
Abstract
Substantial research identifies mothers of children with a disability as a vulnerable group with compromised health outcomes and restrictions for their own self-care, social, economic and leisure participation. This study investigated perceptions and experiences of mothers following attendance at health education and empowerment workshops (Healthy Mothers Healthy Families). Mixed methods evaluated mothers’ experiences. A pragmatic qualitative approach was applied to data analysis of interviews with mothers (N = 19). Four themes emerged: Changes for me; Changes for my family; Wisdom gained; and Worthwhile workshops. Mothers described feeling validated and empowered in this facilitated group intervention and valued education about women’s health, tailored research findings, individualised goal setting, time to learn and share with other mothers, and the workshop environment.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Families raising a child/young person with a disability function differently from other families, and have different experiences of health (Brehaut et al. 2009, 2004), leisure (Dodd et al. 2009) and access to both economic and social participation (Ketelaar et al. 2017). Family systems theory has long maintained that what affects one family member will directly or indirectly affect all other family members who share the same environment (Bowen 1966). The lived family environment has a profound influence on the health and opportunities of family members including mothers (Bourke-Taylor et al. 2010; Zablotsky et al. 2013), fathers (Bonsall 2014), other children and the child with a disability (Ketelaar et al. 2017).
Emerging evidence suggests that fathers experience stress related to their child’s perceived acceptability and other specific service barriers (Ly and Goldberg 2014). However, mothers are usually the ‘parent most knowledgeable’ (PMK) about the child’s health, development, service needs and interactions, and are known to experience higher rates of unrelenting stress and mental health issues (Bourke-Taylor et al. 2010, 2012; Chan et al. 2015; Montes and Halterman 2007). Although mothers and fathers may have different roles and health experiences (Allen et al. 2013; Miodrag et al. 2015), parents drive family routines around health, work, education, usual daily activities and leisure together (Dodd et al. 2009). However, when disability affects a family, such routines may be based around the child’s needs (Dodd et al. 2009; Larson 2010) and parents may forego time together, enjoyable family activities, and their own health appointments, secondary to meeting the equipment, service and other requirements of their child’s care (Bourke-Taylor et al. 2015). Although the need for effective interventions to better support mothers and fathers has been established, few evidence based programs are available (Golfenshtein et al. 2016; Law et al. 2014; Sartore et al. 2013).
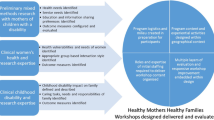
The first step towards designing an evidence based program is determining need. Then, based on the needs of the population of interest, the program can be created and then evaluated. In line with the creation and evaluation of a program for mothers of children with a disability, Healthy Mothers Healthy Families (HMHF) is a program specifically designed following an exploratory mixed methods research project by the first author about the health and situation of mothers of a child with a disability. Key issues related to maternal health were identified including challenging behaviour (Bourke-Taylor et al. 2010), maternal empowerment and service navigation issues (Bourke-Taylor et al. 2012), maternal inability to participate in paid work (Bourke-Taylor et al. 2011), chronic sleep interruption (Bourke-Taylor et al. 2013), risk factors associated with family constellation (Bourke-Taylor et al. 2012), and lack of social supports. Subsequently, collaboration with an expert women’s health physician/general practitioner and researcher (second author) resulted in development of the HMHF pilot program. Hence, HMHF is an evidence informed program (see Table 1 for an overview of the HMHF content).
The overall aim of the HMHF pilot program was to improve the mental and physical health of mothers, maternal empowerment around the child’s disability and family issues, increase help-seeking behaviours and use goal setting for healthy lifestyle redesign within a group based workshop run over six sessions (18 hours). An embedded mixed methods design was used to evaluate the pilot HMHF to allow both qualitative and quantitative data to be collected together (see Table 1, columns 5–7). The embedded design allows triangulation of data and more in-depth insights into the perspectives and impact of the program (Creswell and Plano Clark 2011). The mixed methods included a quantitative study over 8 months and a qualitative component that occurred at the end of the workshops. The quantitative study aimed to detect significant changes in the areas that the program targeted. Findings included statistically significant improvements reported by mothers as follows: participation in healthy activity (p = .017); reduction in depression, anxiety, stress symptoms (p = .017, 0.016, 0.037 respectively); improved empowerment (p = .009); improved family cohesion (p = .05); and improved maternal report of their child’s psychosocial quality of life (p < .001). The qualitative study was completed to explain mothers experiences within and consequential to the HMHF pilot and are presented in this paper.
The aim of this paper is to present the qualitative findings that explored the experiences and perspective of the mothers subsequent to attending the HMHF program. Research questions were:
-
1.
What were mothers’ perspectives on how the HMHF workshops influenced their own mental health, social participation and wellbeing?
-
2.
What were the experiences of mothers who attended HMHF workshops in relation to their own participation in health related activity?
Methods
An embedded mixed methods design was applied to the evaluation of the pilot HMHF program (Creswell and Plano Clark 2011). Qualitative data were collected within 2 weeks of the end of the program (see Table 1, columns 5–7).
Pragmatic Qualitative Approach Within Embedded Mixed Methods Design
A pragmatic qualitative methods approach was applied to this project. Patton (2015) identified ten pragmatic principals for qualitative inquiry and all were relevant to this research: a practical mixed methods approach; real world constraints contained interviews and data collected as participants were busy women with minimal free time to participate in research; data were analysed with a view to actionable findings; inductive and deductive reasoning approaches were applied to the data; transparent reporting of processes; and the pragmatic inquiry was informed by the assumption that women participated in interviews because they found some aspect of the program useful, although such disclosure may constitute a partial truth and veil what was not effective or helpful.
In line with a pragmatic approach, the research questions informed the development of interviews. Semi-structured interview guides (See Table 2) were piloted and configured with probes. The authors were the developers and presenters of the program and had a participatory involvement as occurs when both groups share an evolving interpretation of the experience using mixed methods (Creswell and Plano Clark 2011). Before any data collection commenced, ethics approval was sought and received from Monash University Human Ethics Research Committee.
Recruitment and Participants
The HMHF workshop series was advertised widely through childhood disability organisations, disability service organisations and specialised schools that supported students with disabilities. The notice invited mothers of school-aged children to participate in a workshop series and the research. However enrolment in the HMHF workshops did not require participation in the research and several women attended the workshops and did not wish to be involved in the research. This qualitative study involved purposive sampling as all participants who attended one of the final three workshops were invited. All participants provided informed consent. Eighteen women were interviewed over the phone with interviews taking 30–45 min and being recorded and later transcribed verbatim. One mother declined interview preferring sharing her experiences via an emailed word document. See Table 3 for information about participants.
Data Collection, Management and Analysis
Interviews were conducted and digitally recorded by a research assistant with knowledge of the program. The authors of the program were not present or involved with interviews. Interviews were then re-identified by the first author. Participants were sent their transcribed interview and were encouraged to make additional comments. No responses of additional comments were received. Data were analysed systematically using manual means and NVivo Version 11. Content analysis was applied to the data in a structured way with records scrupulously kept, ensuring replicability and dependability of the study. Data were initially coded (identification of rich text), then categorised into patterns of like concepts, followed by labelling the primary patterns into themes and subthemes (Patton 2015). A second research assistant, and both authors, were involved in content analysis. First, like concepts (patterns) were identified for each interview, and then categories across interviews were compared. Configuration of common categories into themes and subthemes continued until all three researchers agreed on categorisation of patterns of data, and derived themes. A deductive process then occurred to consider themes and subthemes in relation to the research questions although many subthemes were interrelated.
Results
Nineteen mothers (see Table 2) participated. The four overarching themes were: Changes for me; Changes for my family; Wisdom gained; and Worthwhile workshops (see Fig. 1). Each major theme had between 2 and 8 sub-themes. Although the figure shows subthemes stemming from overarching themes, sub-themes were not hierarchically organised with one being more important or prominent than another. Thematic findings with representational quotes are presented below.

Themes resulting from content analysis of interviews (N = 19)
Theme One: Changes for Me
All participants attributed some positive changes to attendance at the workshops. Two sub-themes were derived: Myself (awareness of and protection of one’s wellbeing) and My Health (one’s health related needs, priorities and changes).
Myself
All mothers reported changes in awareness about the importance of protecting and promoting their own wellbeing. Strategies described included increasing supports, containing and overcoming feelings of guilt for prioritizing their own needs, making time for leisure or returning to paid work. Many of the sub-themes were intertwined.
Support
Many mothers described new understanding about the importance of identifying, cultivating and extending support around themselves and their families. Some women identified other mothers of children with a disability as a source of support, such as Mia: “I realised the importance of social support or friendships to my health. I don’t think that I had really made that link before… It was nice to make new contacts at the workshops.” Other mothers described reaching out to their family and friends. Kylie recognised the need to actively find support: “I’ve been more open with people about when I need help. I’m able to communicate that more… to look after myself and to relieve some of the pressure and burden”. Louisa stated: “I now realise the importance of cultivating friendships with like-minded families.”
Diane recognised that informing others of her situation and needs would help reduce isolation: “…because 12 months ago I was pushing everyone away. I just thought, they don’t understand… But it’s up to me to change that. It’s not up to them, because only I can inform them.”
Not Feeling Guilty
Guilt featured in some interviews. Many mothers described feeling guilty about taking time for themselves and their own health. Gretal realised that attending to her own needs was “…not a frivolous thing, it’s a good thing…” As explained by Mia: “This whole series has made me realise that I don’t have to feel guilty about spending time on my own well-being. Actually, that phrase in each workshop, that I am important.” Louisa stated: “I’ve been thinking a lot about my own health. I realise how important it is to look after myself. I have finally given myself permission to take time out, relax and express my own needs.” Odette described feeling guilty about grieving:
…the main thing we need to be taught is not to feel guilty… grief won’t go away, it’s manageable… I’m seeing the other children going in a different direction to my daughter and it’s grief for what could have been… but I’m allowed to feel like this, it’s okay. And I think there’s a lot of mums out there doing it tough, who don’t realise that it’s okay.”
Other women, such as Amber, discussed guilt associated with accessing services for their child:
[I’ve realised] I have permission to feel like I need help and to ask for help. My husband and I have always felt [our son] has moderate issues… We always feel that other people deserve more respite or more of this or more of that [but]… as my son gets older his… difference from other children gets wider…
Enjoyment from Leisure and Work
Activities in the workshops encouraged reflection on time use and health. The common experience was limited time to follow interests outside of mothering and caring. Diana recognised that she needed to prioritize time for leisure: “I do need to have a bit more of ‘me’ time, like active and inactive leisure, I haven’t done that yet.” Kylie considered her past interests and hoped to return to “…playing the piano and I loved singing… it’s about figuring out where we could fit it in.”. Mia reflected on the time use activity (Workshop1):
We did that time use activity at the beginning… I realised that most of my time is productive time, and very little is for leisure. I realised that I feel guilty if I even think about doing something for me, because there’s this never-ending list of things that I should be doing for my two sons with extra needs… so any time that I would spend in leisure, seems to me counter-productive because that means I’m not moving through that list… it’s like a little black cloud hanging over me…
Several women aspired to return to paid work. Kylie stated: “I’m even looking at going back to some paid work, I’ve had a couple of job interviews…I enjoy working”. Beatrice returned to paid work after starting the workshops, stating that she needed “another role than just being a mother.”
My Health
The workshops contained substantial content about women’s health at different ages, and lifestyle redesign ideas to promote health. Specific research pertaining to mothers of children with a disability was also presented. Mothers described implementing change to become more active, reduce stress and find services to address health.
Feeling Better, Feeling Energized
Dianna, similar to most mothers, described being “run off my feet… just running around trying to fit in therapy… getting that all in place with the right people”. However the workshops had improved her “mental and physical wellbeing… I just have more energy… I feel a lot more stable and focused.” Gretal described previously forgoing healthy activities: “if I’ve got a thousand things to do the first thing to go is the gym for me. But now I think, “No, I just have to do that one,”… the gym gives me more energy. Now I make sure that I do things for my health.”
Being More Active
Physical activity became a priority for many mothers such as Kylie: “I am trying to walk more, when I wasn’t walking at all. Through the workshops I’ve learned that it is okay to look after myself… I’ve always been told: “If you don’t look after yourself, who’s going to look after your family?” Now I’ve started to really grasp the meaning of those words and I am trying to put some things in place that help me.” Fifi also recognized the importance of exercise for family health: “exercise is important for all of us… my kids and I have been doing a lot more walking, parking half way to school and walking the rest of the way… I’ve started Yoga which I’m really enjoying… It’s important for me to be healthy for us to function better as a family…”
New Strategies to Reduce Stress
Stress management strategies were included within the workshops. Kylie described mindfulness: “practise[d] incidentally throughout my days. I’ve found that I do have more joy in my day… I’m finding myself to be less stressed.” Dianna found seeking perspective as an effective strategy: “Because I have depression and anxiety… it’s something I have to manage every day… I have a battle with it, but I just have to be focused and perspective [taking] and the mindfulness. That’s really helped me”.
Sally used stress management to assist her to remain calm in school meetings about her daughter that were “always horrible. I just get shot down to the ground…” However, Sally described implementing some strategies that “really calmed me before going in… I had to really make my case and just stay calm through it… I kept getting blown off… finally at the end, when I brought it up again, the special needs director [agreed].” Nora found that some strategies had “a flow-on effect that I’m still utilising things from the course, even though I’m not there anymore.”
Going to Health Services Myself
Eighteen of nineteen mothers interviewed stated that they had visited their general practitioner (GP) as a result of the workshops. Help seeking and goal setting were included in the workshops. Heather had taken her two children to the dentist regularly but she “hadn’t been to the dentist for 7 years”. Furthermore, Heather followed up with “my skin had been worrying me for the last 18 months… I’ve been to the GP”. Kylie also went to the dentist after admitting that she had “been putting that off for a number of years…it’s been good.” Other women such as Isla and Gretal followed up to see their GP to commence a mental health care plan (ten publicly-funded mental health professional visits in Australia):
I’ve seen my GP and I’ve got a mental health plan and I’m seeing a psychologist… I never got around to doing anything about [my mental health]… the most valuable [part for me] was realising that you treat a mental illness as you would a physical illness. (Isla)
Since the workshops… I went and got a mental health plan and have seen a psychologist a couple of times… [and] got all my health tests done, started doing yoga once a week. Taking on that as a necessary thing, as opposed to a nice-to-have-if-I-can-fit-it-in thing. (Gretal)
Women appreciated research findings that they could relate too, as Dianna noted:
When [the presenters] put up the statistics… I just thought, hey, I’m an older mum… I really need my energy, because my two boys are five and three… Instead of just saying, “I’ll get to it 1 day”, I thought, no, I’ll address it... I [saw] a rheumatologist to address everyday pain… my GP… the dentist….”
Heather realised that prevention was important: “beforehand I was, yeah, I look after myself, I eat well, I exercise, yeah. But I’m not looking after myself properly. Because I’m actually not seeing the [health professionals] that I need to see...”
Theme Two: Changes for My Family
The workshops primarily emphasised women’s health, wellbeing and daily activities/occupations. However mothers applied their knowledge to their children, partner and family life.
My Health and My Child/ren
Mothers often described their own and their child’s health as related. Nora felt emotionally “fused with my child’s emotions and issues. It was something that I was unaware that I was even doing… but becoming aware of that has actually freed me up a little bit with my own emotional wellbeing.” Tania described taking her daughter with suspected pneumonia to the doctor, “and the doctor confirmed that she did, and then the doctor said to me, “Oh I just need to listen to your chest”. She said, you have pneumonia too… it hadn’t occurred to me… I felt a bit foolish that I hadn’t noticed.” Mia made an appointment with the GP for herself, following the women’s health workshop, however “it turned out that something had come up with my son, so the appointment ended up being about my son, rather than me. But I will try and make another time to discuss my own general health.”
Changes Managing My Child’s Needs
Mothers experienced changes to their own health and some aspects of the way they managed their child’s needs. Fifi was dedicated to being “healthier and fitter… I’ve been spending a lot of time one on one with my autistic son. We’ve been going for walks together… He doesn’t like to tell me much so it’s a really good opportunity to try and [talk]…” Odette described a change in the way she interacted with her child: “with my little girl…I’ve got so much to do. But now I stop and actually listen to what she has to say… she doesn’t talk a lot, but when she talks I need to listen.” Sally managed to address her child’s sleep issues:
I realised I wasn’t getting enough sleep and not enough rest time… She would not go to sleep... Tired children are really exhausting, like they’re grumpy and it just made everything really difficult, and I didn’t get any time… armed with this information I went to the GP… it’s been an absolute blessing, she’s in bed by 8:30 and asleep at quarter to nine.
Impact on My Child’s Services
Some mothers described becoming more assertive, discriminating with services and clearer with decision making. Diane described feeling more “resilient and more definite about my decisions. I used to um and ahh… Now, I just make a decision.” Diane gave the example of changing her child’s therapist, asking herself: “are we sure about this therapist? No, I’m not. She’s not the right person… there was no rapport…” Others discussed changes in managing appointments and interactions with the health and medical system. Nora’s interactions with “with multiple agencies that you have to work with has probably been more measured… rather than emotive.” Tania shared a scenario where she remained calm when she might otherwise have experienced a “heart beating stressed state” when an X-ray for her child made them 40 min late for the appointment with the doctor. Tania “felt a lot calmer…everything was calm and ran smoothly… it was a much better way to be.”
Mia described changes in the support her child received at school, after years of the school asking: “can you come and pick him up early from camp, pick him up early from the zoo expedition… I felt like I needed to be available all the time.” Mia decided to return to work after learning about the health benefits of paid work. This changed her availability to the school: “they said can you pick him up early… I said, sorry I can’t pick him up, I’m working… so they found another solution… [and my son] exceeded their expectations… I knew he was fine.”
Changes at Home
Feeling calm meant that mothers described their homes as “a lot calmer”. Beatrice described: “leaning more on the children’s father, sharing the load when I would normally handle everything myself… I feel better.” Other mothers reported changes in their partnerships, including Louisa: “I am more positive and motivated at home with my husband and improving our relationship and calmer with my son.” Amber realised that both she and her partner needed time away from their children, however solutions were not available: “we made enquiries to the council about respite, thinking that we need to have an afternoon together and a night together, and it’s too expensive… it would cost us $30.00 an hour to get someone from the council out, and we can’t afford that.” Gretal relayed a story about change to the family dynamics when Gretal’s dance group was performing for the end of year concert:
…it meant my husband had my disabled child all weekend… he didn’t realise the impact it would have on him and got a bit snotty and grumpy about it… I may have bent over backwards at one stage to do something else but then kind of went, “No, I’m not even going to offer to do that. He’ll get over it.”…he got over it. He even came to one of the performances, which he hadn’t committed to doing. He brought my daughter along and it turned out to be a really good night.
Other women described changes relating to their children without disabilities. Amber dedicated one to one time for her child who did not have a disability: “actually concentrating on what he’s doing for that time. So with a special needs child you would set aside time for appointments and you would do that with them, but with your normal children you don’t really do that”.
Theme Three: Wisdom Gained
Workshops brought women together to share experiences, learn and gain perspective. Collectively these experiences created a new wisdom for mothers.
Learning and Understanding the Journey
The workshops presented a framework about the journey of mothers, and activities in the workshops enabled mothers to reflect on their ‘journey’. Based in research, the ‘Journey of mothers’ educated participants about common experiences: adapting to a child’s developmental or health status; adapting to the role demands of mothering a child with a disability; and parallel social, health and wellbeing experiences. Mia described the journey as “very true for me”. Estelle stated that the phases “really resonated with me. I could clearly identify where I was and where I’d been and where I wanted to go too.” Although some mothers found the information “confronting”, Catherine’s words echoed what most mothers experienced:
It was helpful to hear about the phases that mothers describe on their journey with their child with a disability. Steps like grieving and eventually achieving life balance. I felt relieved knowing that I’m not crazy, I’m not cuckoo. I am following the phases like other mothers and I feel good that I’m like everyone else.
Tania agreed that: “it’s a recurring cycle, every time the child transitions from one place to another or does something new… acceptance of disability is a journey that you go on”. Tania’s child did not have a clear diagnosis and hers was described as an “up in the air journey”.
Catherine captured the common experience of mothers regardless of their child’s diagnosis: “we all went through the same things, the same emotions. We all felt hopelessness and we felt useless, and we didn’t know where to turn… we all connected, we’re all so similar. We went through all the same things.” Nora noted that “it’s hard when the majority of people that you know don’t have to worry about the disability side of things. They say, “Oh, you’re so consumed with this”. But actually [the workshops] gave me a perspective... I walked away empowered in my journey because all of my feelings had been validated”.
Knowledge About Women’s Health and Myself
All women valued the women’s health information, such as Amber: “To put it in a package made the message hit home.” Dianna compared the workshops to those that she had attended in the past stating: “You go to programs learning about autism and they might touch on a little bit about looking after yourself… you just think, well, what does that mean?... but when it’s analysed or dissected in front of you, that’s when you really see it and say, “This is what I need to do for myself"…” Jessica noticed that information for parents and their health and wellbeing was easily “lost in the other things that need to be done” for the child with a disability. Kylie described being “quite blown away by the whole process” of the workshops, “the health aspect really made me more aware. Because I want to be here for my kids. I want to be a happy mum. I don’t want to be a grumpy mum.”
Pia noted that “there’s a lot to be gained” by learning about one’s health and wellbeing. Such information was “extremely valuable” because “when you know about things, you can actually handle them a lot better…[and] know when you need to go and get help.”
Jessica noted that poor health “is not something that we have to accept. Looking at the health statistics for women versus the health statistics for women with a child with a disability was pretty eye-opening. I thought that was a very valuable piece of information. I’m a data girl, so that spoke to me.”
Experiences in the Workshops
This subtheme encapsulated mothers shared experiences and camaraderie during the workshops. All mothers enjoyed spending time with others who had a shared life experience. As Pia described, mothers “walk a harder road because of our family situation… There were some women at the workshops that had some really incredible stories and enormous strength. There was amazing strength throughout the whole workshop…” The planned milieu of the workshops was one of comradery, emotional safety and support as described by Rochelle: “the whole interaction and being there with other mothers was a really essential part of why it was so good…. [it’s] rare [to be] in an accepting environment [where] you don’t have to tell people about your story, that’s a big part of what I found really helpful”. Many mothers identified other mothers as a strength of the workshops, such as Louisa who experienced: “a sense of belonging… The social interaction was invaluable and such a bonus. I met some really amazing women and have continued to keep in touch with a few.”
Women described feeling grateful, such as Gretal’s comments:
My daughter has Rett syndrome, so she’s physically and intellectually disabled but she’s a happy little sausage and most of the time she doesn’t have the behavioural issues… my girlfriend who was sitting next to me, she has a daughter with the same disorder and we just looked at ourselves at one point and just went, you know, in some ways, they’re physically taxing and you worry a lot but we don’t have necessarily the behavioural stuff every day to deal with.
Amber appreciated the emphasis on mothers rather than children, “because I think it becomes a bit of a competition on who’s got the worse scenario, and who must be suffering the most.”
Perspective
Many mothers spoke about gaining a new perspective. Reflection was useful for mothers, such as Amber: “I always feel that I’m a terrible mother and I’m not doing enough and all that kind of stuff, and it’s probably not true.” Heather stated:
I’m constantly, oh have I done enough for [child with autism]? … Is he well-balanced, is he this, is he that. Then, oh my gosh, have I neglected [other child] because I’ve put so much effort into [child with autism]. I was constantly questioning myself…Upon reflection, I thought, I can’t possibly do any more for these children, and I’m doing my best. I’ve now started to tell myself that a bit more often.
Perspective assisted Nora: “my journey with my children has been validated, that I’m not alone, I’m not going crazy, it actually is a valid stress that people don’t give credence too. So I am probably walking a little bit taller.”
Theme Four: Worthwhile Workshops
Mothers who participated in the interviews found many aspects of the workshops to be worthwhile.
Direction and Goals for Me
The workshops emphasised a strengths approach, encouraging mothers to lead change through building strengths and containing challenges. The structure appealed to most women, as described by Sally “…the course really gave me an incentive to sort of keep looking at areas that are causing problems in our lives and really keep finding solutions because the payoff is really worth it”. Mothers set goals around desired change, such as Nora: “I know what I can and can’t do and what is a realistic goal and what’s not a realistic goal and how to go about starting that change”. Further, Nora stated that the “SMART Goals were invaluable… what an amazing way to tackle issues and/or tasks.”
Gretal noticed the similarities between the goals she set for herself and her daughter:
Setting little achievable goals… take little steps, not the whole thing at once, break it down a little bit. If I look at my daughter’s education, that’s exactly what they did… they celebrate all the little things, just because she doesn’t achieve the big thing (walking), the little things are successes as well.
Mia expresses benefits after initial doubts: “Originally when I first looked at doing it, I thought, how am I going to get there, that’s a big commitment. Here I am at the other end thinking, I wish I had more time!”
Relevant and Tailored to Me
Mothers acknowledged the relevance and tailored delivery of the workshops. Sally stated that “it was the focus on information provision that I found extremely helpful, with the suggestion of how we might incorporate those things into our lives.” Similar to others, Louisa liked the “activity sheets [that]… it was good to reflect…” Jessica stated “the handouts really meant that you made the time to say, well what are my supports? How am I feeling? What is out there? There were handouts every session that helped”.
Mothers recognised the role and necessity of professional leaders, including Nora who appreciated the moderating of group conversations to prevent a minority of mothers from “monopolising” discussions. Further, the professional leaders kept the program “moving along” and kept everyone’s attention on the workshop’s purpose. Rochelle stated that “…it’s very hard for mothers… Often they do need professionals to say, look, you do need to do this, or it is important that you go…” Other mothers commented about plans for the workshops to go online: “if there’s a website, people can enter it and exit it, even if they can’t physically go somewhere. It’s a fantastic alternative.” (Jessica). Pia stated:
I remember [the presenters] saying at the beginning, “This is not about your children. This is not about what’s going on in your family life. This is about you and what’s going on in your life and how to keep yourself strong and healthy.” I do think that [presenters] certainly achieved that objective.
Mia believed that:
A schedule of when the workshops are running should come with the diagnosis… With the diagnosis, we get told what kind of therapies are going to be beneficial for our children, and you get referred on to early intervention if you find out early… I think that we should also be sent along to the seminars, right at the beginning. I can’t tell you, when I look at it now, what a difference having this information could have made.
Odette held a similar belief, stating: “I just wish you guys had been around when my daughter was diagnosed… because it would have been so much more helpful when I was trying to get resources around me.”
Rochelle stated that “there’s so much pressure on mothers to just give up everything so that they can look after their children and forget about themselves… this workshop was clearly about mothers…” Pia described the workshop participants: “Women are such an important part of families in the community. I think we’re unsung heroes…”
Discussion
This research presents the experiences of nineteen mothers who participated in HMHF that revealed positive change towards better health, wellbeing and lifestyle changes. The current study presented qualitative findings of a mixed methods preliminary evaluation of HMHF. Although the quantitative findings demonstrated that the program was effective, achieving set aims, this paper provides the context and experiences that triangulate findings within the context of the mother’s lives. For example, although HMHF focused on the mother, there were changes within family systems. Mothers described the fathers taking more responsibility and experiencing growth in relation to responsibilities and time spent with the child with a disability. Siblings were recognised as needing their own intensive and alone time with the mother, and the child with a disability was incorporated into the mothers leisure time.
Mothers described feeling validated and valued through experiences in the workshops; feeling inspired by other women; and the benefits of meeting other women based on the shared carer parent role rather than being grouped according to their child’s diagnosis or with families from one disability service. This finding is important as researchers and service providers may tend to configure programs by grouping families according to the child’s diagnosis, thereby potentially reinforcing a siloed approach to disability. The HMHF was delivered within a community, thereby demonstrating family centred practice (FCP) at a broader population level.
Past research has suggested that shared experience is valuable and that there are benefits to improving peer support among parents (Sartore et al. 2013). Similar to women in the HMHF groups, other mothers have described the empowerment gained through meeting other mothers (Kuhaneck et al. 2010), a reduction in the negative impact of stigma and improved coping and problem solving capacity to manage carer related challenges (Kuhaneck et al. 2010; Law et al. 2014; VanLeit and Crowe 2002).
Mothers in the current study found that stress management techniques could be applied easily to daily life. One other study found that parent programs that aim to reduce stress via the use of mindfulness and other strategies were effective for parents with a child with Autism (Bluth et al. 2013). Other emerging evidence suggests that programs that support parental mental health and wellbeing can substantially reduce parental distress (Dykens et al. 2014) and that resilience can be learned and serves as a protective factor for parents of children with a disability (Bekhet et al. 2012).
Experiences described in the current research suggested that many women did increase their participation in health enhancing activities. Mothers in this study reported increasing their physical activity and including time with other family members. Such findings are consistent with family systems theory in that changes to behaviour and lifestyle of the mother, influenced the behaviour and participation of other family members (Piotrowska et al. 2017). Other research has reported improved wellbeing around maternal goal setting to increase ‘me time’ and roles outside of mothering (Kuhaneck et al. 2010; McGuire et al. 2004; VanLeit and Crowe 2002). Mothers in the current study identified stress, grief, feelings of hopelessness and guilt as issues that prevented their progress. Further, a lack of time to themselves or with a partner, anxiety and depression, reduced sleep, unwell or high needs children all impacted on mothers’ ability to achieve wellbeing. Mothers believed that the workshops were instrumental in bringing about positive changes for themselves and other family members.
An unexpected finding was the extent to which mothers described influences their family and individual members. These findings suggest that individual-focused interventions, such HMHF can have an impact on the entire family. Another finding reported by some mothers was clear attempts to find time to spend with their partners (usually the child’s father). Whilst the HMHF program did include an activity that reflected on the mothers identified life supports (usually their spouse/the child’s father), no other relationship or co-parenting advice was included in HMHF.
Limitations and Future Research
It is important to note that only half of mothers who attended the workshops were interviewed—nineteen out of 37 who attended more than one workshop. Therefore this research paper presents the experiences of a self-selecting sample who experienced positive effects in their lives. Other women may not have experienced positive effects and future research will need to include investigations of such experiences. The research is a part of a mixed methods evaluation (see Table 1 for details of data collection points, reported in detail in tbc). The current study will inform a more rigorous evaluation, such as a mixed methods, randomised control trial with cross over design in the future.
Conclusion
The HMHF pilot was developed to address the health and lifestyle needs of mothers who have primary caring responsibilities related to a child/young person with a disability. The experiences of mothers as described in this study suggest that the program has value and should continue to be developed to extend reach to families. Based in some principles of family systems theory and congruent with FCP which identifies all family members as crucial to children’s health and participation, HMHF is an evidence informed program that aims to specifically facilitate maternal wellbeing. Findings from this study can inform professionals delivering services within a FCP model to understand mothers’ needs and perspectives. HMHF is an example of broad application of FCP at a community level.
References
Allen, K. A., Bowles, T. V., & Weber, L. L. (2013). Mothers’ and fathers’ stress associated with parenting a child with autism spectrum disorder. Autism Insights, 5, 1. https://doi.org/10.4137/AUI.S11094.
Bekhet, A. K., Johnson, N. L., & Zauszniewski, J. A. (2012). Resilience in family members of persons with autism spectrum disorder: A review of the literature. Issues in Mental Health Nursing, 33(10), 650–656.
Bluth, K., Roberson, P. N. E., Billen, R. M., & Sams, J. M. (2013). A stress model for couples parenting children with autism spectrum disorders and the introduction of a mindfulness intervention. Journal of Family Theory Review, 5(3), 194–213. https://doi.org/10.1111/jftr.12015.
Bonsall, A. (2014). Fathering occupations: An analysis of narrative accounts of fathering children with special needs. Journal of Occupational Science, 21(4), 504–518.
Bourke-Taylor, H., Cotter, C., & Stephan, R. (2015). Complementary, alternative and mainstream service use among families with young children with cerebral palsy: Costs and family sacrifice to access choices. Physical and Occupational Therapy in Pediatrics, 35(3), 311–325.
Bourke-Taylor, H., Howie, L., & Law, M. (2010). Impact of caring for a school-aged child with a disability: Understanding mothers’ perspectives. Australian Occupational Therapy Journal, 57(2), 127–136. https://doi.org/10.1111/j.1440-1630.2009.00817.x.
Bourke-Taylor, H., Pallant, J. F., Law, M., & Howie, L. (2013). Relationships between sleep disruptions, health and care responsibilities among mothers of school-aged children with disabilities. Journal of Paediatrics and Child Health, 49(9), 775–782. https://doi.org/10.1111/jpc.12254.
Bourke-Taylor, H. M., Howie, L., & Law, M. (2011). The preclusion of mothers of school aged children with disabilities from paid work and relationship to health related quality of life. Journal of Intellectual Disability Research, 55(5), 511–520.
Bourke-Taylor, H. M., Howie, L., Law, M., & Pallant, J. F. (2012). Self reported mental health of mothers with a school aged child with a disability in Victoria: A mixed method study. Journal of Paediatrics and Child Health, 48(2), 153–159.
Bourke-Taylor, H. M., Law, M., Howie, L., & Pallant, J. F. (2010). Development of the child’s challenging behaviour scale (CCBS) for mothers of school aged children with disabilities. Child: Care, Health and Development, 36(4), 491–498.
Bourke-Taylor, H. M., Pallant, J., Law, M., & Howie, L. (2012). Predicting mental health among mothers of school-aged children with developmental disabilities: The relative contribution of child, maternal and environmental factors. Research in Developmental Disability, 33(6), 1732–1740.
Bowen, M. (1966). The use of family theory in clinical practice. Comprehensive Psychiatry, 7(5), 345–374.
Brehaut, J. C., Kohen, D. E., Garner, R. E., Miller, A. R., Lach, L. M., Klassen, A. F., & Rosenbaum, P. L. (2009). Health among caregivers of children with health problems: Findings from a Canadian population-based study. American Journal of Public Health, 99(7), 1254–1262. https://doi.org/10.2105/AJPH.2007.129817.
Brehaut, J. C., Kohen, D. E., Raina, P., Walter, S. D., Russell, D. J., Swinton, M., & Rosenbaum, P. (2004). The health of primary caregivers of children with cerebral palsy: How does it compare with that of other Canadian caregivers? Pediatrics, 114(2), e128–e191.
Chan, K. G., Lim, K. A., & Ling, H. K. (2015). Care demands on mothers caring for a child with Down syndrome: Malaysian (Sarawak) mothers’ perspectives. International Journal of Nursing Practice, 21(5), 522–531. https://doi.org/10.1111/ijn.12275.
Creswell, J. W., & Plano Clark, V. L. (2011). Designing and conducting mixed methods research (2nd edn.). ed.). Thousadn Oaks, CA: SAGE.
Dodd, D. C., Zabriskie, R. B., Widmer, M. A., & Eggett, D. (2009). Contributions of family leisure to family functioning among families that include children with developmental disabilities. Journal of Leisure Research, 41(2), 261–286.
Dykens, E. M., Fisher, M. H., Taylor, J. L., Lambert, W., & Miodrag, N. (2014). Reducing distress in mothers of children with autism and other disabilities: A randomized trial. Pediatrics, 134(2), e454–463.
Golfenshtein, N., Srulovici, E., & Deatrick, J. A. (2016). Interventions for reducing parenting stress in families with pediatric conditions: An integrative review. Journal of Family Nursing, 22(4), 460–492.
Ketelaar, M., Bogossian, A., Saini, M., Visser-Meily, A., & Lach, L. M. (2017). Assessment of the family environment in pediatric neurodisability: A state-of-the-art review. Developmental Medicine and Child Neurology, 59(1), 259–269.
Kuhaneck, H. M., Burroughs, T., Wright, J., Lemanczyk, T., & Darragh, A. R. (2010). A qualitative study of coping in mothers of children with an Autism Spectrum Disorder. Physical & Occupational Therapy in Pediatrics, 30(4), 340–350. https://doi.org/10.3109/01942638.2010.481662.
Larson, E. (2010). Identifying indicators of well-being for caregivers of children with disabilities. Occupational Therapy International, 17(1), 29–39. https://doi.org/10.1002/oti.284.
Law, E. F., Fisher, E., Fales, J., Noel, M., & Eccleston, C. (2014). Systematic review and meta-analysis of parent and family based interventions for children and adolescents with chronic medical conditions. Journal of Pediatric Psychology, 39(8), 866–886.
Ly, A. R., & Goldberg, W. A. (2014). New measure for fathers of children with developmental challenges. Journal of Intellectual Disability Research, 58(5), 471–484.
McGuire, B. K., Crowe, T. K., Law, M., & VanLeit, B. (2004). Mothers of children with disabilities: Occupational concerns and solutions. OTJR: Occupation, Participation and Health, 24(2), 54–63. https://doi.org/10.1177/153944920402400203.
Miodrag, N., Burke, M., Tanner-Smith, E., & Hodapp, R. M. (2015). Adverse health in parents of children with disabilities and chronic health conditions: A meta-analysis using the Parenting Stress Index’s health Sub-domain. Journal of Intellectual Disability Research, 59(3), 257–271.
Montes, G., & Halterman, J. S. (2007). Psychological functioning and coping among mothers of children with autism: A population-based study. Pediatrics, 119(5), e1040–e1046.
Patton, M., Q. (2015). Qualitative Research and Evaluation Methods. (Fourth Ed. (Ed.)). Thousand Oaks, CA: SAGE.
Piotrowska, P. J., Tully, L. A., Lenroot, R., Kimonis, E., Hawes, D., Moul, C., Frick, P. J., Anderson, V., & Dadds, M. R. (2017). Mothers, fathers, and parental systems: A conceptual model of parental engagement in programmes for child mental health—connect, attend, participate, enact (CAPE). Clinical Child and Family Psychology Review, 20(2), 146–161.
Sartore, G., Lagioia, V., & Mildon, R. (2013). Peer support interventions for parents and carers of children with complex needs. Cochrane Databases of Systematic Reviews, 6, CD010618.
VanLeit, B., & Crowe, T. K. (2002). Outcomes of an occupational therapy program for mothers of children with disabilities: Impact on satisfaction with time use and occupational performance. American Journal of Occupational Therapy, 56(4), 402–410. https://doi.org/10.5014/ajot.56.4.402.
Zablotsky, B., Bradshaw, C. P., & Stuart, E. A. (2013). The association between mental health, stress, and coping supports in mothers of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 43(6), 1380–1393. https://doi.org/10.1007/s10803-012-1693-7.
Acknowledgments
The authors acknowledge and thank the following for financial support: Monash University and the Victorian Women’s Benevolent Trust fund. The authors acknowledge the following presenters: Ms Michelle Bihary; Dr Craig Hassad; Ms Paula Brodie; Mr Tony Catanese. The authors also sincerely thank occupational therapists Josie Duncan and Aislinn Lalor for assistance at different stages of delivery of the program and the conduction of this research. The research has been presented at the Australian Cerebral Palsy and Development Medicine conference in Adelaide in 2016, at the Australian National Occupational therapy Conference in Perth in 2017, and at the International Carers Conference in Adelaide Australia in 2017.
Funding
This study was funded by VictorianWomen’s Beneveolent Trust fund (no number) and Monash University Formative Grant (No number). Helen M. Bourke-Taylor and Fiona M. Jane received research grants from the Victorian Women’s Benevolent Trust and Monash University to deliver the workshops and conduct this research.
Author information
Authors and Affiliations
Contributions
The contributors to this research and manuscript are Helen Bourke-Taylor and Fiona Jane. Associate Professor Helen Bourke-Taylor PhD, is an occupational therapist within the School of Primary and Allied Health Care in the Faculty of Medicine Nursing and Health Sciences, at Monash University, Frankston, Australia and is the corresponding author. General Practitioner Fiona Jane MBBS is also a Research Fellow in the Women’s Health Research Program, School of Epidemiology and Preventative Medicine, Faculty of Medicine Nursing and Health Sciences, Monash University, Melbourne, Australia.
Corresponding author
Ethics declarations
Conflict of interest
Helen Bourke-Taylor and Fiona Jane have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all participants included in the study.
Rights and permissions
About this article

Cite this article
Bourke-Taylor, H.M., Jane, F.M. Mothers’ Experiences of a Women’s Health and Empowerment Program for Mothers of a Child with a Disability. J Autism Dev Disord 48, 2174–2186 (2018). https://doi.org/10.1007/s10803-018-3486-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-018-3486-0