
Abstract
Purpose
The aim of this study is to report challenges encountered when conducting inter-institutional data collection of obstetric (prenatal and postpartum) and delivery outcomes for research purposes and to propose solutions for enhanced efficiency.
Methods
Data were collected from women who consented to collection of obstetric and delivery records for an observational study of pregnancy and delivery outcomes following infertility treatment. We analyzed key issues relevant to improving efficiency of obstetric and delivery data collection via quantification of effort (such as number of calls and faxes) required to obtain records from different types of obstetric clinics and hospitals before and after utilization of a revised authorization.
Results
At time of analysis, records were successfully collected from 320 of the 451 participants who had delivered. The 320 participants received obstetric care at 63 institutions and delivered at 27 hospitals, with 168 (52.5 %) delivering at institutions other than home facility. At time of consent (8 weeks gestation), 155 of 320 (48.5 %) correctly predicted where they would receive obstetric care and 176 (55 %) where they would delivery. Most facilities (nearly 90 %) rejected our original authorization, but most (90 %) accepted the revised authorization described in this manuscript.
Conclusions
Collecting records is time-consuming but important as over 50 % of our participants received care outside of the home facility. To efficiently collect outside records, we recommend that researchers interested in maternal and neonatal outcomes consider the guidelines outlined in this manuscript. This report also provides strong evidence of the need to develop data sharing through electronic health records for research purposes.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
It is becoming increasingly recognized that infertility treatment outcomes should include not only an analysis of live birth rate but also details regarding maternal and child health outcomes [1]. Multiple studies have raised concerns about an increased risk of adverse maternal and neonatal outcomes in women with infertility and with treatment of infertility, including an increased risk of preterm birth [2,3], low birth weight [4–6], perinatal hospitalizations, cesarean deliveries, hypertensive disorders [7], major fetal congenital anomalies [8, 9], and metabolic syndrome [10]. Although prior authors have emphasized the need to better understand the relationship between adverse outcomes and infertility treatments [11–14], there is a dearth of literature describing how to best conduct efficient pregnancy and delivery record collection from the variety of obstetric practice types and hospitals providing prenatal, delivery, and postpartum care to women after infertility treatment.
One could hypothesize that the use of electronic health records (EHR) would have greatly simplified the process for obtaining medical records. Prior studies have suggested ways for institutions to increase use of electronic research systems within clinical practices [15] and to increase inter-institutional data-sharing efficiency for clinical care [16–18]. However, EHR are not yet optimized for research [19] and data sharing. Furthermore, guidance regarding collection of medical records is particularly important for studies examining pregnancy outcomes after infertility, given that over half of all obstetrics and gynecology practices are either solo or single specialty and are not part of a larger integrated medical system [20]. The aims of this study are to assist researchers by reporting challenges encountered when conducting inter-institutional data collection of obstetric and delivery outcomes for research purposes and to propose solutions for improved efficiency.
Methods
Data for this manuscript were collected while conducting “Pregnancy Outcomes Following Infertility” (POFI), a longitudinal study funded by the National Institute of Health (NIH). All participants in POFI are female partners of couples experiencing infertility and receiving evaluation and treatment at the home academic institution’s fertility and reproductive health practice. POFI’s hypothesis requires the collection of data from prenatal, delivery, and postpartum care records. A research coordinator enrolled women in the fertility clinic at 8 weeks gestation following confirmation of pregnancy viability. At the time of consent to participate in POFI, participants signed a study-specific authorization form to be used to request their prenatal, delivery, and postpartum data, and provided the name of the obstetric practice and hospital where they planned to receive care. Included in the analysis are data of participants who signed consent at time of study initiation on October 6, 2011 until May 21, 2014, and whose prenatal, delivery, and postpartum records were successfully collected by the time that data analysis for this manuscript was initiated on June 12, 2015. Participants whose records we had not successfully collected by June 12, 2015, pregnancies that resulted in miscarriages, and participants withdrawn from the study were excluded. Our team defined miscarriage as a spontaneous loss of the fetus before 20 weeks of gestation. Miscarriage pregnancies were excluded from the analysis because the purpose of this NIH-funded project is to examine the effect of fertility treatment on the maternal outcomes (e.g. incidence of pre-eclampsia) among viable pregnancies. Reasons for withdrawal included delivery outside of the USA or patient choice. The POFI study and this analysis were approved by the home association’s Institutional Review Board (IRB).
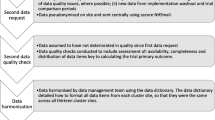
Medical records collection process (Fig. 1)
When collecting outcomes, we accessed data via the home institution’s EHR system (Electronic Privacy Information Center, EPIC) for patients who delivered at the home institution. Obstetrics records were available in home institution’s EPIC system if women received obstetrics care at the home institution; prenatal records were also available in the home institution’s EPIC by review of scanned documents for women who delivered at the home institution but received prenatal care elsewhere. However, no prenatal, postpartum, or delivery records were available in the home institution’s EPIC if the participant did not deliver at the home institution.

Methods of record collection for participants who delivered outside of the home institution
Many of our research participants either did not know where they would receive prenatal, delivery, and postpartum care at consent or changed their mind since time of consent at 8 weeks gestation. Therefore, after the expected time of delivery, the home institution hospital records were first checked to see if the patient delivered at the home institution. If we confirmed that they did not deliver at the home institution, we called participants to ask where they received prenatal, delivery, and postpartum care in order to request records from the appropriate institution. If needed, we contacted the clinic or hospital to determine if these outside institutions required a different authorization form from the one signed at consent, and to determine if we needed to send participants a follow-up authorization form (see Fig. 1). For participants who delivered outside of the home institution, we sent an authorization form to the relevant prenatal and postpartum provider(s) and delivery hospital to request records. If a participant received prenatal and postpartum care at more than one facility, we requested records from all to collect all available data.
When we began requesting records, most facilities did not accept our original, IRB-approved, study-specific authorization form. Some external institutions declined this original form due to one or more of the following missing items: detailed description of requested items, authorization expiration date, authorization purpose, statements of revocation, re-disclosure, and patient’s rights. Once our authorization form’s limitations were identified, we revised our form to include these Health Insurance requirements [21] (see Supplemental Table 1). New participants signed the revised form at the time of consent. We mailed the revised form to our previously consented participants. Institutions that did not accept this revised authorization form directed us to their institutional-specific form.
Documentation which allowed us to assess the data collection process for this manuscript
As a routine practice, we documented the number and type of obstetric facilities and delivery hospitals from which each patient received care. We recorded the date, frequency, and nature of contact attempts to participants, obstetric facilities, and hospitals. Contact attempts included calling participants, obstetric facilities, and hospitals; mailing follow-up authorization packets to participants for them to sign; and mailing or faxing authorizations to facilities to request records.
Statistical analysis
Differences between data collection processes and resources used during data collection per type of medical facility were tested using the Kruskal-Wallis test or Wilcoxon rank-sum test as appropriate with significance set at the 0.05 level. Statistical analyses were performed using statistical software R 3.1.2.
Results
The number of POFI participants who met inclusion criteria for this analysis was 320, with a mean age of 36 ± 4.4 years (Table 1). The majority of the participants were non-Hispanic Asian (48.4 %) or Caucasian (45 %). The participants received care from a mean of 1.1 obstetric facilities as some switched facility during pregnancy or moved geographically. At the time of consent, nearly half of participants accurately predicted where they would receive obstetric care and about half accurately predicted where they would deliver.
Our original authorization form was not accepted by 85.7 % of the outside obstetric facilities and 88.9 % of outside delivery hospitals. In contrast, only 6.4 % of obstetric facilities and 18.5 % of hospitals did not accept our revised authorization form. We felt it important not to abandon our efforts at obtaining records from facilities who did not accept even the revised form because although a low percentage of facilities declined our revised form, many of our participants received care at these facilities. Nearly one third (32.1 %) of participants received care at an obstetric clinic that did not accept the revised form, and over half (51.2 %) of women delivered at a hospital that did not accept the revised form.
For the 168 participants who delivered outside of the home institution, 33 signed an authorization form at consent that was accepted by their prenatal, delivery, and postpartum facilities, while 135 participants signed an authorization that was rejected by at least one of their care facilities (Table 2). Some of these women had signed the original form, while others signed the revised form that was not accepted by one or more of the facilities where care was received. A mean of 1.52 follow-up authorization forms were mailed to each of these 135 participants to collect the correct authorization form. In some cases, more than one follow-up authorization was mailed per participant because she moved from the area, misplaced, or never received the initial authorization. In order to collect the appropriate follow-up authorization, we made significantly more calls (p = 0.001) and mailed significantly more authorizations (p < 0.001) to the 135 participants with rejected authorization forms than to the 33 with accepted forms.
It is notable that less than a quarter of the women who received fertility care at the home institution also received their prenatal care at the home institution (Table 3). In general, there were no statistically significant differences in the work required to obtain records depending on what type of outside obstetric clinic or outside hospital the participant utilized. Exceptions are that we sent significantly more faxes to multi-specialty than to single-specialty obstetric facilities (p = 0.018) but made significantly more calls to solo obstetric facilities than multi-specialty (p = 0.007). There was tremendous variance in time-elapsed between requesting and receiving records, even when considering just any one type of obstetric clinic or hospital. However, once the correct authorization form was signed by the participant and returned, it took on average one month to request and receive all requested records (data not shown).
A charge was incurred for 13.8 % of record requests. The maximum value requested was $55 with a mean charge of $6.77 for all solo obstetric facilities, $6.04 for all single specialty, and $8.69 for all multi-specialty. The mean for all community hospitals was $2.67.
Discussion
To the best of our knowledge, this is the first paper focused on reporting key issues to consider in collecting pregnancy and delivery data for research purposes from women who conceived following fertility treatment in the United States. This report is timely given the recognition that some fertility treatments may increase the risk of obstetric complications such as pre-term delivery [2, 3] and pre-eclampsia [22], and therefore, fertility specialists performing research need these records to better understand what maternal characteristics and treatment parameters will optimize outcomes. Relying only on patient report of outcomes provides much less detail than is needed to rigorously correlate specific aspects of fertility treatment with the course of pregnancy, delivery, and neonatal outcome. Data from this manuscript may also help centers estimate research coordinator effort and cost of obtaining full prenatal care and delivery records.
Our experience clearly demonstrated the value of using an authorization form that is HIPAA compliant (see Supplementary Figure 1 for required elements) and accepted by the majority of obstetric clinics and hospitals. Having this authorization form signed when the participant is finalizing her care at the fertility practice significantly reduces the number of faxes sent and calls made, therefore, saving coordinator time and expediting data collection process. Because fewer than 50 % of women accurately predicted where they would receive obstetric care at time of their 8-week obstetric ultrasound in the fertility practice, a single universal form is critical to maximizing efficiency.
Even when all HIPAA requirements were met, a few institutions did not accept our revised authorization form due to institutional-specific requirements that were not listed on Supplementary Figure 1, and many of our patients received care at these institutions. For example, some facilities required the authorization form to have 14-point font per California’s Confidentiality of Medical Information Act (CMIA) Civil Code § 56.11a, and a few facilities required patients to date the authorization after the date of service. We now contact facilities to inquire about additional authorization requirements if a patient is receiving care from a facility where we have no prior experience.
Much hope has been placed on the possibility that EHR will increase the efficiency of the healthcare system. With the help of the Health Information Technology for Economic and Clinical Health Act of the American Recovery and Reinvestment Act in 2009 as well as the Medicare Electronic Health Records Incentive Program in 2011, there has been a recent increase in the number of hospitals and medical clinics using EHR systems [23–25]. With many practices adopting EHR systems, one may hope that the acquisition of obstetric and delivery records could be simply accomplished through electronic health information exchange [24] which should enable more efficient care coordination [25]. The American Congress of Obstetrics and Gynecology (ACOG) found that as of 2013, 72.7 % of OB/GYN practices in the United States used EHR [20]. However, EHRs are designed primary for financial, scheduling, and clinical care needs, not for research [19]. Additionally, among the facilities that use electronically based systems, most physician offices still did not share data electronically with other providers, at least as of 2013 [25]. Some obstetric practices in our community including our home institution use the electronic health information exchange system, CareEverywhere, which allows protected health information (PHI) to be shared among other EPIC users for care coordination. Unfortunately, CareEverywhere was inadequate for our research team as we were not able to access all needed records due to privacy regulations and because the available information was too limited. In addition, use of CareEverywhere required a separate verbal or written consent. Thus, for the majority of patients whose records were available on CareEverywhere, we still needed to collect the appropriate authorization and request their records via fax. Edwards describes similar barriers that impede effective electronic inter-institutional data sharing, such as lack of inter-institutional [26]. Electronic inter-institutional PHI-sharing tools will not simplify the current research data collection process until these problems have been systemically resolved. However, available inter-institutional electronic PHI sharing tools are worth exploring. Our difficulties of collecting these medical records via fax and mail provide evidence of the urgent need to push forward the development of more efficient data-sharing via electronic health records for research purposes.
It has been suggested that efficiency may be improved by having IRB approval to access records at all delivery hospitals or to use a central IRB that covers multiple hospitals [13]. While this is a reasonable suggestion, such a process would not be feasible in our area as there is no central IRB which covers most hospitals, and the number of hospitals and obstetrics clinics where our patients receive care is very high. In addition, facilities in our community generally require a written authorization instead of an IRB approval.
We propose several other recommendations that we wish to share based on experience, even though we acknowledge that we did not specifically collect data to validate the recommendations. We routinely contact participants between their third trimester and three months postpartum to reduce the risk of loss to follow-up. Although we did not collect data to quantitatively report the impact of waiting until longer than three months after delivery to contact the participant, we did encounter some cases where women were more difficult to reach and records were difficult to obtain when a longer time elapsed between delivery and our initial contact with the participant. When requesting newborn records, one must have a second authorization form that lists the newborn as the patient and is signed by the guardian. Basic newborn information (birth weight, sex) will be in maternal delivery records, but more in-depth information (length of time in NICU, diagnoses discovered in NICU, long-term diagnoses, etc.) will be in newborn, not maternal, records, thus requiring this second authorization form. We noticed that not all medical records employees were medically trained and that many medical records departments used institutional-specific terms when referring to common aspects of patients’ records. We were most successful when using non-technical terms to describe records so that laypeople can identify the appropriate reports (e.g. nurses’ notes, prenatal labs) and institutional-specific terms that we collected by contacting each facility.
Our report has several limitations. Initially, our research team had aimed to receive all prenatal, delivery, and postpartum records within three months of delivery. 451 patients had delivered before or on March 12, 2015; however, by June 12, 2015, when we began this analysis, we had only received records from 320 of these participants. The remaining 131 participants with pending records delivered at outside institutions, and their obstetric and delivery records are currently being requested. Thus, about two thirds of our patients deliver outside of the home institution, instead of less than one half (Table 2), if all of these women are included in the denominator. The effort that will be required to obtain all records is almost certainly underestimated in this manuscript, as these most difficult and time-consuming cases were not included.
Although significant time and effort are involved in collecting records from obstetric clinics and hospitals outside of the home academic institution, we believe that such effort is important. Limiting the pregnancy follow-up to just those who receive care at our home institution would severely limit the sample size, as over 80 % of our fertility patients attended an outside obstetric clinic (including those whose records we have not yet received), and two thirds of the population from our fertility practice delivered at an outside hospital. Many fertility practices are not hospital-based and thus would have no immediate access to delivery records. Limiting to only the home institution would also make our results less generalizable to the overall population.
Conclusion
It is critically important that investigators who are studying pregnancy outcomes after infertility have access to records that will allow them to determine what patient and treatment factors affect maternal and fetal health during pregnancy, delivery, and in the postpartum. We suggest that to increase efficiency, it is important to prepare a HIPAA-compliant authorization that is accepted by the appropriate institutions before initiating recruitment. We also propose other recommendations as outlined in this manuscript. Although electronic data sharing tools are not yet sufficient research purposes, the data presented in this paper provide evidence of the need for such tools, and we strongly support future work to develop these options.
References
Henningsen AK, Pinborg A. Birth and perinatal outcomes and complications for babies conceived following ART. Semin Fetal Neonatal Med. 2014;19:234–8.
Tepper N, Farr S, Cohen B, Nannini A, Zhang Z, Anderson J, et al. Singleton preterm birth: risk factors and association with assisted reproductive technology. Matern Child Health J. 2012;16:807–13.
Qin J, Liu X, Sheng X, Wang H, Gao S. Assisted reproductive technology and the risk of pregnancy-related complications and adverse pregnancy outcomes in singleton pregnancies: a meta-analysis of cohort studies. Fertil Steril. 2016;105:73–85.
Declercq E, Luke B, Belanoff C, Cabral H, Diop H, Gopal D, et al. Perinatal outcomes associated with assisted reproductive technology: the Massachusetts Outcomes Study of Assisted Reproductive Technologies (MOSART). Fertil Steril. 2015;103:888–95.
Pinborg A, Wennerholm U, Romundstad L, Loft A, Aittomaki K, Soderstr- rom-Anttila V, et al. Why do singletons conceived after assisted reproduction technology have adverse perinatal outcome? Systematic review and meta-analysis. Hum Reprod Update. 2013;19:87–104.
Baker VL, Brown MB, Luke B, Conrad KP. Association of number of retrieved oocytes with live birth rate and birth weight: an analysis of 231,815 cycles of in vitro fertilization. Fertil Steril. 2015;103:931–8.
Stern JE, Luke B, Tobias M, Gopal D, Hornstein MD, Diop H. Adverse pregnancy and birth outcomes associated with underlying diagnosis with and without assisted reproductive technology treatment. Fertil Steril. 2015;103:1438–45.
Davies MJ, Moore VM, Willson KJ, Van Essen P, Priest K, Scott H, et al. Reproductive technologies and the risk of birth defects. N Engl J Med. 2012;366:1803–13.
Pelkonen S, Hartikainen AL, Ritvanen A, Koivunen R, Martikainen H, Gissler M, et al. Major congenital anomalies in children born after frozen embryo transfer: a cohort study 1995–2006. Hum Reprod. 2014;29:1552–7.
Shankaran S. Outcomes from infancy to adulthood after assisted reproductive technology. Fertil Steril. 2014;101:1217–21.
Harbin Consensus Conference Workshop Group. Improving the reporting of clinical trials of infertility treatments (IMPRINT): modifying the CONSORT statement. Fertil Steril. 2014;102:952–9.e15.
Barnhart K. Live birth is the correct outcome for clinical trials evaluating therapy for the infertile couple. Fertil Steril. 2014;101:1205–8.
Silver R. Infertility trial outcomes: healthy moms and babies. Fertil Steril. 2014;101:1209–16.
Legro RS, Wu X. Introduction: choosing the main outcome of an infertility trial is harder than you think. Fertil Steril. 2014;101:1201–2.
Fernandopulle R, Patel N. How the electronic health record did not measure up to the demands of our medical home practice. Health Aff. 2010;29:622–8.
Vest JR, Issel LM, Lee S. Experience of using information systems in public health practice: findings from a qualitative study. Online J Public Health Inform. 2014;5:227.
Kho AN, Hynes DM, Goel S, Solomonides AE, Price R, Hota B, et al. CAPriCORN: Chicago area patient-centered outcomes research network. J Am Med Inform Assoc. 2014;21:607–11.
Health Quality Ontario. Electronic tools for health information exchange: an evidence-based analysis. Ont Health Technol Assess Ser. 2013;13:1–76.
Sung NS, Crowley Jr WF, Genel M, Salber P, Sandy L, Sherwood LM, et al. Central challenges facing the national clinical research enterprise. JAMA. 2003;289:1278–87.
Johnson T. 2013 Socioeconomic Survey of ACOG Fellows. In: HIPAA Authorization for Research. In: Educational Materials, Authorizations. U.S. Department of Health and Human Services: National Institute of Health. 2013. http://www.acog.org/-/media/Departments/Practice-Management-and-Managed-Care/2013SocioeconomicSurvey.pdf. Accessed 27 Jun 2015.
Clinical Research and the HIPAA Privacy Rule. In: HIPAA for Professionals. In: Special Topics, Research. In: Clinical Research Fact Sheet. U.S. Department of Health and Human Services: National Institute of Health. 2004. https://privacyruleandresearch.nih.gov/clin_research.asp. Accessed 14 Mar 2015.
Wa tanabe N, Fujiwara T, Suzuki T, Jwa SC, Taniguchi K, Yamanobe Y, et al. Is in vitro fertilization associated with preeclampsia? A propensity score matched study. BMC Pregnancy Childbirth. 2014;14:69.
Hsiao CJ, Jha AK, King J, Patel V, Furukawa MF, Mostashari F. Office-based physicians are responding to incentives and assistance by adopting and using electronic health records. Health Aff. 2013;32:81470–7.
Charles D, Gabriel M, Furukawa MF. “Adoption of electronic health record systems among U.S. non-federal acute care hospitals: 2008–2013”, ONC data brief, no. 16. Washington, DC: Office of the National Coordinator for Health Information Technology; 2014.
Furukawa MF, King J, Patel V, Hsiao CJ, Adler-Milstein J, Jha AK. Despite substantial progress in EHR adoption, health information exchange and patient engagement remain low in office settings. Health Aff. 2014;33:91672–9.
Edwards A, Hollin I, Barry J, Kachnowski S. Barriers to cross-institutional health information exchange: a literature review. J Healthc Inf Manag. 2010;24:22–34.
Acknowledgments
The authors would like to thank all participants, prenatal/postpartum facilities, and delivery hospitals that enabled the collection of these data. This study was funded by Award Number P01 HD 065647-01A1 from the National Institute of Child Health and Human Development. Frauke von Versen-Hoeynck was funded by the German Research Foundation (VE490/8-1).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Capsule
To efficiently collect outside records, we recommend that researchers interested in maternal and neonatal outcomes consider the guidelines outlined in this manuscript.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Figure 1
(DOCX 84.5 kb)
Rights and permissions
About this article

Cite this article
Floyd, E.G., von Versen-Höynck, F., Liu, J. et al. Collection of pregnancy outcome records following infertility—challenges and possible solutions. J Assist Reprod Genet 33, 993–999 (2016). https://doi.org/10.1007/s10815-016-0733-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-016-0733-1