
Abstract
We examined the relationship between Tourette’s Disorder (TD) and parent reported stress. About 84 parents of children with TD participated by completing questionnaires assessing parental stress, TD symptom severity, co-morbid disorders, services received by the child, and parents’ perception of their child’s academic ability. The results indicate that parent reported stress reached clinically significant levels when a co-morbid disorder was present, but not with a diagnosis of TD alone. Similarly, parents report higher levels of stress when they view their child as performing below other students academically. Finally, the types of services that the child receives were found to have little or no relationship to parent reported stress. Limitations of this study, directions for future research, and implications for intervention are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Tourette’s Disorder (TD) is a neuropsychiatric condition characterized by multiple, repeated, uncontrollable body movements (motor tics) and vocalizations (vocal tics). TD is the most severe of the four types of tic disorders delineated in the Diagnostic and Statistical Manual of Mental Disorder-Text Revision-Fourth Edition (DSM-IV-TR 2000). Diagnostic criteria for TD consists of multiple motor and one or more vocal tics, though not necessarily concurrent, nearly every day for at least 1 year with no “tic-free” periods that last more than 3 months and with onset of tics before age 18 years (American Psychiatric Association (APA) 2000).
Typical age of onset is about age six or seven. Symptoms become more frequent and variable as the child ages, with tics and associated symptoms generally peaking by about age 12. Once considered rare, it is estimated that four in every 10,000 people in the United States have symptoms associated with TD (DSM-IV-TR) (APA 2000). Some studies indicate that the rate may be as high as one in 95 boys and one in 759 girls (Comings et al. 1990). More recently, studies suggest prevalence rates ranging from 0.1% to 3% (Hornsey et al. 2001; Kadesjo and Gillberg 2000; Olson 2004).
Chowdhury and Heyman (2005) conceptualize TD as a spectrum of disorders ranging from mild, transient tics (affecting about 10% of school aged children) to TD complicated by comorbid psychopathology requiring multiple interventions. Though most tic disorders, including TD, require little or no medical treatment (Chowdhury and Heyman 2005), TD is frequently complicated by the presence of comorbid disorders that interfere with management and that complicate intervention. It is estimated that 32–83% of children with TD have Attention Deficit/Hyperactivity Disorder (ADHD) (Comings and Comings 1988). Likewise, rates of comorbidity between TD and Obsessive Compulsive Disorder (OCD) range from 30% to 70% (Carter et al. 1994; Geller et al. 1996; Grad et al. 1987; Kadesjo and Gillberg 2000; Nee et al. 1982; Walkup 1999).
Other comorbid problems include externalizing behavioral problems (oppositional defiant disorder (ODD), aggressive behaviors, conduct problems, and explosive outbursts), depression, and bipolar disorder. Researchers report that 25–35% of children with TD have explosive outbursts, significant temper tantrums, and conduct problems (Budman et al. 2000; Kadesjo and Gillberg 2000; Stefl 1983). Of students with TD and comorbid ADHD, approximately 23% also presented with a co-occurring learning disability (Schuerholz et al. 1996). In addition, children with TD have higher rates of depression and bipolar disorder compared to the general population (Comings and Comings 1987; Kerbeshian et al. 1995). Further, the presence of depression or bipolar disorder is a major predictor of psychiatric hospitalization and dysfunction (Coffey et al. 2000). Finally, as noted, these comorbid conditions may be of more consequence to children and caregivers than the TD itself.
While the individual frequently describes challenges and problems related to TD, family members are also stressed by the disorder. Stefl (1983) reported that family members described themselves as being “bewildered” when TD symptoms first appear. Families with a child, a spouse, or a parent suffering from TD report increased marital difficulties, alcohol problems, and substance abuse problems. Unfortunately, Stefl (1983) did not separate adults and children when analyzing her data, so it is difficult to differentiate family effects when the affected individual is a child versus when the affected individual is an adult.
Until recently, there was little research that directly examined the impact of childhood TD on parent caregivers. Cohen et al. (1988) describe some of the frustrations and limitations that parents feel, noting in particular that parents’ perceptions of their child’s tics are more negative than the perceptions of people outside the family. Furthermore, they reported that the parent–child relationship is influenced more significantly when TD symptoms are accompanied by co-morbid symptoms, especially ADHD and aggression.
To our knowledge, the only controlled study of the impact of TD on caregivers was conducted by Cooper et al. (2003). This investigation compared a group of children with TD to a group of children with asthma from the same outpatient clinic in London. Parents were asked to complete the Child and Adolescent Impact Assessment (CAIA) and the General Health Questionnaire (GHQ). Results indicated that mothers of children with TD had significantly higher rates of mental health problems and felt a significantly greater burden than mothers of children with asthma. These results suggest that the stresses associated with TD exceed those of a chronic, life-threatening physical illness. Moreover, whereas mothers of children with asthma reported that the source of their stress is illness-related, mothers of children with TD reported that the source of their stress was related more to managing the child’s daily activities and to the child’s behavior. Such findings underscore the potential effects of comorbid psychopathology on parent stress.
In one of the first studies to investigate directly the effects of TD on caregivers, Wilkinson et al. (2001) reported a significant correlation between the number of comorbid behavior disorders and the impact that the disorder has on the family. The study is limited in that questionnaires were mailed to members of a local Tourette’s Syndrome Association, so respondents may not be typical. Also, family effects were based on the total score of the Parenting Stress Index—Short Form (Abidin 1995). Still, the authors concluded that the cumulative effect of comorbid conditions exerted a greater influence on family stress than the TD itself. A similar conclusion was reached by Sukhodolsky et al. (2003), who reported that parents indicate that it is the comorbid conditions and not the tics that pose the greatest challenges. In addition, Woods et al. (2005) reported that negative effects on the family are related more to internalizing and ADHD symptoms than tic severity.
Due to the co-morbidity of various disorders in TD, it is useful to review the literature on the effects of these disorders on family functioning. There have been several studies conducted to evaluate how ADHD affects the family and has focused on the interactions between the parent and the child (Barkley and Cunningham 1979; Barkley et al. 1992; Fischer 1990; Mash and Johnston 1990), parental psychopathology (Anastopoulos et al. 1992; Barkley et al. 1992; Fischer 1990; Mash and Johnston 1990), and parent–child conflict resolution (Barkley et al. 1992). In short, researchers have demonstrated that parents of children with ADHD report poor parent–child interactions (Barkley and Cunningham 1979; Barkley et al. 1992; Fischer 1990; Mash and Johnston 1990) and increased maternal depression and anxiety (Barkley et al. 1992; Campbell et al. 1991). Other behavior problems, including oppositionality and conduct problems, have been found to negatively affect spousal agreement and support, marital adjustment, and the social life of parents (Donenberg and Baker 1993; Eyberg et al. 1992; Floyd and Gallagher 1997; Suarez and Baker 1997; Westerman and Schonholtz 1993).
It is also important to examine the reported impact that OCD has on family functioning because of the high rate of co-morbidity of OCD with TS. The impact that obsessive–compulsive symptoms have had on the family has been examined in several studies. Hibbs et al. (1993) reported that mothers of children with OCD had more relationship conflict with other family members, felt that they had achieved less personal growth than the mothers of the normal controls had, and suffered from a psychiatric disorder. Similarly, Cooper (1996) found that family members of a person with OCD felt as though the family member with OCD has negatively affected the personal life as well as the social life of others in the family and has caused marital discord.
Several studies have examined the effects of childhood mood disorders on the family (Kashani et al. 1995; Robertson et al. 2001; Stein et al. 2000; Tamplin et al. 1998). Overall, these studies have demonstrated a significantly negative impact of mood disorders in children and adolescent on family functioning and mental health (Kashani et al. 1995; Stein et al. 2000; Tamplin et al. 1998). Robertson et al. (2001), on the other hand, found no relationship between bipolar disorder or unipolar depression and negative family functioning. The researchers of this study believe that the impact of mood disorders on the family is dependent on how recent the diagnosis and the presence of acute symptoms.
Researchers have also identified several negative sequelae in parents of children with learning disabilities (Al-Yagon 2007; Johnson et al. 2006). Specifically, parents of children with learning disabilities report significantly more symptoms of depression and poor parent coping strategies (Al-Yagon 2007). In addition, parents of children with a learning disability report higher stress levels than parents of children without learning difficulties (Shechtman and Gilat 2005).
While there is some existing research studies that have examined treatments for patients with TD (Bergin et al. 1998; Earles and Myles 1994; Silver et al. 1999; Toren et al. 1999) and the impact that TD has on individuals (Bawden et al. 1998; Kurlan et al. 1996), there is far less research examining the effect that a child with TD has on the family, especially on the primary caregiver. The literature that does exist suggests that the co-morbid mood and behavior disorders as well as learning difficulties associated with TD contribute to parental stress. However, previous literature has not adequately examined the reported parental stress experienced in the presence of a child with uncomplicated TD as compared to TD complicated by comorbid conditions. The purpose of this study was to examine more closely the nature and extent of the relationship between TD, co-morbid conditions, and parental stress. Specific co-morbid conditions explored included ADHD, ODD, CD, OCD, mood disorders, and parent perceived learning difficulties. Co-morbidity is based solely upon parent perception of problems. Therefore, the actual presence of diagnostic criteria was not assessed. Rather, the interest lies in the parent’s perception of the presence and significance of the reported symptoms. Parental stress is conceptualized, for this study, to involve distress experienced by parents as a result of their child’s behavior, the parents’ perception of their ability to manage their child’s needs, and the perceived quality of parent–child interactions.
Our goal for this study was to evaluate the impact that TD and frequently occurring conditions have on parent reported stress. We expected that parents of children with TD will report significantly more parental stress when the TD is accompanied by more than one co-morbid disorder. In particular, we believed co-morbidity in general will contribute more to parent stress than any other variable. In addition, we proposed that TD complicated by ADHD will result in significantly higher parent reported stress. We also believed that TD and comorbid conditions will negatively impact parent perceived academic performance and that parents will report less stress when their child is receiving intervention services in the school and outside of the school than when the child is receiving services in the school only.
Method
Participants
Participants for this study were parents of children with a diagnosis of TD between the ages of 7 and 12. Potential participants were identified through collaboration with the National Tourette’s Syndrome Association, Inc. (TSA). Each TSA state chapter has a database containing the names, addresses, and demographic information (e.g., who in the family has TD, age, gender) of its members. Following approval by the TSA Medical Advisory Board, the Florida, Georgia/South Carolina, and Greater Washington, DC chapters of the TSA were contacted to assist in identifying potential participants for this study.
Research Design
This study was a survey design using data collected through self-report parent questionnaires.
Sample
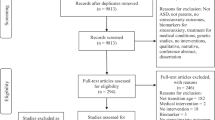
A total of 120 survey packets were mailed to the Florida, Georgia/South Carolina, and Greater Washington, DC chapters of the National Tourette’s Syndrome Association. A total of 84 (34 from Florida, 15 from Georgia/South Carolina, and 35 from Greater Washington, DC) packets were returned completed, for a return rate of 70%. This is considered to be a very positive response rate for survey research (Mangione 1998). Questionnaires in some packets did not have all items completed, hence, the total sample sizes of some comparisons may vary.
Participants
In this study, the mean (SD) age of the child with TD was 10.70 (1.41) years. About 87% were males, and 81% were Caucasian. The remainder of the sample was made up of 1% African American, 6% Hispanic, 2% Asian, and 10% “other” (including multiracial). Seventy-seven percent of the families had an annual income of over $45,000. About 8% had incomes between $30,000 and $45,000, 7% had incomes between $18,000 and $30,000, and 1% had an annual income between $12,000 and $18,000. About 6% of the participants did not respond to that question. Forty-two percent of the participants had a family member in the household with a graduate education. Thirty-one percent had a 4-year degree, 12% had a 2-year degree, 13% had only a high school diploma, and 2% had a GED or did not graduate from high school.
Dependent Measures
Each parent completed a family information form and four rating scales that provided information regarding family demographics, the behavioral characteristics of the child, the child’s school performance, and levels of parental stress.
Family Demographics
A family information data sheet was used to gather information related to marital status, household income, race, parent education, and current medications of the child with TD.
Parenting Stress Index-third Edition Short Form (PSI-SF)
The PSI-SF contains 36 items taken directly from the Parenting Stress Index-Third Edition (PSI, Abidin 1995). The PSI-SF measures three factors: Parental Distress (PD), Parent–Child Dysfunctional Interaction (P-CDI), and Difficult Child (DC). These three factors are combined to provide a Total Stress score. A Total Stress score of 86 or higher is considered clinically significant and suggests that the individual is experiencing significant stress.
Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-kid)
The MINI-kid was used to identify co-morbid conditions. An adaptation of the Mini International Neuropsychiatric Interview (MINI; Sheehan et al. 1998), the MINI-kid is a rewording of the original MINI, intended to increase parent and child understanding of the Interview items. For this study, only the sections of the MINI-kid related to ADHD, OCD, ODD, Conduct Disorder (CD), Depression, and Mania were used. Additionally, four questions were added to assess the presence, frequency, duration, and intensity of rage attacks or outbursts of anger the child demonstrated in the past week. Further modifications were made for this study which involved altering the MINI-kid items from “yes/no” responses to a Likert-type scaling. Each item was worded in such a manner that the parent could rate the presence of the symptom on a scale of 0–3. For this questionnaire, a score of 0 means that the child “Never” exhibits the behavior, a score of 1 means the child “sometimes” exhibits the behavior, a score of 2 means that the child “often” exhibits the behavior, and a score of 3 means that the child exhibits the behavior “Always.” Any item rated with a 2 or a 3 was considered as sufficient for meeting DSM-IV-TR criteria for a particular disorder, because DSM-IV-TR symptoms are considered present if they occur “often.”
Intervention/school Questionnaire
One of the authors (BJW) developed an intervention/school questionnaire that served two purposes. First, the questionnaire identified school-based interventions and community-based interventions that either the parent or the child was receiving. School-based services include all exceptional student education services a child would receive under IDEA (Individuals with Disabilities Education Act), as well as regular education accommodations (including extra test-taking time, tutoring, and academic support). Community-based services include out-of-school tutoring and mental health interventions provided by a psychologist, a therapist, or a psychiatrist.
Second, the questionnaire assessed parental perception of the child’s school performance in reading, math, and writing in relation to other children in the same grade. This information was scored on a Likert-type scale where “0” means that the child is performing below most students, “1” means the student is performing equal to most students, and “2” means the child is performing above most students.
Procedure
Selection of Participants
Participants for this study were enrolled through a multi-step process. First, the computer database of the TSA state chapters was used to identify members with a child between ages 7 and 12 with a diagnosis of TD. Individuals meeting this criterion were sent a letter describing the study and a return postcard with postage for the member to send to their state chapter indicating their intention to participate.
Material Preparation
Each parent packet included the following: A Family Information Form, a PSI, a TODS, a MINI-kid, an Intervention/School Questionnaire, a letter to the parent explaining the study and providing directions for completing the questionnaires, and a self-addressed, stamped envelope for the return of the completed (or non-completed) questionnaires. In an effort to counterbalance response-order effect, the parents were instructed to complete the questionnaires in a specific order.
Mailings
To ensure confidentiality, all mailings were sent from the individual state chapters of the TSA. The researcher sent all prepared materials to the individual chapters where mailing labels were placed on each envelope and packet. To track responses, each packet was assigned a code number and the TSA state chapter assigned one of the numbers to each potential participant. The TSA state chapters kept the “key” so that only they knew to whom each number belongs. This key was used with a follow-up process to maximize participation. Approximately three weeks after the initial mailing, a postcard was mailed to all participants whose packets had not been received as a reminder to complete and return the questionnaires.
Results
To determine the relationships between parent stress and co-morbidity, a Pearson Product Moment Correlation was used to assess the relationship between total parental stress on the PSI-SF and number of co-morbid disorders from the MINI-kid Parent Questionnaire. The number of comorbid disorders reported in 83 of 84 children with TD ranged from zero to four. As Table 1 illustrates, there was a significant positive correlation (r = 0.58099, p < .0001) between the number of co-morbid disorders and parental stress.
To compare the stress reported by parents of children with uncomplicated TD to those with TD with ADHD, a one-way analysis of variance (ANOVA) was used to compare the total parental stress on the PSI-SF of parents of children who had TD (N = 40) and those who had TD with ADHD as the only co-morbid disorder (N = 14). A significant difference was found between the two groups (F(1,52) = 14.93, p = .0003). Parents of children with TD and ADHD had higher total stress scores (M = 102.643, SD = 15.76) than those with TD only (M = 80.65, SD = 19.11). See Table 2 for the results of the ANOVA.
To explore the impact that child intervention utilization has on parent reported stress, a one-way ANOVA was used to compare the parental stress of parents of children who receive no services (N = 18, M = 87.89, SD = 25.84), those who receive only school-based services (N = 24, M = 91.04, SD = 23.05), and those who receive school based and community-based services (N = 34, M = 100.35, SD = 25.68). No significant differences were found between groups (F(2,73) = 1.80, p = .1723). In fact, total stress tends to increase as the child receives additional services.
A Pearson Product Moment Correlation was used to explore the relationship between parent’s perception of their child’s performance in Reading, Writing, and Mathematics to the number of co-morbid disorders. About 81 completed packets were used for this analysis. Significant negative correlations were found between the number of co-morbid diagnoses and parental rating of the student’s reading, writing, and mathematics performance. These results suggest that the child with more co-morbid diagnoses is at greater risk for academic failure. See Table 3 for the results of this analysis.
A 3 × 3 factorial ANOVA was used to test for differences in parent reported stress between groups assigned based upon parental perception of the child’s academic performance (either below, at, or above the performance of other children) in reading, writing and mathematics. About 80 of 84 participants reported their child’s performance in all three academic areas. There was a significant main effect for academic performance across the three subject areas (F(2,231) = 8.73, p = .0002). T-tests were used as post hoc analyses to compare all of the possible pairs (below other children versus same as other children; same as other children versus above other children; and below other children versus above other children) with a Bonferroni adjusted alpha level of .0125 (.05 divided by 4). The results of these analyses indicated that only one of the three possible pairwise comparisons (below other children versus above other children) was significant (F(1,141) = 15.73, p = .0001). The result of this analysis suggests that the parents of children who view their child as performing below other children reported higher levels of total stress than parents who view their child as performing above other children. See Table 4 for a summary of the analysis.
It is worth noting that the level of stress reported by parents of children performing below average increased as the number of co-morbid disorders increased. Further, regardless of the child’s academic performance, parents of children with no co-morbid disorders reported stress below the threshold of clinical significance. The addition of one or more co-morbid disorders, however, resulted in parent reported stress levels within the clinically significant range. Table 5 provides a summary of the relationships between child’s overall level of academic performance in reading, writing, and mathematics, number of co-morbid disorders, and parent reported stress.
Finally, to evaluate the relative contribution of co-morbidity, school performance and use or nonuse of services to parent reported stress, a multiple regression analysis was conducted. Following a forward regression, it was apparent that the number of co-morbid diagnoses was the best predictor, accounting for 33% of the variance in parent reported stress. Parental perception of reading, writing, and math performance accounted for 2, 2, and 0.7% of the variance in parental stress respectively. Use or nonuse of services was not included in the forward selection process. See Table 6 for a summary of the analysis.
Discussion
An earlier study found a significant correlation between the number of comorbid behavior disorders and the impact that TD had on the family (Wilkinson et al. 2001). The current study sought to specify the relative contribution of comorbid conditions and academic performance on parent-reported stress. This section discusses the results of the study, as well as implications for interventions and directions for future research.
In contrast to previous research that reports significant parental stress with TD alone (Carter et al. 1994; Cohen et al. 1988), the present investigation found that parents of children with TD without co-morbid disorders did not report significant levels of stress. Consistent with previous findings that co-morbid disorders are related to parental stress (Sukhodolsky et al. 2003; Wilkinson et al. 2001) the present study found that parent-reported stress is significantly higher when a child has TD and one or more co-morbid disorders. Further studies are needed to determine whether it is characteristics of TD (e.g., symptom severity), the characteristics of the specific co-morbid disorders, or a combination of TD and comorbid conditions that contributed to higher parent reported stress in this sample. For example, previous research has demonstrated that parents of children with ADHD and ODD report clinically significant levels of stress (Anastopoulos et al. 1992; Barkley et al. 1992). Therefore, in children with TD, it may be the presence of externalizing behavior disorders (e.g., ADHD) rather than the TD that produces more parent stress.
There was no relationship between support services provided directly to their child and parental stress. That is, the implementation of school-based interventions did not have an effect on parent reported stress. Therefore, even when parents believe that their child’s educational needs are being addressed by the school system, they continue to experience stress. This finding is consistent with previous research which suggested that child based interventions do not necessarily have positive effects on the rest of the family (Anastopoulos et al. 1993; Harper 1992; Robin 1998). Family-based interventions are typically comprehensive and include a parent education component designed to assist parents in understanding their child’s disorder, counseling for both the parents and child, and facilitating linkages to community-based supports.
The significant negative correlation between co-morbid disorders and academic performance suggests that academic performance declines as the number of co-morbid diagnoses increases. This is consistent with the results reported by Wodrich (1998) that linked TD and co-morbid behavioral and emotional symptoms with poorer academic performance. Reports from Wodrich (1998) and the present study provide strong support for the notion that it is the combination of TD and other co-morbid conditions that negatively affects academic performance. This is not surprising, in as much as the characteristics associated with externalizing behavior disorders (e.g., inattention, hyperactivity, and defiance) have been shown to exert a negative effect on academic performance (Kuhne et al. 1997). Students with externalizing behavior disorders have difficulty remaining engaged with academic tasks, and as a result, have reduced learning opportunities compared with students without these problems.
This study found that parents of a child with TD, complicated by co-morbid disorders, experienced more stress when the child was performing poorly in school. Rather than the TD or the addition of academic problems, it was the presence of externalizing disorders that affected stress. This finding is consistent with previous research that demonstrated that parents of children with learning difficulties (e.g., learning disabilities) and externalizing behavior problems report significantly higher levels of stress than parents of students without learning problems (Baker and McCal 1995; Michaels and Lewandowski 1990). That parents in the current study reported higher levels of stress when academic performance declined is consistent with earlier reports. These results suggest that co-morbid disorders rather than academic performance influence parental stress.
School psychologists and other school-based mental health professionals play an integral role in intervention planning for students with learning and behavioral problems. Because interventions are typically implemented and monitored by teachers and parents, it is important to consider factors that could influence parent and teacher effectiveness. The results of this study demonstrate that TD and co-morbid disorders are related to parent reported stress. Elevated parental stress could, in turn, influence parent effectiveness in implementing interventions. These findings have several implications for psychologists and others who work with students with TD. First, the effects of co-morbid disorders must be considered when designing interventions for children with TD. Second, when possible, family-based interventions should be incorporated along with school-based interventions when developing strategies to reduce parental stress. As part of intervention development, psychoeducation regarding the potential impact of TD and comorbid conditions on parental stress should be discussed with the child’s family.
The present study has two primary limitations: sampling bias and the use of self-report measures for data collection. External validity is influenced because participants were recruited solely from members of the TSA. As a result, the support and education regarding TD that the families receive from the TSA may reduce the negative effects of TD on the caregivers. Furthermore, specific demographic characteristics of the participants indicate a need for caution in interpreting the results. For example, 77% of the participants reported incomes of more than $45,000 per year and 42% of the participants had a family member in the home with some graduate level education. Neither of these may be representative of families of children with TD.
Second, self-report measures limit the interpretation of the study (Bordens and Abbott 1996). Self-report questionnaires do not measure behavior directly; instead, they provide the rater’s perception of the behavior. Perception may be influenced by extraneous factors. For example, reports of previous behavior may be influenced by subsequent events as well as behaviors occurring at the time of questionnaire completion. In addition, honesty is in question when data are collected by self-report questionnaires. Participants may report in such a way as to make themselves appear more socially acceptable. Finally, the psychometric properties of several of the scales used in this study (i.e., the MINI-kid Parent Questionnaire, TODS) have not been completely determined. The lack of reliability and validity data for these measures weakens the interpretation of the scores on the measures as well as the results of the study.
These limitations notwithstanding, the results of this and similar investigations suggest that comorbid disorders and academic difficulties contribute significantly to parent reported stress. Professionals should include provisions for the child’s emotional, behavioral, and academic problems in intervention planning. It is also advised that parent education aimed at explaining the relationship between comorbidity and the child’s functional status be a routine part of treatment for TD.
The results of this study suggest a number of directions for future research. First, further exploration of the impact of multiple diagnoses on parental stress is needed. The prevalence of multiple co-morbid disorders in children with TS is very high (e.g., Carter et al. 1994; Comings and Comings 1988; Kerbeshian et al. 1995). There has been little research on the impact of multiple diagnoses on family and child functioning (academic, social, and emotional). Because of the high prevalence and the negative effects of co-morbid disorders, it is important that research continues to identify factors that lead to more effective interventions.
Further studies should examine the impact of co-morbid disorders on school performance. Though some studies have examined the effect of individual disorders on school performance (e.g., Dooley et al. 1999; Silver and Hagin 1990), there are few definitive studies of the impact of multiple disorders on school performance (e.g., Kuhne et al. 1997). Answers to these questions will help practitioners to provide services and individualized interventions for students with multiple needs.
There needs to be additional focus on services provided for children with TS. The findings from this study and previous research (Harper 1992) indicate that typical (child-centered) services provided by schools have little effect on reducing parental stress associated with having a child with TS. Previous research has demonstrated the effectiveness of family-based programs in reducing parental stress caused by having a child with a chronic condition (Anastopoulos et al. 1993; Harper 1992; Robin 1998). However, there has been little research demonstrating how schools can address, effectively, the needs of families with these children. Research should also study the impact of interventions for children with TS and co-morbid disorders. Current research focuses on the ineffectiveness of traditional interventions for the TS population (Wodrich 1998). In addition, there needs to be more research that helps to guide practitioners in addressing symptoms; for example, should intervention address one behavior at a time or a combination of behaviors/symptoms? Finally, it is critical to identify those services that help students with TS perform well. These findings will inform providers as to the resiliency characteristics found in some children with TS, and lead to interventions aimed at fostering those characteristics in others, to help them to become more successful.
References
Abidin, R. R. (1995). Parenting stress index, third edition: Professional manual. Odessa, FL: Psychological Assessment Resources, Inc.
Al-Yagon, M. (2007). Socioemotional and behavioral adjustment among school-age children with learning disabilities: The moderating role of maternal personal resources. The Journal of Special Education, 40, 205–217.
American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders—4th edition—text revision (DSM-IV-TR). Washington, D.C.: Author.
Anastopoulos, A. D., Guevremont, D. C., Shelton, T. L., & DuPaul, G. J. (1992). Parenting stress among families of children with attention deficit hyperactivity disorder. Journal of Abnormal Child Psychology, 20, 503–520.
Anastopoulos, A. D., Shelton, T. L., DuPaul, G. J., & Guevremont, D. C. (1993). Parent training for attention-deficit hyperactivity disorder: Its impact on parent functioning. Journal of Abnormal Child Psychology, 21, 581–596.
Baker, D. B., & McCal, K. (1995). Parenting stress in parents of children with attention-deficit hyperactivity disorder and parents of children with learning disabilities. Journal of Child and Family Studies, 4, 57–68.
Barkley, R. A., Anastopoulos, A. D., Guevremont, D.C., & Fletcher, K. E. (1992). Adolescents with attention deficit hyperactivity disorder: Mother-adolescent interactions, family beliefs and conflicts, and maternal psychopathology. Journal of Abnormal Child Psychology, 20, 263–288.
Barkley, R. A., & Cunningham, C. E. (1979). The effects of methylphenidate on the mother–child interactions of hyperactive children. Archives of General Psychiatry, 36, 201–208.
Bawden, H. N., Stokes, A., Camfield, C. S., Camfield, P. R., & Salisbury, S. (1998). Peer relationship problems in children with Tourette’s disorder or diabetes mellitus. Journal of Child Psychology and Psychiatry, 39, 663–668.
Bergin, A., Waranch, H. R., Brown, J., Carson, K., & Singer, H. S. (1998). Relaxation therapy in Tourette syndrome: A pilot study. Pediatric Neurology, 18, 136–142.
Bordens, K. S., & Abbott, B. B. (1996). Research design and methods: A process approach (3rd ed.). Mountain View, CA: Mayfield Publishing Company.
Budman, C. L., Bruun, R. D., Park, K. S., Lesser, M., & Olson, M. (2000). Explosive outbursts in children with Tourette’s disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 1270–1276.
Campbell, S. B., March, C. L., Pierce, E. W., Ewing, L. J., & Szumowski, E. K. (1991). Hard-to-manage preschool boys: Family context and the stability of externalizing behavior. Journal of Abnormal Child Psychology, 19, 301–318.
Carter, A. S., Pauls, D. L., Leckman, J. F., & Cohen, D. J. (1994). A prospective longitudinal study of Gilles de la Tourette’s syndrome. Journal of the American Academy of Child and Adolescent Psychiatry, 33, 377–385.
Chowdhury, U., & Heyman, I. (2005). Tourette’s syndrome in children. Retrieved June 3, 2005, from http://www.bmj.bmjjournals.com/cgi/content/full/329/7479/1356.
Coffey, B. J., Biederman, J., Geller, D. A., Spencer, T. J., Kim, G. S., Bellordre, C. A., Frazier, J. A., Cradock, K., & Magovcevic, M. (2000). Distinguishing illness severity from tic severity in children and adolescents with Tourette’s disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 556–561.
Cohen, D. J., Ort, S. I., Leckman, J. F., Riddle, M. A., & Hardin, M. T. (1988). Family functioning and Tourette’s syndrome. In D. Cohen, R. Brunn, & J. Leckman (Eds.), Tourette’s syndrome and tic disorders (pp. 179–196). New York: John Wiley.
Comings, B. G., & Comings, D. E. (1987). A controlled study of Tourette syndrome. V: Depression and mania. American Journal of Human Genetics, 41, 804–821.
Comings, D. E., & Comings, B. G. (1988). Tourette’s syndrome and attention deficit disorder. In D. Cohen, R. Brunn, & J. Leckman (Eds.), Tourette’s syndrome and tic disorders (pp. 119–135). New York: John Wiley.
Comings, D. E., Himes, J. A., & Comings, B. G. (1990). An epidemiologic study of Tourette’s syndrome in a single school district. Journal of Clinical Psychiatry, 51, 463–469.
Cooper, M. (1996). Obsessive compulsive disorder: Effects on family members. American Journal of Orthopsychiatry, 66, 296–304.
Cooper, C., Robertson, M. M., & Livingston, G. (2003). Psychological morbidity and caregiver burden in parents of children with Tourette’s disorder and psychiatric comorbidity. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 1370–1375.
Donenberg, G., & Baker, B. L. (1993). The impact of young children with externalizing behaviors on their families. Journal of Abnormal Child Psychology, 21, 179–198.
Dooley, J. M., Brna, P. M., & Gordon, K. E. (1999). Parent perceptions of symptom severity in Tourette’s syndrome. Archives of Disabled Children, 81, 440–441.
Earles, T. L., & Myles, B. S. (1994). Using behavioral interventions to decrease coprolalia in a student with Tourette’s syndrome and autism: A case study. Focus on Autistic Behavior, 8(6), 1–10.
Eyberg, S. M., Boggs, S. R., & Rodriguez C. M. (1992). Relationships between maternal parenting stress and child disruptive behavior. Child and Family Behavior Therapy, 14(4), 1–9.
Fischer, M. (1990). Parenting stress and the child with attention deficit hyperactivity disorder. Journal of Clinical Child Psychology, 19, 337–346.
Floyd, F. J., & Gallagher, E. M. (1997). Parental stress, care demands, and use of support services for school-age children with disabilities and behavior problems. Family Relations, 46, 359–371.
Geller, D. A., Biederman, J., Griffin, B. A., Griffin, S., Jones, J., Lefkowitz, T. R. (1996). Comorbidity of juvenile obsessive-complusive disorder with disruptive behavior disorders. Journal of the American Academy of Child & Adolescent Psychiatry, 35, 1637–1646.
Grad, L. R., Pelcovitz, D., Olson, M., Matthews, M., & Grad, G. J. (1987). Obsessive–compulsive symptomatology in children with Tourette’s syndrome. Journal of the American Academy of Child and Adolescent Psychiatry, 26, 69–73.
Harper, G. (1992). The family in Tourette syndrome. In T. N. Chase, A. J. Friedhoff, & D. J. Cohen (Eds.), Advances in neurology (pp. 319–322). New York: Raven Press Ltd.
Hibbs, E. D., Hamburger, S. D., Kruesi, M. J. P., & Lenane, M. (1993). Factors affecting expressed emotion in parents of ill and normal children. American Journal of Orthopsychiatry, 63, 103–112.
Hornsey, H., Banerjee, S., Zeitlin, H., & Robertson, M. (2001). The prevalence of Tourette syndrome in 13–14 year olds in mainstream schools. Journal of Child Psychology and Psychiatry, 42, 1035–1039.
Hsueh-Ling, C., Ming-Je, T., & Huei-Shyong, W. (2004). Tourette’s syndrome: Psychopathology in adolescents. Psychiatry and Clinical Neurosciences, 58, 353–358.
Johnson, R. F., O’Reilly, M., & Vostanis, P. (2006). Caring for children with learning disabilities who present problem behaviours: A maternal perspective. Journal of Child Health Care, 10, 188–198.
Kadesjo, B., Gillberg, C. (2000). Tourette’s disorder: Epidemiology and comorbidity in primary school children. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 548–555.
Kashani, J. H., Allan, W. D., Dahlmeier, J. M., Rezvani, M., & Reid, J. C. (1995). An examination of family functioning utilizing the circumplex model in psychiatrically hospitalized children with depression. Journal of Affective Disorders, 35, 65–73.
Kerbeshian, J., Burd, L., & Klug, M. G. (1995). Comorbid Tourette’s disorder and Bipolar disorder: An etiological perspective. American Journal of Psychiatry, 152, 1646–1651.
Kuhne, M., Schachar, R., & Tannock, R. (1997). Impact of co-morbid oppositional or conduct problems on attention-deficit hyperactivity disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 36, 1715–1725.
Kurlan, R., Daragjati, C., Como, P. G., McDermott, M. P., Trinidad, K. S., Roddy, S., Brower, C. A., & Robertson, M. M. (1996). Non-obscene complex socially inappropriate behavior in Tourette’s syndrome. Journal of Neuropsychiatry and Clinical Neurosciences, 8, 311–317.
Mangione, T. W. (1998). Mail surveys. In L. Bickman, & D. J. Rog (Eds.), Handbook of applied social research methods (pp. 399–427). Thousand Oaks, CA: Sage Publications.
Mash, E. J., & Johnston, C. (1990). Determinants of parenting stress: Illustrations from families of hyperactive children and families of physically abused children. Journal of Clinical Child Psychology, 19, 313–328.
Michaels, C. R., & Lewandowski, L. J. (1990). Psychological adjustment and family functioning of boys with learning disabilities. Journal of Learning Disabilities, 23, 446–450.
Nee, L. E., Polinsky, R. J., & Ebert, M. H. (1982). Tourette syndrome: Clinical and family studies. Advances in Neurology, 35, 291–295.
Olson, S. (2004). Making sense of Tourette’s. Science, 305, 1390–1392.
Robertson, H. A., Kutcher, S. P., Bird, D., & Grasswick, L. (2001). Impact of early onset bipolar disorder on family functioning: Adolescents’ perceptions of family dynamics, communication, and problems. Journal of Affective Disorders, 66, 25–37.
Robin, A. L. (1998). Training families with ADHD adolescents. In R. A. Barkley (Eds.), Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment (2nd ed.). New York: The Guilford Press.
Schuerholz, L. J, Baumgardner, T. L., Singer, H. S., Reiss, A. L., & Denckla, M. B., (1996). Neuropsychological status of children with Tourette’s syndrome with and without attention deficit hyperactivity disorder. Neurology, 46, 958–965.
Shechtman, Z., & Gilat, I. (2005). The effectiveness of counseling groups in reducing stress of parents of children with learning disabilities. Group Dynamics: Theory, Research, and Practice, 9, 275–286.
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., Hergueta, T., Baker, R., & Dunbar, G. C. (1998). The mini-international neuropsychiatric interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry, 59(Suppl. 20), 22–33.
Silver, A. A., & Hagin, R. A. (1990). Disorders of learning in childhood. New York: John Wiley & Sons, Inc.
Silver, A. A., Shytle, R. D., & Sanberg, P. R. (1999). Clinical experience with transdermal nicotine patch in Tourette syndrome. CNS Spectrums, 4, 68–76.
Stefl, M. E. (1983). The Ohio Tourette study. Cincinnati: School of Planning, University of Cincinnati.
Stein, D., Williamson, D. E., Birmaher, B., Brent, D. A., Kaufman, J., Dahl, R. E., Perel, J. M., & Ryan, N. D. (2000). Parent–child bonding and family functioning in depressed children and children at high risk and low risk for future depression. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 1387–1395.
Suarez, L. M., & Baker, B. L. (1997). Child externalizing behavior and parents’ stress: The role of social support. Family Relations, 47, 373–381.
Sukhodolsky, D. G., Scahill, L. H. B., Zhang, H., Peterson, B., King, R. A., Lombroso, P. J., Katsovich, L., Findley, D., & Leckman, J. F. (2003). Disrputive behavior in children with Tourette’s syndrome: Association with ADHD comorbidity, tic severity, and functional impairment. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 98–105.
Tamplin, A., Goodyer, I. M., & Herbert, J. (1998). Family functioning and parent general health in families of adolescents with major depressive disorder. Journal of Affective Disorders, 48, 1–13.
Toren, P., Laor, N., Cohen, D. J., Wolmer, L., & Weizman, A. (1999). Ondansetron treatment in patients with Tourette’s syndrome. International Clinical Psychopharmacology, 14, 373–376.
Towbin, K. E. (1988). Obsessive-compulsive symptoms in Tourette’s syndrome. In D. Cohen, R. Brunn, & J. Leckman (Eds.), Tourette’s syndrome and tic disorders (pp. 137–149). New York: John Wiley.
Walkup, J. T. (1999). The psychiatry of Tourette syndrome. CNS Spectrums, 4, 54–61.
Westerman, M. A., & Schonholtz, J. (1993). Marital adjustment, joint parental support in a triadic problem-solving task, and child behavior problems. Journal of Clinical Child Psychology, 22, 97–106.
Wilkinson, B. J., Newman, M. B., Shytle, R. D., Silver, A. A., Sanberg, P. R., Sheehan, D. S. (2001). Family impact of Tourette’s syndrome. Journal of Child and Family Studies, 10, 477–483.
Wodrich, D. L. (1998). Tourette’s syndrome and tics: Relevance for school psychologists. Journal of School Psychology, 36, 281–294.
Woods, D. W., Himle, M. B., & Osmon, D. C. (2005). Use of the impact on family scale in children with tic disorders: Descriptive data, validity, and tic severity impact. Child & Family Behavior Therapy, 27, 11–21.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wilkinson, B.J., Marshall, R.M. & Curtwright, B. Impact of Tourette’s Disorder on Parent Reported Stress. J Child Fam Stud 17, 582–598 (2008). https://doi.org/10.1007/s10826-007-9176-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-007-9176-8