
We compared family risk and protective factors among potential high school dropouts with and without suicide-risk behaviors (SRB) and examined the extent to which these factors predict categories of SRB. Subjects were randomly selected from among potential dropouts in 14 high schools. Based upon suicide-risk status, 1,083 potential high school dropouts were defined as belonging to one of four groups; 573 non-suicide risk, 242 low suicide risk, 137 moderate suicide risk and 131 high suicide risk. Results showed significant group differences in all youth self-reported family risk and protective factors. Increased levels of suicide risk were associated with perceived conflict with parents, unmet family goals, and family depression; decreased levels of risk were associated with perceived parental involvement and family support for school. Perceived conflict with parents, family depression, family support satisfaction, and availability of family support for school were the strongest predictors of adolescent SRB. Our findings suggest that suicide vulnerable youth differ from their non-suicidal peers along the dimensions of family risk and protective factors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Suicide is a leading cause of death among youth aged 15–19 years (Anderson, 2002). In a nationwide survey of high school students, Grunbaum et al. (2004) reported that 16.9% of students had seriously considered attempting suicide, 16.5% had made a specific plan to attempt suicide, and 8.5% had attempted suicide during the 12 months preceding the survey. These findings are consistent with those reported for high school samples (Allison, Pearce, Martin, Miller, & Long, 1995, 1992; Fergusson, Woodward, & Horwood, 2000; Wichstrøm, 2000).
The family is an important environmental context related to adolescent suicide and suicidal behaviors (Johnson et al., 2002; Resnick, et al., 1997; Wagner, 1997). Studies employing community samples have begun to explore factors contributing to suicide-risk behaviors among high school students (Fergusson et al., 2000; Johnson et al., 2002; Perkins & Hartless, 2002; Wichstrøm, 2000). These studies examined a variety of risk and protective factors which, increasingly, include family factors. However, our knowledge of critical family risk and protective factors remains somewhat limited.
Family psychopathology and exposure to family suicide have been identified in community samples as characteristics that increase a youth's vulnerability to suicide. Garber, Little, Hilsman, and Weaver (1998) found that adolescents whose mothers had ever had a mood disorder diagnosis evidenced increased risk for suicidal behaviors. Young people reporting suicidal behavior were more likely to come from families characterized by a constellation of family risk factors that include parental alcohol problems and illicit drug use (Fergusson et al., 2000). Potential high school dropouts with suicide ideation reported more problems related to parental alcohol and other drug (AOD) use when compared to similar youth without suicidal ideation (Thompson, Moody, & Eggert, 1994). Family suicidality is identified as a risk factor for adolescent suicidal behavior (Rubenstein et al., 1989) and a predictor of adolescent suicide risk (Resnick et al., 1997). However, in another sample of high school students, exposure to a family member's suicide-risk behavior was not significantly associated with either past or future attempts (Lewinsohn, Rhode, & Seeley, 1994).
The terms family stress, family strain and family dysfunction seem to be used similarly in studies of suicide-risk behaviors as a global indicator of family problem behavior. Stressful relationships, with parents differentiated attempters from both a depressed/ideator group and a comparison group (Wagner, Cole, & Schwartzman, 1995). Suicide ideators were distinguished from their high-risk peers as well as typical youth reporting higher levels on unmet family goals, conflict with parents, unreasonable parental expectations, and thoughts of running away from home (Thompson et al., 1994). In another study, family dysfunction was found to make an independent contribution to adolescent depression, which accounted for significant variance in suicide-risk behaviors (Martin, Rozanes, Pearce, & Allison, 1995). Garber et al. (1998) reported that family functioning mediated the relationship between maternal history of depression and adolescent suicide symptoms measured over time.
Family or parent-adolescent conflict is frequently associated with suicide-risk behaviors; it is either considered as part of a broad indicator such as family strain (Thompson et al., 1994) or family function (Garber et al., 1998), or examined as a separate construct (Lewinsohn et al., 1993). Suicidal behaviors were said to increase steadily as numbers of unresolved conflicts with parents increased (Toumbourou & Gregg, 2002). Allison et al. (1995) observed a higher rate of reported maternal and paternal criticism when suicidal youth were compared to their non-suicidal peers. Reports of suicidal behaviors increased when both parents and adolescents reported parent-adolescent relationship difficulties (Breton, Tousignant, Bergeron, & Berthiaume, 2002). Serious fights with family members were significantly associated with increased risk for attempts in late adolescence or early adulthood (Johnson et al., 2002). Yet it remains difficult to determine the contribution of parent-adolescent conflict to adolescent suicide risk behavior given the association of these conflicts with adolescent psychological problems (Gould, Greenberg, Velting, & Shaffer, 2003).
A variety of scales have been used to measure family cohesion, family connectedness and parental bonding. When parental care and protection were examined significant negative relationships were identified between low care/high protection (affectionless control) and suicide-risk behavior (Allison et al., 1995). An adolescent who described his/her family as highly cohesive was significantly less likely to be suicidal than an adolescent who saw his/her family as non-cohesive (Rubenstein et al., 1989). Conversely, the risk for suicide was increased among young people reporting problematic family circumstances during childhood that included less secure attachments to parents characterized by low levels of trust and communication (Fergusson et al., 2000). Similarly, low levels of parental care and over protection predicted both previous and subsequent attempts in a community sample of over 12,000 Norwegian students (Wichstrøm, 2000).
Perceived family support was predictive of recent suicide attempts independent of depression and attempters were differentiated from non-attempters on family support in a native Hawaiian sample (Yuen et al., 1996). Low perceived family support was associated with future attempts even after controlling for depression (Lewinsohn et al., 1993; 1994). Dubow et al. (1989) reported non-ideators were distinguishable from serious ideators on family support. When comparing youth hospitalized for suicide attempts and a community sample composed of both youth self-reporting attempts and “average” adolescents, hospitalized suicide attempters sought support from parents significantly less often than youth in the other groups; support from parents was found to protect from self-harm (Groholt et al., 2000).
The purpose of our study was to compare the levels of perceived family risk and protective factors among potential high school dropouts with and without suicide-risk behaviors (SRB); and to examine the extent to which these family factors predict categories of SRB.
METHODS
Study Design and Sample
We used a two-stage, cross sectional survey design. Both survey and interview data with youth were used to examine the relationships among perceived family risk and protective factors relative to suicide-risk behaviors in a population of potential high school dropouts. Participants included 1,083 potential high-school dropouts in grades 9 to 12, from 14 high schools; 11 in the Pacific Northwest and three in the Southwest.
Procedures
Case Identification and Invitation
A 2-step process was used to identify high-risk youth. First, a pool of potential high school dropouts was identified from each school district's database using indicators known to predict future dropout, including academic performance, attendance, and prior dropout status (Eggert, Thompson, & Herting, 1994b). From this population, youth were randomly sampled and personally invited to participate in the study. IRB approved, informed assent was obtained from students and informed consent was obtained from at least one parent/guardian. Students completed a comprehensive survey, the High School Questionnaire: Profile of Experiences (HSQ; Eggert, Herting, & Thompson, 1995), which tapped key study variables and included the Screen for Suicide Risk (SRS) (Thompson & Eggert, 1999). Indicators included suicidal behaviors (thoughts, threats, and attempts), depression, and drug involvement. Tests of the SRS case-finding model showed it was reliable, and had concurrent and predictive validity (Eggert et al., 1994b; Thompson & Eggert, 1999).
Comprehensive Assessment
Within a week of screening, all youth were assessed using a computer-assisted interview, the Measure of Adolescent Potential for Suicide (MAPS) (Eggert et al., 1994b). The content of the assessment taps three constructs of suicide potential: direct suicide risk factors (suicide thoughts, planning/preparation, prior attempts, threats and suicide exposure), related risk factors (stressors, depression, hopelessness and anxiety), and protective factors (coping and social support resources). For ethical reasons and as part of the MAPS assessment protocol, each youth, whether at suicide risk or not, was personally introduced to a school “case manager” following the interview. In addition, each youth's parent or guardian of choice was contacted by telephone and advised of the youth's suicide-risk status, strengths and support needs.
Subject Recruitment and Retention
The sample pool of potential high school dropouts represented 15–35% of each school's population. Of 1,494 youth randomly selected from the total pool, 83% or 1,240 accepted. Of those accepting, 91% or 1128 completed the HSQ and, of these, 96% or 1,083 completed the MAPS interview.
Measurement
The Suicide Risk Screen (SRS)
The SRS, which is embedded in the High School Questionnaire (HSQ), allows for incremental measurement of levels of suicide risk. These levels of risk are defined by three sets of empirically-based criteria, including indicators of: (1) suicidal behaviors (5 items tapping suicidal ideation, direct/indirect threats, prior attempts; α=.88), (2) depression (5-item scale from the CES-D; α=.87); and (3) drug involvement (a composite score of 10 items tapping AOD use, polydrug use, drug use control problems; α=.90). Preliminary construct, discriminant and predictive validity was established for the SRS with an independent sample; a confirmatory factor analysis resulted in a good-fitting three-dimensional SRS measurement model (χ2 (22)=26.85, AGFI=.96; n=515) (Eggert, Herting, & Nicholas, 1994a).
The suicide risk screen (SRS) criteria were used to categorize the level of suicide risk among potential high school dropouts. Subjects were divided into one non-suicide risk group and three suicide-risk groups (Low, Moderate and High) based on the SRS criteria (Thompson & Eggert, 1999). Youth at low risk evidenced any of the following behaviors: a) moderate suicide ideation (≥2), b) indirect/ direct threats of suicide (≥2), c) prior attempts (≥1), and/or d) moderate depression (2–3.4). Youth at moderate risk evidenced two or more of the behaviors listed above for low risk or may report drug involvement in addition to one or more of the low risk criteria. Youth at high risk evidenced any of the following: a) prior attempts (≥2), b) high suicide ideation (≥3), and/or high depression (≥3.4). These levels of risk should not be seen as differentiating clinical risk. That is, all youth, whether categorized as Low, Moderate or High, require clinical assessment to determine their current need for support and/or referral.
Family Risk and Protective Factors
Measures of family risk and protective factors were taken from youth reports on the HSQ and the MAPS. In combination, these instruments measure a broad range of perceptions regarding risk and protective factors, including measures of the family constructs of interest in this study. Table I provides a summary description of the key measures. Unless otherwise indicated, items were measured using a seven-point, Likert-type scale, ranging from 0 (never) to 6 (always/many times). The higher the scale value, the greater the level of the measured construct. Cronbach's alpha values reflecting internal consistency reliability for the current sample were moderate to high, ranging from .61 to .89.
Analysis
Data analyses were conducted using the Statistical Package for the Social Sciences for Windows, Release 8.0 (SPSS, 1998) and LIMDEP 7.0 (Greene, 1995). Graphic representations and appropriate descriptive statistics (including kurtosis, skewness) were used to examine distributional properties of variables. Due to non-normal distribution (extreme skews) three variables – family violence, family AOD use, and family suicide exposure – were re-coded as dichotomous variables (1=presence, 0=absence). Results were based on analysis of variance (ANOVA) for group comparisons, Scheffé post-hoc tests for multiple comparisons, Chi-square tests for nominal variables, and ordered logistic regression for tests of the extent to which family factors predict suicide risk among potential high school dropouts.
RESULTS
Sample and Subject Characteristics
Students participating in the study ranged in age from 14–19 years (M= 16 years); 53% were male. The ethnic composition was 59% minority (22% Hispanic/Latino, 18% African American, 12% Asian/Pacific Islander, 5% American Indian/Alaska Native, 2% mixed ethnic background). Only 39% of the subjects lived in a family unit where both natural parents were present; 34% lived in a single parent family, and 16% lived with one natural and one stepparent. The remainder of the youth (11%) lived with grandparents, other relatives, or alone. Baseline differences on gender, age, grade, ethnic background, and family composition among the four suicide-risk groups (high, moderate, low and non-risk) were examined. ANOVA and Chi-square tests detected no significant differences at baseline on age, grade, ethnic background, and family composition.
Gender was the only significant difference among the four groups (χ2 = 20.70; df = 3; N=1083; p < .00). Specifically, there were more females (N=275) than males (N=235) in the suicide-risk group. Conversely, there were more males (N=336) then females (N=237) in the group identified as non-suicide risk. Females at suicide-risk had significantly higher levels of suicidal behaviors, including prior suicide attempts, suicide ideation, and direct/indirect suicide threats, when compared to males at suicide-risk (M=0.97 vs. 0.72, t=2.67, p < .01). Females reported significantly more depression than males. This was true for all three suicide-risk groups (High to Low) (M=2.93 vs. 2.56, t=3.30, p < .01) as well as the non-suicide risk group (M=0.98 vs. 0.81, t=3.50, p < .01).
While there were no significant differences among the groups on drug involvement, males in the suicide risk group reported greater alcohol and poly drug use than females. In the non-suicide risk group there was no difference between males and females on either use or control problems.
Comparisons of Risk and Protective Factors across Suicide-Risk Groups
The mean score and standard deviation for all youth reported family factors among the four suicide-risk groups are presented in Table II. ANOVAs were used for testing gender (2) by group (4) differences. Results from ANOVAs revealed significant group differences in all family risk and protective factors. Scheffé post-hoc tests with multiple comparisons were used to test for differences between the four groups. Despite the gender differences observed relative to suicide-risk behaviors, only one gender difference was observed when within group differences were examined. Females reported greater suicide exposure F (1, 1073)=17.4 (p < .001).
Risk Factors by Suicide Risk Status
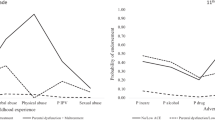
Perceived conflict with parents and unmet family goals revealed a significant step down pattern among groups (i.e., the higher the level of suicide risk demonstrated, the higher the level of conflict with parents and unmet family goals experienced). Perceptions of family depression also differentiated the suicide-risk groups from the non-risk group. The three suicide-risk groups were significantly higher on perceived family depression than the non-suicide risk group. Family violence, family AOD use, and number of family stressors were associated with the highest levels of suicide risk. The two groups at highest suicide risk experienced significantly higher levels of perceived family violence and AOD use compared to the group at lowest suicide risk and the non-risk group. Similarly, the two groups at highest suicide risk had a significantly higher number of stressors than the non-risk group. Finally, on suicide exposure, the group at highest suicide risk was significantly different from both the low and non-risk group.
Protective Factors by Suicide Risk Status
While the groups at moderate and low suicide risk reported no statistically significant differences in any of the family protective factors, an interesting pattern among the groups was observed. Perceived family support satisfaction and support availability for depression and suicidal thoughts differentiated all youth at suicide risk from their non-risk peers. Likewise, youth in the two groups at highest suicide risk were differentiated from the non-suicide risk group on perceived parental involvement and the amount of family support for school.
Family Factors Predicting Suicide Risk
Ordered logistic regression in LIMDEP was used to assess the relationship between perceived family risk and protective factors and suicide risk status. The analysis allows for the determination of the independent effects of the specific family factors of interest in the presence of the effects of other variables; included in the regression were controls for the effects of demographic variables (age, gender, ethnic background, and family composition). The analysis included initial multinomial logistic regression and cumulative logistic regressions to examine whether the parallel regression assumption of the ordered regression was reasonable, and whether any of the categories of suicide risk could be collapsed. The results clearly indicated the 4 categories of suicide risk could not be collapsed. The analysis of the parallel regression assumption indicated few substantial departures. The only substantial effects not evident in the ordered logistic regression was the significant effect of perceived family violence and unmet family goals, which both increased the odds of being in the medium category of suicide risk vs. no risk. In addition, the ordered logistic regression suggests a constant effect of total family support and gender which, in the multinominal logistic regression, the effects appear to be significant for only the highest level of suicide risk. Therefore, we elect to present the ordered regressions for the sake of simplicity.
The ordered logistic regression revealed that perceived conflict with parents, family depression, family AOD use, family support satisfaction, family support for school, and support availability for feelings of depression and suicidal thoughts were the significant family predictors of adolescent suicide-risk behaviors after controlling for age, gender, ethnicity, and family composition (see Table III). That is, the higher the level of perceived family conflict, family depression, and family AOD use, the greater the level of suicide-risk behavior. Correspondingly, the higher the perceived amount of support for school, support availability for feelings of depression and suicidal thoughts, and general support satisfaction, the lower the level of risk for suicide. Age and gender were also significantly related in the regression; risk increased with age and being female.
To test for interaction effects, we added all two-way interactions of gender with the eleven family variables, and compared the fit of this model to the model without these interactions. The results suggested there were no strong interactions present (χ2 diff=18, df=11, p=ns). Only the perception of family support satisfaction appeared to differ by gender (β=−0.23. p ≤ .059), having a slightly greater effect in reducing suicide risk among females.
DISCUSSION
Within a multi-ethnic, community sample of potential high school dropouts, 47% of the participating youth were identified as at risk for suicide. As is commonly observed (Garrison, Jackson, Addy, McKeown, & Waller, 1991; Wichstrøm & Rossow, 2002), more females than males reported higher levels of suicide-risk behaviors (e.g., prior attempts, suicide ideation) and depression. Despite gender differences in suicide-risk behaviors, when comparing across groups on self-reported family variables, the risk groups did not differ by gender; the exposure to an attempt or suicide by a family member was the only exception. Based on their own report, youth in the suicide risk groups were differentiated from their non-suicide risk peers on perceptions of conflict with parents, unmet family goals, family depression, support satisfaction, and support availability for feelings of depression and suicide ideation. Youth at higher risk of suicide (high and moderate groups) reported higher levels of perceived family violence, family alcohol and other drug (AOD) use, and number of family stressors. Perceived family conflict, family depression and family AOD use were predictive of suicide-risk status; higher levels of risk were associated with higher perceived levels of these three risk factors. Lower levels of suicide risk were predicted by higher levels of general satisfaction with support, higher levels of support for school, and support when feeling depressed and/or thinking about suicide.
Findings from our study confirm the significance of self-reported family characteristics relative to youth suicide-risk status reported in previous studies (Garber et al., 1998; Rubenstein et al., 1989). Perceived family depression, violence and AOD use differentiated youth at risk for suicide from their non-suicide risk peers in this sample of potential high school dropouts. Youth in the highest risk groups (high and moderate) reported experiencing significantly higher levels of family violence and AOD use. All three suicide-risk groups reported perceptions of higher levels of family depression than the non-risk group. Perceptions of family violence did not predict suicide-risk status; however, the higher the levels of perceived family AOD use and family depression, the higher the risk of suicide. These findings support the need for selective, preventive interventions for youth from households where they are exposed to family member depression and/or AOD use.
Family stress—variously defined as family dysfunction, family conflict and parent-adolescent conflict—has been associated either directly or indirectly with adolescent suicide-risk behavior. In this study, both perceptions of parent-adolescent conflict and unmet family goals differentiated among various levels of suicide risk. In addition, the number of family-related stressors a youth reported experiencing differentiated youth at risk for suicide from those youth in the non-risk group. Only youth perception of parent-adolescent conflict predicted suicide risk; higher perceived levels of parent-adolescent conflict predicted higher levels of suicide risk. Again, these findings were consistent with the literature on parent-adolescent conflict (Allison et al., 1995; Breton, et al., 2002; Kienhorst, de Wilde, Diekstra, & Wolters, 1995; Toumbourou & Grett, 2002). Beyond conflict, it is apparent that youth perceptions of family failures to meet traditional goals such as having fair rules, open communication, doing things together, and valuing the teen's capabilities are associated with increasing suicide risk. Additionally, teens reporting greater numbers of stressors, including perceived family conflict, problematic parental behaviors, family member illness, job losses, and deaths, comprise a group at greater suicide risk. Taken together, these findings speak to the need to involve parents in suicide prevention programming. Specifically, it seems critically important to focus on increasing communication competence among family members and to enhance the provision of support teens experience for increasing coping strategies and stress management techniques.
While support from parents is commonly associated with decreased risk for suicide (Dubow et al., 1989; Lewinsohn et al., 1994; Perkins & Hartless, 2002; Yuen et al., 1996), explicit aspects of this support have not been previously explored. In this sample of potential high school dropouts, teens perceptions of support for school, having someone available to help with feelings of depression and thoughts of suicide, as well as perceived parental involvement (i.e., knowing and approving of teen's friends, participating in school events) differentiated those youth at highest risk (high and moderate risk groups) from the non-risk group. Furthermore, youth reported feelings of specific support for school, availability of family members to talk about depression and suicidal ideation, and support satisfaction (i.e., satisfaction with time spent together, expression of affection, and availability of help) predicted lower suicide-risk status. These findings are consistent with studies that link adolescent psychological adjustment with family support (Eccles, Early, Frasier, Belansky, & McCarthy, 1997; McFarlane, Bellissimo, & Norman, 1995). Among potential high school dropouts, increasing connections to school through parental collaboration with available school-based support resources may be an important first step. Unique to this population is helping parents communicate in ways their teens find supportive around feelings of depression and thoughts about suicide. Parents frequently report being unaware of their teen's suicide risk (Breton et al., 2002; Garrison et al., 1991); thus, programs need to focus on identifying the warning signs, available sources of help, and provide opportunities to practice support strategies and asking about suicide.
Our study has several strengths and limitations that warrant discussion. Importantly, we employed a large, ethnically diverse sample selected at random from among potential high school dropouts. Suicide-risk status was identified using a comprehensive, reliable and valid measure. The sample, albeit large and representative of this pool of high-risk youth, does not allow generalization to all youth. Given that the sample included both those youth at risk for suicide and those not at risk, there is increased confidence in the generalizability of study findings to this high-risk population. In addition, the study included a comprehensive measure of multiple family constructs providing a detailed picture of the youths’ perception of family characteristics, family stress and family support resources. Data reported here were all self-report (questionnaire and interview) from participating teens, not actual observation of family behavior, and while this represents a limitation, individual participants remain the best source of information on internal states such as depression and suicide thoughts as well as perceptions of their personal experience. Neither the cross-sectional study design nor the statistical analysis employed provide sufficient evidence of causal relationships between predictors and adolescent suicidal behaviors; thus, these findings must be interpreted as evidence of associations present in the data and not explicitly as causal. Despite these limitations, the study results provide important insights into the role of family risk and protective factors relative to suicide risk among high-risk youth, laying the ground work for future research and suggesting directions for prevention programming.
We believe the results have implications for designing interventions to address suicide risk among high-risk adolescents. There are several implications that can be drawn from this study. First, replication of this study using a longitudinal design would allow for a more complete examination of the effects family characteristics, family stress and family support on adolescent suicide-risk behaviors. Additional replication studies with typical high school students and other high-risk groups can potentially enhance the generalizability of these findings. Second, research to test family-based prevention trials, using experimental designs, is in its infancy. While the current findings are to be interpreted with care, they have potential value for informing prevention efforts aimed at reducing adolescent suicide and suicidal behaviors. Findings herein indicated that youth perceptions of family characteristics, namely family depression and family AOD use, predict suicide-risk behaviors in this population. Furthermore, perceived conflict with parents predicts risk, while perceived support for school, support availability for feelings of depression and suicidal thoughts, and general support satisfaction predict lower levels of risk for suicide. These findings suggest the importance of designing and testing indicated prevention programs that target both youth and parents. While it has been demonstrated that potential high school dropouts who are at risk for suicide benefit from brief, school-based, indicated suicide preventive interventions we found no studies reporting on outcomes of programs for parents and youth at risk for suicidal behaviors (Randell, Eggert, & Pike, 2001; Thompson, Eggert, Randell, & Pike, 2001). These findings, coupled with those from previous studies (Garber et al., 1998; Martin et al., 1995; Wagner et al., 1995), have implications for designing and testing preventive interventions: (1) youth from households where family members experience depression, youth witness or experience violence, are exposed to family substance use, and/or report distress related to these family behaviors represent high-risk groups that would likely benefit from selective preventive efforts; (2) programs designed to decrease depression among family members and to decrease the occurrence of family violence and AOD use should also serve to decrease suicide-risk among these high-risk youth; and (3) indicated prevention programs that include skills training activities that assist both youth and parents to: (a) increase communication and problem-solving skills, (b) establish fair rules, (c) increase the positive time family members spend together, and (d) enhance the availability of support for school and accessing help for feelings of depression and suicide ideation, warrant efficacy testing.
References
Allison, S., Pearce, C., Martin, G., Miller, K., & Long, R. (1995). Parental influence, pessimism and adolescent suicidality. Archives of Suicide Research, 1, 229–242.
Anderson, R. N. (2002). Deaths: Leading causes for 2000. National Vital Statistics Reports, 50(16). Hyattsville, MD: National Center for Health Statistics.
Breton, J. J., Tousignant, M., Bergeron, L., & Berthiaume, C. (2002). Informant-specific correlates of suicidal behavior in a community survey of 12- to 14-year olds. Journal of the American Academy of Child & Adolescent Psychiatry, 41, 723–730.
Dubow, E. F., Kausch, D. F., Blum, M. C., Reed, J., & Bush, E. (1989). Correlates of suicidal ideation and attempts in a community sample of junior high and high school students. Journal of Clinical Child Psychology, 18, 158–66.
Eccles, J., Early, D., Fraiser, K., Belansky, E., & McCarthy, K. (1997). The relation of connection, regulation, and support for autonomy to adolescents’ functioning. Journal of Adolescent Research, 12, 263–286.
Eggert, L. L., Herting, J. R., & Nicholas, L. J. (1994a). Prevention research program: Reconnecting at-risk youth. Issues in Mental Health Nursing, 15, 107–135.
Eggert, L. L., Herting, J. R., & Thompson, E. A. (1995). High School Questionnaire: Profile of experiences, University of Washington, Seattle, WA.
Eggert, L. L., Thompson, E. A., & Herting, J. R. (1994b). A measure of adolescent potential for suicide (MAPS): Development and preliminary findings. Suicide & Life Threatening Behavior, 24, 359–381.
Fergusson, D. M., Woodward, L. J., & Horwood, L .J. (2000). Risk factors and life processes associated with the onset of suicidal behaviour during adolescence and early adulthood. Psychological Medicine, 30, 23–39.
Garber, J., Little, S., Hilsman, R., & Weaver, K. R. (1998). Family predictors of suicidal symptoms in young adolescents. Journal of Adolescence, 21, 445–457.
Garrison, C. Z., Jackson, K. L., Addy, C. L., McKeown, R. E., & Waller, J. L. (1991). Suicidal behaviors in young adolescents. American Journal of Epidemiology, 133, 1005–1014.
Gould, M. S., Greenberg, T., Velting, D. M., & Shaffer, D. (2003). Youth suicide risk and preventive interventions: A review of the past 10 years. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 386–405.
Greene, W. H. (1995). LIMDEP User's Manual (Version 7). Bellport, NY: Econometric Software.
Grohølt, B., Ekeberg, Ø., Wichstrøm, L., & Haldorsen, T. (2000). Young suicide attempters: A comparison between a clinical and an epidemiological sample. Journal of the American Academy of child and Adolescent Psychiatry, 39, 868–875.
Grunbaum, J. A., Kann, L., Kinchen, S., Ross, J., Hawkins, J., Lowry, R., Harris, W. A., McManus, T., Chyen, D., & Collins, J. (2004). Youth Risk Behavior Surveillance – United States, 2003 (Abridqed). Jaurnal of School Health, 74, 307--324.
Johnson, J. G., Cohen, P., Gould, M. S., Kasen, S., Brown, J., & Brook, J. S. (2002). Childhood adversities, interpersonal difficulties, and risk for suicide attempts during late adolescence and early adulthood. Archives of General Psychiatry, 59, 741–749.
Kienhorst, C. W. M., de Wilde, E. J., Diekstra, F. W., & Wolters, W. (1995). Adolescents’ image of their suicide attempt. Journal of the American Academy of Child and Adolescent Psychiatry, 34, 623–628.
Lewinsohn, P. M., Rohde, P., & Seeley, R. (1993). Psychosocial characteristics of adolescents with a history of suicide attempt. Journal of the American Academy of Child and Adolescent Psychiatry, 32, 60–68.
Lewinsohn, P. M., Rohde, P., & Seeley, R. (1994). Psychosocial risk factors for future adolescent suicide attempts. Journal of Consult & Clinical Psychology, 62, 297–305.
Martin, G., Rozanes, P., Pearce, C., & Allison, S. (1995). Adolescent suicide, depression and family dysfunction. Acta Psychiatrica Scandinavica, 92, 336–344.
McFarlane, A. H., Bellissimo, A., & Norman, G. R. (1995). The role of family and peers in social self-efficacy: Links to depression in adolescence. American Journal of Orthopsychiatry, 65, 402–410.
Perkins, D. F., & Hartless, G. (2002). An ecological risk-factor examination of suicide ideation and behavior of adolescents. Journal of Adolescent Research, 17, 3–26.
Randell, B. P., Eggert, L. L., & Pike, K. C. (2001). Immediate post intervention effects of two brief youth suicide prevention interventions. Suicide and Life-Threatening Behavior, 31, 41–61.
Resnick, M. D., Bearman, P. S., Blum, R. W., Bauman, K. E., Harris, K. M., Jones, J., et al. (1997). Protecting adolescents from harm: Findings from the national longitudinal study on adolescent health. Journal of the American Medical Association, 278, 823–865.
Rubenstein, J. L., Heeren, T., Housman, D., Rubin, C., & Stechler, G. (1989). Suicidal behavior in ``normal'' adolescents: Risk and protective factors. American Journal of Orthopsychiatry, 59, 59–71.
SPSS. (1998). SPSS for Windows Release 8.0. Chicago, IL: Author.
Thompson, E. A., & Eggert, L. L. (1999). Using the Suicide Risk Screen to identify suicidal adolescents among potential high school dropouts. Journal of the American Academy of Child & Adolescent Psychiatry, 38, 1506–1514.
Thompson, E. A., Eggert, L. L., & Herting, J. R. (2000). Mediating effects of an indicated prevention program for reducing youth depression and suicide risk behaviors. Suicide and Life-Threatening Behavior, 30, 252–271
Thompson, E. A., Eggert, L. L., Randell, B. P., & Pike, K. C. (2001). Evaluation of indicated suicide-risk prevention approaches for potential high school dropouts. American Journal of Public Health, 91, 742–752.
Thompson, E. A., Moody, K. A., & Eggert, L. L. (1994). Discriminating suicide ideation among high-risk youth. Journal of School Health, 64, 361–367.
Toumbourou, J. W., & Gregg, M. E. (2002). Impact of an empowerment-based parent education program on the reduction of youth suicide risk factors. Journal of Adolescent Health, 31, 277–285.
Wagner, B. M. (1997). Family risk factors for child and adolescent suicidal behavior. Psychological Bulletin, 121, 246–298.
Wagner, B. M., Cole, R. E., & Schwartzman, P. (1995). Psychosocial correlates of suicide attempts among junior and senior high school youth. Suicide and Life-Threatening Behavior ,25, 358– 372.
Wichstrøm, L. (2000). Predictors of adolescent suicide attempts: A nationally representative longitudinal study of Norwegian adolescents. Journal of the American Academy of Child & Adolescent Psychiatry, 39, 603–610.
Wichstrøm, L., & Rossow, I. (2002). Explaining the gender difference in self-reported suicide attempts: A nationally representative study of Norwegian adolescents. Suicide and Life-Threatening Behavior, 32, 101–116.
Yuen, N., Andrade, N., Nahulu, L., Makini, G., McDermott, J. F., Danko, G., et al. (1996). The rate and characteristics of suicide attempters in the native Hawaiian adolescent population. Suicide and Life-Threatening Behavior, 26, 27–36.
ACKNOWLEGMENTS
This research was supported by grants R01 NR 03548 and R01 NR 03550 from the National Institute on Nursing Research (L. L. Eggert, principal investigator). We are indebted to the high school personnel and the young people whose participation enhanced our understanding of factors contributing to and protecting against suicide risk behaviors and to the dedicated efforts of the clinical and research staff that comprise the Reconnecting Youth Prevention Research team.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Randell, B.P., Wang, WL., Herting, J.R. et al. Family Factors Predicting Categories of Suicide Risk. J Child Fam Stud 15, 247–262 (2006). https://doi.org/10.1007/s10826-006-9020-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-006-9020-6