
Abstract
Purpose
The purpose of this study was to identify trends in gonadotropin therapy in patients undergoing in vitro fertilization (IVF) treatment worldwide.
Methods
Retrospective evaluation utilizing the results of a Web-based survey, IVF-Worldwide (www.IVF-worldwide.com) was performed.
Results
Three hundred fourteen centers performing a total of 218,300 annual IVF cycles were evaluated. Respondents representing 62.2% of cycles (n = 135,800) did not believe there was a difference between urinary and recombinant gonadotropins in terms of efficacy and live birth rate. Of the respondents, 67.3% (n = 146,800) reported no difference between recombinant and urinary formulations in terms of short-term safety and risk of ovarian hyperstimulation syndrome. In terms of long-term safety using human urinary gonadotropins, 50.6% (n = 110,400) of respondents believe there are potential long-term risks including prion disease. For 95.3% of units (n = 208,000), the clinician was the decision maker determining which specific gonadotropins are used for IVF. Of the units, 62.6% (n = 136,700) identified efficacy as the most important factor in deciding which gonadotropin to prescribe. While most (67.3%, n = 146,800) were aware of new biosimilar recombinant FSH products entering the market, 92% (n = 201,000) reported they would like more information. A fraction of respondents (25.6%, n = 55,900) reported having experience with these new products, and of these, 80.3% (n = 46,200) reported that they were similar in efficacy as previously used gonadotropins in a similar patient group.
Conclusions
Respondents representing the majority of centers do not believe a difference exists between urinary and recombinant gonadotropins with respect to efficacy and live birth rates. While many are aware of new biosimilar recombinant FSH products entering the market, over 90% desire more information on these products.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Gonadotropin therapy is critical to ovulation induction protocols to stimulate the ovaries for in vitro fertilization (IVF). Medications in this class function similarly to two hormones produced by the pituitary gland: luteinizing hormone (LH) and follicle-stimulating hormone (FSH) [1, 2]. Research underlying the current gonadotropin preparations used for contemporary IVF has spanned for at least five decades [3]. Gonadotropin manufacturing has evolved from the extraction of purified gonadotropins from urine to the application of recombinant techniques to yield a variety of preparations for ovarian stimulation. Currently, multiple gonadotropin formulations are available worldwide and in use for IVF treatment [2].
Historically, gonadotropin preparations have been purified from animals, cadavers, and FSH developed in 1983 [4]. Eventually, DNA technology was used to develop recombinant FSH (rFSH) from Chinese hamster ovary cells [5, 6]. Newer-generation recombinant and pure synthetic molecules remain a focus of new research [2]. Data regarding long-term effects of these medications are limited, specifically those linking the risk of prion disease transmission to human urinary preparations [7]. The risk of ovarian hyperstimulation syndrome (OHSS) continues to be an area of interest [3]. Numerous studies have tried to establish whether there is any clinical difference in terms of efficacy or safety among these modalities [1, 8,9,10]. Ovarian stimulation typically involves administration of human FSH derived from either urinary sources or recombinant techniques and/or human menopausal gonadotropin (hMG), which is derived from postmenopausal urine and has both LH and FSH activities [3, 11].
Biosimilars are biological medicinal drugs produced by DNA technology, similar to an originator biological compound [12, 13]. Recently, the impending patent expiration of widely used recombinant FSH products incited pharmaceutical interest in FSH biosimilars. Two FSH biosimilars were recently approved for IVF marketing in Europe by the European Medicines Agency (EMA). While these agents are also available in other regions such as China, India, and Latin America, they are not yet available in the USA. Two newly marketed FSH biosimilars include the follitropin α biosimilar XM17 (Ovaleap, Teva Pharma B.V., Utrecht, The Netherlands) and another follitropin α biosimilar (Bemfola, Finox Biotech AG, Burgdorf, Switzerland) [5].
IVF-Worldwide (www.IVF-Worldwide.com) is a comprehensive IVF-focused website for physicians, embryologists, nurses, and social workers. It allows members to locate IVF centers anywhere in the world to communicate directly, facilitating the sharing of ideas and discussion of treatment and medication regimens. This non-commercial, non-profit website has an advisory panel of 52 leaders in the fertility field and routinely performs surveys focusing on various aspects of assisted reproductive technologies (ART).
The purpose of this Web-based survey was to identify trends in gonadotropin therapy performed worldwide and to correlate these results with the current evidence-based literature. Given the variety of medical options available, medication choices depend on the clinical context, cost, convenience, and provider preference. This information may prove useful to providers seeking guidance in using various gonadotropin preparations for optimizing fertility treatment protocols.
Materials and methods
A 19-item survey entitled “The use of gonadotropins and biosimilars in ART treated cycles” was compiled and posted on the IVF-Worldwide website from 9 March 9, 2015 to April 30, 2015. Please refer to the questions stems in Appendix Table 1. Survey questions focused on various aspects of preference of urinary versus recombinant gonadotropin formulations and attitudes and experiences regarding recombinant biosimilars. Additional questions involved GnRH agonist protocols and use of the GnRH agonist trigger. This study was determined to be exempted from the institutional review board approval by the Johns Hopkins University School of Medicine.
Quality assurance methods
Minimization of duplicate reports from a unit as well as possible false data was achieved via a computerized software program that assessed the consistency of four parameters from self-reported data of the unit surveyed with existing data of units registered on the IVF-Worldwide website. These parameters included the name of the unit, name of the unit director, country, and e-mail address. These checkpoints were in place to prevent duplicate responses from a center from more than one clinician and prevent more than one response from a given center. At least three of the parameters from the survey had to match archived data on the website in order for the reporting site’s data to be included as part of the study.
Statistical analysis
The analysis was based on the number of IVF cycles reported by the unit and not on the number of units in the study. Thus, the relative proportion of answers reflects the total proportion of IVF cycles represented rather than the proportion of individual respondents to the survey questions. The survey was structured as a sequence of multiple choice questions, in which respondents could select a single answer. For example, for a question with four possible answers (a, b, c, and d), results were calculated by using the following formulas as described in previously reported research from the IVF-Worldwide network [14]:
Results
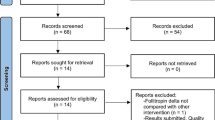
A total of 314 IVF centers from 73 countries responded to the survey and met the computerized system’s quality assurance standards. Overall, respondents reported on 218,300 IVF cycles performed annually. International representation of the cycles was diverse: 44.4% European (n = 97,000), 24.8% Asian (n = 54,100), 7.1% North American (n = 15,400), 10.9% South American (n = 23,900), 7.7% African (n = 16,700), and 5.1% from Australia and New Zealand (n = 11,200). The ten most represented countries included Spain (n = 23,700), India (n = 15,300), the USA (n = 15,000), the UK (n = 12,600), Turkey (n = 13,000), Australia (n = 10,900), Germany (n = 8500), Israel (n = 8200), Brazil (n = 8200), and Italy (n = 8100).
When asked whether urinary and recombinant gonadotropins differed in terms of efficacy and live birth rate, respondents representing the majority of cycles (62.2%, n = 135,800) did not believe a difference existed. Among remaining respondents, 26.7% (n = 58,300) believe that recombinant formulations are more efficacious, 7.7% (n = 16,700) felt urinary preparations were more efficacious, and 3.4% (n = 7500) did not know. Likewise, most felt recombinant and urinary formulations did not differ in terms of safety and risk of OHSS (67.3%, n = 146,800) while 21.3% (n = 46,500) believed recombinant formulations are safer, 9.2% (n = 20,000) felt urinary preparations were safer, and the remainder (2.3%, n = 5000) did not know. In terms of long-term safety issues associated with the use of human urinary gonadotropins, just over half of all respondents (50.6%, n = 110,400) believe there are potential long-term risks such as prion disease. Of the respondents, 38.8% (n = 84,700) reported they did not think there were long-term safety risks and 10.6% (n = 23,200) responded that they did not know.
For 95.3% of units (n = 208,000), the clinician was named as the most important decision maker in determining which gonadotropins are used for IVF. Only a few listed the hospital (2.9%, n = 6300) or other (1.8%, n = 4000) in making this decision. Efficacy was selected as the most important factor in deciding which gonadotropin to prescribe in 62.6% (n = 136,700) of units. Other factors selected less often included the following: price (13.6%, n = 29,600), range of doses available (8.8%, n = 19,300), safety (6.4%, n = 14,000), delivery system (5.1%, n = 11,100), and patient preference (3.5%, n = 7600). Half of respondents (50.3%, n = 109,800) reported that they prescribed mostly recombinant gonadotropins to IVF patients while 27.6% (n = 60,300) prescribe an equal proportion of the two types of product. Fewer (13.7%, n = 29,900) prescribe mostly urinary formulations, only urinary formulations (2.7%, n = 5900), or only recombinant formulations (5.5%, n = 11,900). When asked which drugs were less expensive in their respective countries, the majority of respondents (74.5%, n = 162,600) indicated that the urinary formulations were least expensive. A smaller percentage (21.4%, n = 46,800) reported that they cost the same, only 2.6% (n = 5700) reported recombinant formulations were less expensive, and 1.5% (n = 3200) reported they did not know the cost.
When asked if they were aware of new biosimilar rFSH products entering the market soon, 73.8% (n = 161,200) of respondents were aware and 26.2% (n = 57,100) were not. An overwhelming majority of respondents (92.1%, n = 201,000) reported they would like more information about these products and 7.9% (n = 17,300) denied wanting to learn more. A small fraction of respondents (25.6%, n = 55,900) reported having experience with these new products and the majority reported having no experience (74.4%, n = 162,400). Of those who reported experience with biosimilar rFSH products, 80.3% (n = 46,200) reported that they were similar in efficacy as previously used gonadotropins in a similar patient group. Much less, 11.0% (n = 6300) reported that they were less efficacious and 8.7% (n = 5000) reported that they were more efficacious.
A subset of seven questions addressed general IVF medication and protocol practices. Most respondents (67.8%, n = 147,900) reported using GnRH antagonist protocols, 25.2% (n = 55,000) use long GnRH agonist protocols, and 6.7% (n = 14,700) use short agonist protocols. There was a consensus among centers regarding how clinicians determined the starting dose for rFSH to initiate an IVF cycle, with 82.7% (n = 180,600) of respondents designating antral follicle count, AMH level, and past performance in IVF. Only 9.9.0% (n = 21,700) indicated that they used antral follicle count alone, 4.2% (n = 9100) used past performance, and 1.6% (n = 3400) used AMH level. Of units that use a long GnRH protocol, nearly half (48.8%, n = 106,400) use gonadotropin formulations with both FSH and LH activities while 26.4% (n = 57,700) use a recombinant FSH product only and the remainder (24.8%, n = 54,200) report they believe it does not matter. For those who use the long GnRH agonist protocol, over half report using a similar dose of medication compared with antagonist cycles (56.1%, n = 122,400), 28.6% (n = 62,500) report using a higher dose, 9.3% (n = 20,200) use a lower dose, and 6.1% (n = 13,200) report none of the above. Of the majority of respondents, 84.6% (n = 184,700) report using a GnRH agonist in selected patients to trigger final follicular maturation while 4.4% (n = 9700) use it in all patients and 10.8% (n = 23,600) only use a beta-HCG trigger. Of those that trigger with a GnRH agonist, 16.2% (n = 35,300) transfer fresh embryos while 46.4% (n = 101,300) freeze the embryos and 37.4% (n = 81,700) make the decision to transfer or freeze based on the individual patient. With respect to thawed-frozen embryo transfer in normal ovulatory women, 41.2% (n = 89,900) prepare the uterine lining with estrogen and progesterone prior to transfer while 30.6% (n = 66,700) perform the transfer in a natural cycle. Of the remaining respondents, 18.0% (n = 39,200) perform both protocols based on the patient, 3.2% (n = 7000) perform stimulated cycles, and 7.1% (n = 15,500) perform all of the above or none. For those respondents who perform thawed-frozen embryo transfer in a natural cycle, roughly one third (34.0%, n = 74,200) administer HCG to schedule the time of transfer, 24.8% (n = 54,100) spontaneous ovulation, 28.6% (n = 62,300) perform both, and 12.7% (n = 27,700) none of the above.
Discussion
To our knowledge, this is the only study to date addressing the practices among an international cohort of fertility centers regarding the use of urinary versus recombinant gonadotropin regimens in treating IVF patients as well as examining provider’s experiences with biosimilar products. Identifying advantages of one gonadotropin preparation over another is valuable in predicting ovarian response and in optimizing live birth rates. Our survey identified many common practices, as well as variations, in the approach to using gonadotropin preparations in patients undergoing IVF. It also identified an overwhelming need for clinicians worldwide to learn more about biosimilar preparations entering the market.
In comparing urinary and recombinant gonadotropin regimens, the majority of respondents noted no major difference in terms of safety or efficacy. This finding is consistent with the published research on the subject. A recent Cochrane review compared recombinant gonadotropins with urinary gonadotropins. In evaluating 28 trials involving 7339 patients, the authors found that utilization of recombinant FSH compared to other gonadotropin preparations did not result in a statistically significant difference in live birth rate (OR 0.97, 95% CI). Nor was there evidence of a difference in the OHSS rate among 32 trials involving 7740 patients (OR 1.18, 95% CI 0.86–1.61) [1]. While it is interesting to note that approximately half of respondents expressed concern over long-term safety risks from the use of urinary gonadotropins, that risk is not currently supported. Following the commercial introduction of recombinant FSH, concerns arose regarding risks from contamination of infectious agents potentially present in urinary preparations, which included prions. A position statement by the European Society of Human Reproduction and Embryology (ESHRE) notes that the incidence of prion-transmitted diseases, namely Cruetzfeldt-Jakob disease (CJD), is extremely rare and that urinary gonadotropins have been used by millions of women for over 50 years with no documented case of CJD through urine-derived gonadotropins [15].
While respondents were not asked about specific diagnoses such as polycystic ovary syndrome (PCOS), there may be scenarios when one preparation is more beneficial. One randomized trial compared purified urinary FSH with recombinant FSH for IVF/ICSI in patients with PCOS. Among the two groups, they found no significant difference between the total amount of FSH used, number of retrieved oocytes or embryos transferred, or ongoing pregnancy rate. However, the urinary FSH group had higher fertilization rates, higher-graded embryos, and more cryopreserved embryos. OHSS rates did not differ between the groups. The researchers hypothesized that the more glycosylated urinary FSH may benefit patients with PCOS [9].
It is notable that while most respondents were aware biosimilar gonadotropic products existed, over 90% wanted to learn more. This is not an unexpected finding as the real impact of FSH biosimilars on ART outcomes is not yet fully established. However, data from early clinical trials does appear to demonstrate similar efficacy in FSH biosimilars compared to their recombinant FSH counterparts. A multicenter, randomized, assessor-blind, study compared Ovaleap to Gonal-F in infertile women 18 to 37 years old undergoing ART. During a 5-day fixed-dose phase, women received 150 IU/day of Ovaleap or Gonal-F, followed by an up to 15-day phase during which doses could be adjusted every 3 to 5 days, up to a maximum of 450 IU/day. The mean ± SD number of oocytes retrieved was 12.2 ± 6.7 in the Ovaleap group and 12.1 ± 6.7 in the Gonal-F group. Regression analysis estimated a mean difference of 0.03 oocyte between the treatment groups (95% CI −0.76–0.82). The two medications showed favorable and comparable safety profiles with no unexpected safety findings [16].
Clinical trials also show positive outcomes for a second follitropin alpha biosimilar, Bemfola (Finox Biotech AG, Burgdorf, Switzerland). A randomized, multicenter study in women undergoing IVF showed Bemfola yielding similar efficacy and safety profiles to Gonal-F. Women aged 20–38 years of age were randomized 2:1 to receive a single, daily, subcutaneous 150 IU dose of either Bemfola or Gonal-F. Compared with Gonal-F, Bemfola treatment resulted in a statistically equivalent number of retrieved oocytes [17]. To date, there are no published reports comparing biosimilar FSH products to urinary gonadotropin products.
As expected, few respondents had experience with biosimilar FSH products and a large majority would like more information on these products. The EMA established the legal basis for evaluating and approving biosimilar products, developing guidelines for both biosimilars in general and specific categories. In the USA, biosimilars are not readily authorized and FSH biosimilars are currently not on the market. As a result, IVF providers in the USA will likely not be familiar with FSH biosimilars as providers in other parts of the world. In contrast, countries such China and India and several in Latin America allow biosimilars without stringent regulation. While the US biosimilar statute was enacted in 2010 and the Food and Drug Administration released its first guidance on biosimilars in 2012, to date, only one product has been approved in the USA as a biosimilar. The development of biosimilars could represent a reasonable alternative to currently available products, given their reduced production costs. As a result, both patients and providers need to be informed on the current technological advances and clinical utility of biosimilars. In 2006, the International Alliance of Patients’ Organizations (IAPO) published a briefing paper to educate the public on the introduction of biological and biosimilar medicines. Additional publications and position statements from major reproductive health organizations are needed to further educate both providers and patients.
Strengths of this study are the comprehensive nature of the survey, focusing on several aspects of antral follicle use in IVF cycles, ranging from clinical indications to treatment protocols to perceived impact on patient outcomes. An additional strength is the large number of IVF centers and cycles represented, as well as diversity in the geographic locations represented. Our study exhibits weakness as well in its potential for selection bias. Units that chose to participate in a worldwide survey may have practice techniques which differ from other centers worldwide that chose not to participate. Additionally, our study included a large cohort of centers worldwide but was not able to take into account local variables that may impact responses and ART outcomes. Likewise, we are unable to correlate responses to a center’s pregnancy rates and safety history. Our study did not explore other developments in gonadotropins including long-acting FSH analogues such as corifollitropin alfa and recombinant LH products [2].
In conclusion, the role of the IVF clinician is to provide treatment that is safe, patient-friendly, and cost-effective while at the same time offering good and high quality treatment. Our survey of IVF centers worldwide demonstrates that in comparing urinary and recombinant gonadotropin regimens, most fertility specialists worldwide do not recognize any major difference in terms of safety or efficacy, as past studies also demonstrated [1]. While biosimilar recombinant FSH products are available in many parts of the world, an overwhelming majority of IVF providers would like to learn more about these products. Education centered on the biosimilar mechanism of action, efficacy, dosing, and side effect profile is needed for IVF practitioners worldwide. Opportunities to disseminate information about biosimilars are available to both pharmaceutical companies and professional organizations.
References
Van Wely M, Kwan I, Burt AL, Thomas J, Vail A, Van der Veen F, Al-Inany HG. Recombinant versus urinary gonadotrophin for ovarian stimulation in assisted reproductive technology cycles. A cochrane review. Hum Reprod Update. 2012;18(2):111. doi:10.1093/humupd/dmr048.
Patil M. Gonadotrophins: the future. J Hum Reprod Sci. 2014;7(4):236–48. doi:10.4103/0974-1208.147490.
Practice T, Medicine R. Gonadotropin preparations: past, present, and future perspectives. Fertil Steril. 2008;90(5):S13–20. doi:10.1016/j.fertnstert.2008.08.031.
Bassett RM, Driebergen R. Continued improvements in the quality and consistency of follitropin alfa, recombinant human FSH. Reprod BioMed Online. 2005;10(2):169–77.
Santi D, Simoni M. Biosimilar recombinant follicle stimulating hormones in infertility treatment. Expert Opin Biol Ther. 2014;14(10):1399–409. doi:10.1517/14712598.2014.925872.
Keene JL, Matzuk MM, Otani T, Fauser BC, Galway AB, Hsueh AJ, Boime I. Expression of biologically active human follitropin in Chinese hamster ovary cells. J Biol Chem. 1989;264(9):4769–75.
Barrenetxea G. Iatrogenic prion diseases in humans: an update. Eur J Obstet Gynecol Reprod Biol. 2012;165(2):165–9. doi:10.1016/j.ejogrb.2012.08.014.
Revelli A, Pettinau G, Basso G, Carosso A, Ferrero A, Dallan C, Canosa S, Gennarelli G, Guidetti D, Filippini C, Benedetto C. Controlled ovarian stimulation with recombinant-FSH plus recombinant-LH vs. human menopausal gonadotropin based on the number of retrieved oocytes: results from a routine clinical practice in a real-life population. Reprod Biol Endocrinol: RB&E. 2015;13(1):77. doi:10.1186/s12958-015-0080-6.
Aboulghar M, Saber W, Amin Y, Aboulghar M, Mansour R, Serour G. Prospective, randomized study comparing highly purified urinary follicle-stimulating hormone (FSH) and recombinant FSH for in vitro fertilization/intracytoplasmic sperm injection in patients with polycystic ovary syndrome. Fertil Steril. 2010; doi:10.1016/j.fertnstert.2010.01.051.
Baker VL, Fujimoto VY, Kettel LM, Adamson GD, Hoehler F, Jones CE, Soules MR. Clinical efficacy of highly purified urinary FSH versus recombinant FSH in volunteers undergoing controlled ovarian stimulation for in vitro fertilization: a randomized, multicenter, investigator-blind trial. Fertil Steril. 2009;91(4):1005–11. doi:10.1016/j.fertnstert.2008.01.064.
Smitz J, Wolfenson C, Chappel S, Ruman J. Follicle-stimulating hormone: a review of form and function in the treatment of infertility. Reprod Sci. 2015; doi:10.1177/1933719115607992.
Roger SD, Mikhail A. Biosimilars: opportunity or cause for concern? J Pharm Pharm Sci. 2007;10(3):405–10.
Orvieto R, Seifer DB. Biosimilar FSH preparations—are they identical twins or just siblings? Reprod Biol Endocrinol. 2016;14(1):32. doi:10.1186/s12958-016-0167-8.
Vaisbuch E, Leong M, Shoham Z. Progesterone support in IVF: is evidence-based medicine translated to clinical practice? A worldwide Web-based survey. Reprod BioMed Online. 2012;25(2):139–45. doi:10.1016/j.rbmo.2012.04.005.
Vernazza PSE, De Sutter P. ESHRE position statement concerning prion detection in urinary gonadotropin formulations. [Website]. Available from: http://www.eshre.eu/Guidelines-and-Legal/ESHRE-Position-Papers.aspx. Accessed 15 May 2016.
Strowitzki T, Kuczynski W, Mueller A, Bias P. Randomized, active-controlled, comparative phase 3 efficacy and safety equivalence trial of Ovaleap(R) (recombinant human follicle-stimulating hormone) in infertile women using assisted reproduction technology (ART). Reprod Biol Endocrinol. 2016;14:1. doi:10.1186/s12958-015-0135-8.
Rettenbacher M, Andersen AN, Garcia-Velasco JA, Sator M, Barri P, Lindenberg S, Van Der Ven K, Khalaf Y, Bentin-Ley U, Obruca A, Tews G, Schenk M, Strowitzki T, Narvekar N, Sator K, Imthurn B. A multi-centre phase 3 study comparing efficacy and safety of Bemfola® versus Gonal-f® in women undergoing ovarian stimulation for IVF. Reprod BioMed Online. 2015;30(5):504–13. doi:10.1016/j.rbmo.2015.01.005.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Christianson, M.S., Shoham, G., Tobler, K.J. et al. Use of various gonadotropin and biosimilar formulations for in vitro fertilization cycles: results of a worldwide Web-based survey. J Assist Reprod Genet 34, 1059–1066 (2017). https://doi.org/10.1007/s10815-017-0952-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-017-0952-0