
Abstract
Purpose
The HLA-G 14-bp insertion/deletion polymorphism had been inconsistently associated with recurrent miscarriage (RM) risk. We examined the association by performing a meta-analysis.
Methods
Eligible articles were searched in PubMed, EMBASE and CNKI without language limitation. We included all the articles about two or more miscarriages associated with HLA-G 14-bp polymorphism. The odds ratios (ORs) with 95 % confidence intervals (CIs) were used to assess the strength of associations. Statistical analyses were performed by the STATA10.0 software.
Results
17 studies were included, representing 1786 cases and 1574 controls. The current meta-analysis showed that 14-bp polymorphism was not associated with RM risk in all genetic models and allele contrast(+14 bp vs. −14 bp: OR = 1.13; 95 % CI, 0.96,1.32; +14 bp/+14 bp vs. −14 bp/−14 bp: OR = 1.16, 95 % CI, 0.85, 1.59; +14 bp/−14 bp vs. −14 bp/−14 bp: OR = 1.21, 95 % CI, 0.92,1.58; dominant model: OR = 1.33; 95 % CI, 0.99,1.78; recessive model: OR = 1.06; 95 % CI, 0.79,1.43). Moreover, a significant heterogeneity was evident across studies. On the other hand, the subgroup analysis demonstrated that there was a significant association between HLA-G 14-bp polymorphism and patients with three or more miscarriages(+14 bp vs. −14 bp: OR = 1.27; 95 % CI, 1.04, 1.55; dominant model: OR = 1.52; 95 % CI, 1.16, 1.99; and model +14 bp/−14 bp versus −14 bp/−14 bp: OR = 1.51; 95 % CI, 1.15, 1.97;).
Conclusions
Our comprehensive meta-analysis indicated that there was insufficient evidence to demonstrate a conclusive association between the HLA-G 14-bp insertion/deletion polymorphism and the risk of RM. But HLA-G 14-bp insertion/deletion polymorphic variation was associated with RM risk in patients with three or more miscarriages. Larger and well-designed studies may eventually provide a better, comprehensive understanding of the association between the HLA-G 14-bp insertion/deletion polymorphism and RM in the future.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Miscarriage is one of the most common complications of pregnancy, which afflicts healthy women. Recurrent miscarriage (RM) occured in 0.5–1 % of couples attempting to have children[1]. Controversy had existed on the number of miscarriages required to define RM. In 2011, the Green-top Guideline from the Royal College of Obstetricians and Gynaecologists stated that “recurrent miscarriage defined as the loss of three or more consecutive pregnancies”[2]. In contrast, the American Society for Reproductive Medicine (ASRM) in 2012 defined RM as “a distinct disorder defined by two or more failed clinical pregnancies”[3]. Jaslow et al. evaluated more than 1,000 women with RM, and their study found no difference in the frequency of abnormal diagnostic factors between women with two and those with three or more miscarriages, and argued that full evaluations should be offered to women who have experienced at least two consecutive pregnancy losses[4].
Identified causes such as uterine malformations, antiphospholipid antibodies, parental cytogenetic anomalies, endocrine disturbances, and infections accounted for only 20–50 % of RM[5]. Aetiologies for the remainder of RM women were the focus of intense research[6]. Immunological mechanisms had been proposed to explain at least some of these cases of ‘unexplained’ RM. Autoimmune and alloimmune factors may play major roles in the immunologic failure of pregnancy in women with RM[7].
The human conceptus was a semi-allograft and hence antigenically foreign to the mother. Therefore, the process of implantation may include mechanisms to prevent allograft rejection, but once the immunological tolerance becomed imbalanced, pathological pregnancy, such as RM, may occur[8].
An interesting molecule was human leucocyte antigen (HLA)-G that seemed to play a major role in immune suppression at the maternal-fetal interface and placental angiogenesis[9]. HLA-G mainly expressed in extravillous trophoblasts (EVTs)[10] of decidual tissue, and had suppressive effects on NK cells, CD4+ and CD8+ T cells, B lymphocytes and antigen presenting cells such as macrophages and dendritic cells[11]. This interaction was essential for the maternal-fetal immune balance needed for optimal trophoblast invasion during implantation and placentation. Soluble HLA-G levels were significantly lower in the RM cases compared to healthy controls[12]. Moreover, a recent meta-analysis indicated that sHLA-G in embryo culture supernatants was moderately helpful to predict the ability to achieve a pregnancy in women undergoing infertility treatment[13]. Although there have been some controversies, the overall picture emerging from a range of different studies published in recent years was that reduced or aberrant HLA-G expression seemed to be associated with certain complications of pregnancy, such as RM, implantation failure in IVF and preeclampsia, and that this may be further linked to HLA-G polymorphisms.
It had been suggested that HLA-G production was controlled by polymorphisms at the 5′ upstream regulatory region and at the 3′ UTR of the HLA-G gene[14]. A deletion/insertion (DEL/INS) of 14 base pairs (14 bp) polymorphism at the 3′ UTR was clearly implicated[15]. The presence of the 14 bp INS affected mRNA stability, protein production[16] and was associated with pregnancy pathologies and autoimmune diseases[17],[18]. HLA-G allele containing 14-bp sequence was associated with a significantly lower mRNA levels than that containing the 14-bp sequence deleted[19–21] and related with a lower HLA-G protein production[15],[22]. Therefore, HLA-G 14-bp polymorphism may play a crucial role in the modulation of HLA-G expression, and women with RM may have a higher frequency of individuals for the 14 bp insertion.
To date, several studies had focused on the specific role for the HLA-G 14 bp polymorphism in RM. But the results were controversial or inconclusive, partly because each study involved few cases and few controls and, therefore, there was not enough information to demonstrate such association. In a recent meta-analysis article of Wang et al.(2013), it was suggested that the 14 bp ins HLA-G allele was associated with increased risk of RM[23]. The studies of Hviid et al. 2004 and Christiansen et al. 2012 which were included in the meta-analysis of Wang et al.(2013) were from the same study group. When there were multiple publications from the same study group, the most informative and recent study was included for review[24]. Moreover, three studies of Akhter A et al. 2012[25], Kano T et al. 2007[26] and Liu YD et al. 2008[27] which reported the association of HLA-G 14-bp polymorphism and RM susceptibility did not be included in the meta-analysis article of Wang et al.,(2013) . Therefore it was necessary to reevaluate the association of HLA-G 14-bp polymorphism and RM susceptibility, by excluding the study of Hviid et al. 2004 and including the studies of Akhter A et al. 2012, Kano T et al. 2007 and Liu YD et al. 2008. In addition, the heterogeneity between studies and the existence of publication bias were explored.
Materials and methods
Selection of studies
A systemic search of the relevant literature was performed without language limitation. We explored PubMed, EMBASE, and China National Knowledge Infrastructure (CNKI) ((last search update 21th Oct 2012). The following keywords were included in the search strategy: (‘human leukocyte antigen’ or ‘HLA’) and (‘polymorphism’ or ‘genotype’ or ‘genetic’) and (‘recurrent spontaneous abortion’ (RSA) or ‘recurrent pregnancy loss’ (RPL) or ‘recurrent miscarriage’ (RM) or ‘recurrent fetal loss’ (RFL)). We included all the articles about two or more miscarriages associated with HLA-G 14-bp polymorphism. The titles and abstracts of publications were screened to identify their relevance. Any clearly irrelevant studies were excluded. The full texts of the remaining articles were read to determine whether they contained information on the topic of interest. Furthermore, literatures cited in the references sections of review articles and other relevant studies were searched manually to find additional eligible studies. A study was included in the analysis if: (i) it was a case–control study; (ii) it contained original data (independence among studies); and (iii) it provided enough data to calculate an odds ratio (OR). We excluded the following: (i) studies that contained overlapping data; (ii) studies in which the number of null and wild genotypes or alleles could not be ascertained; and (iii) studies in which family members had been studied because their analysis was based on linkage considerations.
Data extraction
From each study, the following information was abstracted: first author, year of publication, ethnicity of the study population, country, inclusion criteria for cases and controls, eligible subjects, the number of cases and controls for HLA-G 14-bp polymorphism genotypes and alleles, and P value of Hardy-Weinberg equilibrium (HWE) in control group. The bibliographic search and data extraction were conducted independently by 2 authors, and disagreements were resolved by consensus for all data. If there were incomplete data on allele and genotype frequency in studies, we tried to get these data by sending emails to the corresponding authors of these studies.
The quality of the included studies was assessed according to the following criteria from the previous meta-analysis[28]:
-
(1)
Description of the case and control groups (adequate, inadequate).
-
(2)
Assessment and validation of miscarriage in the patients (adequate, inadequate, not stated). Adequate validation would include confirmation by scan or pathological examination; inadequate validation would include recollection of the patient as the only evidence or a biochemical pregnancy without ultrasound evidence of pregnancy.
-
(3)
Description of the laboratory procedures for the genotyping (adequate, inadequate).
-
(4)
Elimination of confounding factors in patients (not described, inadequate, adequate). Adequate elimination refered to the exclusion of the proven causes of recurrent miscarriage (chromosomal abnormalities of the couples, uterine abnormalities, antiphospholipid antibodies, protein C/S and antithrombin-III deficiency).
-
(5)
Equal assessment for confounding factors in the case and control groups (equal, unequal, not stated).
Evaluation of statistical associations
The association between HLA-G 14-bp polymorphism and RM was estimated by calculating a pooled OR and 95 % CI under the co-dominant model, dominant model, recessive model and allelic contrast, respectively. In addition, heterogeneities were assessed by using Cochran’s Q-statistic and the I2 metric, which quantified between-study heterogeneity irrespective of the number of studies. The effect of heterogeneity was quantified by using I2, which ranged between 0 and 100 % and represented the proportion of between study variability attributable to heterogeneity rather than chance[29]. I2 values of 25 %, 50 %, and 75 % were nominally defined as low, moderate, and high estimates. In this study, we applied the random-effects model for all comparisons because this accommodated the possibility that the underlying effect differed across studies. For practical use, the random-effects model was more conservative and had a wider CI than that of the fixed-effects model[30].
Funnel plots were used to detect publication bias, but they required a range of studies of varying sizes and subjective judgments, and thus we evaluated publication bias using Begg’s rank correlation method and the Egger’s weighted regression method. To adjust for multiple comparisons, we applied the Bonferroni adjustment(Bon)[31].
Data analyses were performed by the Stata software (version 10). P < 0.05 considered representative of statistical significance.
Results
Studies included in the meta-analysis
The literature review identified 306 papers that met the search criteria. However, after screening the titles and abstracts, 281 studies were excluded secondarily as they were review articles or irrelevant to the current analysis. We retrieved the 25 remaining relevant manuscripts for detailed review. Among these, 4 studies were excluded due to duplicate publications[32–35], three had incomplete data on allele and genotype frequency which we failed to get by emails to the corresponding authors [36–38], and an additional one was excluded due to the absence of a control group[39]. Consequently, the remaining 17 case–control studies which examined the association between the HLA-G 14-bp polymorphism and RM were finally included[12, 17, 25–27, 40–51] (Fig. 1).

Flow diagram of the studies selection process
Study characteristics were summarized in Table 1. There were 12 studies analysing Asian patients and 5 studies analysing White patients. Studies had been carried out in China, India, Japan, USA, Poland, Brazil, Denmark and Iraq. The total number of subjects enrolled in the 17 studies was 3360, comprising 1786 patients and 1574 controls. All the 17 articles were published as full manuscripts. The HWE test that was performed in the control group of each study revealed that only one article violated the HWE, and two papers can not perform the HWE test because of incomplete data(Table 1). The distribution of the genotype in these studies and the inclusion criteria for cases and controls were listed in Table 1.
Association between RM and HLA-G 14-bp insertion/deletion polymorphism allele
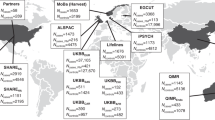
Sixteen studies were included in assessing the association between HLA-G 14-bp insertion/deletion polymorphism allele and RM[12, 17, 25–27, 40–50]. As shown in Fig. 2, compared with 14-bp deletion(−14 bp) allele, 14-bp insertion(+14) allele was not associated with RM risk(OR = 1.13; 95 % CI, 0.96,1.32, Pheterogeneity =0.01, I2 = 49.5 %).

Forest plots on association between HLA-G 14-bp insertion/deletion polymorphism and RSA risk. Results of individual and summary odds ratio (ORs) estimates, 95 % confidence intervals (CIs) and weight of each study are shown. a Allele contrast (+14 bp vs. -14 bp); b +14 bp/+14 bp vs. -14 bp/-14 bp; c +14 bp/-14 bp vs. -14 bp/-14 bp; d Dominant genetic model; e Recessive genetic model
Association between RM and HLA-G 14-bp insertion/deletion polymorphism genotype
Sixteen studies were included in assessing the association between HLA-G 14-bp insertion/deletion polymorphism genotype and RM[12, 17, 25–27, 40–43, 45–51]. As shown in Fig. 2, compared with the −14 bp/−14 bp genotype, the +14 bp/+14 bp and +14 bp/−14 bp genotypes were not associated with RM risk(+14 bp/+14 bp vs. −14 bp/−14 bp: OR = 1.16, 95 % CI, 0.85, 1.59, Pheterogeneity =0.13, I2 = 30.5 %; +14 bp/−14 bp vs. −14 bp/−14 bp: OR = 1.21, 95 % CI, 0.92,1.58, Pheterogeneity =0.02, I2 = 48.6 %). Similarly, no associations were found in the dominant and recessive models (dominant model: OR = 1.33; 95 % CI, 0.99,1.78, Pheterogeneity =0.001, I2 = 62 %; recessive model: OR = 1.06; 95 % CI, 0.79,1.43, Pheterogeneity =0.04, I2 = 42.1 %).
Sensitivity and subgroup analyses
We subsequently performed sensitivity and subgroup analyses to investigate the origin of this heterogeneity.
After removing seven studies which included a small number of cases (n < 50), no difference from overall meta-analysis was noted(data not shown). Moreover, exclusion of studies in which controls were not in HWE did not alter the results of the meta-analysis(Table 2).
Stratified analyses by country also detected no significant association(Table 2). Since there were only 17 studies included, it was difficult to stratify analysis by ethnicity for small number of studies. So we did not stratify analysis by ethnicity. However, limiting the analysis to the studies about three or more miscarriages, we observed a significantly increased risk in allele contrast(OR = 1.27; 95 % CI, 1.04, 1.55, p = 0.022, Bon = 0.01; Pheterogeneity =0.03, I2 = 50.3 %), dominant model(OR = 1.52; 95 % CI, 1.16, 1.99, p = 0.002, Bon = 0.01; Pheterogeneity =0.12, I2 = 36.3 %) and model +14 bp/−14 bp versus −14 bp/−14 bp (OR = 1.51; 95 % CI, 1.15, 1.97, p = 0.003, Bon = 0.01; Pheterogeneity =0.17, I2 = 29.5 %), although there was non-significantly increased RM risk in recessive model(OR = 1.15; 95 % CI, 0.80, 1.66; Pheterogeneity =0.05, I2 = 47.7 %) and model +14 bp/+14 bp versus −14 bp/−14 bp (OR = 1.45; 95 % CI, 0.99, 2.13; Pheterogeneity =0.13, I2 = 34.3 %). For model +14 bp/+14 bp versus −14 bp/−14 bp, if fixed-effects model was used considering the Pheterogeneity > 0.1, there was significantly increased odds ratio for RM risk(OR = 1.52; 95 % CI, 1.15, 2.01, p = 0.004, Bon = 0.01;).
Christiansen OB et al. reported that HLA-G polymorphism may be more relevant in secondary RM than in primary RM. So we limited the analysis to the primary and secondary RM. There were four studies[26, 27, 40, 46] assessing the association between HLA-G 14-bp polymorphism genotype and primary RM. No association of HLA-G 14-bp polymorphism and primary RM was found in all genetic models and allele contrast(Table 2). There was only one study[33] about the association between HLA-G 14-bp polymorphism and secondary RM, in which the frequency of HLA-G 14 bp ins homozygotes among patients with secondary RM was significantly higher than that of the controls.
Publication bias
Begg’s rank correlation method and Egger’s weighted regression method were performed to evaluate publication bias of the literatures on RM and HLA-G 14-bp polymorphism. The statistical results did not show publication bias(+14 bp versus −14 bp: Begg’s test P = 0.69, Egger’s test P = 0.76; +14 bp/+14 bp versus −14 bp/−14 bp: Begg’s test P = 0.92, Egger’s test P = 0.61; +14 bp/−14 bp versus −14 bp/−14 bp: Begg’s test P = 0.32, Egger’s test P = 0.49; dominant model: Begg’s test P = 0.22, Egger’s test P = 0.34; recessive model: Begg’s test P = 0.37, Egger’s test P = 0.29).
Discussion
This comprehensive meta-analysis indicated that there was not a significant association between the HLA-G 14-bp insertion/deletion polymorphism and the risk of RM . Moreover, a significant heterogeneity was evident across studies. On the other hand, there was a significant association between HLA-G 14-bp insertion/deletion polymorphism and patients with three or more miscarriages. Our meta-analysis results were different from the outcomes of the previous meta-analysis of Wang et al. 2013 [23]. After adding the study of Hviid et al. 2004 which was included in the meta-analysis of Wang et al. 2013 and deleting the studies of Akhter A et al. 2012, Kano T et al. 2007 and Liu YD et al. 2008 which were not included in the meta-analysis of Wang et al. 2013, the results of meta-analysis were the same as those of Wang et al. 2013(data not shown). Therefore, the difference may be resulted from that our meta-analysis included more eligible studies and excluded the duplicate publication.
Recent evidence indicated that HLA-G played an important role in the pathogenesis of RM. Although there were some controversies, the overall picture in recent years was that reduced or aberrant HLA-G expression was associated with RM[52]. Complications during pregnancy, such as pre-eclampsia, miscarriage, IUGR, and premature birth, were associated with a low or undetectable level of soluble HLA-G in the maternal blood circulation[53] . In the HLA-G gene, several polymorphisms had been identified, which might have a role in the pathogenesis of infertility and RM. 14-bp insertion polymorphism in the 3'UTR end (exon 8) of the HLA-G gene, expressed at a significantly lower level than the corresponding HLA-G mRNA isoform with the 14-bp sequence deleted, possibly providing an explanation for the increased frequency of 14-bp insertion in women with RM[20]. Theoretically, +14 bp/+14 bp may be association with reduced HLA-G expression, and consequently promoted development of RM. However, studies that have examined the association between the HLA-G 14-bp insertion/deletion polymorphism and RM showed inconsistent, even contradictory results. Thus a systematic meta-analysis of association between HLA-G 14-bp insertion/deletion polymorphism and RM risk was of great value. Our present meta-analysis demonstrated no conclusive association between the HLA-G 14-bp insertion/deletion polymorphism and the risk of RM, possibly due to the significant heterogeneity between different individual studies.
The risk of miscarriage increased progressively with the number of pregnancy losses. The risk of having a first miscarriage was estimated to be ~10 % of first pregnancies, while 24 % for the second, 26 % for the third and 32 % for the fourth [54]. We speculated that compared with normal women, women with more pregnancy losses may be more likely to have diverse gene loci, such as HLA-G 14-bp insertion/deletion polymorphism. Like our meta-analysis, in three or more miscarriages women HLA-G 14-bp polymorphism increased risk of RM, compared with controls. On the contrary, HLA-G 14-bp polymorphism did not increase risk of RM in all RM women including two miscarriages. We speculated that in most women with only two miscarriage there may be no maternal cause(especially the genetic cause) for the miscarriages, so including these women in the RM group may “dilute” the group with respect to cases caused by maternal factors. Our speculation was confirmed by the results of Zhu’s article, in which the + 14 bp allele frequency was highest in patients with four or more miscarriages, medium in those with two miscarriages, and lowest in fertile controls, although the differences did not reach the statistical significance[45].
In addition, the subgroup analysis also showed some other interesting results. Although there were no associations between HLA-G 14-bp polymorphism and primary RM in all genetic models and allele contrast, one study[33] reported the association between HLA-G 14-bp polymorphism and secondary RM, in which the frequency of HLA-G 14 bp ins homozygotes among patients with secondary RM was significantly higher than that of the controls. Secondary RM, in contrast to primary RM, was preceded by a pregnancy lasting to the last trimester. Secondary RM represented a poorly understood subgroup in which a distinction from primary RM was seldom made in the published literature or in clinical practice[55]. There were some observations to support the theory that immunological factors played a greater role in women with a series of miscarriages after a birth (secondary RM) than in women with RM who had never had a successful pregnancy (primary RM). The HLA-DR3 allele found to be associated with RM displayed a much stronger association to secondary than to primary RM[56], and some evidence from immunotherapy studies suggested that a possible therapeutic effect of intravenous immunoglobulin (IvIg) seemed to be restricted to women with secondary RM[57]. During pregnancy fetal cells entered the maternal circulation of the women with secondary RM[58] and in late pregnancy apoptotic syncytiotrophoblast debris is normally shed in large quantities (several grams per day) from the placenta[59]. SRM was hence preceded by a possible priming of the immune system of the mothers that may theoretically lead to harmful immunological reactions against the semi-allogeneic fetus. Many women with secondary RM had developed a harmful immunological reaction against male-specific antigens(HY-antigens) on the trophoblast, and that this results in a subsequent increased miscarriage rate of male conceptions[57]. HY-derived peptides may be presented to maternal immune cells by HLA-G molecules on the trophoblast[60]. Therefore HLA-G 14-bp insertion/deletion polymorphism may be associated with secondary RM by regulating the expression of HLA-G.
When between-study variation cannot be explained by chance, exploration of the reasons for heterogeneity emerged as the main goal of a meta-analysis. The heterogeneity test in our analysis showed that there were significant differences between individual studies. Therefore, sensitivity and subgroup analyses were performed to find out the underlying causes of heterogeneity.
Our sensitivity analysis showed that even after excluding studies with a small number of cases (n < 50), or having controls without HWE, the results of the meta-analysis did not change.
Alternatively, the subgroup analysis showed some interesting results. Although the country does not seem to have obvious influence on the statistical results and heterogeneity of our analysis, subjects with three or more miscarriages had a significant association between the HLA-G 14-bp insertion/deletion polymorphism and RM under allele contrast and co-dominant and dominant model, whereas heterogeneity still existed. Thus possible sources of heterogeneity, such as country, HWE in controls, study sample size and subtype of RM may be not causes of heterogeneity. It is possible that other limitations of recruited studies may partly contribute to the observed heterogeneity.
It was prudent to acknowledge that several potential limitations were apparent. First, the number of studies and the number of subjects in the studies included in the meta-analysis were small. It was critical that larger and well-designed studies based on different ethnicities should be performed to re-evaluate the association. Second, we did not receive a response from the corresponding authors of three studies[36–38] and therefore we did not acquire the data on genotyping frequency necessary for analysis. These articles were excluded from our meta-analysis. Third, only published studies were included in the meta-analysis and thus we cannot exclude the possibility of publication bias, although the results of statistical tests showed that publication bias was unlikely. Fourth, HLA-G expression both in the woman and the embryo/fetus may be important for pregnancy and its complications. It was also apparent that a gene with putative immunosuppressive and immune tolerant potential might be functional both in the mother and the embryo/fetus/placenta. In this regard, mother, placenta and fetus may form a synthesis. Therefore, future studies should address HLA-G 14-bp insertion/deletion polymorphism in both the couple and the fetus to re-evaluate the association. Fifth, The pooled estimates may also be influenced by gene–gene interactions. The overall lack of association between the polymorphisms and RM might be due to some other unidentified functional mutations that existed in the HLA-G gene, affecting the susceptibility to RM. It was suggested that HLA-G*01:04:01 showed a negative association with the 14 bp segment in RM patients and a positive association in controls[42], and the T allele of HLA-G T1570C was in linkage disequilibrium with the 14-bp deletion in cases of RM[46]. Therefore, the association between the HLA-G 14-bp insertion/deletion polymorphism and RM may be influenced by other loci. Sixth, the potential contribution of differences in patient populations (e.g. maternal age, influence of male and so on) might lead to different results on RM[61, 62]. Sometimes the association between polymorphisms and diseases may only be found in stratification analysis according to the clinical character. However in our article, this information cannot be gotten completely, we can not perform the stratification analysis according to the clinical character. Seventh, because there was only one study on the association of HLA-G 14-bp polymorphism in secondary RM and four studies in primary RM, more studies about the association of HLA-G 14-bp polymorphism in primary and secondary RM are needed to reevaluate the relationship between HLA-G polymorphism and susceptibility to primary and secondary RM.
In conclusion, our comprehensive meta-analysis indicated that there was insufficient evidence to demonstrate a conclusive association between the HLA-G 14-bp insertion/deletion polymorphism with the risk of RM, whereas a significant heterogeneity was evident across the individual studies. The subgroup analysis indicated that there was a significant association between HLA-G 14-bp insertion/deletion polymorphic variation and RM risk in patients with three or more miscarriages. Larger and well-designed studies estimating the effect of gene–gene interactions may eventually provide a better, comprehensive understanding of the association between the HLA-G 14-bp insertion/deletion polymorphism with RM.
References
Mishell Jr DR. Recurrent abortion. J Reprod Med. 1993;38:250–9.
Royal College of Obstetricians and Gynaecologists. The investigation and treatment of couples with recurrent first-trimester and second-trimester miscarriage. In: Green-top Guideline No17. London: Royal College of Obstetricians and Gynaecologists; 2011.
American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98:1103–11.
Jaslow CR, Carney JL, Kutteh WH. Diagnostic factors identified in 1020 women with two versus three or more recurrent pregnancy losses. Fertil Steril. 2010;93:1234–43.
Stephenson M. Frequency of factors associated with habitual abortion in 197 couples. Fertil Steril. 1996;66:24–9.
Ren AG, Wang J. Methylenetetrahydrofolate reductase C677T polymorphism and the risk of unexplained recurrent pregnancy loss: A meta-analysis. Fertil Steril. 2006;86:1716–22.
Pandey MK, Rani R, Agrawal S. An update in recurrent spontaneous abortion. Arch Gynecol Obstet. 2005;272(2):95–108.
Trowsdale J, Betz AG. Mother’s little helpers: mechanisms of maternal–fetal tolerance. Nat Immunol. 2006;7:241–6.
Kovats S, Main EK, Librach C, Stubblebine M, Fisher SJ, DeMars R. A class I antigen HLA-G, expressed in human trophoblasts. Science. 1990;248:220–3.
Goldman-Wohl DS, Ariel I, Greenfield C, Hochner-Celnikier D, Cross J, Fisher S, et al. Lack of human leukocyte antigen-G expression in extravillous trophoblasts is associated with pre-eclampsia. Mol Hum Reprod. 2000;6:88–95.
Hunt JS, Morales PJ, Pace JL, Fazleabas AT, Langat DK. A commentary on gestational programming and functions of HLA-G in pregnancy. Placenta. 2007;21:S57–63.
Jassem RM, Shani WS, Loisel DA, Sharief M, Billstrand C, Ober C. HLA-G polymorphisms and soluble HLA-G protein levels in women with recurrent pregnancy loss from Basrah province in Iraq. Hum Immunol. 2012;73:811–7.
Vercammen MJ, Verloes A, Van de Velde H, Haentjens P. Accuracy of soluble human leukocyte antigen-G for predicting pregnancy among women undergoing infertility treatment: meta-analysis. Hum Reprod Update. 2008;14:209–18.
Consiglio CR, Veit TD, Monticielo OA, Mucenic T, Xavier RM, Brenol JC, et al. Association of the HLA-G gene +3142C > G polymorphism with systemic lupus erythematosus. Tissue Antigens. 2011;77:540–5.
Hviid TV, Rizzo R, Christiansen OB, Melchiorri L, Lindhard A, Baricordi OR. HLA-G and IL-10 in plasma in relation to HLA-G genotype and polymorphisms. Immunogenetics. 2004;56:135–41.
Tan V, Randall G, Fan V, Camoretti-Mercado B, Brockman-Schneider R, Pan L, et al. Allele-specific targeting of microRNAs to HLA-G and risk of asthma. Am J Hum Genet. 2007;81:829–34.
Yan WH, Lin V, Chen XJ, Dai MZ, Gan LH, Zhou MY, et al. Association of the maternal 14-bp insertion polymorphism in the HLA-G gene in women with recurrent spontaneous abortions. Tissue Antigens. 2006;68:521–3.
Hviid TV, Christiansen OB. Linkage disequilibrium between human leukocyte antigen (HLA) class II and HLA-G - possible implications for human reproduction and autoimmune disease. Hum Immunol. 2005;66:688–99.
Hiby SE, King A, Sharkey A, Loke YW. Molecular studies of trophoblast HLA-G: polymorphism, isoforms, imprinting and expression in preimplantation embryo. Tissue Antigens. 1999;53:1–13.
Hviid TV, Hylenius S, Rorbye C, Nielsen LG. HLA-G allelic variants are associated with differences in the HLA-G mRNA isoform profile and HLA-G mRNA levels. Immunogenetics. 2003;55:63–79.
Rousseau P, Le Discorde M, Mouillot G, Marcou C, Carosella ED, Moreau P. The 14 bp deletion-insertion polymorphism in the 3′ UT region of the HLA-G gene influences HLA-G mRNA stability. Hum Immunol. 2003;64:1005–10.
Rizzo R, Hviid TV, Stignani M, Balboni A, Grappa MT, Melchiorri L, et al. The HLA-G genotype is associated with IL-10 levels in activated PBMCs. Immunogenetics. 2005;57:172–81.
Wang X, Jiang W, Zhang D. Association of 14-bp insertion/deletion polymorphism of HLA-G gene with unexplained recurrent spontaneous abortion: a meta-analysis. Tissue Antigens. 2013;81:108–15.
Gong M, Long J, Liu Q, Deng HC. Association of the ADIPOQ rs17360539 and rs266729 polymorphisms with type 2 diabetes: a meta-analysis. Mol Cell Endocrinol. 2010;325:78–83.
Akhter A, Faridi RM, Das V, Pandey A, Naik S, Agrawal S. In vitro up-regulation of HLA-G using dexamethasone and hydrocortisone in first-trimester trophoblast cells of women experiencing recurrent miscarriage. Tissue Antigens. 2012;80:126–35.
Kano T, Mori T, Furudono M, Ishikawa H, Watanabe H, Kikkawa E, et al. Human leukocyte antigen may predict outcome of primary recurrent spontaneous abortion treated with paternal lymphocyte alloimmunization therapy. Am J Reprod Immunol. 2007;58:383–7.
Liu YD, Shao JC, Wang ZM, Jing YM, Hu DC. Relationship of polymorphism of HLA-G 14 bp and RSA in the Kunmin. China Healthc Front. 2008;3:4–5.
Su MT, Lin SH, Chen YC. Genetic association studies of angiogenesis- and vasoconstriction-related genes in women with recurrent pregnancy loss: a systematic review and meta-analysis. Hum Reprod Update. 2011;17:803–12.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58.
Wenquan N, Yue Q, Pingjin G, Dingliang Z. Association between angiotensin converting enzyme G2350A polymorphism and hypertension risk: a meta-analysis. J Renin-Angiotensin-Aldosterone Syst. 2011;12:8–14.
Wu XY, Lu JJ, Zhang JX, Li H. The Bonferroni Method for Multiple Comparisons. J Evidence-Based Med. 2006;6:361–3. 374.
Xue SG, Yang JQ, Yao FJ, Xu LD, Fan LA. Study on the polymorphism of the 14 bp deletion of HLA-G allele in patients with recurrent spontaneous abortion of unknown origin and normal deliveries. Curr Immunol. 2006;26:318–21.
Li CQ, Zhang X, Bao WG, Ling AF, Yan WH. Association of the maternal 14-bp insertion polymorphism in the HLA-G gene in women with recurrent spontaneous abortions. Zhejiang Pract Med. 2009;14:449–50.
Hviid TV, Hylenius S, Lindhard A, Christiansen OB. Association between human leukocyte antigen-G genotype and success of in vitro fertilization and pregnancy outcome. Tissue Antigens. 2004;64:66–9.
Hviid TV, Hylenius S, Hoegh AM, Kruse C, Christiansen OB. HLA-G polymorphisms in couples with recurrent spontaneous abortions. Tissue Antigens. 2002;60:122–32.
Sosnina KO, Zastavna DV, Terpylyak OI. The role of HLA-G 14 base pairs insertion/deletion polymorphism in the genesis of human early reproductive losses. Tissue Antigens. 2012;80:83.
Larsen MH, Dahl M, Pass MB, Hviid TV, Christiansen OB, Bzorek M, et al. The non-classical human leukocyte antigen (HLA)-G in human reproduction and complications of pregnancy. Tissue Antigens. 2010;75:543–4.
Da Graca BM, Dos Santos SJ. Sarturi P; HLA-G 14 bp/del genotypes in Brazilian couples with recurrent spontaneous abortions. Tissue Antigens. 2009;74:91–2.
Kolte AM, Steffensen R, Nielsen HS, Hviid TV, Christiansen OB. Study of the structure and impact of human leukocyte antigen (HLA)-G-A, HLA-G-B, and HLA-G-DRB1 haplotypes in families with recurrent miscarriage. Hum Immunol. 2010;71:482–8.
Christiansen OB, Kolte AM, Dahl M, Larsen EC, Steffensen R, Nielsen HS, et al. Maternal homozygocity for a 14 base pair insertion in exon 8 of the HLA-G gene and carriage of HLA class II alleles restricting HY immunity predispose to unexplained secondary recurrent miscarriage and low birth weight in children born to these patients. Hum Immunol. 2012;73:699–705.
Shankarkumar U, Shankarkumar A, Chedda Z, Ghosh K. Role of 14-bp deletion/insertion polymorphism in exon 8 of the HLA-G gene in recurrent spontaneous abortion patients. J Hum Reprod Sci. 2011;4:143–6.
Vargas RG, Sarturi PR, Mattar SB, Bompeixe EP, Silva Jdos S, Pirri A, et al. Association of HLA-G alleles and 3′ UTR 14 bp haplotypes with recurrent miscarriage in Brazilian couples. Hum Immunol. 2011;72:479–85.
Aruna M, Sirisha PV, Andal Bhaskar S, Tarakeswari S, Thangaraj K, Reddy BM. Role of 14-bp insertion/deletion polymorphism in HLA-G among Indian women with recurrent spontaneous abortions. Tissue Antigens. 2011;77:131–5.
Berger DS, Hogge WA, Barmada MM, Ferrell RE. Comprehensive analysis of HLA-G: implications for recurrent spontaneous abortion. Reprod Sci. 2010;17:331–8.
Zhu Y, Huo Z, Lai J, Li S, Jiao H, Dang J, et al. Case–control study of a HLA-G 14-bp insertion-deletion polymorphism in women with recurrent miscarriages. Scand J Immunol. 2010;71:52–4.
Suryanarayana V, Rao L, Kanakavalli M, Padmalatha V, Raseswari T, Deenadayal M, et al. Association between novel HLA-G genotypes and risk of recurrent miscarriages: a case–control study in a South Indian population. Reprod Sci. 2008;15:817–24.
Sipak-Szmigiel O, Cybulski C, Lubiński J, Ronin-Walknowska E. HLA-G polymorphism in a Polish population and reproductive failure. Tissue Antigens. 2008;71:67–71.
Xue S, Yang J, Yao F, Xu L, Fan L. Recurrent spontaneous abortions patients have more −14 bp/+14 bp heterozygotes in the 3′UT region of the HLA-G gene in a Chinese Han population. Tissue Antigens. 2007;69:153–5.
Tripathi P, Abbas A, Naik S, Agrawal S. Role of 14-bp deletion in the HLA-G gene in the maintenance of pregnancy. Tissue Antigens. 2004;64:706–10.
Shao JC, Hu DC, Chen J, Liu YD, Wang ZM. Relationship of polymorphism of HLA-G 14 bp and the expression of HLA-G mRNA with unexplained recurrent spontaneous abortion. J Pract Obstet Gynecol. 2011;27:698–701.
Zhao YM, ZhenG ML, Zhang GL, Zhang YL, Hua AL, He JM. Related study between Serum levels of sHLA-G, HLA-G14bp insertion/deletion polymorphism and recurrent spontaneous abortion. Shanxi Med J. 2009;38:390–1.
Cecati M, Giannubilo SR, Emanuelli M, Tranquilli AL, Saccucci F. HLA-G and pregnancy adverse outcomes. Med Hypotheses. 2011;76:782–4.
Rizzo R, Andersen AS, Lassen MR, Sorensen HC, Bergholt T, Larsen MH, et al. Soluble human leukocyte antigen-G isoforms in maternal plasma in early and late pregnancy. Am J Reprod Immunol. 2009;62:320–38.
Hill JA, Anderson DJ. Immunological mechanisms in recurrent spontaneous abortion. Arch Immunol Ther Exp. 1990;38:111–9.
Rai R, Regan L. Recurrent miscarriage. Lancet. 2006;368:601–11.
Kruse C, Steffensen R, Varming K, Christianen OB. A study of HLA-DR and -DQ alleles in 588 patients and 562 controls confirms that HLA-DRB1*03 is associated with recurrent miscarriage. Hum Reprod. 2004;19:1215–21.
Christiansen OB, Pedersen B, Rosgaard A, Husth M. (2002) A randomized, double-blind, placebo-controlled trial of intravenous immunoglobulin in the prevention of recurrent miscarriage: evidence for a therapeutic effect in women with secondary recurrent miscarriage. Hum Reprod. 2002;17:809–16.
Adams KM, Nelson JL. Microchimerism: an investigative frontier in autoimmunity and transplantation. J Am Med Assoc. 2004;291:1127–31.
Huppertz B, Kaufmann P, Kingdom J. Trophoblast turnover in health and disease. Fetal Matern Med Rev. 2002;13:103–18.
Christiansen OB, Pedersen B, Nielsen HS, Nybo Andersen AM. Impact of the sex of first child on the prognosis in secondary recurrent miscarriage. Hum Reprod. 2004;19(12):2946–51.
Bulletti C, Flamigni C, Giacomucci E. Reproductive failure due to spontaneous abortion and recurrent miscarriage. Hum Reprod Update. 1996;2:118–36.
Sbracia M, Cozza G, Grasso JA, Mastrone M, Scarpellini F. Semen parameters and sperm morphology in men in unexplained recurrent spontaneous abortion, before and during a 3 year follow-up period. Hum Reprod. 1996;11:117–20.
Author information
Authors and Affiliations
Corresponding author
Additional information
Capsule The comprehensive meta-analysis indicated that there was insufficient evidence to demonstrate a conclusive association between the HLA-G 14-bp insertion/deletion polymorphism and the risk of RM. But HLA-G 14-bp insertion/deletion polymorphic variation was associated with RM risk in patients with three or more miscarriages.
Rights and permissions
About this article
Cite this article
Fan, W., Li, S., Huang, Z. et al. Relationship between HLA-G polymorphism and susceptibility to recurrent miscarriage: A meta-analysis of non-family-based studies. J Assist Reprod Genet 31, 173–184 (2014). https://doi.org/10.1007/s10815-013-0155-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-013-0155-2