported depression symptoms on the CDI between youngsters who fit the CBCL profile (M = 13.4, SD = 8.4) and youngsters who did not fit the CBCL profile (M = 11.1, SD = 7.7), t (256) = 1.86.
Youngsters who fit the CBCL profile exhibited greater impairment in psychosocial functioning on the CGAS. Psychiatrists rated youngsters who fit the CBCL profile (M = 46.7, SD = 5.9) as more impaired than youngsters who did not fit the CBCL profile M = 49.1, SD = 5.9) t (300) = −2.70, p < .005.
Moreover, youngsters who fit the CBCL profile were more likely to have been suspended or expelled from school than were youngsters who did not fit the CBCL profile (44% vs 20%), X2 (1) = 14.58, p < .01, N = 307. However, the groups did not differ in the number of children receiving special education services (youngsters who fit the CBCL profile = 67%, youngsters who did not fit the CBCL profile = 70%) or the number of children who repeated a grade (youngsters who fit the CBCL profile = 20%, youngsters who did not fit the CBCL profile = 19%). Finally, there were no significant differences on psychiatrists’ global rating of severity of illness between youngsters who fit the CBCL profile (M = 4.51, SD = 1.3) and youngsters who did not fit the CBCL profile (M = 4.30, SD = 1.0), t (66.8) = 1.15.
DSM-IV Diagnoses
There were significant group differences for the total number of DSM-IV diagnoses and the number of externalizing disorder diagnoses. Youngsters who fit the CBCL profile received more DSM-IV diagnoses (M = 5.2, SD = 2.0) than youngsters who did not fit the CBCL profile (M = 3.5, SD = 2.0), t (278) = 5.16, p < .001. Youngsters who fit the CBCL profile also were diagnosed with more externalizing diagnoses (M = 2.1, SD = 0.5) than youngsters who did not fit the CBCL profile (M = 1.5, SD = 0.7), t (119.50) = 5.16, p < .001.
Discussion
The present study compared youngsters who fit the CBCL bipolar disorder profile with youngsters who did not fit this profile in a sample of children and adolescents who were evaluated in a pediatric psychopharmacology clinic. Youngsters fit this CBCL profile if they had a T-score of 70 or greater on the Anxious/Depressed, Attention Problems, and Aggressive Behavior subscales. In the present sample, 18% of children and adolescents fit the CBCL bipolar disorder profile. Results indicate that the youngsters who fit the CBCL bipolar disorder profile exhibited serious dysregulation in multiple domains including attention, mood, and behavior.
Parent ratings on the CBCL indicated that youngsters who fit the bipolar disorder profile exhibited severe psychopathology. A T-score of 70 on the CBCL indicates clinically significant problems (Achenbach 1991), and youngsters who fit the CBCL bipolar disorder profile had mean T-scores of at least 70 on the Aggressive Behavior, Anxious/Depressed, Attention Problems, Social, Thought Problems, and Delinquent Behavior subscales. For youngsters who fit the CBCL profile, the mean score on the Aggressive Behavior subscale was 80.8.
With the exception of the Withdrawn subscale, youngsters identified by the CBCL profile had significantly higher scores on all CBCL subscales than youngsters who did not fit the CBCL profile.
In addition to the CBCL, the present study included several measures of aggression and hostility. On parent-rating scales, youngsters who fit the CBCL bipolar disorder profile had significantly higher levels of aggressive behavior than youngsters who did not fit the CBCL profile. On the Modified Overt Aggression Scale (Sorgi et al. 1991; Yudofsky et al. 1986), parents rated youngsters who fit the CBCL profile as exhibiting higher levels of verbal aggression, aggression against objects (impulsive property destruction), and physical assault. Parents also rated youngsters who fit the CBCL profile as significantly higher on both proactive and reactive aggression (Dodge et al. 1997). These findings are consistent with other reports that youngsters who fit the CBCL bipolar disorder profile exhibit extremely aggressive, or even violent, behavior (Wozniak et al. 1995).
For parent reports of self-injurious behavior on the Modified Overt Aggression Scale (Sorgi et al. 1991; Yudofsky et al. 1986) there were no significant differences between youngsters who fit the CBCL bipolar disorder profile and those youngsters who did not fit the profile. This finding is inconsistent with other reports that this CBCL profile is associated with parent reports of the child’s suicidal thoughts or behaviors (Althoff et al. 2006; Volk and Todd 2007). Moreover, there were no significant group differences for child-reported Expressed and Perceived Hostility (Buss et al. 1956; Treiber et al. 1989). This finding suggests that youngsters who fit the CBCL profile did not view themselves as more hostile than youngsters who did not fit the CBCL profile.
Results for ADHD symptoms were inconsistent. Youngsters who fit the CBCL bipolar disorder profile had significantly higher scores than youngsters who did not fit the CBCL profile on the parent-report ADHD Rating Scale (DuPaul et al. 1998). For teacher ratings, there were no significant group differences on the Conners Teacher Questionnaire (Conners 2001). It is unclear whether this inconsistency reflects situational differences in the level of hyperactive and impulsive behavior, or whether it is due to measurement differences.
The CBCL bipolar disorder profile was associated with other indicators of severe dysfunction in this sample. Psychiatrists rated youngsters who fit the CBCL profile with greater impairment in psychosocial functioning than youngsters who did not fit the CBCL profile, and youngsters who fit the CBCL profile were twice as likely to have been suspended or expelled from school as youngsters who did not fit the CBCL profile. Youngsters who fit the CBCL profile also received more DSM-IV diagnoses, and more externalizing diagnoses than youngsters who did not fit the CBCL profile.
Overall, results of this study indicate that the CBCL profile of elevated scores on the Attention Problems, Anxious/Depressed, and Aggression subscales identifies youngsters who exhibit multiple, severe problems across several domains of functioning. Specifically, youngsters who fit this CBCL profile exhibit severe problems with mood, behavior, and cognition (Althoff 2010). It is particularly noteworthy that youngsters who fit this CBCL profile exhibited very high levels of aggressive behavior.
A growing body of research shows that the CBCL profile identifies youngsters with severe impairment (Biederman et al. 1995; Diler et al. 2009; Doerfler et al. 2010; Faraone et al. 2005; Hazell et al. 1999; Holtmann et al. 2007; Volk and Todd 2007; Youngstrom et al. 2005), but there is disagreement about how to conceptualize the psychopathology identified by this combination of three CBCL scales. Biederman and colleagues (Biederman et al. 1995, 1996) argued that the CBCL profile measures mania or bipolar disorder, but recent research has found that even though this profile is more common among youngsters diagnosed with bipolar disorder, the profile is not specific to bipolar disorder (Youngstrom 2007). In some studies, a large number of youngsters who fit the CBCL profile were diagnosed with externalizing disorders instead of bipolar disorder (Doerfler et al. 2010; Holtmann et al. 2007; McGough et al. 2008; Volk and Todd 2007).
It is possible that instead of bipolar disorder, youngsters who fit the CBCL profile exhibit a complex combination of disorders. Elevations on these three CBCL scales indicate the presence of numerous internalizing and externalizing symptoms that can be associated with a wide variety of diagnoses. Carlson (2007) argued that youngsters who exhibit severe mood dysregulation that is thought to characterize pediatric bipolar disorder actually have several comorbid disorders rather than bipolar disorder. Consistent with this position, youngsters who fit the CBCL profile generally have multiple diagnoses (Doerfler et al. 2010; McGough et al. 2008), especially disorders like ADHD or oppositional defiant disorder, which are marked by disinhibited behavior.
An alternative to the notion that the CBCL profile indicates complex comorbid disorders is the proposal that this CBCL profile measures a single syndrome that does not appear in DSM-IV (Althoff 2010; Ayer et al. 2009). According to Ayer et al. (2009), this syndrome is characterized by significant problems in regulating attention, mood, and behavior. Supporting this proposal, Ayer et al. (2009) reported that structural equation modeling of these three CBCL subscales identified a single latent construct. According to Ayer et al. (2009), this CBCL profile identifies youngsters who have severe problems with self-regulation, and youngsters with this self-regulation problem experience impairment in multiple domains. Based on the growing literature suggesting that this CBCL profile is not specific to pediatric bipolar disorder, Ayer et al. (2009) recommended that the profile be renamed the CBCL Dysregulation Profile.
At this point, it is uncertain whether the youngsters who fit the CBCL profile simply present with several comorbid conditions (Carlson 2007) or whether these youngsters exhibit a single disorder that does not appear in DSM-IV (Althoff 2010; Ayer et al. 2009). In the present study, youngsters who fit the CBCL profile had an average of 5 DSM-IV disorders (but youngsters who did not fit the CBCL profile averaged 3.5 DSM-IV disorders). A priority for future research should be to clarify the diagnostic profile of youngsters who fit the CBCL profile.
Regardless of the resolution of this diagnostic question, it is clear that a large percentage of youngsters referred to this psychopharmacology clinic exhibited severe psychopathology and impairment across multiple domains. These youngsters comprised 18% of referrals to this outpatient clinic. Of great concern, the present study indicates that youngsters who fit this CBCL profile exhibit severe levels of multiple forms of aggression. Because of the complexity of these problems, case conceptualization and intervention decisions are uncertain. Based on these findings that a large number of youngsters who fit the CBCL profile identified by Biederman and colleagues (Biederman et al. 1995, 1996) fit criteria for externalizing disorders like ADHD or oppositional defiant disorder, it does not appear that this CBCL profile measures bipolar disorder in children and adolescents. Hence, it may be prudent to follow Ayer et al.’s (2009) recommendation and rename this CBCL profile so that it is consistent with what the profile appears to be measuring. However, it is unclear whether the best description for this profile is the CBCL Dysregulation Profile.
As with all research, this study has some limitations that should be considered when evaluating these findings. One possible limitation may be a referral bias because youngsters were referred to a pediatric psychopharmacology clinic at a university hospital. Most youngsters referred to this clinic exhibited severe psychopathology and the findings may not generalize to other outpatient mental health or community settings. This clinic was not a specialty clinic and no specific diagnosis or presenting problem was required for referral. Hence, the results are not biased by preselection on diagnosis or other research grounds.
Another limitation is that most information concerning diagnosis and other symptomatology was provided by the younster’s parent. Most experts recommend that assessment of child and adolescent problems include information from the child and parent(s), but significant discrepancies between parent- and child-report are often found (Achenbach et al. 1987; De Los Reyes and Kazdin 2005). With respect to the diagnosis of bipolar disorder, Youngstrom et al. (2006) found that assessment measures completed by parents provided better information about manic symptoms than child- or teacher-report measures. Moreover, combining information from multiple informants did not provide additional information.
Finally, almost all children and adolescents in this sample were Caucasian. As a result, findings from this study should not be generalized beyond Caucasian children from predominantly middle-income families.
In summary, our results suggest that about 1 in 5 children in our clinical sample present with a constellation of mood, attention, and behavioral symptoms accompanied by severe aggression that remains poorly addressed by current classification methods. The clinical diagnosis of bipolar disorder does not seem to adequately characterize these children. Given their prevalence in the clinical setting further research should determine if these symptoms of dysregulation across multiple domains of functioning represent a unitary construct or multiple comorbid vulnerabilities.
Notes
Degrees of freedom for this variable were adjusted because the groups had unequal variances.
References
Achenbach, T. M. (1991). Manual for the child behavior check list/4–18 and 1991 profile. Burlington: University of Vermont, Department of Psychiatry.
Achenbach, T. M., McConaughy, S. H., & Howell, C. T. (1987). Child/adolescent behavioral and emotional problems: Implications for cross-informant correlations for situational specificity. Psychological Bulletin, 101, 213–232.
Althoff, R. R. (2010). Dysregulated children reconsidered. Journal of the American Academy of Child and Adolescent Psychiatry, 49, 302–305.
Althoff, R. R., Rettew, D. C., Faraone, S. V., Boomsma, D. I., & Hudziak, J. J. (2006). Latent class analysis shows strong heritability of the Child Behavior Checklist— Juvenile Bipolar Phenotype. Biological Psychiatry, 60, 903–911.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4 Text Revision ed.). Washington, DC: American Psychiatric Association.
Ayer, L., Althoff, R., Isanova, M., Rettew, D., Waxler, E., Sulman, J., et al. (2009). Child behavior checklist juvenile bipolar disorder (CBCL-JBD) and CBCL posttraumatic stress problems (CBCL-PTSP) scales are measures of a single dysregulatory syndrome. Journal of Child Psychology and Psychiatry, 50, 1291–1300.
Bartko, J. J. (1966). The intraclass correlation coefficient as a measure of reliability. Psychological Reports, 19, 3–11.
Biederman, J., Faraone, S., Mick, E., Wozniak, J., Chen, L., Ouelette, C., et al. (1996). Attention-deficit hyperactivity disorder and juvenile mania: An overlooked comorbidity? Journal of the American Academy of Child and Adolescent Psychiatry, 35(1996), 997–1008.
Biederman, J., Mick, E., Faraone, S. V., Spencer, J., Wilens, T. E., & Wozniak, J. (2000). Pediatric mania: A developmental subtype of bipolar disorder? Biological Psychiatry, 48, 458–466.
Biederman, J., Wozniak, J., Kiely, K., Ablon, S., Faraone, S., Mick, E., et al. (1995). CBCL clinical scales discriminate prepubertal children with structured interview-derived diagnosis of mania from those with ADHD. Journal of the American Academy of Child and Adolescent Psychiatry, 34, 464–471.
Buss, A. H., Durkee, A., & Baer, M. B. (1956). The measurement of hostility in clinical situations. Journal of Abnormal Psychology, 52, 84–86.
Carlson, G. A. (2007). Who are the children with severe mood dysregulation, a.k.a “rages?”. American Journal of Psychiatry, 164, 1140–1142.
Carlson, G., & Kelly, K. (1998). Manic symptoms in psychiatrically hospitalized children— what do they mean? Journal of Affective Disorders, 51, 123–135.
Carlson, G., Loney, J., Salisbury, H., & Volpe, R. (1998). Young referred boys with DICA-P manic symptoms vs two comparison groups. Journal of Affective Disorders, 51, 113–122.
Cohen, J. (1960). A coefficient of agreement for nominal scales. Educational and Psychological Measurement, 20, 37–46.
Conners, C. K. (2001). Manual for Conners’ rating scales—revised. North Tonawanda, NY: Multi-Heath Systems.
De Los Reyes, A., & Kazdin, A. E. (2005). Informant discrepancies in the assessment of childhood psychopathology: A critical review, theoretical framework, and recommendations for further study. Psychological Bulletin, 131, 483–509.
Diler, R. S., Birmaher, B., Axelson, D., Goldstein, B., Gill, M., Strober, M., et al. (2009). The child behavior checklist (CBCL) and the CBCL-bipolar phenotype are not useful in diagnosing pediatric bipolar disorder. Journal of Child and Adolescent Psychopharmacology, 19, 23–30.
Diler, R. S., Uguz, S., Seydaoglu, G., & Avci, E. N. (2007). Differentiating bipolar disorder in Turkish prepubertal children with attention-deficit hyperactivity disorder. Bipolar Disorders, 9, 243–251.
Dodge, K. A., Lochman, J. E., Harnish, J. D., Bates, J. D., & PEttit, G. S. (1997). Reactive and proactive aggression in school children and psychiatrically impaired chronically assaultive youth. Journal of Abnormal Psychology, 106, 37–51.
Doerfler, L. A., Connor, D. F., & Toscano, P. F. (2010). Aggression, ADHD symptoms, and dysphoria in children and adolescents diagnosed with bipolar disorder and ADHD. Unpublished manuscript.
DuPaul, G. J., Power, T. J., Anastopoulos, A. D., & Reid, R. (1998). ADHD rating scale-IV: Checklists norms, and clinical interpretation. New York: Guilford Press.
Edelbrock, C., Costello, A. J., Dulcan, M. K., Conover, N. C., & Kala, R. (1986). Parent-child agreement on child psychiatric symptoms assessed via structured interview. Journal of Child Psychology and Psychiatry and Allied Disciplines, 27, 181–190.
Faraone, S. V., Althoff, R. R., Hudziac, J. J., Monuteaux, M., & Biederman, J. (2005). The CBCL predicts DSM bipolar disorder in children: A receiver operating characteristic curve analysis. Bipolar Disorders, 7, 518–524.
Fields, B. W., & Fristad, M. A. (2009). Assessment of childhood bipolar disorder. Clinical Psychology: Science and Practice, 16, 166–181.
Giles, L. L., DelBello, M. P., Stanford, K. E., & Strakowski, S. M. (2007). Child behavior checklist profiles of children and adolescents with and at high risk for developing bipolar disorder. Child Psychiatry and Human Development, 38, 47–55.
Green, B., Shirk, S., Hanze, D., & Wanstrath, J. (1994). The children’s global assessment scale in clinical practice: An empirical evaluation. Journal of the American Academy of Child and Adolescent Psychiatry, 33, 1158–1164.
Grills, A. E., & Ollendick, T. H. (2002). Issues in parent-child agreement: The case of structured diagnostic interviews. Clinical Child & Family Review, 5, 57–83.
Guy, W. (1976). Assessment manual for psychopharmacology. Washington, DC: US Department of Health, Education, and Welfare.
Hazell, P. L., Lewin, T. J., & Carr, V. J. (1999). Confirmation that child behavior checklist clinical scales discriminate juvenile mania from attention deficit hyperactivity disorder. Journal of Pediatrics and Child Health, 35, 199–203.
Holtmann, M., Goth, K., Wockel, L., Poustka, F., & Bolte, S. (2007). CBCL-pediatric bipolar disorder phenotype: Severe ADHD or bipolar disorder? Journal of Neural Transmission, 115, 155–161.
Kim, E. Y., & Miklowitz, D. J. (2002). Childhood mania, attention deficit hyperactivity disorder and conduct disorder: A critical review of diagnostic dilemmas. Bipolar Disorders, 4, 215–225.
Kovacs, M. (1992). Children’s depression inventory. NY: North Tonawanda.
Mattison, R., Bagnato, S., Mayes, S., & Felix, B. (1990). Reliability and validity of teacher diagnostic ratings for children with behavioral and emotional disorders. Journal of Psychoeducational Assessment, 8, 509–517.
McGough, J. J., Loo, S. K., Mccracken, J. T., Dang, J., Clark, S., Nelson, S. F., et al. (2008). CBCL pediatric bipolar disorder profile and ADHD: Comorbidity and quantitative trait loci analysis. Journal of the American Academy of Child & Adolescent Psychiatry, 47, 1151–1157.
Mick, E., Biederman, J., Pandina, G., & Faraone, S. V. (2003). A preliminary meta-analysis of the child behavior check list in pediatric bipolar disorder. Biological Psychiatry, 53, 1021–1027.
Orvaschel, H. (1995). Schedule for affective disorders and schizophrenia for school-aged children. Epidemiologic version–5. Fort Lauderdale, FL: Center for Psychological Studies, Nova Southeastern University.
Schniering, C. A., Hudson, J. L., & Rapee, R. M. (2000). Issues in the diagnosis and assessment of anxiety disorders in children and adolescents. Clinical Psychology Review, 20, 453–478.
Shaffer, D., Gould, M. S., Brasic, J., Ambrosini, P., Fisher, P., Bird, H., et al. (1983). A children’s global assessment scale (CGAS). Archives of General Psychiatry, 40, 1228–1231.
Sorgi, P., Ratey, J., Knoedler, D. W., Mardert, R. J., & Reichmann, M. (1991). Rating aggression in the clinical setting: A retrospective adaptation of the overt aggression scale. Journal of Neuropsychiatry and Clinical Neuroscience, 3, S52–S56.
Treiber, F. A., Musante, L., Riley, W., Mabe, P. A., Carr, T., Levy, M., et al. (1989). The relationship between hostility and blood pressure in children. Behavioral Medicine, 15, 173–178.
Volk, H. E., & Todd, R. D. (2007). Does the child behavior checklist juvenile bipolar disorder phenotype identify bipolar disorder? Biological Psychiatry, 62, 115–120.
Wozniak, J., Biederman, J., Kiely, K., Ablon, J. S., Faraone, S. V., Mundy, E., et al. (1995). Mania-like symptoms suggestive of childhood-onset bipolar disorder in clinically referred children. Journal of the American Academy of Child and Adolescent Psychiatry, 34, 867–876.
Youngstrom, E. (2007). Pediatric bipolar disorder. In E. J. Mash & R. A. Barkley (Eds.), Assessment of childhood disorders (Vol. 4, pp. 253–304). New York: Guilford.
Youngstrom, E., Meyers, O., Youngstrom, J. K., Calabrese, J. R., & Findling, R. L. (2006). Diagnostic and measurement issues in the assessment of pediatric bipolar disorder: Implications for understanding mood disorder across the life cycle. Development and Psychopathology, 18, 989–1021.
Youngstrom, E., Youngstrom, J. K., & Starr, M. (2005). Bipolar diagnoses in community mental health: Achenbach child behavior checklist profiles and patterns of comorbitiy. Biological Psychiatry, 58, 569–575.
Yudofsky, S. C., Silver, J. M., Jackson, W., Endicott, J., & Williams, D. (1986). The overt aggression scale for the objective rating of verbal and physical aggression. American Journal of Psychiatry, 143, 35–39.
Acknowledgments
Preparation of this manuscript was supported by a Faculty Development Grant from Assumption College to Leonard A. Doerfler. Portions of this paper were presented at the 43rd annual meeting of the Association of Behavioral and Cognitive Therapies in New York in November, 2009.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Doerfler, L.A., Connor, D.F. & Toscano, P.F. The CBCL Bipolar Profile and Attention, Mood, and Behavior Dysregulation. J Child Fam Stud 20, 545–553 (2011). https://doi.org/10.1007/s10826-010-9426-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-010-9426-z