
Abstract
Purpose: The aim was to establish the impact of human granulosa cell apoptosis and reactive oxygen species (ROS) production on fertilization competence of the oocyte, embryo developmental stage and implantation rate.
Methods: Thirty women undergoing IVF-ET for tubal factor infertility were included; GnRH antagonists and gonadotrophins were used for ovarian stimulation. Granulosa cells were isolated from each aspirated follicle using gradient centrifugation. Apoptosis was studied by flow cytometry using annexin V and propidium iodide. ROS production was studied with hydroethidine staining and analyzed by flow cytometry.
Results: There were no differences in characteristics of granulosa cells between the follicles with fertilized and non-fertilized oocytes. The analyzed characteristics of granulosa cells in corresponding follicles had no effect on embryo developmental stage on day 5. The percentage of ROS producing granulosa cells was lower in the follicles giving rise to blastocysts that resulted in implantation compared to those that did not (39.9% versus 69.9%, P = 0.031).
Conclusions: Apoptosis and ROS production in granulosa cells have no significant impact on fertilization and do not correlate with the development of blastocysts. An increased percentage of ROS producing granulosa cells results in fewer oocytes retrieved and diminishes implantation rate.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Programmed cell death or apoptosis is an ongoing process in all stages of ovarian and follicular development. It is responsible for depletion of ovarian germ cells in embryonic and fetal development; it initiates follicular atresia during reproductive life and is also responsible for degeneration of the corpus luteum [1].
In vitro fertilization and assisted reproduction techniques have made the analysis of folliculogenesis more accessible. Granulosa cells are essential in normal follicular maturation process since they produce steroidal hormones and growth factors, and they play a crucial role in follicular atresia [2]. Apoptosis of granulosa cells seems to have a negative effect on conception and pregnancy rates in an in vitro fertilization and embryo transfer (IVF-ET) programme [3, 4]. A higher incidence of apoptotic granulosa cells has been associated with a higher incidence of empty follicles, fewer oocytes retrieved and poorer quality of oocytes and embryos [3]. Furthermore, different ovarian stimulation protocols affect the incidence of apoptotic granulosa cells differently [5].
The role of reactive oxygen species (ROS) in gynecological diseases and assisted reproduction has been widely studied in recent years [6–11]. Low ROS concentrations in the follicular fluid have been proposed to be important for successful IVF outcome [12]. It seems that increased ROS levels impair oocyte and embryo quality [13, 14].
The aim of this study was to establish the effect of granulosa cell apoptosis and ROS production in granulosa cells on fertilization competence of the oocyte, development of human embryo to the blastocyst stage, and on the implantation rate.
Materials and methods
The study was carried out between February and October 2005 at the Reproductive Unit of the Department of Obstetrics and Gynecology, University Medical Centre Ljubljana. We enrolled 30 normally cycling women undergoing an IVF-ET programme for tubal factor infertility; the women with endometriosis or endocrine diseases and those with male factor infertility were excluded. Twelve women (40%) were in their first IVF cycle, the remaining ones were in their second or third IVF cycle. Each included woman gave written informed consent prior to enrolment. The study design was approved by the national medical ethics committee. The women were stimulated with the GnRH antagonists and gonadotrophins. They were given 3 ampoules (225 IU) of gonadotrophin folitrophin alpha (Gonal F; Industria Farmaceutica Serono S.p.A, Bari, Italy) from the day 2 of the cycle on. When the dominant follicle measured 14 mm in diameter, 3 mg of GnRH antagonist cetrorelix acetate (Cetrotide; Asta Medica AG, Frankfurt, Germany) was given. When at least three follicles measured ≥18 mm and the serum estradiol level was ≥0.40 nmol/l per follicle, 5000 IU of HCG> (Pregnyl; N.V. Organon, Oss, The Netherlands) was administered. Ultrasound-guided transvaginal oocyte retrieval was carried out 34–36 h after HCG administration.
Oocyte retrieval was done after the injection of local anesthetic. Follicular fluid was aspirated separately from each follicle. We used aspiration needle set TIK (TIK d.d., Kobarid, Slovenia). This set has 1.5 ml of residual fluid, as described previously [15]. To overcome the problem of mixing follicular aspirates, the residual volume was captured to another tube (marked at 1.5 ml) immediately after entering the next follicle. The residual volume was then added to the follicular fluid of the previously aspirated follicle. After removal of the oocytes, we measured the amount of follicular fluid from each aspirate that contained an oocyte and collected 1 ml of follicular fluid in a separate tube for isolation of granulosa cells. We pooled follicular fluids from follicles without an oocyte and again collected 1 ml of follicular fluid for isolation of granulosa cells. Follicular fluids that were contaminated with blood were excluded from the analysis.
Each oocyte was cultured individually in Universal IVF medium (Medi-Cult, Jyllinge, Denmark) and inseminated 2 h after oocyte retrieval. Fertilization results were assessed after 18 h. Embryos were cultured to the blastocyst stage in sequential media (Blast Assist System; MediCult, Jyllinge, Denmark). On day 5 embryonic developmental stage was evaluated (≤10-cell embryo, morula, blastocyst) and a maximum of two blastocysts were transferred; supernumerary blastocysts were cryopreserved; supernumerary embryos of lower developmental stages were discarded. Implantation was assessed 14 days after embryo transfer using serum β-HCG measurement. When two embryos were transferred, we considered both corresponding follicles to contribute to implantation, therefore both were considered in the analysis.
Immediately after removal of the oocyte, follicular fluids were centrifuged at 500 g for 10 min. The pelleted cells were resuspended in 1 ml of Universal IVF medium (MediCult, Jyllinge, Denmark). The suspension was carefully overlaid on 50% gradient, made of 1 ml of Universal IVF medium and 1 ml of filtrated PureSperm 100 (NidaCon International AB, Mölndal, Sweden), and centrifuged at 400 g for 25 min. Granulosa cells were collected from the interface.
Flow cytometry samples were prepared by incubating the granulosa cell layer with CD45 antibodies (Becton Dickinson Pharmingen, San Diego, CA, USA); granulosa cells were identified as highly granular CD45 negative cells.
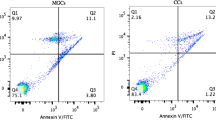
Apoptotic granulosa cells were detected using an early phenomenon of the apoptotic process. Prior to nuclear condensation and fragmentation apoptotic cells lose the asymmetry of their cellular membranes. Disruption of the membrane asymmetry with surface exposure of phosphatidylserine (PS) was detected with fluorescein isothiocyanate conjugated annexin V (AnV-FITC; Becton Dickinson Pharmingen, San Diego, CA, USA). The granulosa cells suspensions were diluted to approximately 1 × 106 cells/ml in RPMI medium (SIGMA-ALDRICH CO., St. Louis, USA) and labelled with 5 μl of AnV-FITC. The samples were stained simultaneously with 1 μg/ml of propidium iodide (PI) (Molecular Probes Inc., Eugene, OR, USA) to discriminate between live and dead cells. The samples were incubated in the dark for 15 min at 18°C, and then analyzed on a FACSCalibur flow cytometer (Becton Dickinson, San Josè, CA, USA). The analysis was set to maximum of 10 000 cells counted per sample. AnV-FITC fluorescence was detected using a 505–545 nm filter (FL1) and PI fluorescence was detected using a 605–635 nm filter (FL2). A cytogram of AnV-FITC fluorescence versus PI fluorescence was used to determine the AnV-FITC negative and positive cells in the live (PI-negative) population, expressed as percentages of the total population collected. According to their reactivity to annexin V and PI, cells were classified as apoptotic (positive annexin V and negative PI), necrotic (positive annexin V and positive PI) or normal (negative annexin V and PI). Unstained samples were used as negative fluorescence controls.
The production of a common member of ROS family, namely superoxide anion radical (O2 −) was measured with hydroethidine (HE). The procedure was modified from the methods previously described by Rothe and Valet [16]. HE was dissolved in N,N-dimethylformamide at a concentration of 22 mM, and stored at 8°C. Before assay, 2 μl of stock solution was dissolved in phosphate-buffered saline (PBS) to obtain working solutions at 44.4 μmol/l HE. Phorbol 12-myristate 13-acetate (PMA) was used to activate cells. It was made into a 10 mmol/l stock solution by dissolving 1 mg PMA in 1.6 ml DMSO. This was stored in 10 μl aliquots at −20°C. Cells (1 × 106/ml) were preincubated for 15 min at 37°C with HE (10 μmol/l) with continuous shaking. Cell suspensions were then split into two different aliquots containing either non-stimulated or PMA-stimulated (320 μmol/l for 15 min at 37°C) cells. Analyses were carried out on a FACSCalibur flow cytometer (Becton Dickinson, San Josè, CA, USA) equipped with an air-cooled Argon (Ar) ion laser. The fluorescence of cells was recorded under 488 nm excitation. Red fluorescences from ethidine were measured in the FL2 channel through a 586-nm band-pass filter. ROS production was quantified by mean DCFH fluorescence intensities and then expressed as percentages of ROS producing granulosa cells. We computed the capability of granulosa cells to produce oxidative bursts by dividing the percentage of ROS producing granulosa cells after PMA stimulation with the percentage of granulosa cells producing ROS in basic conditions.
Statistical analysis was performed using statistical package SPSS 13.0 for Windows (SPSS, Inc., Chicago, IL, USA). We computed the percentages of apoptotic, necrotic, normal granulosa cells and granulosa cells that produce ROS in relation to the presence or absence of an oocyte in the corresponding follicle, to fertilization, to embryo development and to implantation. Logistic regression analysis was used to determine the effect of apoptosis and ROS production in granulosa cells on the presence or absence of an oocyte, fertilization competence of the oocyte, embryo development and implantation. Linear regression was used for computing the relationship between ROS production and apoptosis. Differences were considered significant when P were <0.05.
Results
We studied 161 follicles from 30 women undergoing IVF-ET. The mean women’s age was 33.4 ± 4.0 years. The mean body mass index was 23.3 ± 4.3 kg/m2. The mean serum FSH level on cycle day 3 was 5.6 ± 1.8 IU/L. We retrieved mean 6.4 ± 4.2 oocytes per woman.
The average number of granulosa cells counted by flow cytometry was 879 (95% confidence interval (CI) = 783 to 976) and ranged from 86 to 3158 granulosa cells. The mean percentage of apoptotic granulosa cells was 36.2% (95% CI = 31.9 to 40.5%). The mean percentage of ROS producing granulosa cells was 64.1% (95% CI = 59.6 to 68.6%). The mean percentage of granulosa cells that produced ROS after stimulation with PMA was 58.5% (95% CI = 54.9 to 63.0%). In 27% (n = 43) of follicles, granulosa cells were capable to produce an oxidative burst.
From the 161 analyzed follicles we retrieved 131 (81.4%) oocytes; 63.4% (83/131) of oocytes fertilized. Altogether, we obtained 76 (91.6%) embryos of which 37 (48.7%) reached the blastocyst stage on day 5.
The percentages of apoptotic, necrotic, normal and ROS producing granulosa cells in relation to the presence or absence of an oocyte in the corresponding follicle are shown in Table 1. The logistic regression analysis revealed a statistically significant difference (P = 0.016) only in the percentage of ROS producing granulosa cells.
The mean percentages of apoptotic granulosa cells in follicles with fertilized oocytes and in those with non-fertilized oocytes were 32.3% (95% CI = 31.8 to 47.3%) and 39.6% (95% CI = 26.3 to 38.4%), respectively. The mean percentages of necrotic granulosa cells in follicles with fertilized oocytes and in those with non-fertilized oocytes were 22.8% (95% CI = 18.2 to 26.9%) and 17.9% (95% CI = 13.1 to 23.8%), respectively. The mean percentage of normal granulosa cells in follicles with fertilized oocytes and in those with non-fertilized oocytes were 44.8% (95% CI = 38.1 to 51.5%) and 42.5% (95% CI = 34.3 to 50.6%), respectively. The mean percentages of ROS producing granulosa cells in follicles with fertilized and in those with non-fertilized oocytes were 59.1% (95% CI = 52.6 to 65.6%) and 64.7% (95% CI = 56.5 to 72.7%), respectively. We observed no statistically significant differences between the characteristics of granulosa cells from the follicles with fertilized and those with non-fertilized oocytes.
The percentages of apoptotic, necrotic granulosa cells and granulosa cells that produce ROS in basic conditions in relation to embryo developed from the oocyte of the corresponding follicle are shown in Table 2. The analysis revealed higher percentages of necrotic and ROS producing granulosa cells in abnormal fertilization group(1 pronucleus in day 1 oocyte or 3 pronuclei in day 1 zygote) compared to normally cleaving embryos on day 3 (P = 0.039 for necrotic cells; P = 0.016 for ROS producing cells), but there was no difference in the characteristics of granulosa cells among normally fertilized zygotes regardless of later embryo development. When we used logistic regression analysis adjusted for all characteristics of granulosa cells and also for women’s age and BMI, these differences were no longer statistically significant.
The percentages of apoptotic, necrotic and ROS producing granulosa cells in relation to implantation, assessed by serum β HCG measurement, are shown in Table 3. We analyzed only those follicles with an oocyte that developed to blastocyst, which was transferred: 32 blastocysts were transferred. In 10 women there were two blastocysts transferred and in these cases the two corresponding follicles were considered in the analysis. In 9 of the 22 women with transferred blastocysts, implantation was detected by serum β-HCG measurement; in two (22.2%) women with positive serum β-HCG two blastocysts were transferred. Logistic regression analysis, additionally adjusted for age and BMI, revealed a correlation between the percentage of ROS producing granulosa cells and implantation; the percentage of ROS producing granulosa cells was lower in the follicles giving rise to blastocysts that resulted in implantation compared to the follicles giving rise to blastocysts that did not (P = 0.031). There were 3 spontaneous miscarriages, whereas 6 pregnancies are ongoing. In the subgroup with spontaneous miscarriages the percentages of apoptotic and ROS producing granulosa cells were 38.0% (95% CI = −72.6 to 148.6%) and 59.7% (95% CI = −63.5 to 182.8%) respectively; while in the subgroup with ongoing pregnancies those percentages were 16.9% (95% CI = −0.2 to 33.9%) and 38.1% (95% CI = 10.7 to 65.6%) respectively. The percentages of apoptotic and ROS producing granulosa cells did not differ significantly between these two subgroups.
Furthermore, we computed the average percentage of apoptotic, necrotic and ROS producing granulosa cells retrieved from follicles that led to implantation assessed by serum β HCG measurement and those that did not. There were no differences between these subgroups of follicles regarding the average characteristics of granulosa cells.
The percentage of ROS producing granulosa cells after stimulation with PMA did not correlate with the presence or absence of an oocyte, fertilization competence, and embryo developmental stage or implantation rate.
Finally, using linear regression analysis we found a relationship between ROS production and apoptosis of granulosa cells; if 1% more ROS producing granulosa cells were present in the follicle, the percentage of apoptotic granulosa cells rose for 0.6% (P = 0.000).
Discussion
The impact of granulosa cells apoptosis on the IVF outcome has already been studied extensively. GnRH agonists have been reported to induce apoptosis in granulosa cells [5]. Other known apoptosis inductive agents are androgens and GnRH [17, 18]. On the other hand, the agents that have antiatretogenic effects are estrogens, FSH, LH and HCG [17, 19]. The women in our study were stimulated with recombinant FSH that is supposed to posses an antiatretogenic effect and GnRH antagonists. The mean percentage of apoptotic granulosa cells in our series was 36.2%. In one study that used annexin V for the measurement of apoptosis, the mean percentage of apoptotic granulosa cells in women stimulated with recombinant FSH and GnRH agonists was reported to be 3.3% [20]. Based on these percentages it seems that GnRH antagonists have an inductive effect on apoptosis of granulosa cells, which appears to be even stronger than that of GnRH agonists. In a recently published study the authors have found comparable percentages of apoptotic granulosa cells in women stimulated with GnRH agonists or GnRH antagonists; they used annexin V as we did in our study, but in pooled follicular fluids from 32 women [21].
We deliberately included only normally cycling women with tubal factor infertility, because women with endometriosis were reported to have higher levels of apoptosis and oxidative stress in granulosa cells when compared to women with male factor of infertility [22].
Follicles with an oocyte showed a tendency to a decreased percentage of apoptotic granulosa cells compared to follicles without an oocyte, although the difference was not statistically significant. In some studies a significantly lower incidence of apoptosis in follicles with an oocyte compared to empty ones was reported; the fertilization rate was higher in oocytes originating from the follicles with less apoptosis [3, 23, 24]. However, we did not observe a significant difference in the percentage of apoptotic granulosa cells between the follicles with a fertilized and those with a non-fertilized corresponding oocyte. We thought that the discrepancy between our results and those of previous studies was due to the fact that we observed the early phenomenon of apoptosis, whereas other authors used DNA fragmentation measurement and thus captured apoptosis in its later stages.
Bearing this discrepancy in mind, we additionally compared the percentages of necrotic and normal granulosa cells in follicles with fertilized and non-fertilized oocytes. Again, we observed no difference. Therefore, we compared our results with those obtained by Clavero et al., the only study using annexin V for apoptosis assessment; they found similar percentages of apoptotic granulosa cells in follicular fluids from which fertilized oocytes were obtained and those with oocytes that were not fertilized–but after intracytoplasmic sperm injection, though [20]. In a recent report the authors did not find a correlation between apoptosis of cumulus cells and the fertilization rate [25]. This is consistent with our results, although they measured apoptosis using a different method (TUNEL) and counted apoptotic bodies in cumulus cells, not in follicular granulosa cells, as we did.
It has been suggested that apoptosis observed in cumulus cells has a more accurate and reliable impact on oocyte and embryo quality than apoptosis observed in follicular granulosa cells [25]. We analyzed apoptosis in granulosa cells obtained from the follicular fluid after removal of the oocyte, because we included couples with pure female infertility factor undergoing conventional IVF. Denudation of the oocyte is not used in conventional IVF; therefore cumulus granulosa cells could not be obtained. We chose to enrol couples undergoing conventional IVF rather than ICSI, because male factor infertility might have an effect on embryo development [26, 27].
At our Department embryos are cultured for 5 days, therefore we were able to assess the impact of granulosa cells apoptosis on the development of embryo to the blastocyst stage. Apoptosis of granulosa cells was not significantly different in the follicles that gave rise to blastocysts compared to the follicles with oocytes yielding morulae or ≤10-cell embryos. This is inconsistent with the only study, to our knowledge, which tracks gametes until day 5 of in vitro development, where the authors have found a significantly decreased rate of apoptosis in cumulus cells of good quality blastocysts compared to poor quality blastocysts or arrested embryos [25]. We speculate that the discrepancy in results is due to the usage of different methods for measuring apoptosis, and also due to the analysis of cumulus rather than follicular granulosa cells, as already mentioned above. Since we observed the early phenomenon of apoptotic process, a proportion of granulosa cells which were classified as apoptotic in our study, would be classified as normal, if a later phenomenon of apoptotic process, i.e. DNA fragmentation, were used. We found a lower percentage of necrotic and a higher percentage of normal granulosa cells in the follicles yielding the development of a blastocyst, morula or ≤10-cell embryo compared to the follicles with no embryo development due to abnormal fertilization, although the differences were not statistically significant.
The analysis of follicles that resulted in implantation revealed a tendency to lower percentage of apoptotic granulosa cells from the corresponding follicle compared to the follicles not resulting in implantation, although statistical significance was not reached. It is known that implantation and pregnancy depend on multiple factors; therefore, the percentage of apoptotic granulosa cells cannot be the only predictor of the occurrence of pregnancy, although it may affect embryo quality. We deliberately included data on implantation assessed by serum β-HCG measurement and not on pregnancy confirmed by ultrasound. On ultrasound, pregnancy can be detected approximately 4 weeks after ET, its course being more dependent on embryonic genome, embryonic-endometrial interactions and maternal factors than pregnancy assessed by serum β-HCG measurement two weeks after ET. We decided to include both corresponding follicles into the analysis in cases when two blastocysts were transferred, because even if the resulting pregnancy would be a singleton pregnancy, we would not be able to know, which of the two blastocysts implanted.
Apoptosis is a process that can be triggered by different intracellular and extracellular mechanisms [28, 29]. Free radicals and ROS can trigger the chain of reactions that lead to apoptosis. We wanted to find out, whether apoptosis of granulosa cells is triggered by ROS that are produced intrinsically in granulosa cells. We found a positive relation between the percentage of ROS producing granulosa cells and the percentage of apoptotic granulosa cells. Ours is the first study to determine ROS production in granulosa cells and its association with apoptosis.
There is evidence that ROS can damage oocytes and reduce their fertilization competence [13]. Oxidative stress in granulosa cells was found to lower fertilization rates and decrease quality of embryos in IVF cycles [14]. We observed that a high percentage of ROS producing granulosa cells in a follicle results in no oocyte retrieved from that follicle. In the follicles with a fertilized oocyte there was a tendency to a decreased percentage of ROS producing granulosa cells compared to the follicles with a non-fertilized corresponding oocyte, but the statistical significance was not reached. We found an increased percentage of ROS producing granulosa cells in the subgroup of follicles with abnormal fertilization, compared to subgroups of follicles with a blastocyst, morula or ≤10-cell embryo development, but again the difference was not statistically significant. Increased percentages of ROS producing granulosa cells diminished implantation rate in our study. Extensive ROS production in granulosa cells seems to have an adverse effect on oocyte, embryo quality and implantation rate. Higher production of ROS in granulosa cells results in oxidative stress in the follicular fluid; excessive levels of oxidative stress in a follicle have been found to have a negative impact on the outcome of IVF [30].
Knowing that phagocytotic lymphocytes are capable of an oxidative burst after stimulation with PMA [16], we analogously assessed whether granulosa cells are capable of producing a similar oxidative burst. The granulosa cells, capable to produce an oxidative burst, were observed in a small number of analyzed follicles only. Granulosa cells seem to produce nearly all ROS in basic conditions and are mainly not capable to produce additional ROS when stimulated with PMA. This finding also confirmed that the analysed samples consisted mainly of granulosa cells; their contamination with lymphocytes would result in a higher ROS production after PMA stimulation.
We conclude that apoptosis and ROS production in granulosa cells have no significant impact on fertilization and do not correlate with the development of blastocyst. Apoptosis of granulosa cells has no effect on implantation rates, while an increased percentage of ROS producing granulosa cells results in fewer oocytes retrieved and diminishes implantation rate assessed by the serum β-HCG measurement.
References
Tilly JL: Apoptosis and ovarian function. Rev Reprod 1996;1:162–72
Tilly JL, Kowalski KI, Johnson AL, Hsueh AJ: Involvement of apoptosis in ovarian follicular atresia and postovulatory regression. Endocrinology 1991;192:2799–801
Nakahara K, Saito H, Saito T, Ito M, Ohta N, Takahashi T, Hiroi M. The incidence of apoptotic bodies in membrana granulosa can predict prognosis of ova from patients participating in in vitro fertilization programs. Fertil Steril 1997;68:312–7
Oosterhuis GJ, Michgelsen HW, Lambalk CB, Schoemaker J, Vermes I: Apoptotic cell death in human granulosa-lutein cells: a possible indicator of in vitro fertilization outcome. Fertil Steril 1998;70:747–9
Kaneko T, Saito H, Takahashi T, Ohta N, Saito T, Hiroi M: Effects of controlled ovarian hyperstimulation on oocyte quality in terms of the incidence of apoptotic granulose cells. J Assist Reprod Genet 2000;17:580–5
Jozwik M, Wolczynski S, Jozwik M, Szamatowicz M: Oxidative stress markers in preovulatory follicular fluid in humans. Mol Hum Reprod 1999;5:409–13
Agarwal A, Saleh RA, Badaiwy MA: Role of reactive oxygen species in the pathophysiology of human reproduction. Fertil Steril 2003;79:829–43
Agarwal A, Allamaneni SSR: Role of free radicals in female reproductive diseases and assisted reproduction. Reprod Biomed Online 2004;9:338–47
Pasqualotto EB, Agarwal A, Sharma RK, Izzo VM, Pinotti JA, Joshi NJ, Rose BI: Effect of oxidative stress in follicular fluid on the outcome of assisted reproductive procedures. Fertil Steril 2004;81:973–6
Sharma RK, Agarwal A: Role of reactive oxygen species in gynecologic diseases. Reprod Med Biol 2004;3:177–99
Agarwal A, Gupta S, Sharma R. Oxidative stress and its implications in female infertility – a clinician’s perspective. Reprod Biomed Online 2005;11:641–50
Attaran M, Pasqualotto E, Falcone T, Goldberg JM, Miller KF, Agarwal A, Sharma RK: The effect of follicular fluid reactive oxygen species on the outcome of in vitro fertilization. Int J Fertil Womens Med 2000;45:314–20
Tarin JJ: Potential effects of age-associated oxidative stress on mammalian oocytes/embryos. Mol Hum Reprod 1996;2:717–24
Seino T, Saito H, Kaneko T, Takahashi T, Kawachiya S, Kurachi H: Eight-hydroxy-2′-deoxyguanosine in granulosa cells is correlated with the quality of oocytes and embryos in an in vitro fertilization-embryo transfer program. Fertil Steril 2002;77:1184–90
Vrtačnik Bokal E, Meden Vrtovec H, Virant Klun I, Verdenik I: Prolonged HCG action affects angiogenic substances and improves follicular maturation, oocyte quality and fertilization competence in patients with polycystic ovarian syndrome. Hum Reprod 2005;20:1562–8
Rothe G, Valet G: Flow cytometric analysis of respiratory burst activity in phagocytes with hydroethidine and 2′,7′-dichlorofluorescin. J Leukoc Biol 1990;47:440–8
Billig H, Furuta I, Hsueh AJW: Estrogens inhibit and androgens enhance ovarian granulosa cell apoptosis. Endocrinology 1993;133:2204–12
Papadopoulos V, Dharmarajan AM, Li H, Culty M, Lemay M, Sridaran R: Mitochondrial peripheral-type benzodiazepine receptor expression. Correlation with gonadotropin-releasing hormone (GnRH) agonist-induced apoptosis in the corpus luteum. Biochem Pharmacol 1999;58:1389–93
Matsubara H, Ikuta K, Ozaki Y, Suzuki Y, Suzuki N, Sato T, Suzumori K: Gonadotropins and cytokines affect luteal function through control of apoptosis in human luteinized granulosa cells. J Clin Endocrinol Metab 2000;85:1620–6
Clavero A, Castilla JA, Nunez AI, Garcia-Pena M, Maldonado V, Fontes J, Mendoza N, Martinez L: Apoptosis in human granulosa cells after induction of ovulation in women participating in an intracytoplasmic sperm injection program. Eur J Obstet Gynecol Reprod Biol 2003;110:181–5
Giampietro F, Sancilio S, Tiboni GM, Rana RA, Di Pietro R: Levels of apoptosis in human granulosa cells seem to be comparable after therapy with a gonadotropin-releasing hormone agonist or antagonist. Fertil Steril 2006;85:412–9
Saito H, Seino T, Kaneko T, Nakahara K, Toya M, Kurachi H: Endometriosis and oocyte quality. Gynecol Obstet Invest 2002;53: 46–51
Lee KS, Joo BS, Na YJ, Yoon MS, Choi OH, Kim WW: Cumulus cell apoptosis as an indicator to predict the quality of oocytes and the outcome of IVF-ET. J Assist Reprod Genet 2001;18:490–8
Host E, Gabrielsen A, Lindenberg S, Smidt-Jensen S: Apoptosis in human cumulus cells in relation to zona pellucida thickness variation, maturation stage, and cleavage of the corresponding oocyte after intracytoplasmic sperm injection. Fertil Steril 2002;77: 511–5
Corn CM, Hauser-Kronberger C, Moser M, Tews G, Ebner T: Predictive value of cumulus cell apoptosis with regard to blastocyst development of corresponding gametes. Fertil Steril 2005;84:627–33
Williams GT, Smith CA: Molecular regulation of apoptosis: genetic controls on cell death. Cell 1993;74:777–9
Shoukir Y, Chardonnens D, Campana A, Sakkas D: Blastocyst development from supernumerary embryos after intracytoplasmic sperm injection: a paternal influence? Hum Reprod 1998;13: 1632–7
Miller JE, Smith TT: The effect of intracytoplasmic sperm injection and semen parameters on blastocyst development in vitro. Hum Reprod 2001;16:918–24
Hsu SY, Hsueh AJ: Tissue-specific Bcl-2 protein partners in apoptosis: An ovarian paradigm. Physiol Rev 2000;80:593– 614
Wiener-Megnazi Z, Vardi L, Lissak A, Shnizer S, Reznick AZ, Ishai D, Lahav-Baratz S, Shiloh H, Koifman M, Dirnfeld M: Oxidative stress indices in follicular fluid as measured by the thermochemiluminescence assay correlate with outcome parameters in in vitro fertilization. Fertil Steril 2004;82:1171–6
Acknowledgements
The authors wish to thank all members of our IVF team for assistance in the study, and Mojca Pirc, B.A., for editing the text.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jančar, N., Kopitar, A.N., Ihan, A. et al. Effect of apoptosis and reactive oxygen species production in human granulosa cells on oocyte fertilization and blastocyst development. J Assist Reprod Genet 24, 91–97 (2007). https://doi.org/10.1007/s10815-006-9103-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-006-9103-8