
Abstract
A sample of 63 licensed foster parents was asked, “What motivates you to foster a child who has a fetal alcohol spectrum disorder?” The responses to this question were grouped together by licensed foster parents. The grouped data were subjected to multidimensional scaling and cluster analysis. Results indicated that foster parents were motivated to care for children with alcohol-related disabilities by witnessing positive changes in the children in their care, helping children focus on their strengths, using their own parenting experience, earning an income, assisting children who have disabilities, and helping children stay connected to their families and communities. Foster parents who foster children with alcohol-related disabilities foster for similar reasons to those who foster children with special needs in general. Differences between the literature on foster parent motives and study results were described. Foster parents who are caring for children with alcohol-related disabilities see their care as specialized, see their roles as long-term helpers facilitators to children, their birth families and home communities, and emphasize positive experiences of fostering.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Since Jones and colleagues first identified ‘fetal alcohol syndrome’ (Jones & Smith, 1973; Jones, Smith, Ulleland, & Streissguth, 1973), there has been a great deal of research and discussion about causes and impact. It has been estimated that, based on the frequency and patterns of drinking among women of childbearing age, combined with rates of unintended pregnancy (Centers for Disease Control, 1999; Ebrahim, Anderson, & Floyd, 1999), about 2 in every 100 North American women could be at risk of an alcohol-affected pregnancy each year (Project CHOICES Research Group, 2002). The frequency of Fetal Alcohol Syndrome (FAS) varies, depending on the timing, location and measures used; many estimates fall between 0.2 and 2.0 per 1000 live births (Centers for Disease Control, 2002).
FAS includes facial abnormalities, growth deficits, and central nervous system abnormalities (National Center on Birth Defects and Developmental Disabilities, 2004). The full spectrum of alcohol-related disorders includes five diagnostic categories, including Fetal Alcohol Syndrome (FAS) with confirmed prenatal exposure, FAS without confirmed prenatal exposure, Partial FAS (pFAS), Alcohol-Related Neurodevelopmental Disorder (ARND), and Alcohol-Related Birth Defects (ARBD) (American Academy of Pediatrics, 2000). The combined frequency of disorders in the fetal alcohol spectrum is approximately 9–10 per 1000 (Health Canada, 2004).
Children with alcohol-related diagnoses are overrepresented in the child welfare system (Aronson & Hagberg, 1998). Previous research has identified several challenges faced by foster parents caring for a child with an alcohol-related disability, including behavioural problems (Brooks & Barth, 1998), finding and maintaining appropriate educational programs (Giunta & Streissguth, 1988), adequate financial resources (Rhodes, Orme, & Buehler, 2001), as well as personal support (Fisher, Gibbs, Sinclair, & Wilson, 2000). However, little is known about foster parent's motives for providing care to these children.
An expanded search on foster parent motives to care for children with special needs, such as in treatment foster care—including children with disabilities, children with severe behavioural problems, or those with serious medical conditions—yielded many more hits. Since many foster parents care for children who have a range of special needs (Cox, Orme, & Rhodes, 2002), a broader search of the literature was warranted.
Many different motives for fostering children with special needs have been reported. Motives included a love for children and a desire to see them improve (Goetting & Goetting, 1993). Some foster parents felt it was their duty to help children with special needs (Andersson, 2001), as well as their birth families (Jivanjee, 1999).Caregivers have also identified with a child's need based on their own family experiences or personal experiences in care (Baum, Crase, & Crase, 2001), parenting experience with special needs children or professional experience working with children who have special needs (Cox, Buehler, & Orme, 2002). Foster parents have expressed a concern over the chronic need for out-of-home placements for children with special needs (Beeman & Boisen, 1999), and were influenced to help out by their family, friends or an organization they were members of (Cox, Buehler, & Orme, 2002). Some foster parents wanted to fill the void left by the loss of a child (Gillis-Arnold, Crase, Stockdale, & Shelley, 1998) or to provide companionship for their children or themselves (Dando & Minty, 1987). Other reasons included wanting children but being unable to conceive (Tyebjee, 2003), and wanting fulfillment of their own preferred family and work roles (Stromberg, 1994).
In the present study, licensed foster parents within a central Canadian province who had fostered a child with an alcohol-related diagnosis were asked about their motives for caring for the child. Responses were analyzed using the concept mapping method (Trochim, 1987), a quantitative approach to qualitative data analysis, which has been used frequently in the social sciences (Paulson & Everall, 2003; Schuck & Liddle, 2004). Their responses will be compared to the available literature on the motives of foster parents to care for children with special needs.
Concept mapping was selected because it appeared to be a novel approach to this research question. We could find no other published studies of foster parent motives for caring for children with special needs that utilized cluster analysis techniques. These techniques are particularly appropriate for sorting cases into groups that maximize within-group similarity (Henry, Tolan, & Gorman-Smith, 2005). A major advantage of concept mapping is that each participant has the opportunity to view and group together the responses from all participants. These groupings are statistically analyzed and combined so that the results equally represent those of each participant. The participants, not the researchers, are the experts. The role of the researcher is to collect data and assign descriptive names to the themes that the participants themselves define through the generation and sorting of statements they collectively make. In the end, the participants define the issues and determine the extent to which they are similar to each other.
Method
According to Trochim (1989), there are six major components to the concept mapping process. The first step is the generation of responses to a particular question asked of a specified group of participants. Second, these responses are edited for clarity. Redundant responses are removed. Third, the responses are sorted into groups of similar responses. The groups are considered to represent general themes. Fourth, two types of statistical analysis are applied to the groupings of statements to describe the relationship statements and their groupings. A decision is made about the optimal number of concepts. Fifth, the major concepts are identified according to the contents of the cluster. Sixth, the map is used for its intended purpose: a graphical representation of the conceptualization process.
Participants and question
A randomized list of home telephone numbers for all licensed foster homes throughout a central Canadian province was provided to the researchers by the provincial authority. Researchers telephoned the home, and asked to speak with a parent. Each parent was asked if there was another parent in the home, and if so, permission was asked to speak to that person. In 12 homes, both parents consented to an interview. In 51 homes, only one parent was interviewed. In 8 homes, there was one foster parent. In the remainder (43), either the other parent was unavailable and could not be contacted (e.g. working out of town for long periods), or declined an interview.
All participants were provided with a verbal description of the study, informed that participation was voluntary, and that their responses would be kept confidential and anonymous. They were also told that they could choose not to answer particular questions and withdraw from the study at any time. Participants provided verbal consent to participate in a telephone interview at a mutually agreeable time. Demographic data were collected in order to judge the variability of the sample. According to demographic characteristics considered relevant to sampling foster parents in this jurisdiction, including urban/rural location, population and region, years of experience, number of placements and number currently placed, the sample reflected sufficient variability.
Participants were asked one screening question: “have you fostered a child with an alcohol-related diagnosis in the past year?” Data collection continued until a point of redundancy, where no novel responses were received in three consecutive interviews across participants. In this study, redundancy was reached after interviewing 63 parents. The majority (43) of the 63 participants were female. Most participants (40/51) resided in urban areas. Many (38/51) families resided in cities, with a population of over 100,000. All nine regions of the province were represented in amounts consistent with the population of each. Participants had fostered for 1–35 years, had from 0 to 5 foster children in their care at the time of interview, and had fostered from 1 to over 100 children.
Each telephone interview included the open-ended question: “What motivates you to foster a child who has a fetal alcohol spectrum disorder?”
Generation of statements
Participants generated responses to the question. These statements represented the domain of interest (Trochim, 1989). Statements were edited for clarity using an inter-rater agreement process. Two authors and a teacher reviewed the statements independently to identify those that were unclear or redundant. The raters compared their ratings and arrived at agreement for each statement. If a statement was redundant, it was removed (e.g. “love for children” and “I love children”). If a statement was unclear, changes were made to improve clarity (e.g. “was raising my young children at home,” changed to “was already parenting young children at home” so that its meaning was clearer for sorters). Male and female responses were initially kept separate. Because there were no apparent differences between the statements by gender, they were combined for the purposes of analysis into a list of 43.
Structuring of statements
At the time of interview, foster parents were asked if they would be interested in sorting the responses into groups. Those participants were contacted by researchers and invited to participate in the sorting task. Of those contacted, 25 were interested. Each was given a verbal description of the sorting procedure. An independent unstructured card sorting procedure was used (Rosenberg & Kim, 1975). Each of the 43 statements was printed on a separate numbered card from 1 to 43. A set of 43 cards, in random order, was mailed to each participant, along with written instructions and a telephone number of a research assistant who they could call with any questions. Participants were asked to read through the cards and group them together in “a way that makes sense to you.” They were told that they could have as many groups as they wished, and provided with a form to record the contents of each group by listing the identifying numbers of the statements. One week after the cards were mailed, a research assistant contacted the participants to confirm receipt and answer any questions. A total of 16 sorts were returned.
Representation of statements
The sort data were analyzed by two statistical procedures. Multidimensional scaling placed the statements spatially on a map, and hierarchical cluster analysis placed the points into clusters representing higher order groupings. The study utilized the Concept System (Trochim, 1987) to conduct these analyses.
To prepare for the analysis, the sort information was placed on an N×N binary, symmetric matrix of similarities, X ij .(Trochim, Cook, & Setze, 1994). For any two items i and j a 1 was placed in X ij if the items were placed in the same pile by the participant (Weller & Romney, 1988). If they were not, a 0 was entered. The total N×N matrix was based on the sums of individual matrices. Any cell in the total matrix could have a value from 0 to 16 (the number of people grouping the statements), indicating the number of people who placed the i and j pair in the same group.
Multidimensional scaling
The purpose of multidimensional scaling is to “represent and provide a basis for understanding the structure inherent in certain types of data involving judgments about stimuli” (MacCallum, 1988, p. 421). In concept mapping, the MDS was limited to two dimensions where the points were placed in a bivariate distribution, because it was easier to work with two-dimensional configurations (Kruskal & Wish, 1978).
The result of this analysis was a two-dimensional representation of the set of statements, based on the logic that statements grouped together by participants most often are more closely situated to each other than statements grouped by participants least often, which are situated further apart.
Cluster analysis
A second analysis was performed to represent the conceptual domain (Trochim, 1989). Hierarchical cluster analysis of the multidimensional scaling values was used (Anderberg, 1973; Everitt, 1980). The analysis used Ward's (1963) minimum variance technique which is a widely used agglomerative hierarchical technique in the behavioural sciences (Blashfield & Anderderfer, 1988; Borgen & Barnett, 1987). The use of MDS solution as the starting point for cluster analysis, forces the analysis to divide the MDS solution into non-overlapping clusters on the two-dimensional space (Trochim et al., 1994).
Number of concepts
Since there is no clear quantitative criterion for the selection of the most appropriate number of concepts, the decision was made by the researchers based on the conceptual fit of the statements within the various cluster solutions generated, and the items contributing most to the uniqueness of each cluster using the average and individual bridging indices. Cluster solutions from 12 to 4 were examined before concluding that the six-cluster solution fit the data best. The 12-cluster solution appeared fragmented with no clear themes apparent. By reducing the number of clusters by two, additional solutions were examined. Insignificant changes were introduced from reducing the number to ten, and then eight. However, reducing the eight-cluster solution to six represented a substantial improvement. Further reduction to the six-cluster solution down to five clusters collapsed the clusters “Positive Change” and “Make Contribution,” and when collapsed further to four clusters, “Parenting Experience” and “Obligation” were collapsed. Both the five- and four-cluster solutions appeared to be over-generalized and less useful. The six-cluster solution provided the best interpretability.
Interpretation and utilization of maps
Following the statistical analysis, the authors labelled concepts based on the statements in each. The resulting map provided a visual summary of the results.
Results
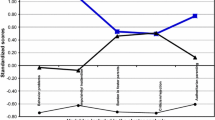
The concept map appears in Fig. 1. Each number, identified by a point on the map, corresponds to a numbered statement in Table 1. Foster parents grouped the 43 statements into six concepts. Foster parents reported that they were motivated to care for children with alcohol-related disabilities by: witnessing positive changes in the children while in their care (Concept One), helping children focus on their strengths (Concept Two), using their own parenting experience (Concept Three), earning an income (Concept Four), wanting to help children who have disabilities (Concept Five), and helping children to stay connected to their families and communities (Concept Six).

Concept map of 43 statements
Discussion
Concept one: Child's positive change
In this concept, the issues of fostering to help a child change or adapt to a disability were raised. There are references in the literature about foster parents wanting to nurture children (Dando & Minty, 1987), help special needs children as well as families (Jivanjee, 1999) (Beeman & Boisen, 1999), and see them improve, in general, (Goetting & Goetting, 1993). However, there is little emphasis on the perceived benefits and drawbacks of particular types of parenting style, as well as family and community supports that may be useful and appropriate, from a foster parent's perspective.
Concept two: Make contribution
Motives associated with making a contribution to the welfare of special needs children are well supported in the existing literature. The desire to nurture children facing multiple challenges is often reported by foster parents as a motivating factor (Stromberg, 1994). Indeed, parents in our study recognized their potential face a high degree of challenge fostering a child with special needs. According to the literature, a love for children (Goetting & Goetting, 1993) may translate into “rescuing” a special needs child (Gillis-Arnold et al., 1998). However, parents in our study did not identify strongly with the notion of rescuing children; they wanted to contribute to positive development in children with disabilities, and expressed only some concern about risk for negative outcomes.
Concept three: Parenting experience
In this concept, foster parents described motives associated with their own positive experiences as parents. In the literature, there is mention of fostering as a way to provide siblings for one's own children (Baum et al., 2001), companionship (Gillis-Arnold et al., 1998), or have children when that is not otherwise possible (Andersson, 2001). According to Stromberg (1994), fulfilment of desired family roles is a motive parents give for fostering children with special needs. Parents we spoke with focussed on both having something to give and something to gain by fostering children with special needs. Although the notion of professional experience working with children who have special needs was found in the literature as a motive (Cox, Buehler, & Orme, 2002), there was no reference made to this by participants in our study. Instead, participants in this study noted that they had learned about special needs children by attending training workshops.
Concept four: Obligation
There are several references in the literature to fostering because of a sense of responsibility as well as financial reasons. Some parents are motivated to foster special needs children because of a sense of responsibility or duty (Cox, Buehler, & Orme, 2002), both in general, because of a shortage of suitable placements (Beeman & Boisen, 1999), or for a particular child because they know she is in need (Baum et al., 2001).
Parents may decide to foster children with special needs because they are financially well off (Tyebjee, 2003). However, fulfillment of their preferred work role, which includes earning an income at home, motivates some to foster special needs children (Stromberg, 1994).
Concept five: Confidence in ability
Foster parents in our study reported that they had learned a lot about parenting children with special needs. In the literature, however, there was little attention to motives related to putting their knowledge into practice. Though we could find reference in the literature to identifying with a child in need (Dando & Minty, 1987), there was little connection to understanding children with special needs or the expertise of parents as a reason why they would foster. Participants in this study described themselves as motivated by their competence as parents who have experience and willingness to learn about caring for children with special needs.
Concept six: Help children
In this concept, foster parents described their motives for fostering as keeping children connected to their families and communities. They recognized a need for homes for children with special needs, and wanted to help out. This is consistent with the available literature (Tyebjee, 2003). The children waiting for foster care outnumber available foster homes. Many of the children have special needs. For these reasons, a sense of social concern, or helping the community, may be a motive for becoming a foster parent (Cox, Buehler, & Orme, 2002). Opening one's home to a child in need may be considered an altruistic action. It may satisfy a person's need to appear good in the eyes of others, or simply provide personal satisfaction (Cox, Buehler, & Orme, 2002). This sense of social responsibility has been found to motivate foster parents to care for children with special needs (Beeman & Boisen, 1999).
Conclusions
In general, there are many similarities between motives that have been reported in the literature for fostering children with special needs, and those reported by foster parents in our study who spoke specifically about fostering children with alcohol-related disabilities. Indeed, it appears that foster parents who foster children with alcohol-related disabilities foster for similar reasons to those who foster children with special needs, in general. Both sources identify a variety of personal, family and community reasons for fostering, with benefits to themselves and their own families as well as others, such as foster children, birth families and communities.
However, there are also some differences. Foster parents who were caring for children with alcohol-related disabilities saw their expertise as more specialized, their roles as ‘helpers’ to children, families and communities, and emphasized the positive effects of fostering on their own and their foster children's lives. These are key differences between the literature on motives for fostering children with special needs, and the motives reported by parents in the present study.
Foster parents in our study saw themselves as having expertise not just as parents but also as parents who can foster children with particular disabilities. They saw a range of supports as necessary for alcohol-affected children in the longer term, including peers, school and family; their role included putting those resources into place for the child to have longer-term success. They also saw the need for education and training to continue to develop their own knowledge and skills. In the interest of recruiting and retaining foster parents who are successful with children who have alcohol-related disabilities, the willingness to be involved with a variety of community support services and continuing education appear to be significant factors.
Parents fostering children with alcohol-related disabilities saw their roles in broad terms. They described a need for long term planning for children with these disabilities, and their role as part of a support network, including other family members—their own and the birth family—as well as community members. They described the need for a community response to the issues affecting children and families because all members have a responsibility to these children, and share in their success and challenges. Foster parents who are well suited to care for children with alcohol-related disabilities may be those who are good facilitators, and can build broad and inclusive networks of support including the child's peers, other families in the community, as well as professionals.
Finally, the parents we spoke to, in contrast to a literature that focuses on problems faced by children with special needs, focused on strengths. Parents who foster alcohol-affected children spoke in very positive terms about the children, the individualistic nature of “success” and “progress,” the need for people who attend to, encourage, and reinforce positive change, in whatever way the child and family envision it. This emphasis on strengths includes recognition of both self-determination and collective responsibility. Parents who are realistic and practical about challenges and strategies to overcome them, see the good in what the child and family are doing, and work to build a support system for the long term, seem well-suited to fostering those with alcohol-related disabilities.
This study was not without its limitations. Participants were drawn from a registry of licensed foster homes in one jurisdiction, which is not representative of parents in other locations. The response rate to the telephone interviews was 73%, and is therefore possible that who consented to participate differed from those who did not. Of those who participated in the interview, only a small number (16/63) completed the sorting task. The way they grouped responses might somehow differ from the way non-respondents would have completed this task. Finally, because no frequency data were collected on the responses, we were unable to describe relative importance of the responses or resulting themes. This may be a topic to be explored in future research on this issue.
This study has implications for foster parent recruitment, retention and training. Foster parents in this study were motivated to foster alcohol-affected children for reasons that were generally similar to those reported in previous work on the motives foster parents have for caring for children with a range of special needs. While some foster parents are motivated to care for children who have special needs, the particular motives vary from parent to parent. Given the challenges associated with placement stability for alcohol-affected children, in particular, specific efforts should be made to recruit those who are interested in special needs fostering, and emphasize the aspects of fostering that are most salient to those parents. Recruitment efforts should be organized along the lines of reasoning that are most salient to potential foster parents. The study, and others like it, suggest that foster parents who care for special needs children in general, and alcohol-affected children in particular, are motivated to foster because they feel some obligation to do so, want to make a difference in the lives of children and families, feel prepared to make that commitment, and expect to see something positive coming out of the experience for the child. The realities of low pay and multiple challenges that also await them are important to incorporate into recruitment efforts, so that expectations are realistic.
Because children who are alcohol-affected fare worse, in general, than other children in the foster care system, as evidenced by elevated rates of placement breakdown and exposure to alternative non-foster placements, great care should be taken to set up placements that have the potential to be long term in nature. Because there is no one motive that all parents subscribe to, any one could be a deal-breaker, and thereby contribute to a broken down placement. Some foster parents foster alcohol-affected children because they ‘like the job’. Others do it because they feel that it is their duty to help out a particular child or a family, or make a contribution within the broader community in which they live. Some others feel particularly prepared, because of their personal or educational experience to foster children with alcohol-related disabilities. Envisioning fostering as a ‘job’, a ‘calling’ or a ‘profession’ has implications for the way their efforts are most appropriately supported and recognized by the system. Each of these parents is motivated to foster, but their reasons for doing so differ, and no one approach to retention can be expected to meet the needs of each.
The training of foster parents to care for a child with an alcohol-related disability could be delivered in the context of care giving for special needs children, in general. That is, there is no evidence from a motives perspective, to suggest that fostering alcohol-affected children is dramatically different than fostering children with other special needs. However, there are some issues, such as those related to diagnosis and specialized support services for alcohol-affected children that should be specifically addressed in training. Preferred approaches to training might well vary, depending on the particular motives that foster parents have for fostering special needs children. Indeed, their perceptions of what a ‘qualified’ trainer might look like and information perceived as useful, may well be different if one sees fostering as a professional endeavour, a charitable act, or a way to earn a living.
REFERENCES
American Academy of Pediatrics. (2000). Fetal alcohol syndrome and alcohol-related neurodevelopmental disorders. Pediatrics, 106, 358–361.
Anderberg, M. R. (1973). Cluster analysis for applications. New York: Academic Press.
Andersson, G. (2001). The motives of foster parents, their family and work circumstances. British Journal of Social Work, 31, 235–248.
Aronson, M., & Hagberg, B. (1998). Neuropsychological disorders in children exposed to alcohol during pregnancy: A follow-up study of 24 children to alcoholic mothers in Goteborg, Sweden. Alcohol Clinical and Experimental Research, 22, 321–324.
Baum, A. C., Crase, S. J., & Crase, K. L. (2001). Influences on the decision to become or not become a foster parent. Journal of Contemporary Human Services, 82, 202–213.
Beeman, S., & Boisen, L. (1999). Child welfare professionals’ attitudes toward kinship foster care. Child Welfare, 78, 315–337.
Blashfield, R. K., & Aldenderfer, M. S. (1988). The methods and problems of cluster analysis. In J. R. Nesselroade & R. B. Cattell (Eds.), Handbook of multivariate experimental psychology (pp. 447–473). New York: Plenum.
Brooks, D., & Barth, R. P. (1998). Characteristics and outcomes of drug-exposed and non drug-exposed children in kinship and non-relative foster care. Children and Youth Services Review, 20, 475–501.
Borgen, F. H., & Barnett, D. C. (1987). Applying cluster analysis in counselling psychology research. Journal of Counselling Psychology, 34, 456–468.
Centers for Disease Control. (1999). Alcohol use among women of childbearing age—United States. Morbidity and Mortality Weekly Report, 51, 273–276.
Centers for Disease Control. (2002). Fetal alcohol syndrome—Alaska, Arizona, Colorado, and New York, 1995–1997. Morbidity and Mortality Weekly Report, 51, 433–435.
Cox, M. E., Buehler, C., & Orme, J. G. (2002). Recruitment and foster family service. Journal of Sociology and Social Welfare, 4, 151–177.
Cox, M. E., Orme, J. G., & Rhodes, K. W. (2002). Willingness to foster special needs children and foster family utilization. Children and Youth Services Review, 24, 293–317.
Dando, I., & Minty, B. (1987). What makes good foster parents? British Journal of Social Work, 17, 383– 400.
Ebrahim, S. H., Anderson, A., & Floyd, R. L. (1999). Alcohol consumption by reproductive-aged women in the USA: An update on assessment, burden and prevention in the 1990s. Prenatal and Neonatal Medicine, 4, 419–430.
Fisher, T., Gibbs, I., Sinclair, I., & Wilson, K. (2000). Sharing the care: The qualities sought of social workers by foster carers. Child and Family Social Work, 5, 225–233.
Gillis-Arnold, R., Crase, S. J., Stockdale, D. F., & Shelley, M. C. (1998). Parenting attitudes foster parenting attitudes, and motivations of adoptive and nonadoptive foster parent trainees. Children and Youth Services Review, 20, 715–732.
Giunta, C. T., & Streissguth, A. P. (1988). Patients with fetal alcohol syndrome and their caretakers. Social Casework, 69, 453–459.
Goetting, A., & Goetting, M. G. (1993). Voluntary parents to multiple children with special needs: A profile. Journal of Child and Family Studies, 2, 353–369.
Health Canada. (2004). Fetal alcohol spectrum disorder: A framework for action. Retrieved July 5, 2004, from http://www.hc-sc.gc.ca/dca-dea/publications/fasd-etcaf/framework_e.html.
Henry, D. B., Tolan, P. H., & Gorman-Smith, D. (2005). Cluster analysis in family psychology research. Journal of Family Psychology, 19, 121–132.
Jivanjee, P. (1999). Professional and provider perspectives on family involvement in therapeutic foster care. Journal of Child and Family Studies, 8, 329–341.
Jones, K. L., & Smith, D. F. (1973). Recognition of the fetal alcohol syndrome in early infancy. Lancet, 2, 999–1001.
Jones, K. L., Smith, D. F., Ulleland, D. W., & Streissguth, A. (1973). Pattern of malformation in offspring of chronic alcoholic mother. Lancet, 1, 1267–1271.
Kruskal, J., & Wish, M. (1978). Multidimensional scaling. Beverly Hills, CA: Sage.
MacCallum, R. (1988). Multidimensional scaling. In J. R. Nesselroade and R. B. Cattell (Eds.), Handbook of multivariate experimental psychology (pp. 421–445). New York: Plenum.
Mathiesen, S. G., Jarmon, B., & Clarke, L. (2001). Searching for family: Voices of Florida's foster children. Journal of Family Social Work, 6, 15–33.
National Center on Birth Defects and Developmental Disabilities (2004). Fetal alcohol syndrome: Guidelines for referral and diagnosis. Atlanta: Centres for Disease Control.
Paulson, B. L., & Everall, R. D. (2003). Suicidal adolescents: Helpful aspects of psychotherapy. Archives of Suicide Research, 7, 309–321.
Rosenberg, G. S., & Kim, M. P. (1975). The method of sorting as a data-gathering procedure in multivariate research. Multivariate Behavioural Research, 10, 489–502.
Rhodes, K. W., Orme, J. G., & Buehler, C. (2001). A comparison of family foster parents who quit, consider quitting, and plan to continue fostering. Social Service Review, 75, 84–115.
Schuck, K., & Liddle, B. J. (2004). The female manager's experience: A concept map and assessment tool. Consulting Psychology Journal: Practice and Research, 52, 75–87.
Soliday, E., McCluskey-Fawcett, K., & Meck, N. (1994). Foster mothers’ stress, coping and social support in parenting drug-exposed and other at-risk toddlers. Children's Health Care, 23, 15–32.
Stromberg, A. H. (1994). Foster parents of children with special medical care needs: Their characteristics and reasons for involvement. Community Alternatives: International Journal of Family Care, 6, 57–75.
Trochim, W. M. (1987). The concept system. Ithaca, NY: Trochim Publishing.
Trochim, W. M. (1989). An introduction to concept mapping for planning and evaluation. Evaluation and Program Planning, 12, 1–16.
Trochim, W., Cook, J., & Setze, R. (1994). Using concept mapping to develop a conceptual framework of staff's views of a supported employment program for individuals with severe mental illness. Journal of Consulting and Clinical Psychology, 62, 766–775.
Twigg, R. C. (1995). Coping with loss: How foster parents’ children cope with foster care. Community Alternatives: International Journal of Family Care, 7, 1–12.
Tyebjee, T. (2003). Attitude, interest, and motivation for adoption and foster care. Child Welfare, 82, 685–706.
Ward, J. H. (1963). Hierarchical grouping to optimize an objective function. Journal of the American Statistical Association, 58, 236–244.
Weller, S., & Romney, A. (1988). Systematic data collection. Newbury Park, CA: Sage.
Wilsnack, S. C., & Wilsnack, R. W. (1995). Drinking and problem drinking in US women: Patterns and recent trends. Recent Developments in Alcoholism, 12, 29–60.
Acknowledgments
The authors would like to acknowledge the financial support of this research through a grant from the Social Sciences and Humanities Research Council of Canada. The authors also wish to thank Bev Wiebe of Manitoba Foster Family Network and Brian Ridd of the Child Protection Branch, Manitoba Family Services and Housing for their support of this project. We would also like to thank the many foster parents who shared their time and expertise with us.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brown, J.D., Sigvaldason, N. & Bednar, L.M. Motives for Fostering Children with Alcohol-Related Disabilities. J Child Fam Stud 16, 197–208 (2007). https://doi.org/10.1007/s10826-006-9078-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-006-9078-1