
Abstract
Autism spectrum disorder (ASD) is a neurodevelopmental disorder. The associations between the cerebellum and clinical traits remain unclear. We performed amplitude of low-frequency fluctuation (ALFF) analysis to explore the associations between spontaneous brain activity and clinical traits. 361 juvenile ASD patients were included from the ABIDEII database. In the ASD group, the mean ALFF values of cerebellum 4 5 were correlated with SRS awareness and communication. The mean ALFF values of cerebellum 6 and vermis 4 5 were both positively correlated with SRS total, awareness, communication, and motivation. In contrast, the mean ALFF values of vermis 1 2 were negatively correlated with SRS total, awareness, and mannerisms. Our study suggests a role of the cerebellum in functional impairments in ASD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD), characterized by the persistent existence of deficits in social cognition and communication and restricted, repetitive patterns of sensory-motor behaviors, is a cluster of mental disorders of the neurodevelopmental type (Association, 2013; Lord et al., 2018). Approximately one in 161 children worldwide suffers from ASD (Elsabbagh et al., 2012), and one in 54 eight-year-old children is diagnosed with ASD in the USA (CDCP, 2020). The pathophysiology of ASD remains unknown despite many available studies, including neuroimaging studies. To date, the temporal and frontal lobe, thalamus, basal ganglia, limbic system, and cerebellum have been reported to be affected in ASD (Hampson & Blatt, 2015; Maximo & Kana, 2019; Pascual-Belda et al., 2018). Among the brain regions involved in ASD, the cerebellum is one of the most studied.
The cerebellum has long been thought to be an important brain region for motor learning and coordination (De Zeeuw & Ten Brinke, 2015; Manto et al., 2012). There is increasing evidence supporting the cerebellum as one of the key brain regions involved in ASD. Genetic risk factors in ASD were estimated to be approximately 80% (Bai et al., 2019). Meanwhile, a few genes have been recognized to be related to cerebellar abnormalities in ASD (Aldinger et al., 2013; Wang et al., 2019). Moreover, ASD patients showed alterations in cerebellar volume and Purkinje cell density (Skefos et al., 2014; Webb et al., 2009). Resting-state brain functional connectivity (FC) analysis also showed altered cerebrocerebellar and within-network cerebellar FCs in ASD (Khan et al., 2015; Stoodley et al., 2017). The findings from genetic, anatomical and neuroimaging studies strongly suggest that the cerebellum plays an important role in the neuropathophysiological mechanisms of ASD. However, the small sample size in most ASD studies has limited the reliability of these findings. Moreover, the results from different studies were not consistent. More importantly, few studies have focused on the associations between brain regions and clinical traits (e.g., cognition, communication, and motivation) in ASD.
The question of how the cerebellum is associated with clinical symptoms of ASD has been a matter of interest in recent studies. A previous neuroimaging study indicated that reductions in gray matter in cerebellar lobule VII (Crus I/II) in children with ASD correlated with the severity of symptoms in social interaction and communication (D’Mello et al., 2015). Regional homogeneity (ReHo) analysis showed that the cerebellum was significantly correlated with clinical traits of ASD when scored by the Social Communication Questionnaire (Dajani & Uddin, 2016). Some other studies, however, failed to detect correlations between FC or spontaneous activity of the cerebellum and symptoms of ASD (Carper et al., 2015; Padmanabhan et al., 2013). Therefore, the relationships between the cerebellum and symptoms of ASD remain to be clarified.
The aim of the present study was to explore the associations between spontaneous activity of the cerebellum and the clinical traits of ASD. For this purpose, we applied amplitude of low-frequency fluctuation (ALFF) analysis to resting-state functional magnetic resonance imaging (fMRI) data to explore spontaneous brain activity divergence between ASD patients and healthy controls. Then, the ALFF values of the region of interest (ROI), used to depict spontaneous activity, were extracted, and their correlations with symptoms of ASD were analyzed.
Materials and Methods
Participants
The data included in the present study were acquired from the Autism Brain Imaging Data Exchange II (ABIDE II, http://fcon_1000.projects.nitrc.org/indi/abide/abide_II.html) (Di Martino et al., 2017) dataset and included data from 19 independent sites. We downloaded the whole dataset including 1114 subjects with resting-state fMRI data and their phenotypic data. Then, juvenile ASD patients (aged less than or equal to 18 years) were selected for the study. Age- and sex-matched healthy subjects were included as controls. The clinical severity of ASD was scored using the Social Responsiveness Scale (SRS) (T scores) (Constantino, 2013) where available and included five subscales: awareness, cognition, communication, motivation, and mannerism.
Data Preprocessing
The scan protocols of resting-state fMRI varied across the 19 sites. Therefore, we preprocessed the neuroimages site by site using a standardized pipeline with the corresponding parameters. The preprocessing steps included removing the first four volumes, slice-timing correction, motion realignment, and spatial normalization using the EPI template to the stereotactic space of the Montreal Neurological Institute (MNI) with a voxel size of 3 × 3 × 3 mm. Then, nuisance covariates, including head motion parameters and linear trends, were regressed out from the BOLD signals. Finally, we performed temporal bandpass filtering (0.01–0.08 Hz) across time series. These preprocessing steps were performed using the data processing and analysis for brain imaging (DPABI) MATLAB toolbox (Yan et al., 2016).
Amplitude of Low-Frequency Fluctuation (ALFF) Analysis
After data preparation, ALFF analysis of each subject’s data was performed using DPABI (Yan et al., 2016). ALFF analysis of fMRI data has been widely applied to measure the magnitude of the energy from blood oxygenation level-dependent (BOLD) signal intensity and indirectly depict the intensity of regional spontaneous brain activity (Deng et al., 2016; Lu et al., 2014; Tu et al., 2015) in the resting state. Such relative activity of the local brain area is caused by the rhythmic activity of brain regions functionally related to other brain regions. Power spectra of the time series were calculated, and the sum of amplitudes within the low-frequency band (0.01–0.08 Hz) was computed for each voxel. Then, the square root was obtained at each power spectrum frequency. The ALFF value of each voxel was taken as the average square root across the band of interest and was divided by the mean ALFF value within the brain mask to obtain a standardized value (Yu-Feng et al., 2007). The location assignments of ALFF differences between ASD patients and NCs were performed by using anatomical automatic labeling template 3 (AAL3) (Rolls et al., 2020).
The ALFF values of ROIs were extracted to characterize the spontaneous activity of the ROIs. The ALFF values of ROIs for each subject were extracted to depict spontaneous brain activity.
Correlation Analysis
To explore the association between clinical severity and spontaneous brain activity, partial correlation analysis between the extracted ALFF values of ROIs and SRS T scores was performed. Age, sex, mean Jenkinson FD, and data site were employed as covariates to diminish the possible effect of other variables. Notably, we defined the ROIs based on the AAL3 atlas, not the results of ALFF analysis. Seventeen subregions of AAL3 within the cerebellum were employed as ROIs (bilaterally combined).
Statistical Analysis
To test the spontaneous brain activity differences between ASD patients and NCs, we carried out ALFF analysis and used a two-sample t test and two-tailed threshold-free cluster enhancement (TFCE) correction with the permutation analysis of linear models (PALM) test (p < 0.01, number of permutations: 1000) (Chen et al., 2018; Winkler et al., 2016). The mean Jenkinson FD was used as a covariate to eliminate the disturbance of micro-head motions. Additionally, age and sex were controlled for. To decrease the effect of site, the site of data collection was also included as a covariate. The edge cluster connectivity criterion, rmm = 5.
Comparisons of the mean ALFF of cerebellar subregions between ASD patients and NCs were performed using a two-sample t test with age, sex, mean Jenkinson FD, and data site regressed out. For the comparisons of mean ALFF values of cerebellar subregions with a P value less than 0.05, further false discovery rate (FDR) corrections were applied. FDR-corrected p < 0.05 was considered statistically significant. We computed Cohen's d for each variable to assess the effect size between two groups.
The relationship between ALFF values and SRS T scores was analyzed using partial correlation analysis with age, sex, mean Jenkinson FD, and data sites as covariates. For the partial correlation coefficients with P less than 0.05, further FDR corrections were applied. Only FDR-adjusted p values lower than 0.05 were considered significant.
Results
Sample Composition
Sample 2 from NYU Langone Medical Center was excluded because the MRI scan did not cover the whole cerebellum. A total of 1087 subjects were included, with data from 18 sites. Of the subjects, 494 were ASD patients (336 males, 63 females) and 593 were normal controls (NCs, 298 males, 143 females) aged less than or equal to 18 years. To decrease the sex bias between the two groups, we randomly included (MATLAB randperm function) 361 ASD patients (302 males, 59 females) and 361 NC (292 males, 69 females) in the subsequent ALFF analysis. Eleven ASD patients had comorbidities, such as attention deficit hyperactivity disorder and simple phobia. No sex or age differences were observed in the two groups. The mean and SEM of the Social Responsiveness Scale Total T scores in ASD patients and NCs were 78.43 ± 0.97 and 44.72 ± 0.32, respectively. The detailed demographics and ID list of the participants are shown in S. Table 1 and S. Table 2.
ALFF Changes of Cerebellum Regions Between ASD Patients and NCs
To test the spontaneous brain activity differences between ASD patients and NCs, ALFF analysis was performed. Three clusters within the cerebellum were obtained, and the locations were assigned by using the AAL3 template. Significant differences were found in extensive cerebellar regions involving three clusters: cluster 1 (cerebellum_9_L, cerebellum_8_L), cluster 2 (cerebellum_4_5_L, vermis_3, cerebellum_3_L, vermis_1_2), and cluster 3 (cerebellum_9_R, cerebellum_8_R). Furthermore, these clusters showed decreased ALFF values compared with those in the NCs (Fig. 1, Table 1).

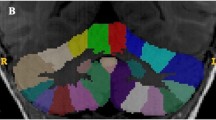
The section cutting and surface view of ALFF showing differences between ASD patients and NCs in the cerebellum. Section cutting view (A) and surface view (B). Two-sample t tests and two-tailed threshold-free cluster enhancement (TFCE) corrections with permutation analysis of linear models (PALM) were used (p < 0.01, number of permutations: 1,000). The yellow outline in A indicates the contour profile of cerebellum 9 of AAL3. The color bar represents the range of voxel intensity values. L, left. R, right. The detailed location assignments are shown in Table 1
Findings From Comparisons of ALFF Values Between ASD Patients and NCs
To explore the possible changes in spontaneous activity of cerebellar subregions in ASD patients, we further compared the mean ALFF values for each subregion within the cerebellum between ASD patients and NCs. The sample was the same as that used in the ALFF analysis. Age, sex, mean Jenkinson FD, and data site were regressed out in the comparisons. After FDR correction, it was noted that the ASD group showed a higher mean ALFF value than the NC group in cerebellum 4 5 (FDR-corrected p < 0.05, t = 2.849, Cohen’s d = 0.203). However, the mean ALFF values of cerebellum 7b, cerebellum 9, and vermis 7 in ASD patients were lower than those of NCs (p < 0.05) (Fig. 2). Other subregions within the cerebellum showed no significant differences.

Comparisons of the mean ALFF values for each ROI between ASD patients and NCs. Two-sample t tests were employed for the comparisons, and age, sex, mean Jenkinson FD, and data site were regressed out. The other cerebellum subregions showed no significant ALFF differences between the two groups. The d values indicated the effect size (Cohen’s d). *p < 0.05 after FDR adjustment
ALFF Values of Spontaneous Brain Activity Were Correlated with SRS Scores
We hypothesized that the cerebellar spontaneous activity depicted by ALFF might be associated with clinical traits depicted by SRS scores. Therefore, to examine the relationships between alterations of ALFF and clinical traits, partial correlation analyses were performed between SRS T scores, including SRS total T scores, SRS awareness T scores, SRS cognition T scores, SRS communication T scores, SRS motivation T scores, and SRS mannerisms T scores, and the mean ALFF values of the two ROIs. Seventeen ROI subregions within the cerebellum were defined using the AAL3 template (Rolls et al., 2020). The mean ALFF values of each ROI for individuals were extracted from the corresponding standardized ALFF results.
We noted that in juvenile ASD patients, the mean ALFF value of the cerebellum vermis 4 5 was significantly positively correlated with SRS awareness scores (r = 0.127, FDR-corrected p < 0.05) and SRS communication scores (r = 0.133, FDR-corrected p < 0.05). The mean ALFF values of cerebellum 6 and vermis 4 5 were both significantly positively correlated with SRS total T, SRS awareness, SRS communication, and SRS motivation (FDR-corrected p < 0.05). In contrast, the mean ALFF values of vermis 1 2 were significantly negatively correlated with SRS total T, SRS awareness, and SRS mannerisms (FDR-corrected p < 0.05) (S. Fig. 1). These findings were not obtained in normal controls (S. Fig. 2).
Medication and Sex Effects and ALFF Values of ROIs
Considering that medication might have impacts on spontaneous brain activity in ROIs, we divided the ASD patients into two groups according to their medication status. We found that the ALFF differences in cerebellum 4 5 and cerebellum 9 between ASD patients with medication (n = 124) and ASD patients without medication (n = 229) did not differ. Interestingly, the SRS T scores, including the five subscale scores, between ASD patients with medication and without medication showed no significant differences after FDR correction. The sex bias of spontaneous brain activity was also investigated. After SRS score correction, we found that male ASD patients (n = 215) showed upgraded ALFF values in the cerebellum 4 5 (t = 2.409, p = 0.017, d = 0.356) compared with those of female ASD patients (n = 44).
Reliability
We assessed reliability through a simple strategy. We further preprocessed the fMRI data with motion scrubbing. Images of time points with Jenkinson FD values larger than 0.2 were deleted. The results of the ALFF analysis remained the same as those of the previous analysis (S. Fig. 3). Another step to ensure the reliability of the present study was that we defined the ROIs based on the AAL3 atlas, not based on our own ALFF clusters.
Discussion
In the present study, we applied ALFF analysis to detect alterations in spontaneous brain activity in ASD patients and explored the associations between spontaneous brain activity and clinical traits. The different ALFF patterns can be related to different spontaneous brain activity patterns of the ASD patients and NCs. The cerebellar subregions of the AAL3 atlas were used as ROIs to investigate whether ALFF was related to the clinical severity of ASD. For this purpose, partial correlation analysis was employed to demonstrate the probable correlations between spontaneous brain activity and clinical traits. Furthermore, subgroup analysis of ASD patients suggested that spontaneous activity of the brain might be impacted by medication status. Finally, ALFF analysis of another randomly selected sample produced a similar ALFF map, which confirmed the high reproducibility of the present study. The combined findings provide evidence for a functional role of the cerebellum in ASD at the functional imaging level.
Based on our findings from functional imaging data, we have confirmed the importance of the cerebellum in ASD, which is in accordance with the findings of previous fMRI studies (Itahashi et al., 2015; Jack et al., 2017). Importantly, the decreased ALFF values of bilateral cerebellum 7b, cerebellum 9, and vermis 7 and increased ALFF values of bilateral cerebellum 4 5 in ASD patients suggest that these subregions of the cerebellum play heterogeneous roles in ASD. This means that dysfunction related to ASD might be partly attributed to enhanced spontaneous brain activity in cerebellum 4 5. Subsequent correlation analysis supported this assumption. The ALFF of cerebellum 4 5 was positively correlated with both the SRS awareness score and SRS communication score. Interestingly, we noted that the spontaneous activity of cerebellum vermis 1 2 was negatively related to SRS total scores and SRS awareness scores in ASD patients, which were not obtained in NCs. These findings support a mechanistic basis for the targeted treatment of ASD-related disorders. Excessive or insufficient spontaneous activity of subregions in the cerebellum could induce disorder in ASD.
As we expected, spontaneous cerebellar activity was associated with clinical severity and functional deficits, which is in good agreement with the results of earlier ALFF analyses (Guo et al., 2017) and task-dependent fMRI studies (Murphy et al., 2017). On the one hand, the mean ALFF values of some cerebellar subregions, including cerebellum 4 5, cerebellum 6, vermis 4 5, and vermis 1 2, were correlated with clinical traits depicted by SRS. On the other hand, we failed to find significant correlations between spontaneous activity and SRS scores in some other cerebellum subregions, including cerebellum 7b, cerebellum 9, and vermis 7, despite these regions showing altered spontaneous activity in ASD patients. These results suggested that these cerebellar subregions play a key role in functional impairments in ASD and further support the notion that no single pattern can characterize the role of the cerebellum in ASD.
A clinical study confirmed that patients with cerebellar lesions might experience cerebellar cognitive affective syndrome (Argyropoulos et al., 2020). Abnormal cerebellar activity has also been found in other diseases with cognitive impairment, such as Parkinson’s disease (Solstrand, 2020). However, the organization of cognitive function is still an unresolved issue. Some cerebellar subregions have been found to send (receive) projections to (from) the cerebral cortex (Bostan et al., 2013) and might functionally couple networks of the cerebral cortex (Buckner, 2013). These brain regions might function as circuits, such as cortico-basal ganglia-thalamic circuits (Nair et al., 2013; Schuetze et al., 2016). Notably, we tried to explore the whole-brain connections of cerebellum 4 5 and cerebellum 9. However, no significant differences in the two regions between ASD patients and NCs were observed. These findings indicated that anatomical and functional heterogeneity together may play a role in the cognitive function of the cerebellum. Different patterns may exist for different subregions of the cerebellum in relation to cognitive function. Further studies are needed to investigate how these cerebellar regions showing significant changes in ALFF interact with other regions in ASD patients.
In the subgroup analysis, it was noted that ASD patients with medication and ASD patients without medication showed no differences in spontaneous brain activities of ROIs after critical FDR correction, which means that the targets of the drugs might not be linked to the ROIs, including the cerebellum, thalamus and SMA. However, a previous study revealed that medication use might affect brain FC in ASD patients (Linke et al., 2017). Considering the significant changes in spontaneous brain activity in ASD patients, regulating spontaneous brain activity might be an important treatment mechanism of ASD medications. However, longitudinal studies should be performed to investigate whether ALFF changes over the course of ASD treatments.
Conclusion
In conclusion, in this functional imaging approach based on ALFF analysis and partial correlation analysis, we were able to demonstrate that ASD patients showed significant alterations in spontaneous activity of cerebellar regions 4 5 and 9. The changes in spontaneous activity of cerebellum 4 5, cerebellum 6, vermis 1 2, and vermis 4 5 were significantly correlated with some clinical traits in ASD. Our study suggests a role for the cerebellum in functional impairments in ASD and supports a mechanistic basis for the targeted treatment of ASD disorders.
Data Availability
The data used are publicly available in the ABIDE II database (http://fcon_1000.projects.nitrc.org/indi/abide/abide_II.html). The IDs of the subjects used in the study are listed in Appendix 1.
Abbreviations
- ASD:
-
Autism spectrum disorder
- ALFF:
-
Amplitude of low-frequency fluctuations
- ReHo:
-
Regional homogeneity
- fMRI:
-
Functional magnetic resonance imaging
- ROI:
-
Region of interest
- SRS:
-
Social responsiveness scale
- FC:
-
Functional connectivity
- AAL3:
-
Automated anatomical labelling 3
References
Aldinger, K. A., Kogan, J., Kimonis, V., Fernandez, B., Horn, D., Klopocki, E., Chung, B., Toutain, A., Weksberg, R., Millen, K. J., Barkovich, A. J., & Dobyns, W. B. (2013). Cerebellar and posterior fossa malformations in patients with autism-associated chromosome 22q13 terminal deletion. American Journal of Medical Genetics. Part A, 161A, 131–136.
Argyropoulos, G. P. D., van Dun, K., Adamaszek, M., Leggio, M., Manto, M., Masciullo, M., Molinari, M., Stoodley, C. J., Van Overwalle, F., Ivry, R. B., & Schmahmann, J. D. (2020). The cerebellar cognitive affective/schmahmann syndrome: A task force paper. Cerebellum, 19, 102–125.
Association, A. P. (2013). Diagnostic and statistical manual of mental disorders, fifth edition (DSM-5). American Psychiatric Publishing.
Bai, D., Yip, B. H., Windham, G. C., Sourander, A., Francis, R., Yoffe, R., Glasson, E., Mahjani, B., Suominen, A., Leonard, H., Gissler, M., Buxbaum, J. D., Wong, K., Schendel, D., Kodesh, A., Breshnahan, M., Levine, S. Z., Parner, E. T., Hansen, S. N., … Sandin, S. (2019). Association of genetic and environmental factors with autism in a 5-country cohort. JAMA Psychiatry. https://doi.org/10.1001/jamapsychiatry.2019.141
Bostan, A. C., Dum, R. P., & Strick, P. L. (2013). Cerebellar networks with the cerebral cortex and basal ganglia. Trends in Cognitive Sciences, 17, 241–254.
Buckner, R. L. (2013). The cerebellum and cognitive function: 25 years of insight from anatomy and neuroimaging. Neuron, 80, 807–815.
Carper, R. A., Solders, S., Treiber, J. M., Fishman, I., & Muller, R. A. (2015). Corticospinal tract anatomy and functional connectivity of primary motor cortex in autism. Journal of the American Academy of Child and Adolescent Psychiatry, 54, 859–867.
Centers for Disease Control and Prevention. (2020). Community Report on Autism. https://www.cdc.gov/ncbddd/autism/addm-communityreport/index.html
Chen, X., Lu, B., & Yan, C. G. (2018). Reproducibility of R-fMRI metrics on the impact of different strategies for multiple comparison correction and sample sizes. Human Brain Mapping, 39, 300–318.
Constantino, J. N. (2013). Social responsiveness scale. In F. R. Volkmar (Ed.), Encyclopedia of autism spectrum disorders (pp. 2919–2929). Springer.
Dajani, D. R., & Uddin, L. Q. (2016). Local brain connectivity across development in autism spectrum disorder: A cross-sectional investigation. Autism Research, 9, 43–54.
De Zeeuw, C. I., & Ten Brinke, M. M. (2015). Motor learning and the cerebellum. Cold Spring Harbor Perspectives in Biology, 7, a021683.
Deng, Z., Chandrasekaran, B., Wang, S., & Wong, P. C. (2016). Resting-state low-frequency fluctuations reflect individual differences in spoken language learning. Cortex, 76, 63–78.
Di Martino, A., O’Connor, D., Chen, B., Alaerts, K., Anderson, J. S., Assaf, M., Balsters, J. H., Baxter, L., Beggiato, A., Bernaerts, S., Blanken, L. M., Bookheimer, S. Y., Braden, B. B., Byrge, L., Castellanos, F. X., Dapretto, M., Delorme, R., Fair, D. A., Fishman, I., … Milham, M. P. (2017). Enhancing studies of the connectome in autism using the autism brain imaging data exchange II. Science Data, 4, 170010.
D’Mello, A. M., Crocetti, D., Mostofsky, S. H., & Stoodley, C. J. (2015). Cerebellar gray matter and lobular volumes correlate with core autism symptoms. NeuroImage: Clinical, 7, 631–639.
Elsabbagh, M., Divan, G., Koh, Y. J., Kim, Y. S., Kauchali, S., Marcin, C., Montiel-Nava, C., Patel, V., Paula, C. S., Wang, C., Yasamy, M. T., & Fombonne, E. (2012). Global prevalence of autism and other pervasive developmental disorders. Autism Research, 5, 160–179.
Guo, X., Chen, H., Long, Z., Duan, X., Zhang, Y., & Chen, H. (2017). Atypical developmental trajectory of local spontaneous brain activity in autism spectrum disorder. Scientific Reports, 7, 39822.
Hampson, D. R., & Blatt, G. J. (2015). Autism spectrum disorders and neuropathology of the cerebellum. Frontiers in Neuroscience, 9, 420.
Itahashi, T., Yamada, T., Watanabe, H., Nakamura, M., Ohta, H., Kanai, C., Iwanami, A., Kato, N., & Hashimoto, R. (2015). Alterations of local spontaneous brain activity and connectivity in adults with high-functioning autism spectrum disorder. Molecular Autism, 6, 30.
Jack, A., Keifer, C. M., & Pelphrey, K. A. (2017). Cerebellar contributions to biological motion perception in autism and typical development. Human Brain Mapping, 38, 1914–1932.
Khan, A. J., Nair, A., Keown, C. L., Datko, M. C., Lincoln, A. J., & Muller, R. A. (2015). Cerebro-cerebellar resting-state functional connectivity in children and adolescents with autism spectrum disorder. Biological Psychiatry, 78, 625–634.
Linke, A. C., Olson, L., Gao, Y., Fishman, I., & Muller, R. A. (2017). Psychotropic medication use in autism spectrum disorders may affect functional brain connectivity. Biological Psychiatry Cognitive Neuroscience and Neuroimaging, 2, 518–527.
Lord, C., Elsabbagh, M., Baird, G., & Veenstra-Vanderweele, J. (2018). Autism spectrum disorder. The Lancet, 392, 508–520.
Lu, D., Jiao, Q., Zhong, Y., Gao, W., Xiao, Q., Liu, X., Lin, X., Cheng, W., Luo, L., Xu, C., Lu, G., & Su, L. (2014). Altered baseline brain activity in children with bipolar disorder during mania state: A resting-state study. Neuropsychiatric Disease and Treatment, 10, 317–323.
Manto, M., Bower, J. M., Conforto, A. B., Delgado-García, J. M., Da Guarda, S. N., Gerwig, M., Habas, C., Hagura, N., Ivry, R. B., Mariën, P., Molinari, M., Naito, E., Nowak, D. A., Oulad Ben Taib, N., Pelisson, D., Tesche, C. D., Tilikete, C., & Timmann, D. (2012). Consensus paper: Roles of the cerebellum in motor control–the diversity of ideas on cerebellar involvement in movement. Cerebellum, 11, 457–87.
Maximo, J. O., & Kana, R. K. (2019). Aberrant “deep connectivity” in autism: A cortico-subcortical functional connectivity magnetic resonance imaging study. Autism Research, 12, 384–400.
Murphy, C. M., Christakou, A., Giampietro, V., Brammer, M., Daly, E. M., Ecker, C., Johnston, P., Spain, D., Robertson, D. M., Consortium, M. A., Murphy, D. G., & Rubia, K. (2017). Abnormal functional activation and maturation of ventromedial prefrontal cortex and cerebellum during temporal discounting in autism spectrum disorder. Human Brain Mapping, 38, 5343–5355.
Nair, A., Treiber, J. M., Shukla, D. K., Shih, P., & Muller, R. A. (2013). Impaired thalamocortical connectivity in autism spectrum disorder: A study of functional and anatomical connectivity. Brain, 136, 1942–1955.
Padmanabhan, A., Lynn, A., Foran, W., Luna, B., & O’Hearn, K. (2013). Age related changes in striatal resting state functional connectivity in autism. Frontiers in Human Neuroscience, 7, 814.
Pascual-Belda, A., Diaz-Parra, A., & Moratal, D. (2018). Evaluating functional connectivity alterations in autism spectrum disorder using network-based statistics. Diagnostics. https://doi.org/10.3390/diagnostics8030051
Rolls, E. T., Huang, C. C., Lin, C. P., Feng, J., & Joliot, M. (2020). Automated anatomical labelling atlas 3. NeuroImage, 206, 116189.
Schuetze, M., Park, M. T., Cho, I. Y., MacMaster, F. P., Chakravarty, M. M., & Bray, S. L. (2016). Morphological alterations in the thalamus, striatum, and pallidum in autism spectrum disorder. Neuropsychopharmacology, 41, 2627–2637.
Skefos, J., Cummings, C., Enzer, K., Holiday, J., Weed, K., Levy, E., Yuce, T., Kemper, T., & Bauman, M. (2014). Regional alterations in purkinje cell density in patients with autism. PloS one, 9, e81255.
Solstrand, D. L., Lungu, O., & Doyon, J. (2020). Cerebellar contribution to motor and Non-motor functions in Parkinson’s disease: A meta-analysis of fMRI findings. Frontiers in Neurology, 11, 127.
Stoodley, C. J., D’Mello, A. M., Ellegood, J., Jakkamsetti, V., Liu, P., Nebel, M. B., Gibson, J. M., Kelly, E., Meng, F., Cano, C. A., Pascual, J. M., Mostofsky, S. H., Lerch, J. P., & Tsai, P. T. (2017). Altered cerebellar connectivity in autism and cerebellar-mediated rescue of autism-related behaviors in mice. Nature Neuroscience, 20, 1744–1751.
Tu, Y., Wei, Y., Sun, K., Zhao, W., & Yu, B. (2015). Altered spontaneous brain activity in patients with hemifacial spasm: A resting-state functional MRI study. PloS one, 10, e0116849.
Wang, C., Pan, Y. H., Wang, Y., Blatt, G., & Yuan, X. B. (2019). Segregated expressions of autism risk genes Cdh11 and Cdh9 in autism-relevant regions of developing cerebellum. Molecular Brain, 12, 40.
Webb, S. J., Sparks, B. F., Friedman, S. D., Shaw, D. W., Giedd, J., Dawson, G., & Dager, S. R. (2009). Cerebellar vermal volumes and behavioral correlates in children with autism spectrum disorder. Psychiatry Research, 172, 61–67.
Winkler, A. M., Ridgway, G. R., Douaud, G., Nichols, T. E., & Smith, S. M. (2016). Faster permutation inference in brain imaging. NeuroImage, 141, 502–516.
Yan, C. G., Wang, X. D., Zuo, X. N., & Zang, Y. F. (2016). DPABI: Data processing & analysis for (resting-state) brain imaging. Neuroinformatics, 14, 339–351.
Yu-Feng, Z., Yong, H., Chao-Zhe, Z., Qing-Jiu, C., Man-Qiu, S., Meng, L., Li-Xia, T., Tian-Zi, J., & Yu-Feng, W. (2007). Altered baseline brain activity in children with ADHD revealed by resting-state functional MRI. Brain and Development, 29, 83–91.
Acknowledgments
The authors acknowledge members of the Autism Brain Imaging Data Exchange and the International Neuroimaging Data-sharing Initiative for their efforts to aggregate and organize phenotypic and imaging data. We thank the Youth Program of the National Natural Science Foundation of China (81804198) and the Special Training Program for Young Scientific and Technological Talents of Southwest Medical University 2020–2022 for sponsorship of Jianghai Ruan.
Funding
This work was supported by the Youth Program of National Natural Science Foundation of China (81804198), Funding of Human Resources and Social Security Department, Sichuan (2018-145, 65), and Youth Fund of Southwest Medical University (2018-ZRQN-003). We thank the Special Training Program for Young Scientific and Technological Talents of Southwest Medical University 2020–2022 for sponsorship of Jianghai Ruan.
Author information
Authors and Affiliations
Contributions
JL: data curation, methodology, formal analysis, visualization, writing—original draft, writing—review & editing. XC: conceptualization, methodology, data curation, writing—original draft. RZ: conceptualization, data curation, writing—review & editing. AC: conceptualization, methodology, writing—review & editing. YZ: methodology, data curation, formal analysis. JR: conceptualization, methodology, supervision, writing—review & editing, funding acquisition.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical Approval
The study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Southwest Medical University (Luzhou, China).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Li, J., Chen, X., Zheng, R. et al. Altered Cerebellum Spontaneous Activity in Juvenile Autism Spectrum Disorders Associated with Clinical Traits. J Autism Dev Disord 52, 2497–2504 (2022). https://doi.org/10.1007/s10803-021-05167-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-021-05167-6