
Abstract
Purpose
As fertilization with unselected apoptotic spermatozoa may contribute to failures in assisted reproductive techniques, it has become essential to remove this type of sperm in order to increase the success rates. Magnetic-activated cell sorting (MACS) is a sperm preparation technique that isolates non-apoptotic spermatozoa based on the expression of phosphatidylserine in the membrane of apoptotic sperm. Therefore, we aimed to evaluate whether there was a significant decrease in sperm DNA fragmentation (sDNAfrag) and verify which protocol was the most efficient.
Methods
Hundred semen samples were allocated into five distinct groups and processed according to a combination of MACS with density gradient centrifugation (DGC) and swim-up (SU) techniques. Sperm DNA fragmentation was evaluated by terminal deoxynucleotidyl transferase dUTP nick-end labeling (TUNEL) assay.
Results
Groups DGC-SU (73.4 %), DGC-MACS-SU (78.9 %), DGC-SU-MACS (53.8 %) and MACS-SU (73.5 %) presented a significant decrease in sDNAfrag but the highest reduction rate was obtained with MACS-DGC-SU (83.3 %). The later was also negatively correlated with sperm vitality, membrane integrity and progressive motility. Additionally, teratozoospermic patients presented a tendency to have lower sDNAfrag reduction rates than asthenozoospermic and asthenoteratozoospermic patients.
Conclusions
Based on the results, MACS showed potential to optimize the sDNAfrag reduction rate, when applied to raw semen, before DGC and SU, especially in samples with low values of progressive motility, vitality and hypoosmotic swelling test.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Semen analysis is one of the most relevant tests used in the evaluation of male factor infertility. The quality of semen is essentially defined based on the assessment of sperm concentration, motility and morphology, according to the World Health Organization (WHO) criteria [1]. These characteristics tend to be superior in fertile than in infertile men [2]. Although WHO values for semen evaluation are a mere reference and may fail rigorous clinical and statistical standards as a significant proportion of patients exhibiting normal semen parameters values have unexplained infertility [3], a strong relationship between the influence of semen quality and the embryological and clinical outcomes has been established [4].
Another essential aspect is the sperm ability to deliver an undamaged nucleus capable of supporting the development of healthy progeny [5]. Apart the analyses of chromosomal abnormalities, several functional tests have been developed to measure sperm DNA integrity and study its impact on fertilization, embryo development and pregnancy, but at present conflicting results have been obtained regardless the assisted reproductive technology (ART) treatment used [6, 7]. Sperm DNA integrity was analyzed through the detection of DNA strand breaks [8–10], by the evaluation of the sperm chromatin structure [11, 12] or by detecting the level of protamination and compaction of the sperm chromatin [13].
Despite the controversies associated with reproductive outcomes using functional tests, it is clear that sperm DNA damage has adverse effects on them. To improve the embryological and clinical outcomes, non-invasive methods were developed to select sperm free of DNA damage for clinical use. Some of these methods gave, however, a limited success [14]. The application of morphologically selected sperm (IMSI), which uses motile sperm organelle morphological examination (MSOME), was shown to only increase the clinical pregnancy and live birth rates in cases of recurrent implantation failure [15]; the negative electrical charge in sperm membrane (Zeta method) was used to isolate mature sperm but this procedure only increased the fertilization rate [16]; the isolation of mature sperm by electrophoresis did not improve embryological outcomes [17]; and isolation of mature sperm by detecting sperm surface hyaluronic acid (HA) binding sites provided no clinical and embryological achievements [18].
In contrast, determination of phosphatidylserine (PS) translocation to the outer membrane leaflet during early apoptosis by annexin-V binding seems to be the most promising method [19], either using flow-cytometry cell sorting or magnetic-activated cell sorting (MACS) [20]. This technique has been applied in addition to the classic sperm preparation techniques that use differential density gradient centrifugation (DGC) and swim-up (SU) methods. Results showed that the combination of DGC-MACS enhances sperm viability [21], maturity [22], and decreases sperm aneuploidy and apoptosis [23]. Similarly, positive effects with the use of DGC-MACS on the embryological and clinical outcomes were observed, as some authors found an increase in the pregnancy rate but not in the implantation and miscarriage rates [24], and others an increase in the fertilization, embryo quality [25], pregnancy [26, 27] and live-birth rates [28].
Based on these results, and using the TUNEL assay to measure sperm DNA fragmentation (sDNAfrag), we evaluated the effect of combining the MACS technology with the classic sperm preparation technique, the DGC, but also with the SU method, in order to define the best method of sperm preparation and undercover any relationship to semen parameters. We compared five groups, DGC-SU, DGC-MACS-SU, DGC-SU-MACS, MACS-DGC-SU and MACS-SU. Although all protocols showed a significant reduction on sDNAfrag rates, the protocol MACS-DGC-SU gave the higher reduction rate. This protocol was also the one that strongly negatively correlated with vitality and membrane integrity and moderately correlated with progressive sperm motility.
Material and methods
Patients and semen sample collection
Semen samples were obtained under informed and written consent according to the National Law on Medically Assisted Procreation (PMA, Law 32/2006) and National Council guidelines on Medically Assisted Procreation (CNPMA, 2008), from patients who were performing spermiogram analysis at clinic (CGR-ABarros). The selected group consisted of 100 men, with a mean age of 34.5 ± 5.0, presenting a sperm count of ≥107/ml (MACS technique inherent limitation). Semen samples were collected into sterile containers, after 3–5 days of sexual abstinence. After liquefaction, semen parameters were evaluated according to WHO guidelines [1]. Each semen sample (one per day) was transferred to university facilities (ICBAS-UP) in order to be processed, with a transportation time of about 30 min.
Experimental design
Semen samples were randomly allocated into five groups of 20 patients. In Group 1, samples were processed according to classic semen preparation techniques, which included DGC followed by SU. In the remaining four groups (Groups 2–5) samples were further treated with MACS technology. The difference between them relied on the moment of application of MACS: after DGC (Group 2), after SU (Group 3) or before DGC (Group 4). In Group 5, DGC was not performed and MACS was applied before SU (Table 1). Semen samples were randomly allocated into five groups of 20 patients; a procedure that produced quite homogeneous independent comparable groupings, by unbiasedly assigning each patient to every assay condition, giving all participants equal chances of selection.
Sperm preparation by DGC and SU
For each sample 1 mL of semen was processed. Seminal fluid was removed by washing with 2 mL of Sperm Preparation Medium (SPM; Medicult Origio, Jyllinge, Denmarck) followed by centrifugation at 445 g for 5 min. Sperm were then resuspended in 1.5 mL SPM, centrifuged at 445 g for 20 min with 90–45 % PureSperm (Nidacon, Gothenburg, Sweden), and the pellet washed twice with SPM at 445 g for 10 min. The pellet was then layered with 0.5 mL in vitro fertilization (IVF) medium (Medicult Origio) and left for 1 h at room temperature (RT).
Isolation of non-apoptotic spermatozoa by MACS
Sperm were incubated with 20 μL of annexin-V conjugated microbeads and 80 μL of binding buffer solution, both provided by the Annexin-V MicroBead Kit (Miltenyi Biotec, Bergisch Gladbach, Germany), for 15 min at RT. After adding more 400 μL of binding buffer, the suspension was loaded on a separation column (MiniMacs; Miltenyi Biotec). The labeled spermatozoa (annexin-V positive) were retained in the column, whereas the non-apoptotic and viable spermatozoa (annexin-V negative) passed through the column. This latter fraction was recovered and further processed.
Determination of sDNAfrag by terminal deoxynucleotidyl transferase dUTP nick-end labeling (TUNEL) assay
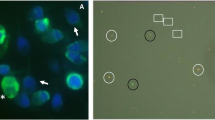
For each patient, sDNAfrag was evaluated by the TUNEL assay after the removal of seminal fluid (T0) and at the end (T1) of each procedure (Table 1), using the In Situ Cell Death Detection Kit (Roche, Mannheim, Germany). Sperm were smeared onto adhesion microscope slides, air-dried and fixed with 4 % paraformaldehyde (Merck, Darmstadt, Germany) in phosphate-buffered saline (PBS; Sigma, Steinheim, Germany), for 1 h at RT. Slides were then washed in PBS and permeabilized with 0,1 % Triton-X (Sigma) in 0,1 % sodium citrate (Merck) for 2 min at 4 °C. After two washes in PBS for 5 min, slides were incubated with a 25 μL TUNEL mixture for 1 h at 37 °C, in a dark moist chamber. After incubation, slides were washed two times in PBS for 2 min and counterstained with 10 μL of Vectashield antifade medium containing 4′,6-diamidino-2-phenylindole (DAPI; Vector Laboratories, Burlingame, CA, USA). On each slide, at least 500 morphologically normal spermatozoa were counted in a Leitz DMRBE fluorescence microscope (Leica, Wetzlar, Germany). The number of spermatozoa emitting green fluorescence (TUNEL-positive) was recorded as a percentage of the total sperm counted (DAPI stained).
Statistical analysis
Statistical tests were performed using the STATISTICA software (Version 12; Statsoft, USA). Levene’s Test and Shapiro-Wilk were carried out to assess normal distribution and homogeneity of variances, respectively. Given that in most cases normality was not observed, non-parametric tests were performed. However, as identical results for both parametric and non-parametric tests were obtained in most cases, we opted for presenting them according to the parametric form. Those cases where different results were obtained, are presented according to the non-parametric form. A paired-samples t-test and a non-parametric Wilcoxon Matched Pairs Test were conducted to compare sDNAfrag between the two populations of spermatozoa for each patient. The one-way ANOVA through Tukey post-test was used to assess the differences between groups and subgroups. In a corresponding manner, the non-parametric Kruskal-Wallis test through Mann–Whitney U post-test was performed. Linear correlation and covariance analysis between sDNAfrag reduction and semen parameters were also performed. A p-value < 0.05 was considered statistically significant for all tests.
Results
Age, semen parameters and sDNAfrag in raw samples
No significant differences were found between groups regarding age (F(4, 95) = 1.057, p = 0.382), progressive motility (PM) (F(4, 95) = 1.697, p = 0.157), vitality (VT) (F(4, 95) = 0.247, p = 0.911), hypoosmotic swelling test (HOST) (F(4, 95) = 0.610, p = 0.656), normal morphology (F(4, 95) = 0.402, p = 0.807), head (F(4, 95) = 0.324, p = 0.861), mid-piece (F(4, 95) = 1.754, p = 0.145) and flagellum (F(4, 95) = 0.869, p = 0.485) abnormalities, as well as sDNAfrag (F(4, 95) = 1.954, p = 0.108) (Table 2). Group 3 showed significant lower sperm concentration (H (4, N = 100) = 18.386, p = 0.001) in relation to the other groups (p < 0.01), and significant lower rapid progressive motility (F(4, 95) = 4.168, p = 0.004) to all groups (p < 0.05) except to Group 5. Although not significant, Group 3 also presented the highest sDNAfrag.
Reduction of sDNAfrag
All groups showed a significant reduction in sDNAfrag between the two times of analysis (T0 and T1), Group 1 (t(19) = 6.15, p = 0.000), Group 2 (t(19) = 5.46, p = 0.000), Group 3 (t(19) = 4.03, p = 0.001), Group 4 (t(19) = 5.48, p = 0.000) and Group 5 (t(19) = 6.37, p = 0.000) (Table 3).
Efficiency of sDNAfrag reduction
Two approaches were used to assess the groups’ greater efficacy in reducing sDNAfrag. Given that the ratio between final fragmentation and initial fragmentation (T1/T0) indicates the amount of DNA fragmentation that remains in the sample of a patient, the unit minus this ratio was used as an individual measure of the sDNAfrag reduction. On the other hand, it was used the difference between initial and final fragmentation (T0 - T1), which indicates the amount of sDNAfrag that was removed from a sample. The mean values obtained for each group are shown in Table 3. Using the ratio approach a statistically significant difference was found (F(4, 95) = 5.181, p = 0.001) for Group 3, which proved to be significantly less efficient in the reduction of sDNAfrag compared to the other groups (p < 0.05). However, using the difference approach, no statistically significant differences were found between groups (F(4, 95) = 0.615, p = 0.653). Although the ratio approach did not show significant differences between groups 1, 2, 4 and 5, an effect size could influence these results. Effect size is estimated by the ratio of the mean difference between the experimental and the control groups divided by the standard deviation of the control group [29]. Using Group 1 as a control and according to Cohen’s guidelines, a value close to “moderate” (d = 0.5) was found for Group 4 (d = 0.41), whereas Group 2 (d = 0.23) and Group 5 (d = 0.01) showed values considered “small” (d = 0.2). By this method, significance could be obtained if samples attained a “high” value (d = 0.8), and thus it is possible that with a larger sample a significant difference would be obtained for Group 4 regarding sDNAfrag reduction.
Efficiency of sDNAfrag reduction and semen parameters
Correlation analysis detected several relationships between semen parameters and sDNAfrag. Using the ratio approach, significant correlations were found only in Groups 1 and 3. For Group 1, the reduction of sDNAfrag was negatively correlated with PM (r = −0.452; p = 0.045) and VT (r = −0.462; p = 0.04), whereas in Group 3 it was positively correlated with age (r = 0.548; p = 0.012). Using the difference approach, significant correlations were found in all groups, except for Group 2. In Group 1, the sDNAfrag difference was positively correlated with flagellum abnormalities (r = 0.553; p = 0.011), whereas in Group 3 it was negatively correlated with PM (r = −0.451; p = 0.046). In Group 4, it was strong negatively correlated with VT (r = −0.842; p = 0.000) and HOST (r = −0.799; p = 0.000), and moderate negatively correlated with PM (r = −0.528; p = 0.017). Concerning Group 5, there was a positive correlation with flagellum abnormalities (r = 0.563; p = 0.010), and a negative correlation with VT (r = −0.635; p = 0.003).
As any of the semen parameters could be influencing the relationships between groups regarding the reduction of sDNAfrag, a covariance analysis was performed. Concerning the ratio approach, the covariates concentration (F(1, 94) = 6.096, p = 0.015) and age (F(1, 94) = 7.835, p = 0.006) demonstrated to be significantly related to the results observed, but when the effect of both was removed ((F(4, 94) = 3.309, p = 0.014) and (F(4, 94) = 4.995, p = 0.001), removal of concentration and age, respectively), no alterations occurred in the results previously described. Still, Group 3 remained the group in which sDNAfrag reduction was lower. An identical result was found using the difference approach. The covariates PM (F(1, 94) = 11.639, p = 0.001), VT (F(1, 94) = 22.68, p = 0.000), HOST (F(1, 94) = 11.862, p = 0.001) and flagellum abnormalities (F(1, 94) = 11.2, p = 0.001) influenced the amount of sDNAfrag removed, but this influence did not alter the results obtained when their effects were removed ((F(4, 94) = 1.032, p = 0.395), (F(4, 94) = 0.7, p = 0.594), (F(4, 94) = 0.583, p = 0.676) and (F(4, 94) = 0.483, p = 0.748) removal of PM, VT, HOST and flagellum abnormalities, respectively).
Efficiency of sDNAfrag reduction using subgroups
As results could be influenced by different semen parameters’ degrees of severity, a further analysis was conducted subdividing groups according to the different pathologies found: asthenozoospermia (A), teratozoospermia (T) and asthenoteratozoospermia (AT) (Table 4). Controls used were derived from samples showing each specific spermiogram parameter normal (≥25 % rapid progressive motility or ≥4 % normal morphology). There were only two patients with oligozoospermia, whereby no comparisons could be done regarding this subgroup. Comparisons between groups revealed a significant lower reduction of sDNAfrag in the A subgroup (H (4, N = 55) = 10.119, p = 0.039) of Group 3 in relation to Groups 1–4 (p < 0.05). Regarding subgroups T (H (4, N = 45) = 7.605, p = 0.107) and AT (F(4, 24) = 2.304, p = 0.088), no differences were found. Comparisons inside groups did not showed significant differences regarding subgroups A, T or AT, for Group 1 (F(2, 21) = 1.843, p = 0.183), Group 2 F(2, 22) = 0.466, p = 0.634), Group 3 (F(2, 26) = 0.582, p = 0.566), Group 4 F(2, 18) = 0.472, p = 0.631) and Group 5 (F(2, 29) = 0.039, p = 0.962). Finally, comparisons between each subgroup and the controls (Table 4) showed no significant differences.
Discussion
Regarding the use of MACS in semen processing, the majority of the studies compared DGC with DGC followed by MACS (DGC-MACS), with sDNAfrag determined by TUNEL assay at the end of both techniques. Comparing DGC with DGC-MACS, in a study comprising 60 patients with intrauterine insemination failures, authors obtained sDNAfrag reduction of about 26.7 % [30]. Using the same comparison, another report on 35 donors, achieved around 32.6 % of sDNAfrag reduction [31]. An additional study obtained a near 96.3 % sDNAfrag reduction. Nonetheless this was accomplished in a strict sample of 6 normozoospermic (NZ) patients with IVF failures and high initial sDNAfrag values [23]. These methods correspond to our Group 1 (DGC-SU) and Group 2 (DGC-MACS-SU), which gave a reduction in sDNAfrag of about 73.4 and 78.9 %, respectively, with no significant differences between both. The higher values here obtained can be explained by several differences: we did not use flow-cytometry, our fluorescence count of 500 sperm was restricted to sperm with normal morphology, and we performed the TUNEL assay after SU (Table 1).
Applying the same comparative method, and in comparison with the raw fraction, others showed that by the DGC-MACS procedure a significant higher sDNAfrag reduction could be obtained, being about 61.5 % (0 % with DGC) in 11 NZ, 72 % (8 % with DGC) in 10 T and 73 % (37.8 % with DGC) in 12 AT patients [22]. Our results exhibited higher sDNAfrag reduction in DGC-SU (about 82.9 % in A, 72.0 % in T and 78.1 % in AT patients) and in DGC-MACS-SU (about 78.3 % in A, 79.3 % in T and 87.5 % in AT patients), but with no differences between both methods. Again, these differences may be due to the fact that authors counted 200 sperm indiscriminately, whereas our fluorescence count of 500 sperm was restricted to sperm displaying normal morphology. Besides we performed the TUNEL assay after SU.
Finally, in a cohort of 15 semen samples randomly collected from men attending infertility consultations, authors compared individually sDNAfrag reduction (TUNEL-fluorescence microscopy) in DGC (28.4 %), MACS (26.9 %), DGC-MACS (40.7 %) and MACS-DGC (48.6 %), and could conclude that all methods efficiently decreased sDNAfrag, that the use of a double procedure was superior to a single process, and that the MACS-DGC method was preferable as together (MACS + DGC) further decreased the sperm apoptotic ratio [32]. These groups corresponded to our Group 1 (DGC-SU: 73.4 %), Group 5 (MACS-SU: 73.5 %), Group 2 (DGC-MACS-SU: 78.9 %) and Group 4 (MACS-DGC-SU: 83.3 %), respectively. This increase in the reduction of the sDNAfrag might be explained by the fact that we have always measured sDNAfrag in the SU fraction, as it is the fraction used for ART treatments [33] and has been recognized to significantly improve sperm selection [34]. Further, at TUNEL analysis, we counted only morphological normal sperm, which adds a new significance to the method. Although, as above, our groups showed a significant reduction in sDNAfrag between the initial and the final steps, there were no differences between them. Also and albeit relative, the best method seemed to be the MACS-DGC as the effect size revealed a value close to moderate for this group, which suggests that an increase in sample size may offer significance in future analysis. Furthermore, it was the MACS-DGC group that evidenced strong negative correlations with sperm VT and sperm membrane integrity, and moderate negative correlations with PM.
Other methods for detection of sperm integrity have also been performed. In a study of 21 infertile patients, authors compared PS translocation in the raw fraction, after DGC and after DGC-MACS, and observed a reduction of annexin-V positive sperm of about 40.7 % after DGC and 69.7 % after DGC-MACS, reinforcing the notion that this last method should be elected for clinical use. However, and curiously, authors could not found an improvement of the results using SU [35]. In another study, with 28 infertile patients, authors compared the membrane-based electrophoretic filtration system technique with the DGC method, but after measuring sDNAfrag using TUNEL/flow-cytometry they found no significant differences between the two techniques [17]. Comparisons were also performed in 51 infertile patients using DGC against the selection of sperm based on its membrane negative charge (Zeta method), with sDNAfrag being detected by TUNEL (200 sperm counted). Besides authors found a higher sDNAfrag reduction with the Zeta method (about 62.8 %) than with the DGC procedure (48.4 %) [16]. Using the same system, others in 26 infertile patients, compared the DGC-Zeta method with MACS-DGC, with sDNAfrag being quantified by TUNEL (500 sperm counted). Results showed a higher reduction in sDNAfrag with the DGC-Zeta method (48.7 %) than with the MACS-DGC procedure (29.7 %) [36]. Lastly, via HA assay and sDNAfrag measured by TUNEL (500 sperm counted), DGC was compared with DGC-HA in 58 IVF patients. Authors observed a significant higher decrease (26.4 %) in sDNAfrag with the DGC-HA method [18].
In conclusion, the present work allowed realizing that even though the classical protocol of sperm preparation DGC-SU is very efficient in reducing sDNAfrag, the further application of MACS has the potential to optimize the sDNAfrag reduction rate. By comparing all possible combinations between DGC, MACS and SU, we could show that the method MACS-DGC-SU yielded the highest sDNAfrag reduction rate, and that this was associated with sperm vitality, membrane integrity and progressive motility. To confirm these results, a larger number of patients should be involved in the study and its clinical application would be of utmost importance. Due to clinical costs of the technique data suggest that it could be firstly applied to sperm samples with low progressive motility, vitality and membrane integrity.
References
World Health Organization (WHO). WHO laboratory manual for the examination and processing of human semen. 5th ed. Geneva: World Health Organization; 2010.
Nallella KP, Sharma RK, Aziz N, Agarwal A. Significance of sperm characteristics in the evaluation of male infertility. Fertil Steril. 2006;85(3):629–34. doi:10.1016/j.fertnstert.2005.08.024.
ASRM. Effectiveness and treatment for unexplained infertility. Fertil Steril. 2006;86(5 Suppl 1):S111–4. doi:10.1016/j.fertnstert.2006.07.1475.
Zinaman MJ, Brown CC, Selevan SG, Clegg ED. Semen quality and human fertility: a prospective study with healthy couples. J Androl. 2000;21(1):145–53. doi:10.1002/j.1939-4640.2000.tb03284.x.
Aitken RJ. Sperm function tests and fertility. Int J Androl. 2006;29(1):69–75. doi:10.1111/j.1365-2605.2005.00630.x. discussion 105–8.
Chohan KR, Griffin JT, Lafromboise M, De Jonge CJ, Carrell DT. Comparison of chromatin assays for DNA fragmentation evaluation in human sperm. J Androl. 2006;27(1):53–9. doi:10.2164/jandrol.05068.
Delbes G, Hales BF, Robaire B. Toxicants and human sperm chromatin integrity. Mol Hum Reprod. 2010;16(1):14–22. doi:10.1093/molehr/gap087.
Simon L, Proutski I, Stevenson M, Jennings D, McManus J, Lutton D, et al. Sperm DNA damage has a negative association with live-birth rates after IVF. Reprod Biomed Online. 2013;26(1):68–78. doi:10.1016/j.rbmo.2012.09.019.
Henkel R, Kierspel E, Hajimohammad M, Stalf T, Hoogendijk C, Mehnert C, et al. DNA fragmentation of spermatozoa and assisted reproduction technology. Reprod Biomed Online. 2003;7(4):477–84.
Benchaib M, Lornage J, Mazoyer C, Lejeune H, Salle B, Francois GJ. Sperm deoxyribonucleic acid fragmentation as a prognostic indicator of assisted reproductive technology outcome. Fertil Steril. 2007;87(1):93–100. doi:10.1016/j.fertnstert.2006.05.057.
Virro MR, Larson-Cook KL, Evenson DP. Sperm chromatin structure assay (SCSA) parameters are related to fertilization, blastocyst development, and ongoing pregnancy in in vitro fertilization and intracytoplasmic sperm injection cycles. Fertil Steril. 2004;81(5):1289–95. doi:10.1016/j.fertnstert.2003.09.063.
Lin MH, Kuo-Kuang Lee R, Li SH, Lu CH, Sun FJ, Hwu YM. Sperm chromatin structure assay parameters are not related to fertilization rates, embryo quality, and pregnancy rates in in vitro fertilization and intracytoplasmic sperm injection, but might be related to spontaneous abortion rates. Fertil Steril. 2008;90(2):352–9. doi:10.1016/j.fertnstert.2007.06.018.
Tavalaee M, Razavi S, Nasr-Esfahani MH. Influence of sperm chromatin anomalies on assisted reproductive technology outcome. Fertil Steril. 2009;91(4):1119–26. doi:10.1016/j.fertnstert.2008.01.063.
Henkel R. Sperm preparation: state-of-the-art–physiological aspects and application of advanced sperm preparation methods. Asian J Androl. 2012;14(2):260–9. doi:10.1038/aja.2011.133.
Boitrelle F, Guthauser B, Alter L, Bailly M, Bergere M, Wainer R, et al. High-magnification selection of spermatozoa prior to oocyte injection: confirmed and potential indications. Reprod Biomed Online. 2014;28(1):6–13. doi:10.1016/j.rbmo.2013.09.019.
Kheirollahi-Kouhestani M, Razavi S, Tavalaee M, Deemeh MR, Mardani M, Moshtaghian J, et al. Selection of sperm based on combined density gradient and Zeta method may improve ICSI outcome. Hum Reprod. 2009;24(10):2409–16. doi:10.1093/humrep/dep088.
Fleming SD, Ilad RS, Griffin AM, Wu Y, Ong KJ, Smith HC, et al. Prospective controlled trial of an electrophoretic method of sperm preparation for assisted reproduction: comparison with density gradient centrifugation. Hum Reprod. 2008;23(12):2646–51. doi:10.1093/humrep/den330.
Tarozzi N, Nadalini M, Bizzaro D, Serrao L, Fava L, Scaravelli G, et al. Sperm-hyaluronan-binding assay: clinical value in conventional IVF under Italian law. Reprod Biomed Online. 2009;19 Suppl 3:35–43.
Almeida C, Sousa M, Barros A. Phosphatidylserine translocation in human spermatozoa from impaired spermatogenesis. Reprod Biomed Online. 2009;19(6):770–7.
Grunewald S, Paasch U. Sperm selection for ICSI using annexin V. Methods Mol Biol. 2013;927:257–62. doi:10.1007/978-1-62703-038-0_23.
Said TM, Grunewald S, Paasch U, Glander HJ, Baumann T, Kriegel C, et al. Advantage of combining magnetic cell separation with sperm preparation techniques. Reprod Biomed Online. 2005;10(6):740–6.
Delbes G, Herrero MB, Troeung ET, Chan PT. The use of complimentary assays to evaluate the enrichment of human sperm quality in asthenoteratozoospermic and teratozoospermic samples processed with Annexin-V magnetic activated cell sorting. Andrology. 2013;1(5):698–706. doi:10.1111/j.2047-2927.2013.00106.x.
Vendrell X, Ferrer M, Garcia-Mengual E, Munoz P, Trivino JC, Calatayud C, et al. Correlation between aneuploidy, apoptotic markers and DNA fragmentation in spermatozoa from normozoospermic patients. Reprod Biomed Online. 2014;28(4):492–502. doi:10.1016/j.rbmo.2013.12.001.
Gil M, Sar-Shalom V, Melendez Sivira Y, Carreras R, Checa MA. Sperm selection using magnetic activated cell sorting (MACS) in assisted reproduction: a systematic review and meta-analysis. J Assist Reprod Genet. 2013;30(4):479–85. doi:10.1007/s10815-013-9962-8.
Sheikhi A, Jalali M, Gholamian M, Jafarzadeh A, Jannati S, Mousavifar N. Elimination of apoptotic spermatozoa by magnetic-activated cell sorting improves the fertilization rate of couples treated with ICSI procedure. Androl. 2013;1(6):845–9. doi:10.1111/j.2047-2927.2013.00140.x.
Rawe VY, Boudri HU, Alvarez Sedo C, Carro M, Papier S, Nodar F. Healthy baby born after reduction of sperm DNA fragmentation using cell sorting before ICSI. Reprod Biomed Online. 2010;20(3):320–3. doi:10.1016/j.rbmo.2009.12.004.
Polakde Fried E, Denaday F. Single and twin ongoing pregnancies in two cases of previous ART failure after ICSI performed with sperm sorted using annexin V microbeads. Fertil Steril. 2010;94(1):351.e15–8. doi:10.1016/j.fertnstert.2009.12.037.
Herrero MB, Delbes G, Chung JT, Son WY, Holzer H, Buckett W, et al. Case report: the use of annexin V coupled with magnetic activated cell sorting in cryopreserved spermatozoa from a male cancer survivor: healthy twin newborns after two previous ICSI failures. J Assist Reprod Genet. 2013;30(11):1415–9. doi:10.1007/s10815-013-0086-y.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. NewJersey: Lawrence Erlbaum Associates; 1988.
Lee TH, Liu CH, Shih YT, Tsao HM, Huang CC, Chen HH, et al. Magnetic-activated cell sorting for sperm preparation reduces spermatozoa with apoptotic markers and improves the acrosome reaction in couples with unexplained infertility. Hum Reprod. 2010;25(4):839–46. doi:10.1093/humrep/deq009.
Said T, Agarwal A, Grunewald S, Rasch M, Baumann T, Kriegel C, et al. Selection of nonapoptotic spermatozoa as a new tool for enhancing assisted reproduction outcomes: an in vitro model. Biol Reprod. 2006;74(3):530–7. doi:10.1095/biolreprod.105.046607.
Tavalaee M, Deemeh MR, Arbabian M, Nasr-Esfahani MH. Density gradient centrifugation before or after magnetic-activated cell sorting: which technique is more useful for clinical sperm selection? J Assist Reprod Genet. 2012;29(1):31–8. doi:10.1007/s10815-011-9686-6.
Oehninger S, Acosta R, Morshedi M, Philput C, Swanson RJ, Acosta AA. Relationship between morphology and motion characteristics of human spermatozoa in semen and in the swim-up sperm fractions. J Androl. 1990;11(5):446–52. doi:10.1002/j.1939-4640.1990.tb00174.x.
Lachaud C, Tesarik J, Canadas ML, Mendoza C. Apoptosis and necrosis in human ejaculated spermatozoa. Hum Reprod. 2004;19(3):607–10. doi:10.1093/humrep/deh130.
de Vantery AC, Lucas H, Chardonnens D, de Agostini A. Removal of spermatozoa with externalized phosphatidylserine from sperm preparation in human assisted medical procreation: effects on viability, motility and mitochondrial membrane potential. Reprod Biol Endocrinol. 2009;7:1. doi:10.1186/1477-7827-7-1.
Zahedi A, Tavalaee M, Deemeh MR, Azadi L, Fazilati M, Nasr-Esfahani MH. Zeta potential vs apoptotic marker: which is more suitable for ICSI sperm selection? J Assist Reprod Genet. 2013;30(9):1181–6. doi:10.1007/s10815-013-0022-1.
Acknowledgments
We would like to acknowledge Ângela Alves, Technical assistant for teaching and research (ICBAS-UP) in laboratorial assistance, Claúdia Osório, Bsc, Biologist (CGR-ABarros) in spermiogram analysis assistance and Gabriela Rodrigues, PhD, Assistant Professor (University of Lisbon) for reviewing the manuscript.
Multidisciplinary Unit for Biomedical Research (UMIB) is funded by National Funds through FCT-Foundation for Science and Technology, under the Pest-OE/SAU/UI0215/2014.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Capsule Semen was processed with MACS and classic sperm preparation techniques. The highest reduction of sDNAfrag was obtained with MACS followed by DGC and SU and in asthenozoospermic patients. Sperm progressive motility, vitality and membrane integrity were negatively correlated with sDNAfrag.
Rights and permissions
About this article

Cite this article
Bucar, S., Gonçalves, A., Rocha, E. et al. DNA fragmentation in human sperm after magnetic-activated cell sorting. J Assist Reprod Genet 32, 147–154 (2015). https://doi.org/10.1007/s10815-014-0370-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-014-0370-5