
Abstract
Deficits in emotion regulation (ER) are commonly observed in individuals with ASD and may contribute to elevated rates of psychiatric comorbidity. The objective of this study was to understand the relationship between ER (self-and caregiver-reported) and clinician-assigned mood and anxiety disorders in emerging adults with ASD (n = 27). Individuals with an anxiety or mood disorder demonstrated significantly greater involuntary engagement (IE) for ER than those without an anxiety or unipolar depression diagnosis. Furthermore, those without anxiety or depression reported significantly more voluntary engagement (VE). However, consistent with prior findings outside of ASD, IE appears closely associated with internalizing diagnoses, even when VE is also utilized. Research on clinical approaches to reduce reliance on involuntary approaches to emotion management should be pursued.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Autism spectrum disorder (ASD) is a neurodevelopmental disorder associated with difficulties in social communication and the presence of restricted or repetitive movements or behaviors (American Psychiatric Association 2013). Approximately one in 59 children was diagnosed with ASD in 2014, and prevalence has steadily increased since 2000 (Baio et al. 2018). ASD is a lifelong disorder, meaning that the associated symptoms last into adulthood for most individuals (Smith et al. 2013). In addition to the developmental difficulties that those with ASD face in relation to the disorder, at least half of ASD youth also meet criteria for at least one other psychiatric disorder (Salazar et al. 2015).
Mood and anxiety disorders are among the most common comorbidities in those with ASD (Lugnegard et al. 2011). The prevalence of anxiety disorders across the developmental trajectory has been established by a number of studies to be in the range of 40–60% (Maddox and White 2015; van Steensel et al. 2011; White et al. 2009). Anxiety disorders are closely linked to core symptoms of ASD, are persistent throughout the lifespan, and often adversely impact quality of life (Howlin et al. 2004; Wood and Gadow 2010). Although depressive symptoms in ASD have been studied relatively less frequently, available evidence suggests that these symptoms are similarly prevalent; although estimates vary widely, figures as high as 47% have been reported (Wigham et al. 2017).
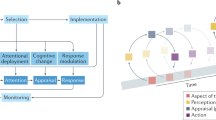
Deficits in one’s ability to manage intense emotion are thought to be a common mechanism across mood and anxiety problems (Mazefsky et al. 2013). Emotion regulation (ER) refers to the management of one’s reactions to everyday thoughts and events, as well as strategies implemented to either increase, decrease, or maintain one’s felt and expressed emotion. ER strategies can be conceptualized based on two continua: the degree to which the strategy is voluntary (versus passive) and the degree to which it involves approach-based engagement (versus withdrawal). This conceptualization yields four quadrants into which strategies can be grouped: voluntary engagement (VE), voluntary disengagement (VD), involuntary engagement (IE), and involuntary disengagement (ID; Connor-Smith et al. 2000). Voluntary strategies are thought of as “controlled responses,” as the use of such strategies is by one’s own will (Silk et al. 2003). Conversely, involuntary responses, also known as “automatic responses,” are not performed volitionally (Silk et al. 2003). Furthermore, engagement refers to actively approaching the stressful situation, while disengagement refers to passively separating oneself from the stressful situation (Silk et al. 2003).
VE strategies, such as problem solving and emotional control, are thought to be adaptive, while IE strategies (e.g., intrusive thoughts, physiological arousal) are generally, though not uniformly, thought to be maladaptive. Although most scholars agree that no single strategy is pathological and, rather, inflexibility or inability to call upon various strategies is sometimes problematic (Aldao et al. 2015), the use of VE techniques has been associated with lower levels of psychopathology (Mazefsky et al. 2014). Conversely, IE strategies are observed more frequently in individuals with multiple psychiatric disorders. More specifically, Gotham et al. (2014) found that rumination, an IE strategy, was positively correlated with depressive symptoms in a sample of adults with ASD. Likewise, Aldao et al. (2010) meta-analysis found significant positive associations between rumination and avoidance and depression and anxiety in clinical and nonclinical samples. Not only are involuntary ER strategies correlated with the presence of comorbidities in those with ASD, but they are also related to the chronicity of the additional disorders (Salters-Pedneault et al. 2006). Salters-Pedneault et al. (2006) noted that poorer ER, including use of IE strategies, contributes to the maintenance of depressive symptoms because of the resulting longer and more severe periods of distress. Additionally, an inability to flexibly implement ER strategies has been proposed to contribute to the emergence and persistence of internalizing symptoms (Kashdan and Rottenberg 2010). Inflexible deployment of ER strategies may be highly prevalent among individuals with ASD given well-documented difficulties with executive functioning in that population (Cai et al. 2018; Happé et al. 2006).
Extant literature suggests that use of maladaptive ER strategies is prevalent among individuals with ASD, and that use of these strategies may be associated with high rates of internalizing symptoms (Mazefsky et al. 2014). However, prior research has not examined clinically ascertained mood and anxiety disorders in relation to ER, relying instead on use of dimensional caregiver-and self-report measures. Utilizing clinician diagnoses helps reduce reporter bias, allows one to more adeptly address specificity in expressed symptoms, and enables the investigation of symptoms with established clinically significant impairment. Additionally, ER and comorbidity have not been thoroughly explored in young adults with ASD that are going through major transitions, such as enrolling in postsecondary school. Emerging adulthood, generally thought to extend from late teens through approximately age 25, has been established as a unique developmental period during which individuals undergo substantial changes that may affect overall mental health (Arnett 2000, 2007). Use of maladaptive ER strategies may be particularly problematic for individuals in this developmental period because of the abundance of life transitions, including graduating secondary school and adjusting to self-advocacy for services (White et al. 2017).
The relative import of adaptive versus maladaptive ER strategies as contributors to psychopathology in the ASD population remain unknown. Aldao et al. (2010) asserted that the effects of ER strategies are asymmetrical. Specifically, adaptive strategies, such as reappraisal, have evidenced relatively weaker negative associations with symptoms than the positive association between maladaptive strategies and psychopathology (Aldao et al. 2010). Another study identified a moderating effect wherein a significant association between adaptive strategies and psychopathology existed only when high levels of maladaptive strategies were used (Aldao and Nolen-Hoeksema 2012). Consideration of an individual’s baseline utilization of adaptive versus maladaptive ER strategies might therefore inform treatment focused on increasing or mitigating use of adaptive and maladaptive strategies, respectively (Conklin et al. 2015). Only one study has explored how the relative use of maladaptive and adaptive strategies are associated with psychopathology. Cai et al. (2018) found that high suppression (generally considered maladaptive) is still associated with positive outcomes and low depression when there is also high reappraisal (generally considered adaptive). However, this study focused only on two specific strategies—namely suppression and reappraisal. Research on the relative use of adaptive versus maladaptive ER strategies, in relation to psychopathology in ASD, is warranted.
The current study therefore had two aims. First, we intended to establish the association between maladaptive ER strategies and the presence of confirmed, clinical diagnoses of anxiety and/or unipolar depression in emerging adults with ASD. Second, we aimed to conduct a preliminary exploration into the effect on different patterns of VE (typically adaptive) and IE (typically maladaptive) ER on internalizing and externalizing symptoms. We hypothesized that elevated maladaptive ER strategies would be associated with greater levels of psychopathology; we also predicted that use of adaptive strategies would mitigate the impact of maladaptive strategies as contributors to psychopathology.
Method
Participants
The current study was approved by the university’s institutional review board. Participants under the age of 18 provided informed assent and caregivers and participants over the age of 18 provided informed consent. Participants were recruited in a rural region of the mid-Atlantic United States through ASD-specific listservs and newsletters, community advertisements, and university-affiliated clinics. Inclusion criteria specified that participants must be between 16 and 25 years old, have average or better cognitive ability (i.e., FSIQ ≥ 85), and be free from severe psychopathology warranting immediate treatment (e.g., active psychosis, acute suicidality).
The sample for the current study consisted of 27 participants ranging in age from 16 to 24 years (M = 18.54, SD = 2.02). The sample was predominantly male (74%) and White (89%). All participants met diagnostic criteria for ASD, which was confirmed by the Autism Diagnostic Observation Schedule-Second Edition (ADOS-2; Lord et al. 2012; n = 20) or, if the person was in school with an active individualized education plan (IEP), with primary disability classification of autism (n = 7). Individuals were of approximately average cognitive ability (M = 103.88, SD = 10.67) based on the Wechsler Abbreviated Scale of Intelligence, Second Edition (WASI-II; Wechsler 2011), and intellectual disability was an exclusion criterion. Some participants were identified, by caregivers or themselves via self-report, as having co-occurring psychiatric disorders (see Table 1). However, participants were not recruited or selected on the basis of anxiety or mood disturbance. Although the rate of anxiety diagnoses is high, recent work has identified prevalence as high as 50% in community samples of adults with ASD (Maddox and White 2015). Given that the current analyses were carried out with a treatment-seeking sample, even higher prevalence of psychiatric comorbidity was expected (Tables 2, 3).
Measures
Anxiety Disorders Interview Schedule (ADIS-C/P; Silverman and Albano 1996)
The ADIS-C/P was administered by a research-reliable clinician to all participants still in secondary school and living with their caregivers, while the ADIS client version (ADIS-5) was administered to participants who had graduated from secondary school. The ADIS was used to identify comorbid disorders and as a means of ruling out severe psychopathology (e.g., active psychosis, depression with acute suicidality) that warranted immediate treatment and served as an exclusion criterion for the current study. Although the full ADIS-C/P or ADIS-5 was administered, only mood and anxiety disorder diagnoses were examined in the current study. All clinicians administering ADIS-C/P and ADIS-5 interviews were advanced doctoral students who had been trained to reliability, and they were closely supervised by a board-certified licensed psychologist.
Response to Stress Questionnaire (RSQ; Connor-Smith et al. 2000)
The RSQ is a 57-item caregiver-and self-report measure indexing a variety of adaptive and maladaptive ER strategies. The measure asks participants to recall stressful social experiences they have encountered and provide ratings of the ways in which they might respond. Reliability and validity of the RSQ in ASD samples has been previously established (Mazefsky et al. 2014). The VE and IE subscales were utilized in the current study, each of which demonstrated excellent reliability in our sample (α = .86 and α = .83, respectively).
Child Behavior Checklist (CBCL; Achenbach and Rescorla 2001)
The CBCL and its adult counterpart, the ABCL, were utilized as dimensional indicators of internalizing and externalizing symptomatology. Both part of the Achenbach System of Empirically Based Assessment (ASEBA), the ABCL and CBCL have been widely validated and are commonly used in ASD samples (Pandolfi et al. 2012). Both the CBCL and the ABCL demonstrated excellent reliability in our sample (α = .95 and α = .94, respectively).
Procedure
Participants were enrolled in a randomized controlled trial to evaluate the feasibility and preliminary efficacy of a college transition program for students with ASD (White et al. 2017). The program aimed to address transition-related issues among two distinct samples. One sample included students still in secondary school, preparing for the transition to postsecondary education, and the other sample consisted of students already matriculated in postsecondary settings. Caregiver participation in the transition program differed between these two samples. For secondary school students, caregivers were actively involved in the treatment process and attended the majority of treatment sessions. Caregivers of students in postsecondary settings reported on their perception of their child’s symptoms, but did not actively participate in treatment in order to promote autonomy and self-determination (White et al. 2017). While data was collected at several time points throughout the program, the current study only analyzed pre-treatment data.
Analytic Plan
All statistical analyses were conducted using IBM SPSS Statistics Version 25 (IBM 2017). Descriptive statistics were calculated for all variables and Pearson correlations were utilized to determine associations between variables of interest. Independent samples t-tests were used to compare the differences in mean IE and VE scores between participants with an anxiety or unipolar depression disorder diagnosis, and those without. Due to the small sample size, directional hypotheses, and the exploratory nature of our study, p values were not corrected for multiple comparisons. We also conducted multiple linear regression to determine if internalizing symptomology was predicted by caregiver-and/or self-reported IE.
To examine our second aim related to the impact of different patterns of VE versus IE strategies, we performed a median split on standardized caregiver-reported RSQ scores to derive two groups (below/above the sample median, hereafter referred to as “low” and “high” respectively). Therefore, participants were categorized into four groups: high IE/high VE (n = 7), high IE/low VE (n = 4), low IE/high VE (n = 6), and low IE/low VE (n = 9). These four groups did not significantly differ on the basis of age, F(3, 20) = .155, p = .93. A one-way ANOVA was used to determine the differences in mean internalizing and externalizing T scores between the four ER groups. Post-hoc tests examined pairwise comparisons across the four groups.
Results
Concerning our first hypothesis, results of an independent samples t-test indicated that individuals with any DSM-5 anxiety disorder demonstrated significantly greater self-reported IE than those without an anxiety disorder diagnosis [t(21) = − 3.11, p = .005]. Those with anxiety disorders self-reported significantly lower VE, [t(21) = 2.11, p = .047] than those without. Caregiver-report scores of IE [t(21) = − 1.72, p = .101] and VE [t(21) = .37, p = .714] did not significantly differ between those with and without anxiety disorder diagnoses.
There was a significant difference between youth with a unipolar depressive disorder (i.e., major depressive disorder, persistent depressive disorder) and those without in self-report of VE, [t(21) = 2.58, p = .017] and IE, [t(21) = − 2.87, p = .009]. Those with unipolar depression self-reported significantly less VE and significantly more IE than those without. Again, caregiver-report of IE, [t(21) = − .72, p = .483] and VE, [t(21) = − .65, p = .524] did not differ between participants with and without unipolar depression.
Self-reported VE was not significantly associated with either internalizing, [r(25) = − .34, p = .094] or externalizing, [r(25) = − .20, p = .332] symptomology. Similarly, associations between self-reported IE and internalizing symptomology, [r(25) = .21, p = .302] and externalizing symptomology, [r(25) = .002, p = .991] were not statistically significant. Caregiver-report of IE was significantly and positively correlated with caregiver-report of both internalizing, [r(25) = .63, p = .001] and externalizing symptomology, [r(25) = .48, p = .014]. However, caregiver-reported VE was not significantly associated with either internalizing, [r(25) = − .29, p = .149] or externalizing, [r(25) = − .35, p = .08] symptomatology.
Results of a one-way ANOVA showed that the four ER groups significantly differed on caregiver-reported internalizing, [F(3) = 8.13, p = .001] and externalizing symptomology [F(3) = 4.55, p = .013]. The results of Tukey post-hoc tests (see Table 4) revealed that the low IE/high VE group had significantly lower internalizing T scores than the high IE/low VE group (p < .001) and the high IE/high VE group (p = .020). Furthermore, the low IE/low VE group had significantly lower internalizing T scores than the high IE/low VE group (p = .037). Regarding externalizing T scores, the low IE/high VE group had significantly lower externalizing T scores than both the low IE/low VE group (p = .012) and the high IE/high VE group (p = .035). A parallel one-way ANOVA with self-reported internalizing and externalizing symptoms was not conducted given that the relevant ASEBA measures (i.e., YSR and/or ASR) were not collected from the sample.
Discussion
We endeavored to examine associations between voluntary and involuntary ER strategies, dimensional measures of internalizing and externalizing symptomatology, and clinical diagnoses of anxiety disorders and unipolar depression in emerging adults with ASD. Results align with prior work in this area in demonstrating significant associations between use of involuntary strategies, but not voluntary ER strategies, and both internalizing and externalizing symptoms (Mazefsky et al. 2014). Our findings are novel in their identification of this pattern in a sample of older adolescents and young adults, a developmental period associated with increased prevalence of mood disorders (Merikangas et al. 2010). Although ER abilities in typically developing youth improve throughout late adolescence and into early adulthood (Zimmerman and Iwanski 2014), this may not be the case for individuals with ASD. Young adults with ASD may be particularly vulnerable to the effects of under-developed ER strategies (Elias and White 2018), which may place them at heightened risk for secondary psychopathology. These results also extend prior research on psychiatric symptom differences by confirming similar patterns of ER differences in individuals with versus without confirmed clinical anxiety and depression diagnoses.
Results provide preliminary evidence that use of adaptive, voluntary ER strategies do not protect against the negative impact of IE on internalizing and externalizing symptoms. This varies from results of a recent study that suggested the habitual use of reappraisal acts as a buffer for habitual suppression in an ASD sample (Cai et al. 2018). The notion of voluntary ER not serving as a protective factor is supported by results demonstrating greater levels of psychopathology among those with both high VE and IE than those with high VE but low IE. Additionally, VE on its own was not associated with lower levels of internalizing or externalizing symptoms. These results are consistent with prior work examining ER in adults without ASD (Conklin et al. 2015) and expand upon previous findings by replicating the pattern in a sample of individuals with ASD. Although data analyzed in the current study did not allow for nuanced explorations of the use of these strategies, different strategies may be deployed based on the severity, regularity, or predictability of the stressor. A recent meta-analysis evaluating the effect of coping flexibility on psychological adjustment identified a small-to-moderate mean effect, moderated by such contextual factors as age and individualistic culture, but not socioeconomic status (Cheng et al. 2014). There exists a clear need for future work to examine these questions, as well as conduct longitudinal studies to explore the directionality of the relationship between difficulty with ER and emergence of psychopathology.
This study’s findings offer clear implications for interventions focused on comorbid psychopathology in adults with ASD. Recent work has proposed that identification of an individual’s predominant coping strategies at the outset of treatment may inform a focus on mitigation of maladaptive strategies or encouragement of adaptive strategies. Evidence suggests the former may be useful in all cases, while the latter may be particularly important for individuals who rely heavily on use of maladaptive strategies (Conklin et al. 2015). At least one intervention recently developed for individuals with ASD has aimed to address ER deficits as a transdiagnostic construct (Conner et al. 2018). In this and other interventions, the relative emphasis placed on altering specific strategies should be informed by evaluation of the individual’s predominant coping style, thus taking a more individualized approach to treatment of comorbid psychopathology in ASD.
Although the results of the current study contribute to our knowledge of ER strategies and comorbid symptomatology in adults with ASD, a number of factors may limit the generalizability of our findings. First, our sample size was too small to examine the impact of adaptive and maladaptive ER strategies present at more severe levels. Analyses with individuals in the top and bottom quartile of IE/VE scores, rather than above and below the medians, may have provided more insight into these relationships. We also elected not to examine covariates, such as age and gender, in order to retain statistical power. However, our groups did not differ significantly on the basis of age or gender, and age was not significantly correlated with either IE or VE. Therefore, we have a strong expectation that our pattern of results would not be altered by the inclusion of these demographic characteristics as covariates.
Our pattern of results also demonstrated several discrepancies between caregiver- and self-reported internalizing and externalizing symptoms. Self-reported use of ER strategies differed between those with and without anxiety and depressive disorders, while caregiver-reported use of strategies did not. Differences in internalizing and externalizing symptomology among the four high/low VE and IE groups were also significant based on caregiver-report, but not self-report, data. Assessment of the association between ER impairment and comorbid psychopathology in ASD may also be complicated by difficulty associated with self-report of ER difficulties. Deficient reporting on internal states, and ER specifically, in ASD is well documented (Berthoz and Hill 2005). However, given the nature of our sample (i.e., average cognitive ability and considering or enrolled in postsecondary education), a significant proportion of our sample may have been able to accurately report on their own internal states. Recent work has also identified moderate to strong correlations between self- and caregiver-report of subjective and internalizing symptoms such as anxiety and quality of life (Hong et al. 2016; Smith et al. 2019). Discrepancies between self- and caregiver-reported data may themselves be informative and reflect distinct, yet comparably valid, viewpoints on internalizing symptoms and ER strategies (Mazefsky et al. 2014).
Despite these limitations, however, the results offer meaningful implications for the study of ER in ASD and for intervention research. Further examination of the use of VE versus IE strategies in varying contexts is warranted, as well as explorations of the contribution of each to psychopathology longitudinally. Practically, our results suggest that interventionists should note the extent to which use of ER strategies—both maladaptive and adaptive—may precipitate or perpetuate psychiatric symptoms in individuals with ASD.
References
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms and profiles. Burlington: University of Vermont, Research Center for Children, Youth, and Families.
Aldao, A., & Nolen-Hoeksema, S. (2012). When are adaptive strategies most predictive of psychopathology? Journal of Abnormal Psychology, 121(1), 276. https://doi.org/10.1037/a0023598.
Aldao, A., Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30, 217–237. https://doi.org/10.1016/j.cpr.2009.11.004.
Aldao, A., Sheppes, G., & Gross, J. J. (2015). Emotion regulation flexibility. Cognitive Therapy and Research, 39, 263–278. https://doi.org/10.1007/s10608-014-9662-4.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th edn.). Washington, DC: American Psychiatric Association.
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55(5), 469. https://doi.org/10.1037/0003-066X.55.5.469.
Arnett, J. J. (2007). Emerging adulthood: What is it, and what is it good for? Child Development Perspectives, 1(2), 68–73. https://doi.org/10.1111/j.1750-8606.2007.00016.x.
Baio, J., Wiggins, L., Christensen, D. L., Maenner, M. J., Daniels, J., Warren, Z.,… Dowling, N. F. (2018). Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network 11 sites, United States, 2014. Surveillance Summaries, 67(6), 1–23. https://doi.org/10.15585/mmwr.ss6706a1.
Berthoz, S., & Hill, E. L. (2005). The validity of using self-reports to assess emotion regulation abilities in adults with autism spectrum disorder. European Psychiatry, 20(3), 291–298. https://doi.org/10.1016/j.eurpsy.2004.06.013.
Cai, R. Y., Richdale, A. L., Dissanayake, C., Trollor, J., & Uljarević, M. (2018). Emotion regulation in autism: Reappraisal and suppression interactions. Autism. https://doi.org/10.1177/1362361318774558.
Cheng, C., Lau, H. P., & Chan, M. P. (2014). Coping flexibility and psychological adjustment to stressful life changes: A meta-analytic review. Psychological Bulletin, 140(6), 1582–1607. https://doi.org/10.1037/a0037913.
Conklin, L. R., Cassiello-Robbins, C., Brake, C. A., Sauer-Zavala, S., Farchione, T. J., Ciraulo, D. A., & Barlow, D. H. (2015). Relationships among adaptive and maladaptive emotion regulation strategies and psychopathology during the treatment of comorbid anxiety and alcohol use disorders. Behaviour Research and Therapy, 73, 124–130. https://doi.org/10.1016/j.brat.2015.08.001.
Conner, C. M., White, S. W., Beck, K. B., Golt, J., Smith, I. C., & Mazefsky, C. A. (2018). Improving emotion regulation ability in autism: The emotional awareness and skills enhancement (EASE) program. Autism. https://doi.org/10.1177/1362361318810709.
Connor-Smith, J. K., Compas, B. E., Wadsworth, M. E., Thomsen, A. H., & Saltzman, H. (2000). Response to stress in adolescence: Measurement of coping and involuntary stress responses. Journal of Consulting and Clinical Psychology, 68(6), 976–992. https://doi.org/10.1037/0022-006X.68.6.976.
Elias, R., & White, S. W. (2018). Autism goes to college: Understanding the needs of a student population on the rise. Journal of Autism and Developmental Disorders, 48(3), 732–746. https://doi.org/10.1007/s10803-017-3075-7.
Gotham, K., Bishop, S. L., Brunwasser, S., & Lord, C. (2014). Rumination and perceived impairment associated with depressive symptoms in a verbal adolescent-adult ASD sample. Autism Research, 7, 381–391. https://doi.org/10.1002/aur.1377.
Happé, F., Booth, R., Charlton, R., & Hughes, C. (2006). Executive function deficits in autism spectrum disorders and attention-deficit/hyperactivity disorder: Examining profiles across domains and ages. Brain and Cognition, 61(1), 25–39. https://doi.org/10.1016/j.bandc.2006.03.004.
Hong, J., Bishop-Fitzpatrick, L., Smith, L. E., Greenberg, J. S., & Mailick, M. R. (2016). Factors associated with subjective quality of life of adults with autism spectrum disorder: Self-report versus maternal reports. Journal of Autism and Developmental Disorders, 46(4), 1368–1378. https://doi.org/10.1007/s10803-015-2678-0.
Howlin, P., Goode, S., Hutton, J., & Rutter, M. (2004). Adult outcome for children with autism. Journal of Child Psychology and Psychiatry and Allied Disciplines, 45(2), 212–229. https://doi.org/10.1111/j.1469-7610.2004.00215.x.
Kashdan, T. B., & Rottenberg, J. (2010). Psychological flexibility as a fundamental aspect of health. Clinical Psychology Review, 30(7), 865–878. https://doi.org/10.1016/j.cpr.2010.03.001.
Lord, C., Rutter, M., DiLavore, P. C., Risi, S., Gotham, K., & Bishop, S. (2012). Autism Diagnostic Observation Schedule (2nd edn.). Torrance: Western Psychological Services.
Lugnegard, T., Hallerback, M. U., & Gillberg, C. (2011). Psychiatric comorbidity in young adults with a clinical diagnosis of Asperger syndrome. Research in Developmental Disabilities, 32, 1910–1917. https://doi.org/10.1016/j.ridd.2011.03.025.
Maddox, B. B., & White, S. W. (2015). Comorbid social anxiety disorder in adults with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(12), 3949–3960. https://doi.org/10.1007/s10803-015-2531-5.
Mazefsky, C. A., Borue, X., Day, T. N., & Minshew, N. J. (2014). Emotion regulation patterns in adolescents with high-functioning autism spectrum disorder: Comparison to typically developing adolescents and association with psychiatric symptoms. Autism Research, 7(3), 344–354. https://doi.org/10.1002/aur.1366.
Mazefsky, C. A., Herrington, J., Siegal, M., Scarpa, A., Maddox, B. B., Scahill, L., & White, S. W. (2013). The role of emotion regulation in autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 52(7), 679–688. https://doi.org/10.1016/j.jaac.2013.05.006.
Merikangas, K. R., He, J., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., Benjet, C., Georgiades, K., & Swendsen, J. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication—Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 49(10), 980–989. https://doi.org/10.1016/j.jaac.2010.05.017.
Pandolfi, V., Magyar, C. I., & Dill, C. A. (2012). An initial psychometric evaluation of the CBCL 6–18 in a sample of youth with autism spectrum disorders. Research in Autism Spectrum Disorders, 6(1), 96–108. https://doi.org/10.1016/j.rasd.2011.03.009.
Salazar, F., Baird, G., Chandler, S., Tseng, E., O’sullivan, T., Howlin, P.,… Simonoff, E. (2015). Co-occurring psychiatric disorders in preschool and elementary school-aged children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(8), 2283–2294. https://doi.org/10.1007/s10803-015-2361-5.
Salters-Pedneault, K., Roemer, L., Tull, M. T., Rucker, L., & Mennin, D. S. (2006). Evidence of broad deficits in emotion regulation associated with chronic worry and generalized anxiety disorder. Cognitive Therapy and Research, 30(4), 469–480. https://doi.org/10.1007/s10608-006-9055-4.
Silk, J. S., Steinberg, L., & Morris, A. S. (2003). Adolescents’ emotion regulation in daily life: Links to depressive symptoms and problem behavior. Society for Research in Child Development, 74(6), 1869–1880. https://doi.org/10.1046/j.1467-8624.2003.00643.x.
Silverman, W. K., & Albano, A. M. (1996). The Anxiety Disorders Interview Schedule for Children for DSM-IV: (Child and parent versions). San Antonio: Psychological Corporation.
Smith, I. C., Ollendick, T. H., & White, S. W. (2019). Anxiety moderates the influence of ASD severity on quality of life in adults with ASD. Research in Autism Spectrum Disorders. https://doi.org/10.1016/j.rasd.2019.03.001.
Smith, L. E., Greenberg, J. S., & Mailick, M. R. (2013). Adults with autism: Outcomes, family effects, and the multi-family group psychoeducational model. Current Psychiatry Reports, 14(6), 732–738. https://doi.org/10.1007/s11920-012-0328-1.
van Steensel, F. J., Bögels, S. M., & Perrin, S. (2011). Anxiety disorders in children and adolescents with autistic spectrum disorders: A meta-analysis. Clinical Child and Family Psychology review, 14(3), 302–317. https://doi.org/10.1007/s10567-011-0097-0.
Wechsler, D. (2011). Wechsler Abbreviated Scale of Intelligence (WASI-II) (2nd edn.). San Antonio: NCS Pearson.
White, S. W., Elias, R., Capriola-Hall, N. N., Smith, I. C., Conner, C. M., Asselin, S. B., et al. (2017). Development of a college transition and support program for students with autism spectrum disorder. Journal of Autism and Developmental Disorders, 47(10), 3082–3078. https://doi.org/10.1007/s10803-017-3236-8.
White, S. W., Oswald, D., Ollendick, T., & Scahill, L. (2009). Anxiety in children and adolescents with autism spectrum disorders. Clinical Psychology Review, 29(3), 216–229. https://doi.org/10.1016/j.cpr.2009.01.003.
Wigham, S., Barton, S., Parr, J. R., & Rodgers, J. (2017). A systematic review of the rates of depression in children and adults with high-functioning autism spectrum disorder. Journal of Mental Health Research in Intellectual Disabilities, 10(4), 267–287. https://doi.org/10.1080/19315864.2017.1299267.
Wood, J. J., & Gadow, K. D. (2010). Exploring the nature and function of anxiety in youth with autism spectrum disorders. Clinical Psychology: Science and Practice, 17(4), 281–292. https://doi.org/10.1111/j.1468-2850.2010.01220.x.
Zimmermann, P., & Iwanski, A. (2014). Emotion regulation from early adolescence to emerging adulthood and middle adulthood: Age differences, gender differences, and emotion-specific developmental variations. International Journal of Behavioral Development, 38(2), 182–194. https://doi.org/10.1177/0165025413515405.
Funding
This study was funded by the National Institute of Mental Health (Grant No. R34MH104337, White).
Author information
Authors and Affiliations
Contributions
ASC, ICS, and SWW conceived of the study. ASC and ICS drafted the manuscript. CAM participated in study design, data analyses, and manuscript writing. SWW directed the study, oversaw data collection, helped with analyses, and contributed to manuscript development.
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Charlton, A.S., Smith, I.C., Mazefsky, C.A. et al. The Role of Emotion Regulation on Co-occurring Psychopathology in Emerging Adults with ASD. J Autism Dev Disord 50, 2585–2592 (2020). https://doi.org/10.1007/s10803-019-03983-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-019-03983-5