
Abstract
Purpose
This study aims to make an account of the children born following transplantation of frozen-thawed ovarian tissue worldwide with specific focus on the perinatal outcome of the children. Furthermore, perinatal outcome of seven deliveries (nine children) from Denmark is reported.
Methods
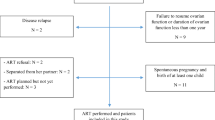
PubMed was searched for papers of deliveries resulting from ovarian tissue cryopreservation (OTC). Seven women underwent OTC prior to chemotherapy. Four of these women still had low ovarian function and had tried to conceive. They therefore had tissue autotransplanted to augment their fertility. The other three women had developed premature ovarian insufficiency (POI) after the end of treatment.
Results
Worldwide, approximately 95 children have been born or will be born in the near future from OTC, including these 9 new children. Information on the perinatal outcome was found on 40 children. The mean gestational age was 39 weeks and the mean birth weight was 3168 g of the singleton pregnancies, which is within internationally recognized normal standards. Furthermore, half the singletons resulted from natural conception and all twins resulted from in vitro fertilization treatment. All seven Danish women became pregnant within 1–3 years after transplantation. They gave birth to nine healthy children.
Conclusion
The data is reassuring and further suggests that cryopreservation of ovarian tissue is becoming an established fertility preservation method. The seven Danish women reported in this study were all in their early thirties when OTC was performed. Most other reported cases were in the women’s twenties. This suggests that the follicular pool in the thirties is large enough and sufficient to sustain fertility.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ovarian tissue cryopreservation (OTC) and transplantation is a relatively new procedure within the area of assisted reproduction technologies (ART). OTC differs from other ART procedures like freezing oocytes or embryos by cryopreserving intact tissue containing small non-growing follicles [1, 2]. Although the cryoprotectant media used to freeze ovarian tissue resemble those media used for oocytes and embryos, there are often subtle differences [3, 4]. Furthermore, extensive investigations on the effects of cryoprotectants on both human and animal ovarian tissue have not revealed any potential side effects. However, studies in women who had frozen-thawed ovarian tissue transplanted have revealed that follicles developing in the transplanted ovarian tissue are more often without oocytes and that the in vitro fertilization (IVF) pregnancy rate is relatively low compared to standard IVF patients [5, 6]. Additionally, the ovarian tissue is often transported close to zero degrees for up to 24 h, which of course is not the case of mature oocytes and embryos. It is still unknown if the handling of the ovarian tissue has an impact on the oocyte development and on the children conceived.
It is therefore important to realize that this is a new technique and that potential unforeseen side effects are revealed only when used in actual clinical practice. Although no reports have indicated that the children should differ from children conceived by healthy women and no malformations and pregnancy complications have been reported, the potential impact of the procedure on the offspring should be followed closely to secure the safety and health of the children.
Currently, the exact number of children born after OTC worldwide is unknown. Donnez and co-workers published 60 reported live births and 5 ongoing pregnancies worldwide [7]. Furthermore, exact information on the perinatal outcome is only included in a fraction of the published studies.
The aim of this study is to make an account of the number of children born following transplantation of frozen-thawed ovarian tissue with specific focus on the reported information on the pregnancy, the delivery, and the perinatal outcome of the children. The peer-reviewed papers were detected based on a PubMed search. A total of 40 children have been found including information on 9 children from our program from whom no previous information has been published.
Materials and methods
PubMed was searched for deliveries using the terms “cryopreservation of ovarian tissue,” “transplantation of ovarian tissue,” and “live births.” We also searched manually the reference lists of the identified articles for other references, which had not been identified in the PubMed search. We only included those peer-reviewed publications that included information on the pregnancies, deliveries, and children. All peer-reviewed publications, which only mentioned a live birth but no other information, were excluded.
We included in our analysis nine unpublished pregnancies of seven women from our personal experience from the Danish cohort. The patients included in this paper were from our cohort of 41 patients who have had OTC performed [8]. All seven patients had OTC prior to receiving chemotherapy, and all nine cases have not previously been reported. Four of these women had tried unsuccessfully to conceive, but could not succeed to facilitate a pregnancy because of a low ovarian function. They therefore requested a transplantation performed to augment their fertility and increase the available pool of follicles. The last three women had all developed POI after the end of chemotherapy.
The cryopreservation program
In Denmark, cryopreservation is offered to patients following counseling of a fertility specialist.
Oophorectomy was performed in either one of three hospitals in Denmark. The ovarian tissue was transported to one central laboratory where preparation and storage took place as previously reported [4, 9, 10]. The transplantation of ovarian tissue was performed in one of the two Danish Fertility Clinics, where this procedure was performed. A fertility specialist counseled the patients and the oncologist or hematologist who was responsible for the oncological treatment was contacted to make sure there were no objections to the transplantations and possible pregnancies. All seven women had the autotransplantation performed because of a pregnancy wish.
The risk of malignant cell contamination and recurrence of cancer after transplantation
For most of the cancer diseases, there were no specific cancer markers. Therefore, in most cases, it was not possible to test for potential malignant cell contamination in the ovarian tissue. Furthermore, if there were available markers and one or two ovarian pieces were tested for cell contamination, this does not necessarily apply to the rest of the remaining pieces of ovarian pieces, which were going to be transplanted. As previously published for this cohort of patients, the relapse rate (i.e., 7%) was identical to the background recurrence rate of the patients having had one ovary excised [8].
The Danish guidelines for retrieving ovarian tissue
A consultant who specialized in fertility preservation counseled each patient and made an individual evaluation. The consultant and the patient together decided on which fertility-preserving treatment was the most appropriate in the given situation. All procedures in connection with fertility preservation are free of cost and paid for by the public health care system.
The specialized counselors use the following clinical guidelines for counseling patients:
-
The estimated risk of developing POI has to be more than 50%.
-
There is no specific upper age limit for a patient who is offered OTC. It depends on the patient’s follicle reserve, which is estimated according to the AMH level and the biological age.
-
The estimated chance of a 5-year survival needs to be more than 50%.
-
The patient should not have disseminated diseases.
-
The patient should not have any contraindications against operation or anesthesia.
Results
In Table 1, the number of births and ongoing pregnancies after OTC has been published in peer-reviewed papers.
An overview of the perinatal outcome of children conceived in women who have had frozen-thawed ovarian tissue transplanted available from peer-reviewed papers, including nine new Danish cases, is given in Tables 2 [13, 18-42], 3, and 4.
Table 2 provides detailed information on the deliveries from published peer-reviewed journals including information on the woman (diagnosis, age at cryopreservation and signs of menopause before transplantation, time from transplantation to pregnancy), the origin of the pregnancy [naturally conceived (NC) or IVF, pregnancy complications, delivery mode], and the babies [gestational age (GA), birth weight (BW), and gender].
All 40 babies were reported healthy at birth.
Table 3 provides similar detailed information on the nine new Danish children (case no. 1–7).
Table 4 gives an overview of the origin of the pregnancy [NC/IVF/intrauterine insemination (IUI)], the births [CS/VD/not specified (NS)], and information on the babies (GA, BW, and gender).
Detailed perinatal outcome for nine babies in the Danish cohort, previously unpublished
Case no. 1/child no. 32 + 33
The patient was diagnosed with a molar pregnancy in 2011 at the age of 30. She had OTC performed prior to receiving treatment with BEP (bleomycine, etoposide, and cisplatin). After the end of the treatment, the patient tried to conceive naturally for 1 year without success. She was therefore referred to a Fertility Clinic where she received counseling regarding possible transplantation of her ovarian tissue. She had irregular menstrual cycles. The FSH level was 13.5 IU/L, LH was 8.2 IU/L, and she had an AMH level below 3 pmol/L. These values and her irregular menstruations indicated that there was still some remaining ovarian activity but too low to support fertility at least within the time frame attempted. She received transplantation in January 2013. Due to numerous adherences and difficulties in mobilizing the ovary, the 12 pieces of ovarian tissue (63% of one ovary) were transplanted to a peritoneal pocket. After 6 months, she had an unsuccessful IVF attempt. During the second IVF cycle, she received dehydroepiandrosterone (DHEA) support. Intra-cytoplasmic semen injection (ICSI) was performed resulting in transfer of one embryo, and the other embryo was frozen for later use. She became pregnant, but started having problems with cervical insufficiency from GA 22+. She was treated with an Arabin cerclage pessary, Tractocile, and bed rest. In June 2014, she gave birth by caesarean section to a healthy baby girl in week 37 + 1 weighing 3000 g. In August 2015, she had an embryo thawed and transferred from the IVF treatment. She conceived again and had an uneventful pregnancy and gave birth again by a caesarean section to a second healthy baby girl weighing 4230 g in week 39 + 0.
Case no. 2/child no. 34
The patient was diagnosed with an estrogen-receptor-positive breast cancer in 2008 at the age of 33 for which she received chemotherapy (three series of cyclophosphamide and epirubicin and three series of Taxotere), but no localized radiotherapy. OTC was performed prior to start of treatment. Subsequently, she received tamoxifen treatment for 3 years. On the request of the patient, tamoxifen treatment was discontinued 2 years prior to the recommended time because of a pregnancy wish. She was not without ovarian activity, her FSH level was 5.3 IU/L on cycle day 3, but her AMH level was below 3 pmol/L. On ultrasound, she had a normal-looking remaining ovary with a total of five antral follicles. During the subsequent 6 months, she failed to obtain a spontaneous pregnancy and it was decided to offer her transplantation of ovarian tissue to increase her chances of pregnancy. In August 2012 (FSH 14 IU/L; LH 15 IU/L), ten pieces of ovarian tissue (36% of one ovary) were grafted to the remaining ovary. Seventeen weeks later at follow-up, her AMH had risen to 3.6 pmol/L and her FSH had declined to 8.3 IU/L. She still reported regular menstrual cycles. As the patient and her partner had emigrated to another country, she was seen only when she was in Denmark on holiday. In January 2013, she underwent one cycle of intrauterine insemination with husband’s semen without getting pregnant. From April 2013 to June 2013, she underwent two cycles of IVF, each time with the aspiration of two oocytes but no fertilization. In October 2013, she became spontaneously pregnant and after an uneventful pregnancy she delivered a healthy baby boy vaginally weighing 3632 g at term.
Case no. 3/child no. 35
The woman was 31 years old when she in 2009 was diagnosed with aplastic anemia during her first pregnancy. It was decided to perform a caesarean section at GA 33+ in order to start immunosuppressive treatment and anti-thymocyte globulin (ATG). She responded partially to the treatment and received another immunosuppressive regime with ATG. Once again, she only responded partially to the treatment. Due to the poor response to treatment and the severity of her disease, she was recommended a stem cell transplantation (SCT) and conditioning with chemotherapy and TBI prior to SCT. She therefore has one ovary removed for cryopreservation prior to treatment. She received conditioning with cyclophosphamide and 4 Gy total body irradiation (TBI) before an allogeneic SCT.
After the SCT, the patient was taking oral contraceptive (OC) by the request of the hematologist in order to avoid menstruations during the rest of her treatment.
In the beginning of 2012, she terminated OC in order to become pregnant. For 11 months, the patient was without menstrual cycles. Her levels of gonadotropins (FSH 88.6 IU/L and LH 45.1 IU/L) were compatible with menopause. An ultrasound of her remaining ovary showed a small right atrophic ovary that measured 22 × 6 mm. She was offered to have a transplantation of ovarian tissue, and in March 2013, eight pieces of ovarian tissue (42% of one ovary) were autotransplanted. Six of the pieces were grafted to the remaining ovary and the last two pieces to a peritoneal pocket in the right broad ligament. Her first menstruation after the transplantation was in the beginning of August 2013. On ultrasound, she had three antral follicles. She tried to conceive naturally for 3–4 months without succeeding. She underwent two antagonist protocols of IVF treatment, but with no fertilization.
In August 2014, she became spontaneously pregnant. During the pregnancy, she developed preeclampsia and labor was therefore induced. She delivered a healthy baby boy vaginally at GA 37 + 5 weighing 3195 g.
Case no. 4/child no. 36
The patient was diagnosed with breast cancer in 2011 at the age of 34. She received adjuvant chemotherapy (six series of cyclophosphamide and epirubicin and three series of docetaxel) and localized radiotherapy. After the end of treatment, she was without ovarian activity. She was amenorrhoic and had menopausal symptoms. In November 2013 (FSH 113 IU/L; LH 66 IU/L; AMH <3 pmol/L), ten pieces of ovarian tissue (37% of one ovary) were transplanted. Two larger pieces (5 × 15 mm) and four smaller pieces (5 × 5 mm) were grafted to the remaining ovary and four pieces to a peritoneal pocket in the broad ligament. Twenty-three weeks later, at follow-up, her AMH was still <3 pmol/L, but her FSH and LH had dropped to 5.7 and 4.5, respectively. In August 2014, she became spontaneously pregnant, and after an uneventful pregnancy, she delivered a healthy baby boy by caesarean section weighing 3300 g at GA 40 + 3 weeks.
Case no. 5/child no. 37 + 38
In 2003, at the age of 23, the patient had acute abdominal pain, and at ultrasound examination, the diagnosis was believed to be a benign ruptured ovarian cyst of the left ovary. During the operation, it was suspected that it could be an ovarian tumor, so the patient had a unilateral salpingo-oophorectomy and omentectomy performed. Tissue was sent to pathology. The result from the pathology report was ovarian cancer (an ovarian mucinous cysteadenocarcinoma) stage 1C, but only in the ruptured ovary. She therefore had a second operation where the right ovary also was removed and OTC was performed on this ovary. Thereafter, she was treated with four series of chemotherapy (Taxol and carboplatin) and ended treatment during 2004. At this point, she was menopausal. She was amenorrhoic and had menopausal symptoms. After 5 years with no sign of a relapse, she wished to become pregnant. In May 2012, nine pieces of ovarian tissue (75% of one ovary) were transplanted. The pieces were grafted just above the sacrouterine ligament (four pieces on the left side and five on the right side). In the middle of August 2012 (14 weeks after transplantation), she regained menstrual cycles, and at this time she almost had no remaining menopausal symptoms. Her FSH was 19.4 IU/L and LH was 6.6 IU/L. She started IVF treatment in September 2012. She was treated with short protocol and 225 IE Menopur. She underwent seven IVF cycles in the antagonist protocol followed by ICSI. She became pregnant after the second cycle, but had a miscarriage in week 8. She was then treated with a long GnRH agonist protocol and ICSI and succeeded in becoming pregnant (September 2014) carrying di-chorionic, di-amniotic twins.
At the end of the pregnancy, she developed preeclampsia and had labor induction in May 2015 at GA 38 + 1. She gave birth vaginally to two healthy boys, weighing 2700 and 2600 g, respectively. After labor, the preeclampsia continued and she was treated with magnesium sulfate regimen.
In August 2015, due to her former ovarian cancer diagnosis, she had the grafted ovarian tissue removed again.
Case no. 6/child no. 39
This patient was 36 years old when in 2011 she was diagnosed with an estrogen-receptor-positive breast cancer. She was mastectomized and received chemotherapy (three series of cyclophosphamide and epirubicin and 3 series of docetaxel), localized radiotherapy, and subsequent tamoxifen treatment for 5 years. She tested positive for the BRCA-2 gene mutation.
Prior to antineoplastic treatment in October 2011, one ovary was cryopreserved. Due to a pregnancy wish, she stopped tamoxifen treatment to become pregnant. She still had some ovarian activity but had longer menstrual cycles (about 5 weeks) than before treatment; her FSH level was 14.6 IU/L and her AMH level was below 3 pmol/L. An ultrasonography showed a normal remaining ovary with one antral follicle. She was offered to have a transplantation of ovarian tissue, but only to the remaining ovary due to the fact that she was BRCA-2 positive, so that after a successful pregnancy the ovary could be removed. In April 2014 (FSH 4 IU/L; LH 3.4 IU/L), eight pieces of ovarian tissue (36% of one ovary) were grafted to the remaining ovary. At follow-up 15 weeks after transplantation, her FSH level was 2.7, but her cycles continued to be short and irregular. On ultrasonography, two corporae luteae, three antral follicles, and a small gestational sac in the top of the uterus were visualized. A positive hCG was measured, but a week later a miscarriage occurred. She became spontaneously pregnant once again the following month and had an uneventful pregnancy. She delivered a healthy baby girl vaginally at GA 41 + 2 weighing 3794 g.
Case no. 7/child no. 40
This patient was 33 years old when she was diagnosed with Non-Hodgkin lymphoma (a diffuse large B-cell lymphoma of the mediastinum) in 2010. After one ovary was removed for cryopreservation, she initiated chemotherapy receiving six series of R-CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) and 40 Gy radiation to the mediastinum.
After the end of treatment, regular menstruation cycles reappeared. Approximately 2 years after the end of treatment, the patient wished to become pregnant. She did not at this time have a partner and therefore began treatment at a Fertility Clinic. In total, she went through six IUI treatments with donor sperm. She became pregnant, but experienced a miscarriage during the first trimester. She was offered a transplantation of ovarian tissue to boost her fertility. Just prior to the transplantation, the hormone levels were measured (FSH 2.4 IU/L and LH 6.6 IU/L). She had a low ovarian reserve with an AMH level below 3 pmol/L. At the time the transplantation was performed, the patient was nearly 37 years old. Eleven pieces of ovarian tissue (50% of one ovary) were transplanted: eight pieces were transplanted to the remaining ovary and 3 pieces just below the ovary in a peritoneal pocket.
The patient went through four further IUI attempts, but without conceiving. In total, the patient underwent ten IUI treatments with donor sperm. The patient then underwent an IVF treatment approximately 1 year after the transplantation. At this time, her FSH level was rising and was now 11.2 IU/L. On her second IVF cycle with donor semen, she succeeded in becoming pregnant. She had an uneventful pregnancy and delivered a healthy baby girl vaginally at GA 39 + 0 weighing 2916 g.
Discussion
In this study, we provide an account of the current number of children conceived following transplantation of frozen-thawed ovarian tissue and focus especially on the perinatal outcome of the children born. The many centers now experiencing success with this treatment, the more than 90 children conceived worldwide, and the reassuring perinatal outcome of the 40 children in whom information is available advance fertility preservation by freezing ovarian tissue as a valid method that is now expanding beyond the experimental stage.
In this study, we further report nine new Danish healthy children conceived after transplantation of cryopreserved ovarian tissue to seven women. Five women had one singleton each, one woman gave birth to two singletons, and one woman gave birth to twins.
In Denmark, a total of 15 healthy children have now been born after transplantation of frozen-thawed ovarian tissue to 41 women [8, 22–25, this study].
In Denmark, the tissue is mainly grafted to the remaining ovary. If the woman does not have a remaining ovary or the remaining ovary is too small to contain all the retransplanted tissue, the graft is positioned in a peritoneal pocket, which can be in the broad ligament close to salpinx. Ideally, she will have a chance of conceiving naturally. Alternatively, the tissue is placed in the anterior abdominal wall, which is easily accessible for egg retrieval in connection with IVF treatment.
Seven children were NC and eight (including the twins) with the help of IVF treatment. All the women who obtained a NC pregnancy had grafts transplanted to the remaining ovary. One woman also had pieces transplanted to a peritoneal pocket in the anterior abdominal wall [23] and two women also had pieces transplanted to one of the broad ligaments (case 3 and 4 in this study). Out of the five women who received IVF treatment, two women had grafts transplanted only to the remaining ovary (three children were conceived, child no. 5–7 in Table 2), one woman had pieces transplanted to the remaining ovary and in a peritoneal pocket just below the ovary (case 7 in this study, who had one child), and two women only in a peritoneal pocket (case 1 and 5, both had two children each) [22, 23, this study].
The seven Danish women presented here all gave birth within 1–3 years after transplantation and had a mean age of 32 years at time of OTC (range 23.5–33.7 years). Most of the women reported so far worldwide who have given birth were in their twenties when OTC was performed, except for two women (Table 2). Six out of the seven women in this study were in their early thirties at the time of OTC. This suggests that even women in their early thirties have a sufficient pool of follicles to be able to regain fertility after OTC and grafting. In several countries that offer OTC to patients, one of the inclusion criteria is that the women should be no more than 30 years old. In Denmark, there is no exact maximum age rather than an individual evaluation of the patient’s reproductive age, which can differ from the patient’s chronological age, although often OTC is not offered to women above 35 years of age due to a diminished ovarian reserve. The outcome from our nine new cases supports that at least women up to the age of 35 should be offered OTC and in selected cases with a good ovarian reserve maybe even older.
Four of the women were not without endogenous ovarian function at the time of transplantation. However, they had tried to conceive without success for a considerable period of time and returned to have tissue transplanted to augment the ovarian pool and their fertility potential. This obviously prevents exact knowledge on whether the oocyte that resulted in the pregnancy originated in the transplanted tissue or not, and this is a limitation which we want to acknowledge.
In the 32 women who have given birth to 40 children worldwide (Tables 2 and 3), very few experienced pregnancy complications. Only 4 of 29 singleton pregnancies developed complications, which potentially would affect the pregnancy. Two women suffered from cervical insufficiency, where one of the two also developed preeclampsia, a third woman developed preeclampsia, and the forth woman developed HELLP syndrome. HELLP syndrome is a life-threatening pregnancy complication and usually considered to be a variant of preeclampsia where the women late in pregnancy or after delivery develop hemolysis (H), elevated liver enzymes (EL), and a low platelet count (LP). Even though there have only been these few reported pregnancy complications, many of the deliveries were by caesarean section (CS). In total, 19 children were delivered by CS including two sets of twins, but in seven cases, the delivery mode is not specified so the number could be even higher than 19 (Tables 2, 3, and 4). This could reflect anxiety from the part of the obstetrician considering these pregnancies to be very precious.
The singletons had a mean GA of 39 weeks and a mean BW of 3168 g, which is within the range of internationally accepted normal BW.
It is noticeable that half of the 40 children on whom perinatal information is available have been conceived naturally and enforce the remaining in situ ovary as a suitable place to graft the tissue. These results further highlight the difference between OTC and conventional ART. It is obviously an advantage for the woman to support NC both in terms of convenience and from an economical perspective. In Denmark, most women are allowed a 1-year period after transplantation to achieve a NC (half a year for the tissue to commence functioning and half a year to conceive) before IVF or other ART techniques are considered.
When the time to pregnancy (TTP) is evaluated, it is found that 18 of the women, who were included in this study, became pregnant within the first 12 months, 9 women became pregnant within 13–24 months, and 7 became pregnant more than 25 months post-transplantation (Tables 2 and 3).
In this study, we have only included the deliveries from peer-reviewed publications, which had information on the women, the pregnancies, and the deliveries. Worldwide, there are now more than 90 reported cases (Table 1), but only a fraction of them included detailed information of the perinatal outcome of the children born.
In the light of the many published long-term follow-up studies on the perinatal outcome of children resulting from IVF treatment, similar data for children conceived following transplantation of frozen-thawed ovarian tissue should also be collected. OTC is a new method, and to gain general acceptance of this procedure as part of modern treatment in young female cancer patients and obtain acceptance of this as an established procedure in general, it is important to collect information on the mothers, the pregnancies, and the children.
Most of the pregnancies have been conceived within the first 3 years after autotransplantation, but Macklon and co-workers reported two new cases where the conception occurred 5 and 6 years after autotransplantation [23], also sustaining long-term fertility.
It is difficult to obtain a complete picture of this procedure’s success rate due to the absence of reports of non-pregnancies in the peer-reviewed papers [43]. The Danish experience is that the success rate of having a positive pregnancy test among the Danish women, who had a pregnancy wish, was 63%. Furthermore, 31% of the women with a pregnancy wish succeed in conceiving at least one child and 50% of the pregnancies were naturally conceived [8].
To conclude, so far data on children born as a result of OTC and transplantation are reassuring. The pregnancies have been uncomplicated in the majority of the cases, the pregnancies are carried to term, and the children have a normal birth weight and seem to be healthy. Long-term follow-up, as has been done on ART children, is still too early for children conceived after OTC and the numbers are still very low, but it is important to have access to the information in the years to come.
References
Anderson RA, McLaughlin M, Wallace WHB, Albertini DF, Telfer EE. The immature human ovary shows loss of abnormal follicles and increasing follicle developmental competence through childhood and adolescence. Hum Reprod. 2014;29:97–106.
Kerr JB, Myers M, Anderson RA. The dynamics of the primordial follicle reserve. Reproduction. 2013;146:R205–15.
Kuwayama M. Highly efficient vitrification for cryopreservation of human oocytes and embryos: the Cryotop method. Theriogenology. 2007;67:73–80.
Rosendahl M, Schmidt KT, Ernst E, Rasmussen PE, Loft A, Byskov AG, et al. Cryopreservation of ovarian tissue for a decade in Denmark: a view of the technique. Reprod BioMed Online. 2011;22:162–71.
Dolmans M-M, Donnez J, Camboni A, Demylle D, Amorim C, Van Langendonckt A, et al. IVF outcome in patients with orthotopically transplanted ovarian tissue. Hum Reprod. 2009;24:2778–87.
Greve T, Schmidt KT, Kristensen SG, Ernst E, Andersen CY. Evaluation of the ovarian reserve in women transplanted with frozen and thawed ovarian cortical tissue. Fertil Steril. 2012;97:1394–8. e1.
Donnez J, Dolmans M-M. Ovarian cortex transplantation: 60 reported live births brings the success and worldwide expansion of the technique towards routine clinical practice. J Assist Reprod Genet. 2015;32:1167–70.
Jensen AK, Kristensen SG, Macklon KT, Jeppesen JV, Fedder J, Ernst E, et al. Outcomes of transplantations of cryopreserved ovarian tissue to 41 women in Denmark. Hum Reprod. 2015;30:2838–45.
Schmidt KLT, Ernst E, Byskov AG, Nyboe Andersen A, Yding Andersen C. Survival of primordial follicles following prolonged transportation of ovarian tissue prior to cryopreservation. Hum Reprod. 2003;18:2654–9.
Rosendahl M, Andersen CY, Ernst E, Westergaard LG, Rasmussen PE, Loft A, et al. Ovarian function after removal of an entire ovary for cryopreservation of pieces of cortex prior to gonadotoxic treatment: a follow-up study. Hum Reprod. 2008;23:2475–83.
Dittrich R, Hackl J, Lotz L, Hoffmann I, Beckmann MW. Pregnancies and live births after 20 transplantations of cryopreserved ovarian tissue in a single center. Fertil Steril. 2015;103:462–8.
Silber S, Pineda J, Lenahan K, DeRosa M, Melnick J. Fresh and cryopreserved ovary transplantation and resting follicle recruitment. Reprod BioMed Online. 2015;30:643–50.
Oktay K, Bedoschi G, Pacheco F, Turan V, Emirdar V. First pregnancies, live birth, and in vitro fertilization outcomes after transplantation of frozen-banked ovarian tissue with a human extracellular matrix scaffold using robot-assisted minimally invasive surgery. Am J Obstet Gynecol. 2016;214:94. e1–e9.
Meirow D, Ra’anani H, Shapira M, Brenghausen M, Derech Chaim S, Aviel-Ronen S, et al. Transplantations of frozen thawed ovarian tissue demonstrate high reproductive performance and the need to revise restrictive criteria. Fertil Steril. 2016;106(2):467–74.
Rodriguez-Wallberg KA, Tanbo T, Tinkanen H, Thurin-Kjellberg A, Nedstrand E, Kitlinski M, et al. Ovarian tissue cryopreservation and transplantation among alternatives for fertility preservation in the Nordic Countries—compilation of 20 years of multicenter experience. Acta Obstet Gynecol Scand. 2016;95(9):1015–26.
Van der Ven H, Liebenthron J, Beckmann M, Toth B, Korell M, Krüssel J, et al. Ninety-five orthotopic transplantations in 74 women of ovarian tissue after cytotoxic treatment in a fertility preservation network: tissue activity, pregnancy and delivery rates. Hum Reprod. 2016;31(9):2031–41.
Dunlop CE, Brady BM, McLaughlin M, Telfer EE, White J, Cowie F, et al. Re-implantation of cryopreserved ovarian cortex resulting in restoration of ovarian function, natural conception and successful pregnancy after haematopoietic stem cell transplantation for Wilms tumour. J. Assist. Reprod. Genet. 2016.
Donnez J, Dolmans MM, Demylle D, Jadoul P, Pirard C, Squifflet J, et al. Livebirth after orthotopic transplantation of cryopreserved ovarian tissue. Lancet. 2004;364:1405–10.
Meirow D, Levron J, Eldar-Geva T, Hardan I, Fridman E, Zalel Y, et al. Pregnancy after transplantation of cryopreserved ovarian tissue in a patient with ovarian failure after chemotherapy. N Engl J Med. 2005;353:318–21.
Demeestere I, Simon P, Emiliani S, Delbaere A, Englert Y. Fertility preservation: successful transplantation of cryopreserved ovarian tissue in a young patient previously treated for Hodgkin’s disease. Oncologist. 2007;12:1437–42.
Demeestere I, Simon P, Moffa F, Delbaere A, Englert Y. Birth of a second healthy girl more than 3 years after cryopreserved ovarian graft. Hum Reprod. 2010;25:1590–1.
Andersen CY, Rosendahl M, Byskov AG, Loft A, Ottosen C, Dueholm M, et al. Two successful pregnancies following autotransplantation of frozen/thawed ovarian tissue. Hum Reprod. 2008;23:2266–72.
Macklon KT, Jensen AK, Loft A, Ernst E, Andersen CY. Treatment history and outcome of 24 deliveries worldwide after autotransplantation of cryopreserved ovarian tissue, including two new Danish deliveries years after autotransplantation. J Assist Reprod Genet. 2014;31:1557–64.
Ernst E, Bergholdt S, Jorgensen JS, Andersen CY. The first woman to give birth to two children following transplantation of frozen/thawed ovarian tissue. Hum Reprod. 2010;25:1280–1.
Andersen CY, Silber SJ, Bergholdt SH, Jorgensen JS, Ernst E. Long-term duration of function of ovarian tissue transplants: case reports. Reprod BioMed Online. 2012;25:128–32.
Roux C, Amiot C, Agnani G, Aubard Y, Rohrlich PS, Piver P. Live birth after ovarian tissue autograft in a patient with sickle cell disease treated by allogeneic bone marrow transplantation. Fertil Steril. 2010;93:2413. e15–e19.
Donnez J, Silber S, Andersen CY, Demeestere I, Piver P, Meirow D, et al. Children born after autotransplantation of cryopreserved ovarian tissue. A review of 13 live births. Ann Med. 2011;43:437–50.
Sanchez-Serrano M, Crespo J, Mirabet V, Cobo AC, Escriba MJ, Simon C, et al. Twins born after transplantation of ovarian cortical tissue and oocyte vitrification. Fertil Steril. 2010;93:268. e11–e13.
Donnez J, Squifflet J, Jadoul P, Demylle D, Cheron AC, Van Langendonckt A, et al. Pregnancy and live birth after autotransplantation of frozen-thawed ovarian tissue in a patient with metastatic disease undergoing chemotherapy and hematopoietic stem cell transplantation. Fertil Steril. 2011;95:1787. e1–e4.
Revel A, Laufer N, Ben MA, Lebovich M, Mitrani E. Micro-organ ovarian transplantation enables pregnancy: a case report. Hum Reprod. 2011;26:1097–103.
Donnez J, Jadoul P, Pirard C, Hutchings G, Demylle D, Squifflet J, et al. Live birth after transplantation of frozen-thawed ovarian tissue after bilateral oophorectomy for benign disease. Fertil Steril. 2012;98:720–5.
Dittrich R, Lotz L, Keck G, Hoffmann I, Mueller A, Beckmann MW, et al. Live birth after ovarian tissue autotransplantation following overnight transportation before cryopreservation. Fertil Steril. 2012;97:387–90.
Kawamura K, Cheng Y, Suzuki N, Deguchi M, Sato Y, Takae S, et al. Hippo signaling disruption and Akt stimulation of ovarian follicles for infertility treatment. Proc Natl Acad Sci U S A. 2013;110:17474–9.
Revelli A, Marchino G, Dolfin E, Molinari E, Delle Piane L, Salvagno F, et al. Live birth after orthotopic grafting of autologous cryopreserved ovarian tissue and spontaneous conception in Italy. Fertil Steril. 2013;99:227–30.
Stern CJ, Gook D, Hale LG, Agresta F, Oldham J, Rozen G, et al. First reported clinical pregnancy following heterotopic grafting of cryopreserved ovarian tissue in a woman after a bilateral oophorectomy. Hum Reprod. 2013;28:2996–9.
Stern CJ, Gook D, Hale LG, Agresta F, Oldham J, Rozen G, et al. Delivery of twins following heterotopic grafting of frozen-thawed ovarian tissue. Hum Reprod. 2014;29:1828.
Callejo J, Salvador C, Gonzalez-Nunez S, Almeida L, Rodriguez L, Marques L, et al. Live birth in a woman without ovaries after autograft of frozen-thawed ovarian tissue combined with growth factors. J Ovarian Res. 2013;6:33.
Suzuki N, Yoshioka N, Takae S, Sugishita Y, Tamura M, Hashimoto S, et al. Successful fertility preservation following ovarian tissue vitrification in patients with primary ovarian insufficiency. Hum Reprod. 2015;30:608–15.
Demeestere I, Simon P, Dedeken L, Moffa F, Tsépélidis S, Brachet C, et al. Live birth after autograft of ovarian tissue cryopreserved during childhood. Hum Reprod. 2015;30:2107–9.
Tanbo T, Greggains G, Storeng R, Busund B, Langebrekke A, Fedorcsak P. Autotransplantation of cryopreserved ovarian tissue after treatment for malignant disease—the first Norwegian results. Acta Obstet Gynecol Scand. 2015;94:937–41.
Rodriguez-Wallberg KA, Karlström P-O, Rezapour M, Castellanos E, Hreinsson J, Rasmussen C, et al. Full-term newborn after repeated ovarian tissue transplants in a patient treated for Ewing sarcoma by sterilizing pelvic irradiation and chemotherapy. Acta Obstet Gynecol Scand. 2015;94:324–8.
Lorenzo F, Villamayor M, Buzzi PJ, Marconi G, Tiberon M, Young ET. Live birth with intrauterine insemination (IUH) after orthotopic transplantation of cryopreserved ovarian tissue in a young patient previously treated with chemotherapy for Askin’s disease. Argentina. e160 ASRM Abstracts Fertil Steril. 2014; 102 (3) Suppl. P-64.
Andersen CY. Success and challenges in fertility preservation after ovarian tissue grafting. Lancet. 2015;385:1947–48.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
This is an established treatment approved and authorized by the Danish Ministry of Health. The Minister of Health has approved the procedure. The collection of data, which were collected from patient records, was approved by the Danish Data Protection Agency and the Minister of Health (J.no.: 30-1372).
Therefore, for this type of study, formal consent is not required.
Conflict of interest
The authors declare that they have no competing interests.
Additional information
The original version of this article was revised: There were errors in the Discussion section and the last paragraph should be removed.
Capsule The data is reassuring and further suggests that cryopreservation of ovarian tissue is becoming an established fertility preservation method.
An erratum to this article is available at http://dx.doi.org/10.1007/s10815-017-0873-y.
Rights and permissions
About this article

Cite this article
Jensen, A.K., Macklon, K.T., Fedder, J. et al. 86 successful births and 9 ongoing pregnancies worldwide in women transplanted with frozen-thawed ovarian tissue: focus on birth and perinatal outcome in 40 of these children. J Assist Reprod Genet 34, 325–336 (2017). https://doi.org/10.1007/s10815-016-0843-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-016-0843-9