
Abstract
This study aimed to investigate factors associated with a delayed autism spectrum (ASD) diagnosis when compared to children with either no or early ASD diagnosis. Among 893 children assessed for ASD before age 8, 39% had no ASD at baseline, of which 21% received a later ASD diagnosis. Autism symptoms, diagnostic history of other developmental disorders, cognitive ability, and socioeconomic factors were associated with delayed ASD. Autism Diagnostic Observation Schedule (ADOS) scores in delayed ASD fell between early and no ASD. Other developmental disorders, time and clinical trends like ADOS use and low parental education distinguished delayed and early ASD, whereas higher frequency of IQ < 70 at baseline and a diagnosis of emotional disorders during follow-up distinguished delayed and no ASD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is a highly heterogeneous disorder with considerable personal and public health impact (American Psychiatric 1994, 2013; World Health 1992). Early diagnosis of ASD is desirable, as it enables treatment and intervention plans, public support systems, and the chance of reducing co-occurring symptoms through individualized interventions (Clark et al. 2018; Daniels and Mandell 2014; Jónsdóttir et al. 2011; Lord et al. 2018; Parikh et al. 2018). Most importantly, early ASD identification and intervention have been shown to have significant impact on function and progress, and result in better overall outcome than when diagnosed at a later age (Clark et al. 2018; Daniels and Mandell 2014; Goodwin et al. 2018; Helt et al. 2008; Parikh et al. 2018; Sheldrick et al. 2017). Although ASD symptoms often present early in life, and despite advances in early diagnosis, many children remain undiagnosed until school age, adolescence or even adulthood (Brett et al. 2016; Daniels and Mandell 2014; Jensen et al. 2014; Sheldrick et al. 2017; Wiggins et al. 2006). In Denmark, rates of diagnosis vary by time, age, and sex with rates higher in boys than girls in childhood and higher in girls than boys in adolescence (Dalsgaard et al. 2019). Another Danish study of persons aged 0–65 years and followed from 1995 to 2010 showed that the diagnosis was made before school-age in 30% of cases, 40% were diagnosed in school-age and adolescence, 20% in young adulthood, and 20% were diagnosed in adulthood (Jensen et al. 2014). A third study of persons born 1980–2012 and followed through 2016 showed that the cumulative incidence of ASD also increased steadily, almost linearly, with age reflecting identification of ASD into adolescence and adulthood (Schendel and Thorsteinsson 2018). Some children may in fact get an ASD diagnosis in later childhood despite early assessment, and hence experience a delay in recognition of ASD. These children may be defined as delayed ASD cases, as they have previously had developmental concerns and a diagnostic evaluation at an early stage resulting in a non-spectrum conclusion, and thus not diagnosed with ASD until assessed at an older age (Bacon et al. 2018; Brian et al. 2016; Davidovitch et al. 2015; Goodwin et al. 2018; Oien et al. 2018; Ozonoff et al. 2018). Possible explanations for the delay in ASD diagnosis comprise; symptoms of other developmental disorders that overshadow social impairments or make social impairments appear secondary; the ASD diagnostic threshold may not be met until at a later age when social demands of the environment begin to exceed the child’s abilities; or the ASD symptoms in early childhood are expressed differently than in later childhood (Bacon et al. 2018; Brian et al. 2016; Davidovitch et al. 2015; Goodwin et al. 2018; Oien et al. 2018; Ozonoff et al. 2018).
Many studies have examined the diagnostic stability of ASD across age (Helt et al. 2008), however, children with an initial ASD-negative assessment have rarely been followed (Ozonoff et al. 2018), and only few studies have examined delayed ASD cases (Brian et al. 2016; Davidovitch et al. 2015; Oien et al. 2018; Ozonoff et al. 2018). Studies conducted in the United States on late ASD cases, so called because of late time of suspicion and diagnosis, show these to be associated with lower maternal education and/or low socioeconomic status, lower ASD symptom severity, average cognitive ability, higher receptive language skills, being a female or belonging to an ethnic minority, and having a younger sibling close in age (Bickel et al. 2015; Brian et al. 2016; Daniels and Mandell 2014; Lord et al. 2018; Parikh et al. 2018; Sheldrick et al. 2017). However, whether these factors are also associated with a delayed ASD diagnosis is unknown. Only a few studies have examined delayed ASD cases and they found that these children initially received different diagnoses, most commonly language impairment, motor impairment, global developmental delay, intellectual disability and inattention problems (Brian et al. 2016; Davidovitch et al. 2015; Oien et al. 2018; Ozonoff et al. 2018).
The delayed ASD cases may represent a distinct group of children with ASD (Bacon et al. 2018; Ozonoff et al. 2018). Examining delayed ASD cases, and comparing similarities and differences between children with ASD whose symptoms develop more slowly and children who show clear symptoms at an early age, may lead to a deeper understanding of the development of ASD symptoms (Bacon et al. 2018; Frenette et al. 2013; Mazurek et al. 2014). Given the importance of timely interventions for improved outcomes, such studies may support the pending task of decreasing the age at initial ASD diagnosis (Bickel et al. 2015; Daniels and Mandell 2014; Davidovitch et al. 2015; Goodwin et al. 2018; Mazurek et al. 2014; Sheldrick et al. 2017).
Using a population-based clinical cohort, the aims of the study were to compare children with a delayed ASD diagnosis (“delayed ASD”) to children with an ASD diagnosis in first assessment ("early ASD") or no ASD diagnosis at first assessment or follow-up ("no ASD") in order to: (1) investigate characteristics of children with a delayed ASD diagnosis and (2) to investigate possible clinical and demographic factors associated with a delayed ASD diagnosis. Based on the literature, we hypothesized that autism symptom severity, diagnostic history of other developmental disorders, cognitive ability, and socioeconomic factors would contribute to a delayed ASD diagnosis.
Methods
Participants
The study population was defined by all children referred before the age of 7 with suspicion of ASD and accepted for evaluation to the Aarhus University Hospital, Department of Child and Adolescent Psychiatry, Denmark (the ASD clinic) in the period 2000–2010. In Denmark all citizens have free and equal access to medical services, and the public ASD clinic was responsible for all assessments of children referred with suspicion of ASD before the age of 7 and residing in the county of Aarhus with an estimated population of 845,000. Study inclusion criteria also included birth between January 1993 and December 2006. A total of 939 children were identified in the administrative records of the ASD clinic and fulfilled the inclusion criteria; 46 children were excluded due to missing data, thus a total of 893 children were included. Further details and the characteristics of the total sample are described in Avlund et al. (2020). Based on diagnostic data from medical records at initial evaluation in 2000–2010 ("baseline"), children were divided into two study groups: children with a diagnosis of ASD (early ASD) (n = 547) and children with no diagnosis of ASD (no ASD baseline) (n = 346). Linkage with registry-reported diagnostic information during follow-up in 2016 allowed division of the no ASD baseline subgroup into two groups: children assigned a diagnosis of ASD in the period between baseline and follow-up in 2016 (delayed ASD) (n = 74), and children without an ASD diagnosis through follow-up (no ASD) (n = 272). The three final study groups, based on ASD case status, are shown in Fig. 1. The age range in 2016 was 10–23 years and mean follow-up time was 10.9 years (SD 3.3).

Study cohort and ASD case status groups. ASD autism spectrum disorder. Baseline: diagnosis at initial assessment in the inclusion period, 2000–2010. Follow-up: diagnosis given during the follow-up period from baseline through 2016
Data Collection and Study Measures
The study was approved by the Danish Patient Safety Authority, The Danish Health Data Authority and Statistics Denmark. Data were collected via structured medical record abstraction and registry linkage. Variables from the ASD clinic’s medical records included clinical and demographic information from the first assessment at the ASD clinic (baseline), i.e. age, gender, year of initial assessment (calendar time), ASD diagnosis and subtype, co-occurring psychiatric diagnoses, Autism Diagnostic Observation Schedule (ADOS) scores (Lord et al. 2000), and cognitive ability. The cohort was linked to Danish nationwide registers using the unique personal identification number assigned to all persons in Denmark (Pedersen 2011; Thygesen et al. 2011). Information on all psychiatric ICD-10 diagnostic codes given at discharge from inpatient or outpatient hospital contacts during the follow-up period were obtained from the Danish National Patient Register (DNPR) (Andersen et al. 1999) and the Psychiatric Central Research Register (DPCR) (Mors et al. 2011). Information on mortality and parental education was obtained from Statistics Denmark (Thygesen et al. 2011). Children without an ASD diagnosis after initial assessment (no ASD baseline) were considered to be "at risk" of an ASD diagnosis from the date of ASD clinic discharge at baseline (2000–2010) and until the date of hospital admission with an ASD diagnosis, or follow-up time ended at 31 December 2016, whichever came first.
Initial ASD Assessment
The initial clinical assessment at baseline was conducted by a multidisciplinary team, and final diagnoses were team consensus decisions based on the total clinical judgment of all assessments. The diagnoses were based on International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) criteria (WHO). The specific subtype of ASD was also determined using the ICD-10 diagnostic codes childhood autism (F84.0), atypical autism (F84.1), Asperger syndrome (F84.5) and pervasive developmental disorder-not otherwise specified, PDD-NOS (F84.8). Diagnoses of other developmental or psychiatric disorders were classified into: attention-deficit/hyperactivity disorder (ADHD) (F90), specific language disorders (F80), and mixed specific developmental disorders (a mixture of specific developmental disorders of speech and language, of scholastic skills, of motor function and of social cognition, in which none predominates sufficiently, F83). The diagnostic process at the ASD clinic is described in more detail in Avlund et al. (2020).
Follow-up Diagnoses
Follow-up diagnoses were obtained from the Danish registries. The quality of childhood autism diagnoses in the DPCR has been found to be valid, and the completeness of ASD diagnoses in the register is considered to be good (Lauritsen et al. 2010; Mors et al. 2011; Parner et al. 2008). For analyses, other non-ASD diagnoses were categorized into either (1) baseline diagnoses other than ASD (retrieved from medical records at initial assessment as described above) or (2) diagnoses at the end of follow-up period other than ASD, which included all assigned diagnoses at baseline as well as the diagnoses the participants had received during the follow-up period.
ASD Symptoms at Baseline
Autism symptoms at baseline were based on ASD subtype and ADOS scores from the initial assessment at baseline. The ADOS is a standardized semi-structured assessment of ASD symptoms that obtains information through direct observation (Lord et al. 2000). ADOS provides an overall total score with empirically derived cut-offs for autism and autism spectrum. This study also used the dichotomous algorithm classification of ASD (autism + autism spectrum = above ADOS cut-off) versus non-spectrum (= below ADOS cut-off). Other ASD symptoms at baseline comprised sub-items from the algorithm that were similar in ADOS modules 1, 2 and 3, along with four items previously found to be discriminative between ASD and ADHD (i.e. quality of social overtures, unusual eye contact, facial expression directed to examiner and amount of reciprocal social communication) (Grzadzinski et al. 2016). Module number was used as a proxy for language ability, since Module 1 is used in children with no- or only single words, Module 2 in children who speaks in phrases, and Module 3 in children with fluent speech. All the clinicians at the ASD clinic who were involved in administering the instrument were certified to use ADOS in a clinical setting. Assessments in the first years of the inclusion period did not necessarily include ADOS (Avlund et al. 2020), and therefore the number of children that could be included in the ADOS analyses was reduced. The number of children with ADOS included in the assessment at baseline was: early ASD n = 504 (92.1%), delayed ASD n = 45 (60.8%), and no ASD = 146 (53.7%).
Cognitive Ability at Baseline
Various cognitive tests were used in the initial assessment based on the child's age, developmental level and verbal fluency. These tests included the Mullen Scales of Early Learning (Mullen 1995), Snijders-Oomen Nonverbal Intelligence Test (Snijders et al. 1997), the Wechsler Preschool and Primary Scale of Intelligence (Wechsler 2002) or the Wechsler Intelligence Scale for Children (Wechsler 1991). The tests were used to calculate either a developmental quotient, a non-verbal IQ or a total IQ, as a best estimate of the cognitive functioning. IQ scores ≥ 70 were recorded as no intellectual disability (ID) and IQ < 70 was recorded as ID. The majority of children (n = 899; 99.6%) were examined with one or more cognitive tests.
Parental Sociodemographic Status (SES) and Psychiatric History
Data on educational level of parents at the day of initiation of the assessment at baseline were obtained from Statistics Denmark and divided in three categories based on the number of years of education; low educational level (< 10 years of education), medium level of education (10–15 years of education) and high educational level (≥ 15 years of education) (Undervisningsministeriet 2020). Both maternal and paternal educational level was extracted, and in case of differences in educational level, the level of the parent with the highest educational level was used for analysis. Due to missing data in educational reports (early ASD; n = 29 (5.3%), delayed ASD; n = 1 (1.4%) and no ASD; n = 10 (3.7%)), the number of participants in the analyses was slightly reduced.
Parental psychopathology (ICD-10-reported diagnostic codes of developmental disorders and psychiatric disorders; F00–F99) reported to the DNPR and DCPR was extracted from the day of their child’s birth to the end of follow-up period, and categorized as a dichotomous variable, whether the diagnosis was reported for the mother, or father, or both.
Analyses
For aim 1, descriptive statistics of participant characteristics (demographic characteristics, ASD subtype, diagnostic history of other developmental disorders, and ID) for delayed ASD were calculated. Continuous variables were described by mean and standard deviation, and categorical variables were described by frequencies and percentages.
For aim 2, descriptive statistics for participant characteristics (the same as the above-mentioned) of the early ASD and no ASD groups were calculated and two sample t-test and chi-square tests were used for group comparisons between delayed ASD and the two other groups. To examine the possible effect of calendar time (Avlund et al. 2020) we analyzed the proportion of delayed cases in two time periods: 2000–2005 and 2006–2010, using the two-sample test of proportions. To explore the associations between demographic and clinical variables at baseline and a delayed ASD diagnosis, a series of multivariate logistic regression models (Odds Ratio (OR), 95% CIs) were estimated. Diagnostic groups (delayed ASD diagnosis vs. either early ASD or no ASD) were the dependent variables and baseline characteristics were the independent variables. Independent variables included baseline diagnostic history (baseline diagnoses other than ASD; ADHD, specific language disorder, and mixed developmental disorder), IQ < 70, parental SES, parental psychiatric history and autism symptoms including ADOS score above/below algorithm cut-off for autism spectrum and domain scores of social reciprocity, social communication, and repetitive rituals and stereotyped behaviors (RRBs). The ADOS analyses could only be applied in children with ADOS included in the initial assessment at baseline. All models were adjusted for age at first assessment, gender and year of referral (calendar year).
All statistical analyses were conducted using the statistical packages STATA version 15.1. Significance level for p-values was set at 0.05. No adjustments for multiple statistical comparisons were made.
Results
Characteristics of Children with a Delayed ASD Diagnosis
The characteristics of children with delayed ASD are shown in Tables 1 and able 2. A total of 74 children were diagnosed with ASD during follow-up, thus representing 8.3% of the total original cohort, 11.9% of all children with an ASD diagnosis, and 21.4% of the children with no ASD at baseline. The mean length of time between first assessment and delayed ASD diagnosis was 7.0 years (range 1.2–14.5 years). Mean age at delayed ASD diagnosis was 12.4 years (SD 4.0); 13.5% of the children with delayed ASD were re-assessed and diagnosed before the age of 7. Among children with delayed ASD, ASD subtypes were represented almost equally, except for Asperger syndrome which was somewhat less frequent than the other subtypes. One third of the delayed ASD cases had an IQ < 70, and ADHD was the most frequent diagnosis given at the initial assessment.
Factors Associated with a Delayed ASD Diagnosis
The characteristics of children with delayed ASD compared to children with early ASD or no ASD are depicted in Table 1 (clinical and demographic characteristics) and Table 2 (ADOS profile). The associations between the independent variables and delayed ASD compared to either early ASD or no ASD, adjusted for age, gender and year of initial assessment, are depicted in Tables 3 and 4. Overall, adjustment had no marked effect on the results compared to unadjusted analyses (Table 5_supplemental and Table 6_supplemental).
Demographic and Clinical Characteristics
There was no difference in age at initial assessment among children in the three ASD case study groups; however, age at follow-up was higher and follow-up time was longer in children with delayed ASD compared to both early and no ASD. Also, year of initial assessment was associated with a delayed ASD diagnosis as 62.2% of delayed ASD cases were assessed in the first half of the baseline period compared to 37.8% in the second half (p = 0.042) (data not shown). Low parental educational level was associated with delayed ASD when compared to early ASD, however, not when compared to no ASD. Psychiatric psychopathology among parents did not differ in the three ASD case status groups (Table 3).
Children with a delayed ASD diagnosis were more likely to have received other developmental or psychiatric disorder diagnoses, except ID, both at baseline and by the end of the follow-up period compared to children with an early ASD diagnosis. A diagnosis of ADHD (at baseline) prior to the ASD diagnosis had the largest risk estimate for delayed ASD compared to early ASD, although risks associated with other diagnoses at baseline in delayed ASD were also high (Table 3). When compared to no ASD, there were no significant differences in diagnoses at baseline except that IQ < 70 at baseline was associated with delayed ASD. At the end of follow-up, emotional disorder was the only diagnosis associated with delayed ASD compared to no ASD. As regards language ability, children with a delayed ASD diagnosis were more likely to be assigned a diagnosis of specific language disorder at baseline, but less likely to be assessed with ADOS module 1 at baseline compared to early ASD. No differences were found in relation to language skills at initial assessment between delayed ASD and no ASD (Tables 3 and 4).
Autism Symptoms
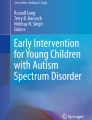
The distribution of ASD subtypes in delayed ASD differed from early ASD, as there was a higher probability of a diagnosis of atypical autism, Asperger syndrome or PDD-NOS in delayed ASD (Table 1). ADOS was used less frequently in delayed ASD at baseline compared to early ASD (60.8% vs. 92.1%, p < 0.001), but compared with no ASD, there was no difference (60.8% vs. 53.7%, p = 0.274). In relation to ADOS total score, 44.4% of delayed ASD cases with ADOS included in the assessment had a score above cut-off compared to 17.8% in no-ASD and 92.1% in early ASD (Fig. 2). In the no ASD baseline group (delayed ASD + no ASD) 43.5% with a score above cut-off on ADOS were later diagnosed with ASD. The odds of being classified as autism on ADOS at baseline based on ADOS total score were lower in delayed ASD compared to early ASD; however, the odds of being classified as autism spectrum were equal (Table 4). In contrast, delayed ASD had higher odds of an ADOS classification of both autism and autism spectrum at baseline based on ADOS total score compared to no ASD. A delayed ASD diagnosis was associated with lower scores on all ADOS domains and almost all items compared to early ASD, and higher scores on ADOS domain and most items compared to no ASD (Table 4).

ADOS classification at initial diagnostic assessment in subgroups. ADOS Autism Diagnostic Observation Schedule, ASD autism spectrum disorder
Discussion
In our population-based cohort of children evaluated for ASD at a young age (referred < 7 years) and then followed up for an average of 11 years, we found that 12% of children with a final ASD diagnosis and 21% of children initially assigned a non-spectrum diagnosis were diagnosed with ASD in later childhood or adolescence, 7.0 years, on average, after initial assessment. Both clinical and demographic factors were associated with a delayed ASD diagnosis. Our hypotheses that autism symptom severity, diagnostic history of other developmental disorders, cognitive ability, and socioeconomic factors were all associated with delayed ASD were confirmed. In addition, year of assessment and the use of ADOS in the assessment were found to be associated with a delayed ASD diagnosis. However, the pattern of differences in these characteristics between delayed ASD and early ASD versus no ASD were quite different. That is, the burden of autism features based on ADOS at an early age in delayed ASD tended to fall between early ASD and no ASD, whereas for the other demographic and clinical features, except for IQ, delayed ASD more closely resembled no ASD than early ASD. In fact, apart from ADOS differences, a greater risk for ID at baseline and a diagnosis of emotional disorders during follow-up were the only distinguishing features between delayed ASD and no ASD.
Diagnostic History and Cognitive Ability
The presence of other developmental and psychiatric disorders at baseline and through follow-up was associated with delayed ASD when compared to early ASD, which was also found in the study by Jónsdóttir et al. (2011). The presence of co-occurring conditions may present a challenge in the recognition of ASD and may delay ASD identification. The overlap between symptoms, especially among young children with milder impairments, has been suggested to contribute to a later diagnosis (Daniels and Mandell 2014; Frenette et al. 2013; Mazurek et al. 2014; Parikh et al. 2018; Simonoff et al. 2008). ADHD was the diagnosis most frequently assigned prior to a delayed ASD diagnosis in the present study, which is in line with several studies that have found that ADHD and developmental delays precede a diagnosis of later ASD (Daniels and Mandell 2014; Davidovitch et al. 2015; Frenette et al. 2013). These results are consistent with a high phenotypic overlap between ASD and ADHD (Sinzig et al. 2009), and shared genetic risk factors in ASD and ADHD (Grove et al. 2019; Parikh et al. 2018; Sinzig et al. 2009). However, ADHD was equally likely in no ASD children; thus, the predictive value of ADHD as identifier of potentially delayed cases may be low.
Specific language disorders have often been shown to precede the diagnosis of ASD (Bacon et al. 2018; Davidovitch et al. 2015; Jónsdóttir et al. 2011; Oien et al. 2018; Parikh et al. 2018). In the present study, one third of children with delayed ASD were assigned a diagnosis of specific language disorder (31%) at initial assessment, with a higher frequency of language disorder diagnoses in delayed ASD compared with early ASD, but no significant difference compared to no ASD. Like ADHD, the predictive value of a diagnosis of language disorder as specific identifier of potentially delayed ASD cases may be low. Results regarding ADOS module number, however, suggest that children with early ASD had more impaired language skills than children in the delayed ASD group. This result is comparable with previous evidence that language impairments in early childhood may increase the chance of an early diagnosis (Bacon et al. 2018; Brett et al. 2016; Brian et al. 2016; Daniels and Mandell 2014).
The fact that emotional disorders were the only disorders distinguishing delayed ASD from no ASD was surprising, although the results may be consistent with the strong genetic overlap between ASD and major depression or neuroticism (Grove et al. 2019). No other studies investigating delayed ASD have examined emotional disorders specifically. However, Lord et al. (2018) states that a late diagnosis of ASD often occurs in the context of co-occurring problems such as anxiety and mood disorders, which corresponds with the high prevalence of co-occurring disorders of anxiety and mood disorder in school-aged children and adolescents with ASD (Lai et al. 2019; Simonoff et al. 2008). In such cases of delayed ASD, referral may be a consequence of un-identified ASD, impaired wellbeing and onset of depressive or anxiety symptoms. In addition, co-occurring anxiety in ASD may intensify autistic symptoms, including social impairments, which may then be associated with the development of depression (Lai et al. 2019).
In the present study, reduced cognitive function was found to be associated with delayed ASD, especially in comparison with no ASD. Previous research regarding the relationship between age at ASD diagnosis and cognitive functioning has shown mixed results (Daniels and Mandell 2014). Higher functioning children may experience significantly greater delays in ASD diagnosis because difficulties in social and language skills may not appear until later in development (Daniels and Mandell 2014; Mazurek et al. 2014). Lower functioning, however, may mask ASD symptoms at initial assessment in younger children (Clark et al. 2018; Frenette et al. 2013), or the ASD symptoms may be interpreted as symptoms of intellectual disability by the clinicians (Pedersen et al. 2017). A final explanation may be a reluctance in diagnosing ASD in children of low mental age. As the ADOS-2 toddler module had not yet been introduced in Denmark at the time of the study (Lord et al. 2013), it could not be used to assess children with a mental age below 18 months, which may have contributed to caution to diagnose ASD in these children. In conclusion, it appears that intellectual functioning may challenge an early ASD diagnosis, especially in children with a variety of other developmental impairments, and therefore may play a particularly important role with regard to the variation in age at diagnosis (Daniels and Mandell 2014; Mazurek et al. 2014; Pedersen et al. 2017). Overall, the results from the present study suggest that it may not be the specific diagnosis prior to the ASD diagnosis that is associated with a delayed diagnosis, but rather the degree of impairment from autism symptoms, symptoms of other developmental disorders, and cognitive ability (i.e. overall symptom load) (Frenette et al. 2013).
Autism Symptoms
The percentage of children with childhood autism was significantly lower in delayed ASD compared to early ASD, and all the other three diagnostic subtypes were significantly more frequent in delayed ASD compared to early ASD. To the best of our knowledge, no previous studies on delayed ASD have reported ASD subtypes; however, in comparison with previous studies examining late ASD we had expected the diagnostic subtypes of Asperger syndrome and PDD-NOS to be the most frequent diagnoses in delayed ASD (Daniels and Mandell 2014) which was not the case in our study. This could indicate that delayed ASD may be somewhat different phenotypically from late ASD with more pronounced autism-like symptoms at an early age in delayed than late ASD.
The main clinical features associated with a delayed ASD diagnosis were autism severity as measured by ADOS; almost half of the children with a delayed ASD diagnosis had an ADOS classification of autism or autism spectrum at initial assessment. Children with a delayed ASD diagnosis had lower scores on ADOS compared to early ASD, and higher compared to no ASD, which were consistent with results from Ozonoff et al. (2018), which confirms our hypothesis that autism symptom severity is associated with a delayed ASD diagnosis. Also, the study by Oien et al. (2018) found delays in social and communicative areas at initial assessment before 18 months, however, Goodwin et al. (2018) and Jónsdóttir et al. (2011) did not find differences in autism symptom severity at initial assessment (Goodwin et al. 2018; Jónsdóttir et al. 2011; Oien et al. 2018). Almost half (44%) of the delayed ASD children examined with ADOS had a score above cut-off, indicating, that these children had symptoms of ASD at baseline, which is comparable with the result from the study by Davidovitch et al. (2015), who found 42% of delayed ASD cases with positive ASD features at baseline. It must be noted, though, that data in Davidovitch et al. (2015) were collected through review of ASD symptoms noted in medical records and not by a structured instrument (Davidovitch et al. 2015) like ADOS as in the present study, which complicates the comparison. In the present study, specific ADOS domains and items revealed no clear association with a delayed ASD diagnosis when compared to either early ASD or no ASD, which corresponds to the result of the ADOS item analysis in the study by Ozonoff et al. (2018). Nevertheless, the results still indicate that ADOS total- and domain scores above cut-off at baseline, despite an initial ASD-negative evaluation, are associated with a delayed ASD diagnosis. In the present study, there were no available data from the medical records which might reveal specific information regarding the clinicians’ decision against ADOS in the cases with an ADOS score above cut-off. The main reason may be that ADOS is only one factor in a thorough assessment and based on review of all the evidence the consensus decision was not ASD (Avlund et al. 2020). An interesting future research focus may be to investigate demographic and clinical characteristics of children with a delayed ASD diagnosis despite a baseline ADOS score above cut-off, and specific reasons affecting clinical decisions in these cases, as it may provide helpful guidelines for clinicians assessing children with suspicion of ASD at a young age. An important note, however, is that half of the children with delayed ASD did not have a score above cut-off on ADOS, indicating that many children may not present clear ASD symptoms at their initial assessment, which is supported by the findings in Davidovitch (2015) and Ozonoff (2018).
Parental Socioeconomic Status and Psychiatric History
Parental educational level was lower for children with delayed ASD compared to early ASD, which is in line with some previous studies on late ASD (Daniels and Mandell 2014; Fountain et al. 2011; Parikh et al. 2018) but not with the study by Davidovitch et al. (2015) investigating delayed ASD. As the children were assessed in young childhood in the present study, early attention was paid to symptoms, and therefore we cannot explain delayed diagnosis in our study as lack of awareness and referral for an evaluation (Daniels and Mandell 2014; Parikh et al. 2018). However, social challenges and problems may be increased in families with lower educational levels, and parents' knowledge of ASD and descriptions of the symptoms of their child may differ from the descriptions which parents with higher education made, which may have influenced the initial diagnostic process. Additionally, we found a relatively high percentage of children with a parental history of psychiatric illness in all three groups (16.2–24.3%), however, no association specifically with a delayed ASD diagnosis. The result corresponds with Frenette et al. (2013) who found that maternal history of psychiatric illness was not associated with age at diagnosis (Frenette et al. 2013). However, Frenette et al. (2013) reported that only 2.6% of children had a maternal history of psychiatric illness. To our knowledge, no other studies have examined the association of parental psychiatric illness and delayed ASD. Thus, the association of a delayed ASD diagnosis and parental socioeconomic status and history of psychiatric illness needs further investigation.
Time Trends
Year of assessment was associated with delayed ASD as more cases of a delayed ASD diagnosis were among children assessed in the early baseline period. Supporting this result, children with a delayed ASD were older at follow-up and had a longer follow-up time than both early ASD and no ASD. The result corresponds to the review by Daniels and Mandell (2014), where most studies investigating age of diagnosis and changes over time found that children who were diagnosed more recently were diagnosed at significantly younger ages. However, adjustment for calendar year of referral (and other covariates) had little effect on associations observed in the multivariate analyses compared to unadjusted analyses. Furthermore, the use of ADOS was much less frequent in delayed ASD compared to early ASD, and ADOS use at the ASD clinic increased across calendar year (Avlund et al. 2020). Thus, not using ADOS in the first assessment may be a contributing factor to delayed ASD. Other less tangible factors contributing to growing clinical awareness around ASD assessments also may have accompanied increased use of the ADOS. The findings suggest that both year of assessment and clinical factors, including use of ADOS and ASD knowledge and awareness, which changed over time contribute to delayed ASD. Although a final diagnosis is based on clinical consensus and not a single test result, using a systematic instrument such as the ADOS in the clinical assessment, along with clinical evaluation, may increase the chance of recognizing the milder and more subtle ASD symptoms and thereby reducing the risk of a delayed ASD diagnosis.
Different Explanations for a Delayed ASD Diagnosis
There may be several reasons for a delayed ASD diagnosis: (1) missed diagnosis: a diagnosis may be missed if clinicians overlook ASD features and fail to diagnose a child with ASD symptoms, (2) clinical caution: a diagnosis may be deferred when clinicians postpone a diagnosis until a later assessment due to e.g. very young mental age and/or ambiguous symptoms, (3) symptom development with age: a diagnosis may be delayed if symptoms have not evolved and become manifest until social demands exceed capacity at a later age, and (4) symptom masking: a diagnosis may be delayed because ASD symptoms are masked or overshadowed by the presence of other developmental diagnoses (American Psychiatric 2013; Davidovitch et al. 2015; Goodwin et al. 2018; Oien et al. 2018; Ozonoff et al. 2018). Based on this study, all of the above explanations may be relevant, however, the relative contribution of each explanation in delayed ASD is not clear. A missed diagnosis may be evident in our observed decrease of delayed cases across time coincident with more frequent use of ADOS. It seems that using systematic standard instruments with the clinical assessment may increase the chance of detecting more subtle symptoms of ASD. In line with this result, the study by Bacon et al. (2018) suggests that differences in age at diagnosis in toddlers may also be due to sensitivity of diagnostic instruments. In relation to ambiguous symptoms at first assessment (clinical caution), we observed that an ADOS score above cut-off but a clinical decision of no ASD diagnosis at first assessment often occurred. In fact, 13.5% of the delayed ASD cases received the ASD diagnosis before the age of 7 in subsequent re-evaluations at the ASD clinic so that the results of the first evaluation may be evidence of clinical caution in those cases. Regarding symptom development with age, it is noteworthy that 56% of children with a delayed ASD diagnosis in this study had an ADOS score below cut-off at baseline. Also, the mean "risk time" for a delayed ASD diagnosis was relatively long (7.0 years), which suggests that a relatively large percentage of children may have developed more ASD symptoms with age. That is, the symptoms may have become clearer as the demands of school and/or social relations increased with age, which corresponds to the mean age of around 12 years of a delayed ASD diagnosis in the present study. Finally, in relation to symptom masking, this may be reflected by the frequent initial diagnoses in delayed ASD of ADHD (69%), specific language disorder (31%) and mixed developmental disorder (27%) given at early ages, and in addition, one third with IQ < 70 at the initial assessment. Also, since the parents and professionals around the child were initially given a different explanation for the child’s difficulties/challenges, request for a re-assessment might only have occurred when the symptoms developed with new or increased challenges that the family were unable to understand or manage.
It is important to note that while a delayed ASD diagnosis may arise in Denmark and elsewhere due to societal stigma or parental fears, this is unlikely to be an important contributing factor for delayed diagnosis in the current study. In our study population children were referred at an early age with developmental delays, after going through services at the primary care level before referral for an autism evaluation and all parents had to actively give their consent before their child was referred. Therefore, we conclude that the present study primarily included parents with less fear of diagnosis.
Strengths and Limitations
To the best of our knowledge, this is the first follow-up study including a large population-based cohort of children assessed in early childhood on suspicion of ASD, and with complete follow-up for diagnoses at least 10 years after the initial assessment. The cohort included children with all ASD subtypes and IQ ranges, thus enhancing generalizability of results to other cohorts. Moreover, data were collected prospectively from medical records and specialist reporting to national registers rather than parent reporting. By adjusting for assessment year in the regression analyses, the challenge of results being biased by calendar time was addressed.
Despite the overall large sample size, the sample of children with a delayed ASD diagnosis was relatively small, although comparable to similar studies (Brian et al. 2016; Clark et al. 2018; Goodwin et al. 2018; Ozonoff et al. 2018). Thus, the power to detect meaningful group differences may have been limited. Also, ADOS was not routinely used throughout the baseline period, especially in the earlier half, and consequently an even smaller number of children were included in the sub-analyses of autism symptom severity measured by ADOS. Another limitation was that children were initially assessed at different ages (between 1 and 7 years), and symptom presentation might have been varying at different ages, but due to sample size limitations it was not possible to compare different age groups at baseline. However, adjustment for age in the multivariate analyses was possible, and it did not change the estimates. Nonetheless, with regard to age and calendar time, a limitation may be that 62.2% of delayed cases had their initial assessment in the early years of the study period when knowledge of ASD and assessment practices were still improving. Finally, we cannot exclude a risk of bias because children and adolescents in the no ASD group had a somewhat shorter follow-up time than the delayed ASD group, although on average children in the no ASD group had more follow-up years (11.5 years) than the mean time for receiving a delayed ASD diagnosis (7.0 years).
Conclusion
The findings from the present study showed that among children assessed at a young age for ASD, 12% of the children with a final ASD diagnosis received a delayed diagnosis. The results also clearly suggest that ASD is present at an early age, albeit to varying degrees of clinical detectability based on clinical tools and practices at the time of the study. Symptom presentation of delayed ASD in early childhood is heterogeneous, and in some children it may not be possible to diagnose ASD until a later age. Based on the results from the current study, it would appear that it is not possible to make a profile of characteristics for a typical delayed ASD case that is clearly distinguishable from both an early ASD diagnosis and no ASD diagnosis, based solely on the clinical and demographic features examined here. Nevertheless, it may be important to recognize that such individuals, who have been identified as ‘at risk’ by virtue of their early age referral for an autism evaluation and possibly other developmental conditions, should be followed over time and also provided with relevant interventions despite the absence of an ASD diagnosis at first referral. Another feature warranting further study was the association of a delayed ASD diagnosis with autism severity as measured by ADOS in which the delayed ASD group scored between early ASD and no ASD groups on most ADOS measures, yet also had other adverse developmental symptoms similar to children with no ASD. If a child has a score close to or above ADOS cut-off, but the total clinical picture indicates no ASD, it may be important to have planned re-evaluations of the child due to risk of being a delayed case. The same is recommended if the child initially is diagnosed with other conditions, especially ADHD, intellectual disability, or language disorder, regardless of ADOS score. Thus, a relevant future research focus would be to develop more sensitive instruments to detect subtle symptoms of ASD, especially in the presence of co-occurring conditions which may overshadow ASD symptoms. In addition, calendar time and accompanying trends in clinical practice including the use of ADOS seemed to lead to a decrease in the frequency of delayed ASD cases; the reduced number of delayed ASD cases in the later years of the study period indicates the value in specialized evaluations and clinicians trained in both a broad ASD assessment and in examining with ADOS. Knowledge of these factors will help clinicians to identify higher risk subgroups and develop additional strategies to reduce ASD diagnostic age in the future, thus increasing the chance of timely intervention and better outcomes.
References
American Psychiatric, A. (1994). Diagnostic and statistical manual of mental disorders: DSM-IV (4th ed.). Washington, DC: American Psychiatric Association.
American Psychiatric, A. (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (5th ed. Arlington ed.): American Psyciatric Publishing.
Andersen, T. F., Madsen, M., Jørgensen, J., Mellemkjoer, L., & Olsen, J. H. (1999). The Danish National Hospital Register. A valuable source of data for modern health sciences. Danish Medical Bulletin, 46(3), 263–268.
Avlund, S. H., Thomsen, P. H., Schendel, D., Jørgensen, M., & Clausen, L. (2020). Time trends in diagnostics and clinical features of young children referred on suspicion of autism: A population-based clinical cohort study, 2000–2010. Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s10803-020-04555-8.
Bacon, E. C., Courchesne, E., Barnes, C. C., Cha, D., Pence, S., Schreibman, L., … Pierce, K. (2018). Rethinking the idea of late autism spectrum disorder onset. Development and psychopathology, 30(2), 553-569. https://doi.org/10.1017/S0954579417001067.
Bickel, J., Bridgemohan, C., Sideridis, G., & Huntington, N. (2015). Child and family characteristics associated with age of diagnosis of an autism spectrum disorder in a tertiary care setting. Journal of Developmental and Behavioral Pediatrics: JDBP, 36(1), 1–7. https://doi.org/10.1097/DBP.0000000000000117.
Brett, D., Warnell, F., McConachie, H., & Parr, J. R. (2016). Factors affecting age at ASD Diagnosis in UK: No evidence that diagnosis age has decreased between 2004 and 2014. Journal of Autism and Developmental Disorders, 46(6), 1974–1984. https://doi.org/10.1007/s10803-016-2716-6.
Brian, J., Bryson, S. E., Smith, I. M., Roberts, W., Roncadin, C., Szatmari, P., & Zwaigenbaum, L. (2016). Stability and change in autism spectrum disorder diagnosis from age 3 to middle childhood in a high-risk sibling cohort. Autism, 20(7), 888–892. https://doi.org/10.1177/1362361315614979.
Clark, M. L. E., Vinen, Z., Barbaro, J., & Dissanayake, C. (2018). School age outcomes of children diagnosed early and later with autism spectrum disorder. Journal of Autism and Developmental Disorders, 48(1), 92–102. https://doi.org/10.1007/s10803-017-3279-x.
Dalsgaard, S., Thorsteinsson, E., Trabjerg, B. B., Schullehner, J., Plana-Ripoll, O., Brikell, I., … Pedersen, C. B. (2019). Incidence rates and cumulative incidences of the full spectrum of diagnosed mental disorders in childhood and adolescence. JAMA Psychiatry, 77(2), 155–164. https://doi.org/10.1001/jamapsychiatry.2019.3523.
Daniels, A. M., & Mandell, D. S. (2014). Explaining differences in age at autism spectrum disorder diagnosis: A critical review. Autism, 18(5), 583–597. https://doi.org/10.1177/1362361313480277.
Davidovitch, M., Levit-Binnun, N., Golan, D., & Manning-Courtney, P. (2015). Late diagnosis of autism spectrum disorder after initial negative assessment by a multidisciplinary team. Journal of Developmental and Behavioral Pediatrics: JDBP, 36(4), 227–234. https://doi.org/10.1097/DBP.0000000000000133.
Fountain, C., King, M. D., & Bearman, P. S. (2011). Age of diagnosis for autism: Individual and community factors across 10 birth cohorts. Journal of Epidemiology and Community Health, 65(6), 503–510. https://doi.org/10.1136/jech.2009.104588.
Frenette, P., Dodds, L., MacPherson, K., Flowerdew, G., Hennen, B., & Bryson, S. (2013). Factors affecting the age at diagnosis of autism spectrum disorders in Nova Scotia, Canada. Autism, 17(2), 184–195. https://doi.org/10.1177/1362361311413399.
Goodwin, A., Matthews, N. L., & Smith, C. J. (2018). Parent-reported early symptoms of autism spectrum disorder in children without intellectual disability who were diagnosed at school age. Autism,. https://doi.org/10.1177/1362361318777243.
Grove, J., Ripke, S., Als, T. D., Mattheisen, M., Walters, R. K., Won, H., … Børglum, A. D. (2019). Identification of common genetic risk variants for autism spectrum disorder. Nat Genet, 51(3), 431–444. https://doi.org/10.1038/s41588-019-0344-8.
Grzadzinski, R., Dick, C., Lord, C., & Bishop, S. (2016). Parent-reported and clinician-observed autism spectrum disorder (ASD) symptoms in children with attention deficit/hyperactivity disorder (ADHD): implications for practice under DSM-5. Molecular Autism. eCollection 2016. https://doi.org/10.1186/s13229-016-0072-1.
Helt, M., Kelley, E., Kinsbourne, M., Pandey, J., Boorstein, H., Herbert, M., & Fein, D. (2008). Can children with autism recover? If so, how? Neuropsychology Review, 18(4), 339–366. https://doi.org/10.1007/s11065-008-9075-9.
Jensen, C. M., Steinhausen, H. C., & Lauritsen, M. B. (2014). Time trends over 16 years in incidence-rates of autism spectrum disorders across the lifespan based on nationwide Danish register data. Journal of Autism and Developmental Disorders, 44(8), 1808–1818. https://doi.org/10.1007/s10803-014-2053-6.
Jónsdóttir, S. L., Saemundsen, E., Antonsdóttir, I. S., Sigurdardóttir, S., & Ólason, D. (2011). Children diagnosed with autism spectrum disorder before or after the age of 6 years. Research in Autism Spectrum Disorders, 5(1), 175–184. https://doi.org/10.1016/j.rasd.2010.03.007.
Lai, M. C., Kassee, C., Besney, R., Bonato, S., Hull, L., Mandy, W., … Ameis, S. H. (2019). Prevalence of co-occurring mental health diagnoses in the autism population: a systematic review and meta-analysis. The Lancet Psychiatry, 6(10), 819–829.
Lauritsen, M. B., Jørgensen, M., Madsen, K. M., Lemcke, S., Toft, S., Grove, J., … Thorsen, P. (2010). Validity of childhood autism in the danish psychiatric central register: Findings from a Cohort sample born 1990–1999. Journal of Autism and Developmental Disorders, 40(2), 139–148. https://doi.org/10.1007/s10803-009-0818-0.
Lord, C., Elsabbagh, M., Baird, G., & Veenstra-Vanderweele, J. (2018). Autism spectrum disorder. Lancet (London, England), 392(10146), 508–520.
Lord, C., Risi, S., Lambrecht, L., Cook Jr, E. H., Leventhal, B. L., Dilavore, P. C., … Rutter, M. (2000). The autism diagnostic observation schedule-generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30(3), 205–223. https://doi.org/10.1023/A:1005592401947.
Lord, C., Rutter, M., Dilavore, P. C., Risi, S., Gotham, K., & Bishop, S. L. (2013). Autism Diagnostic Observation Schedule 2nd ed. (ADOS-2). Danish version.
Mazurek, M. O., Handen, B. L., Wodka, E. L., Nowinski, L., Butter, E., & Engelhardt, C. R. (2014). Age at first autism spectrum disorder diagnosis: The role of birth cohort, demographic factors, and clinical features. Journal of Developmental and Behavioral Pediatrics: JDBP, 35(9), 561–569. https://doi.org/10.1097/DBP.0000000000000097.
Mors, O., Perto, G. P., & Mortensen, P. B. (2011). The Danish psychiatric central research register. Scandinavian Journal of Public Health, 39(7 Suppl), 54–57. https://doi.org/10.1177/1403494810395825.
Mullen, E. M. (1995). Mullen scales of early learning (MSEL). Circle Pines, MN: American Guidance Service.
Oien, R. A., Schjolberg, S., Volkmar, F. R., Shic, F., Cicchetti, D. V., Nordahl-Hansen, A., … Chawarska, K. (2018). Clinical features of children with autism who passed 18-month screening. Pediatrics, 141(6), https://doi.org/10.1542/peds.2017-3596.
Ozonoff, S., Young, G. S., Brian, J., Charman, T., Shephard, E., Solish, A., & Zwaigenbaum, L. (2018). Diagnosis of autism spectrum disorder after age 5 in children evaluated longitudinally since infancy. Journal of the American Academy of Child and Adolescent Psychiatry, 57(11), 849-857.e842.
Parikh, C., Kurzius-Spencer, M., Mastergeorge, A. M., & Pettygrove, S. (2018). Characterizing health disparities in the age of autism diagnosis in a study of 8-year-old children. Journal of Autism and Developmental Disorders, 48(7), 2396–2407. https://doi.org/10.1007/s10803-018-3500-6.
Parner, E. T., Schendel, D. E., & Thorsen, P. (2008). Autism prevalence trends over time in Denmark: Changes in prevalence and age at diagnosis. Archives of Pediatrics & Adolescent Medicine, 162(12), 1150–1156. https://doi.org/10.1001/archpedi.162.12.1150.
Pedersen, A. L., Pettygrove, S., Lu, Z., Andrews, J., Meaney, F. J., Kurzius-Spencer, M., … Cunniff, C. (2017). DSM criteria that best differentiate intellectual disability from autism spectrum disorder. Child Psychiatry & Human Development, 48(4), 537-545. https://doi.org/10.1007/s10578-016-0681-0.
Pedersen, C. B. (2011). The Danish civil registration system. Scandinavian Journal of Public Health, 39(7 Suppl), 22–25. https://doi.org/10.1177/1403494810387965.
Schendel, D. E., & Thorsteinsson, E. (2018). Cumulative Incidence of autism into adulthood for birth cohorts in Denmark, 1980–2012. JAMA, 320(17), 1811–1813. https://doi.org/10.1001/jama.2018.11328.
Sheldrick, R. C., Maye, M. P., & Carter, A. S. (2017). Age at first identification of autism spectrum disorder: An analysis of two US Surveys. Journal of the American Academy of Child and Adolescent Psychiatry, 56(4), 313–320.
Simonoff, E., Pickles, A., Charman, T., Chandler, S., Loucas, T., & Baird, G. (2008). Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child and Adolescent Psychiatry, 47(8), 921–929. https://doi.org/10.1097/CHI.0b013e318179964f.
Sinzig, J., Walter, D., & Doepfner, M. (2009). Attention deficit/hyperactivity disorder in children and adolescents with autism spectrum disorder: Symptom or syndrome? Journal of Attention Disorders, 13(2), 117–126.
Snijders, J. T., Tellegen, P. J., & Laros, J. A. (1997). Snijders-Oomen Nonverbaler Intelligenztest SON-R 5.5-17. Göttingen: Hogrefe.
Thygesen, L. C., Daasnes, C., Thaulow, I., & Brønnum-Hansen, H. (2011). Introduction to Danish (nationwide) registers on health and social issues: Structure, access, legislation, and archiving. Scandinavian Journal of Public Health, 39(7 Suppl), 12–16. https://doi.org/10.1177/1403494811399956.
Undervisningsministeriet. (2020). Det ordinære uddannelsessystem i Danmark (Ministry of Eduation). Retrieved from https://www.uvm.dk/uddannelsessystemet/overblik-over-det-danske-uddannelsessystem/det-ordinaere-uddannelsessystem.
Wechsler, D. (1991). Wechsler intelligence scale for children (3rd ed.). San Antonio, TX: Psychological Corporation.
Wechsler, D. (2002). Wechsler preschool and primary scale of intelligence (3rd ed.). San Antonio, TX: Psychological Corporation.
Wiggins, L. D., Baio, J., & Rice, C. (2006). Examination of the time between first evaluation and first autism spectrum diagnosis in a population-based sample. Journal of Developmental and Behavioral Pediatrics, 27(2 Suppl), S79-87. https://doi.org/10.1097/00004703-200604002-00005.
World Health Organisation. (1992). The ICD-10 Classification of Mental Health and Behavioral Disorders. Diagnostic criteria for research. Geneva: World Health Organisation.
Acknowledgments
The authors would like to thank Emilie Riis Kjeldsen and Katrine Jaquet Mavraganis for assistance in the data collection process, and Astrid Voldstedt Lund Høy for reviewing cognitive test results. All authors contributed to the study conception, design and interpretation of results. Data collection and analyses were performed by Sara Højslev Avlund. The first draft of the manuscript was written by Sara Højslev Avlund and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
None of the authors have any financial or personal relationships with people or organizations that could influence the work of this article. This work was supported by Aarhus University Hospital, Psychiatry, Department of Child- and Adolescent Psychiatry, and by grants from the Research Fund of Child and Adolescent Psychiatry, Central Denmark Region, Denmark, the Sofie Foundation, Butcher Wörzner and Wife Memorial Fund, and Mrs C. Hermansen Memorial Fund. The funders had no involvement in any aspects of the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that the present paper was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Avlund, S.H., Thomsen, P.H., Schendel, D. et al. Factors Associated with a Delayed Autism Spectrum Disorder Diagnosis in Children Previously Assessed on Suspicion of Autism. J Autism Dev Disord 51, 3843–3856 (2021). https://doi.org/10.1007/s10803-020-04849-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-020-04849-x